
Abstract
Basic needs such as shelter and safety are at the core of any hierarchy of needs [1]. Individuals with mental illness often identify adequate shelter and a decent home as integral to their quality of life [2], [3]. Further, it is concerning that a significant proportion of people who are treated by mental health services are reported to be homeless. For example, a study undertaken in South Australia found that 27% of people admitted to an acute psychiatric unit were homeless prior to admission [4], while another study found that 15% of people experienced an episode of homelessness prior to or within 24 months of their first psychiatric hospitalization [5]. These figures compare with an estimated rate of 53.2 per 100 000 people homeless in the general population [6].
The reasons for the high rates of homelessness among people with mental disorders [7], [8] are not clear. Individuals with severe mental illness may be less able to advocate for themselves, have impaired problem-solving abilities, and be vulnerable to exploitation. The poverty associated with having a mental disorder may limit options available, especially when rental properties are in short supply. In addition, stigma and discrimination may make it difficult for people with a mental disorder to compete for the limited housing that is available and affordable to people living on restricted incomes. While there is some evidence to suggest that the onset of the mental disorder precedes the episode of homelessness [9], [10], in reality the relationship is likely to be complex, with a range of individual vulnerabilities and structural factors contributing to homelessness among people with a mental illness [11].
Research examining housing problems and homelessness among the mentally ill is problematic because there is no commonly agreed definition of homelessness. While narrow definitions define homelessness as the absence of housing, that is, people sleeping in areas not intended for human habitation such as public parks, it is also common for people living in shelters or welfare institutions to be regarded as homeless [12]. In Australia it has been suggested that homelessness should be subdivided into three distinct subtypes. These are: primary homelessness, which refers to people with no conventional housing; secondary homelessness, which describes people who move from one temporary form of housing to another; and tertiary homelessness, which refers to circumstances when housing falls below an acceptable community standard [13]. These different approaches to defining homelessness have different public health implications. More restrictive definitions of homelessness, which are limited to people without housing or who are staying in a temporary shelter, are important in identifying a vulnerable group of people who require specific, targeted interventions. Appropriately, much research has focused on the needs of this group [8], [14].
Understanding the relationship between housing and mental illness will be facilitated by the use of a broader definition of homelessness, which includes the concept of housing quality (tertiary homelessness). But if we are to advance research in this area, there is a need to develop an agreed basic set of measures of housing [15]. Although a measure of quality or ‘acceptable standard’ is critical if we are to further examine this area, defining what constitutes ‘adequate quality’ or an ‘acceptable standard’ of housing is complex. While the type and characteristics of housing are important in assessing quality, it is likely that the person's own perception will also be equally relevant. Indeed it could be argued that an individual's perception is the ultimate arbiter of quality. But the lack of attractiveness of alternative housing options may result in the acceptance of poor-quality housing among people with a mental disorder [16].
If we accept that having a stable, affordable, safe and appropriate place to live is important to a person's mental well-being, then it follows that public mental health services have an important role in assisting patients to achieve and maintain adequate housing. In Britain, the Health of the Nation Strategy [17] set specific mental health targets, one of which was ‘to improve significantly the health and social function of mentally ill people’. Acknowledging the importance of housing, the Health of the Nation Outcome Scales (HoNOS) lists housing and locality as one of the 12 items used to measure the achievement of this target.
Although there are data on the rates of homelessness among the mentally ill, little is known of the overall quality of housing (and the rates of tertiary homelessness) among patients treated by public mental health services in Australia. The aims of the present study were to (i) assess the quality of housing for patients receiving treatment from an area mental health service; (ii) compare estimates of quality of housing using two different methods: housing type versus housing characteristics; (iii) determine whether either method for assessing quality is more useful that a combination; and (iv) examine the relationship between housing quality and the case manager's assessment of the impact of the housing on the patient's mental disorder. Patient self assessment of the quality of their housing was not included in the study because of ethical and logistical difficulties.
Setting: Loddon Campaspe Southern Mallee Region, Australia
The Loddon Campaspe Southern Mallee (LCSM) Region is located in North Central Victoria, Australia (Figure 1). The region stretches from Gisborne in the south to beyond Swan Hill in the north and has a population of approximately 241 000 people. The region includes communities with diverse social, cultural and economic characteristics.
Loddon Campaspe Southern Mallee catchment area.
The central sector includes the regional city of Bendigo and surrounding suburbs and has a population of approx 99 000. The northern sector includes the townships of Swan Hill, Echuca and Kerang with a population of approx 72 000. It is characterized by substantial areas of socioeconomic disadvantage and has a significant proportion of Indigenous residents. The southern sector includes rural townships such as Castlemaine and Kyneton and the urban fringe regions of Gisborne, Woodend and Macedon with a population of approx 72 000.
Housing options in the region include private owned or rented house/flat, public housing, community housing (such as group housing, transitional housing, and crisis housing managed by non-government organizations on a not-for-profit basis), caravan parks, houseboats, motels and hotels. The number of public housing properties varies markedly across the region and there are large numbers of people on waiting lists for these properties [18].
Method
Housing survey
The development of a survey to audit the housing circumstances of patients of the LCSM Service is described elsewhere [18]. The survey included patient details (gender, age, treating team); housing type (e.g. rented flat, public housing, caravan); living arrangements (i.e. who the patient had been living with over the last 2 weeks); housing characteristics as assessed by the patient's case manager (affordability of housing, risk of violence, security of tenure, structural safety of the housing, and appropriateness of the housing to the patients physical needs); and an overall assessment by the case manager of the impact that the housing had on the patient's mental disorder.
The survey was completed by case managers in the continuing care and intensive case management teams located in the central region (Bendigo), the four rural teams (Swan Hill, Echuca, Castlemaine and Kyneton), and in the crisis assessment and treatment team. Case managers were asked to complete the housing survey on all patients seen during a 2 week period in 2003. The social worker located on the inpatient unit completed the survey for all patients admitted to the inpatient unit over a 3 month period.
Judgements about housing characteristics were made by the case manager using a 5-point scale. Each characteristic was rated on a 5-point scale from 0 = never true to 4 = always true. In determining whether a property was affordable, case managers made a judgement guided by the approach used by the Office of Housing. This approach considers as affordable, properties that are within 30% of income including rent assistance for low-income households. Assessment of the other characteristics was based on case managers’ knowledge of the patient and their housing circumstances.
Case managers were also asked to rate on a 10-point scale how much of an impact the patient's current housing was likely to have on their mental status, where a score of 1 = significantly negative impact on mental status, and 10 = minimal–low impact. Scores on housing characteristics were collapsed into two groups. A score of 0, 1 or 2 indicated that the characteristic was absent, while a score of 3 or 4 indicated that the characteristic was present. Scores on the 10-point scale were also collapsed into two categories: significant impact (scores 1–3) and minimal–low impact (scores 4–10).
To prevent patients being counted twice in the survey (e.g. patients included in the community sample may have been admitted to the inpatient unit) a sticker was placed on the cover of the file indicating that data had been collected. Clinicians completing the survey were advised to exclude patients for whom data had been previously collected.
Statistical method
Logistic regression was performed to determine predictors of case managers’ rating of housing impact on patients’ mental status. The criterion variable was whether the impact was significant (yes/no). The predictor variables were housing characteristics: affordability of housing, risk of violence, security of tenure, ability to access services, structural safety of the housing, and appropriateness of the housing to the patient's needs. These were also presented in the format (yes/no) to indicate whether the characteristic was present.
Results
Study population
Surveys were completed for a total of 362 patients (female, n = 179, 49%, mean age, 38.1±12.8 years; male, n = 183, 51%, mean age 36.8±11.7 years). This sample is similar to the patients treated by the service. In 2003, 1991 adults were treated in the community (48% male; 52% female). The average age of men was 36.8 years while women were slightly older at 38.1 years. In the same year, 223 people were admitted to the acute inpatient unit (52% male; 48% female) with the average age for men of 35.1 years while that for women was 40.2 years.
The majority of patients surveyed lived alone (37.6%), 19.1% lived with a parent and 15.4% lived with a partner.
Housing type
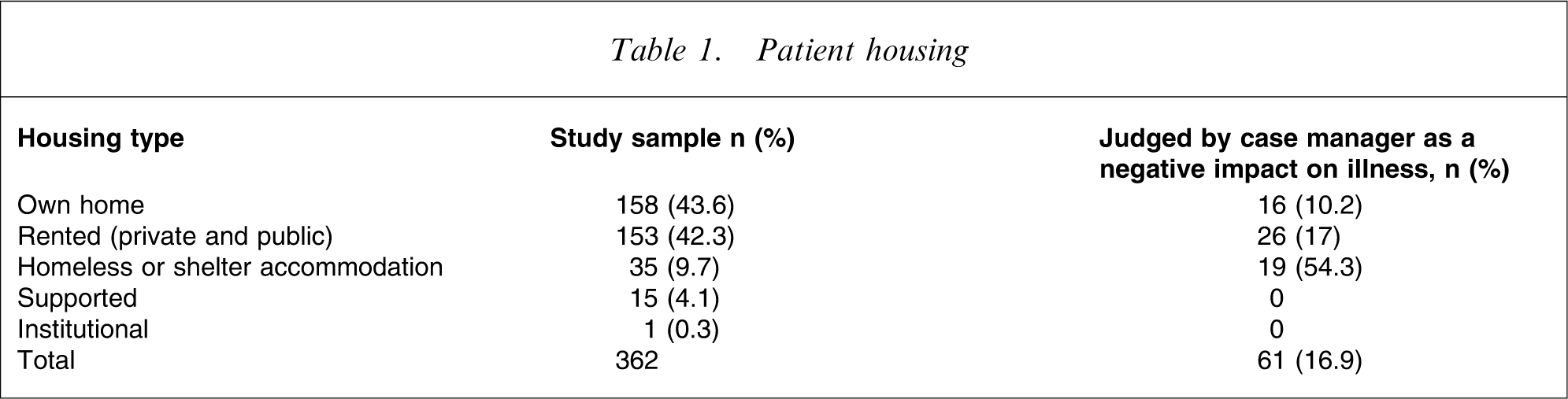
As shown in Table 1 most patients lived in their own home or rented premises. Just under 10% of patients (n = 35, 9.7%), were identified as homeless in that the person either had no housing or was living in a shelter or accommodation frequently associated with homeless persons (such as private hotel, caravan park).
Patient housing
Housing characteristics
Almost half (n = 173, 47.8%) of the patients in the sample had housing that was either not affordable, not secure, not safe or not appropriate to their needs, that is, their housing met at least one of the five criteria of poor housing characteristics as presented in Table 2.
Problematic housing characteristics
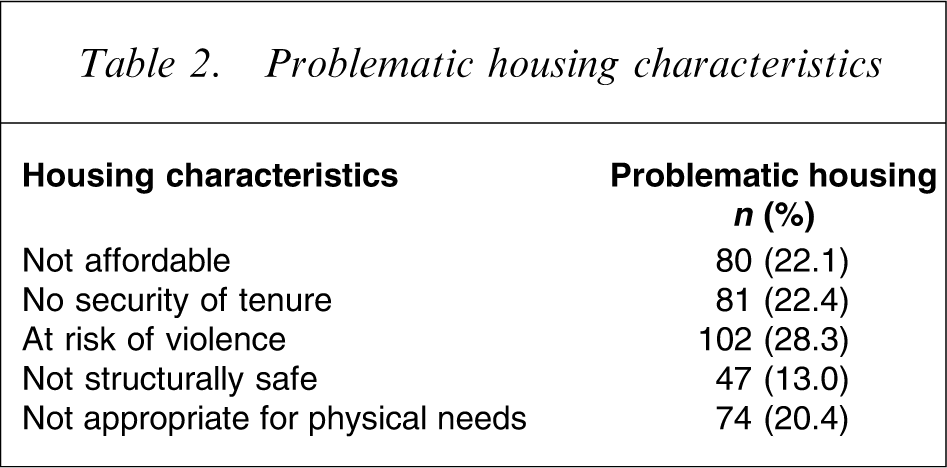
Of the 173, 18 (10%) had housing that met all five criteria for poor housing, that is, housing was not affordable, there was no security of tenure, there was risk of violence, or the housing was structurally unsafe and was not appropriate for the patients’ physical needs. Of these 18 individuals, one (5.6%) lived in his/her own or family home, seven (38.9%) lived in rental accommodation (private, n = 5; public, n = 2), and 10 (55.6%) were in a living situation defined as primary or secondary homelessness (caravan park, n = 2; squat, n = 1; staying with friends, n = 2; slept rough, n = 5). Two or more reasons for unsafe and insecure housing were endorsed for 95 patients (26.2%) in the sample. Of note for 102 patients (28.3%), risk of violence was identified as a factor affecting housing quality.
Of the 173 patients with problematic housing, just over one-third (n = 66, 38.2%) were living either in their own or the family home, 41.6% (n = 72) were living in rented accommodation and only 15.6% (n = 27) were living in a situation meeting the definition of primary or secondary homelessness. A smaller number were in supported accommodation (4.6%).
Judgement by case manager of impact of housing on patient mental illness
Case managers judged that housing had a significant negative impact on the individual's mental illness in 61 patients (16.9%), including 16 patients (10.2%) living in their own or the family home, 26 (17%) in rented accommodation and 19 (54.3%) in homeless or shelter accommodation.
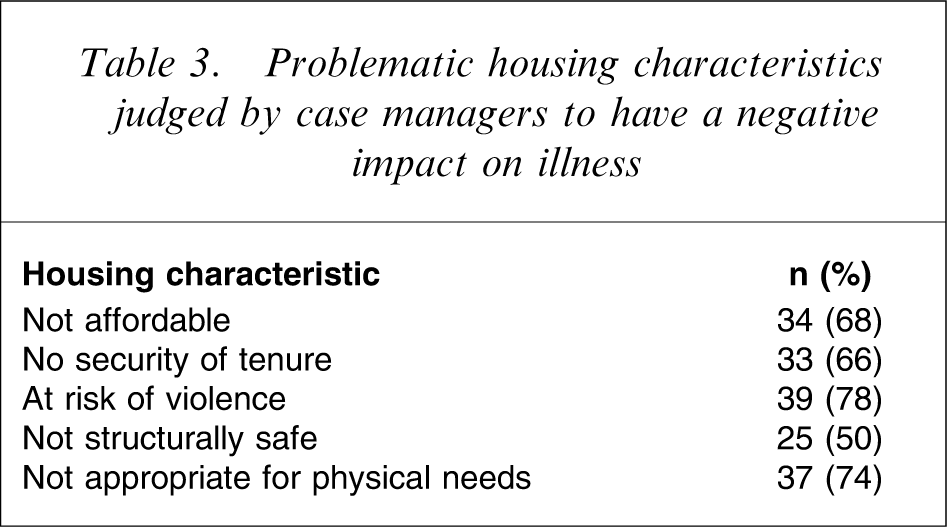
Table 3 lists the housing characteristics of the 50 individuals who had at least one problematic housing characteristic and whose housing was judged by their case manager to have a negative impact on their illness. Housing that was considered not structurally safe or not appropriate for the patients’ physical needs was most often considered to have a negative impact on a patient's mental status. To determine predictors of case managers’ rating of housing impact on patients’ mental status, a logistic regression was performed. The predictor variables (housing characteristics) were rated by the case manager who also rated the impact of those characteristics on mental health status (the grouping variable) and therefore were not independent. Allowing for this, the results showed that the two housing characteristic variables had a significant impact on mental health. First, the mental health of those judged to have housing inappropriate to their physical needs was 25% more likely to be judged to suffer compared to those whose housing was judged appropriate to their needs (odds ratio (OR) = 0.25; 95% confidence interval (CI) = 0.10–0.61). Second, the mental health of those without secure tenure of housing was 20% more likely to be judged to suffer compared to those with secure tenure of housing (OR = 0.20; 95% CI = 0.09–0.46). Although a high number of individuals were identified as being at risk of violence in their housing this was the least common housing characteristic associated with the case managers’ judgement that housing had a negative impact on the individual's mental illness.
Problematic housing characteristics judged by case managers to have a negative impact on illness
Eleven individuals had housing that was deemed by the case manager to be affordable, secure, safe, and appropriate to their needs but which nevertheless was judged by their case manager to have a significant negative impact on their illness. Five (45.5%) lived in their own or the family home, four (36.4%) were living in rental accommodation (private, n = 2; public, n = 2) and two (18.2%) were living in caravan parks.
Discussion
The present study illustrates that many individuals being treated by an area mental health service have poor-quality housing. When quality was judged by type of housing, the majority appeared to be in accommodation of an acceptable standard. In contrast, when judged by housing characteristics, just over 50% were in accommodation of an acceptable standard. Many of these people were living in their own or the family home, generally regarded as acceptable standard accommodation, or in rented accommodation, a term that covers a range of types of housing. This group can be regarded as meeting the definition of tertiary homelessness.
Generally, case managers failed to identify any negative impact of problematic housing on the mental state of patients. Their judgement of the impact of housing on a person's mental illness appeared to be largely influenced by the type of housing and appropriateness of the housing for the person's physical needs and security of tenure. Of note, although risk of violence was the characteristic most commonly identified in those with housing problems (n = 102, 28.3%), it was not common in those cases where the case manager judged housing to have a negative impact on the individual's mental illness. Perhaps case managers did not regard risk of violence as a characteristic of housing, but as a characteristic of the social environment within the housing.
How can the disparity between level of identified problematic housing characteristics and judgement of the likely impact of housing on an individual's mental illness be understood? Case managers may have a lack of knowledge about importance of quality housing for a person's mental health, or may simply judge the housing by type (such as caravan park) or physical characteristics (such as physical structure). The repeated exposure of case managers to patients with poor-quality housing may desensitize the case manager to housing problems among patients.
A reliable way of measuring housing quality or ‘acceptable standard’ is a clinical priority that will assist in identifying patients who need assistance to improve their housing circumstances. The data here suggest that such a measure should focus on characteristics rather than type of accommodation. This approach recognizes that some types of housing commonly regarded as ‘not acceptable’ such as caravans or houseboats may indeed be safe, secure and appropriate, while apparently ‘acceptable standard’ types of housing such as one's own or the family home are not always so.
Although not used in the present study, the patient's own perception of the quality of their housing is also likely to be an essential dimension of housing quality. Combining the person's subjective assessment of quality with an objective assessment of housing characteristics is likely to provide a useful method of assessing housing quality.
Implications for public mental health services
The poor quality of housing among many of the people treated by this public mental health service suggests that focusing on a narrow definition of homelessness (primary and secondary homelessness) seriously underestimates the magnitude of the housing problem among the seriously mentally ill. While it is possible that the problems identified here are local to this area, it is more likely that these difficulties will be found to be widespread. Consistent with this, it is now being acknowledged that mental health services and mental health professionals must take an interest in housing issues. Emphasizing this, Shepherd and Murray stated that ‘housing should be at the centre of community psychiatry’ [19]. The data here strongly support this statement and provide a challenge to public mental health services as well as to a variety of other services. Many of the solutions to the problem of housing among people with a mental disorder are beyond the scope of public mental health services. Factors such as lack of public housing, inadequate income support and stigma and discrimination, are all likely to be contributing to poor-quality housing.
Limitations of the study
Although logistical and ethical limitations prevented the inclusion of a patient self-report of housing quality, it is essential that future research include such a dimension. In addition, future studies should explore more broadly what patients believe are the important factors contributing to the quality of housing and what factors contribute to accommodation being identified as, and accepted as, ‘home’. No measure of inter-rater reliability was included in the development of the instrument, which needs further refinement as a measure of housing quality. In addition the study was conducted in a regional area. It is unclear whether the results are generalizable to other regional and urban settings.
Conclusion
Many patients treated by an area mental health service appear to have poor-quality housing. Housing characteristics identified a higher proportion of people with poor-quality housing than did housing type. Case managers’ assessments generally failed to identify the negative impact of problematic housing on the person's mental disorder.
Footnotes
Acknowledgements
This study was funded by the Latrobe University Bendigo Larger Grants Scheme. The authors gratefully acknowledge the assistance of the case managers and the inpatient unit social worker who provided the data presented here.