
Abstract
Objective:
The over-representation of mental illness among homeless people across the globe is well documented. However, there is a dearth of Australian literature on the mental health needs of homeless individuals. Furthermore, longitudinal research examining the factors that contribute to better housing outcomes among this population is sparse. The aim of this research is to describe the mental illness profile of a sample of homeless men in an Australian urban centre (in Sydney) and examine the factors associated with better housing outcomes at 12-month follow-up.
Methods:
A longitudinal survey was administered to 253 homeless men who were involved in the Michael Project: a 3-year initiative which combined existing accommodation support services with assertive case management and access to coordinated additional specialist allied health and support services. A total of 107 participants were followed up 12 months later. The survey examined the demographics of the sample and lifetime mental disorder diagnoses, and also included psychological screeners for current substance use and dependence, psychological distress, psychosis, and post-traumatic stress.
Results:
Consistent with existing literature, the prevalence of mental illness was significantly greater amongst this sample than the general Australian population. However, mental illness presentation was not associated with housing situation at 12-month follow-up. Instead, type of support service at baseline was the best predictor of housing outcome, wherein participants who received short to medium-term accommodation and support were significantly more likely to be housed in stable, long-term housing at the 12-month follow-up than participants who received outreach or emergency accommodation support.
Conclusions:
This study provides evidence to support an innovative support model for homeless people in Australia and contributes to the limited Australian research on mental illness in this population.
Introduction
Mental illness is one of many potential pathways into homelessness (Rota-Bartelink and Lipmann, 2007; Shelton et al., 2009), and its prevalence among the homeless population is an ever-growing concern (Toro et al., 2007). However, the task of measuring the prevalence of mental illness in homeless populations is inherently difficult, not least because of the transient lifestyle of many people experiencing homelessness. Prevalence estimates are also dependent on factors related to measurement, including how narrow or broadly the population is defined (Minnery and Greenhalgh, 2007), and the specific disorders included (Fazel et al., 2008). Large discrepancies between estimates of mental illness in this population reflect these and other methodological differences. Additionally, the presence of psychopathology in an individual who is enduring extreme social exclusion and physical deprivation will also affect the estimate made (Daiski, 2007). When considering the relationship between mental illness and homelessness, there are two distinct approaches that may be taken. First, one may consider the prevalence of homelessness in the mentally ill population (for example, Holmes et al., 2005; Jablensky et al., 2000). The second approach considers the prevalence of mental illness in the homeless population. This paper takes the latter approach.
A meta-analysis of prevalence studies conducted across seven western countries, including Australia, found that alcohol and drug dependence were the most common mental disorders observed among people experiencing homelessness, with prevalence estimates of 38% and 24%, respectively (Fazel et al., 2008). Personality disorder was the next most common mental disorder (23%), followed by psychotic illness (13%), and major depression (11%). In spite of establishing strict criteria for study selection using a systematic review approach, there was a high level of heterogeneity in prevalence estimates between studies resulting from diversity in the study populations and differences in methods adopted to measure prevalence.
Research conducted in Germany observed marked dissimilarities between a representative sample of 265 homeless men and an age-matched comparison group on the prevalence of mental disorders outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV; American Psychiatric Association, 1994). Overall, 93% of the homeless men had at least one lifetime DSM-IV axis I diagnosis, compared to only 38% of the community controls (Fichter and Quadflieg, 2001). Specifically, a large proportion of the homeless men met criteria for a mood disorder (33% vs 3% control), anxiety disorder (16% vs 6% control), and psychotic disorder (10% vs 0.6% control). A 3-year follow-up of the participants indicated that there was a marked improvement in housing situation (Fichter and Quadflieg, 2005). Furthermore, rates of mental illness reduced from 79% to 66%, which the authors contend may be a consequence of improved housing and increased medical/psychiatric support. Interestingly, mental health status at baseline did not predict housing situation at follow-up.
Only a few Australian studies have been carried out. A review of 4252 case files of clients accessing a specialist homelessness service in Melbourne found that 30% of the sample had mental health issues (Chamberlain et al., 2007). However, this figure is likely to be an underestimate given that individuals accessing homelessness support may not be forthcoming about mental illness (including substance use issues), or may have never been adequately assessed for mental illness by a mental health professional. In another study, which conducted structured clinical interviews with 210 randomly selected homeless individuals in Sydney, 73% of men and 81% of women met criteria for at least one mental disorder (Teesson et al., 2004). Specifically, a large proportion met criteria for alcohol dependence/abuse (men=49%; women=15%), drug dependence/abuse (men=34%; women=44%), mood disorder (men=28%; women=48%), anxiety disorder (men=22%; women=36%), and schizophrenia (men=23%; women=46%). All rates were substantially higher than the general Australian population. Moreover, over 90% of 119 men and all 38 women interviewed had experienced at least one traumatic event in their lifetime (Buhrich et al., 2000). In contrast, only 57% of the general Australian population report one major traumatic event in their life (O’Donnell et al., 2012). Given the over-representation of trauma experiences in homeless populations, it is perhaps not surprising that both the lifetime and 12-month prevalence rates for post-traumatic stress disorder (PTSD) amongst another sample of adults experiencing homelessness in Sydney were found to be high: 79% and 41%, respectively (Taylor and Sharpe, 2008). In another study, among a representative sample of men and women living in marginal housing in Melbourne (which excluded participants who were sleeping rough), the estimated prevalence for lifetime psychotic disorders was also found to be high at 42% (Herrman et al., 2004).
In line with the significant social and physical deprivation associated with homelessness, psychological distress has also been found to be higher in this group than in the general population. Research conducted in the USA found distress symptoms to be most pervasive and persistent among homeless individuals who had a severe mental illness (Wong, 2002). Specifically, 90% of participants with a severe mental disorder were classified as experiencing psychological distress, while 61% of participants who were substance dependent and 54% of participants with no diagnosis were classified as experiencing psychological distress.
High rates of comorbid mental illness, substance abuse, physical disorders, and cognitive impairment have been observed in this population, with prevalence estimates of comorbidity ranging from 2% to 34% of the homeless population (Drake et al., 1991; Spence et al., 2004). This pattern of multiple complex health concerns exacerbates the burden of disability and is linked to poorer treatment outcomes (Compton III et al., 2003). In turn, the provision of services to individuals with this type of comorbidity has been identified as one of the most pressing issues in the mental health field (Drake, 2007; Lee et al., 2012). However, the complexity and diversity within the homeless population presents a challenge for developing effective services appropriate to the needs of individuals within this population (Chamberlain et al., 2007).
There are few published Australian studies that document the specific mental health needs of the local homeless population, and even fewer longitudinal studies that examine the long-term mental health and housing outcomes of homeless individuals with a mental illness. The absence of a rich evidence base ultimately impacts on the development of appropriate policy and interventions in the homelessness service sector. Thus, the first aim of this paper is to describe an Australian sample of homeless individuals and document the mental health needs of this group. The second aim is to examine whether mental health impacts on the achievement of stable, long-term housing at 12-month follow-up. Lastly, this paper will investigate whether the achievement of stable housing has any impact on participants’ mental health.
Method
Design 1
The study used a longitudinal design and surveyed participants at entry to support (W1) and at 3 (W2) and 12 months (W3) post-baseline. Only data from W1 and W3 is used in the present study. This research derives from a broader study that explored the effectiveness and cost-effectiveness of the Michael Project (MP), a 3-year initiative (2007–2010) working with homeless men in Sydney. The MP was run by Mission Australia (MA), a non-denominational Christian community service organisation, and funded philanthropically. The MP was a unique model of support designed around the principles of client-centered care and integrated service delivery. It combined existing accommodation support services offered by MA with assertive case management (ACM), and access to a suite of additional specialist allied health and support services.
Specifically, prior to the introduction of the MP, MA already provided seven homelessness services around Sydney, including: a mobile outreach service to homeless people on the streets; an overnight crisis accommodation service; three short-term accommodation services providing accommodation for up to 3 months; a medium-term accommodation service providing somewhat longer support; and a transitional housing service. The suite of specialist services was wrapped around these existing homelessness services to form the MP. The specialist services included: an alcohol and other drug (AOD) counsellor, a psychologist, an occupational therapist, dental health services, a podiatrist, an outreach nurse, an Indigenous outreach worker, a recreational officer, a barber, a computer tutor, and a literacy and numeracy tutor. While the MP assisted clients to find housing as part of case management goals, the model itself did not provide housing. The ACM approach drew on evidence-based practice from the assertive community treatment model, and particularly focused on being persistent and active, following clients’ self-directed priorities and timing, respecting clients’ autonomy, and nurturing trust (Lee et al., 2010; Rosen et al., 2007). Clients across all services were linked into the specialist services through the ACM approach, in which all caseworkers were trained.
Participants
Given this study was part of a larger service-based program evaluation, two slightly different recruitment methods were used based on the duration of support provided by the different services involved. In the short–medium-term accommodation services (‘short-medium sample’), the client survey was undertaken by caseworkers as part of the assessment and case management process. Thus there was an expectation that all clients were approached. At the time of data collection there was no centralised service database and consequently the participation rate among all clients could not be verified, nor could the profile of participants and non-participants be compared. However, periodic visits to the services by the research team during the recruitment phase did not reveal any problems in the uptake of the research or in the confidence of caseworkers to undertake the client survey.
There was less capacity to undertake the client survey with every client that accessed the outreach and emergency accommodation services (‘outreach/emergency sample’) as the nature of these services meant the duration of contact with clients was relatively short. Thus only every second client was approached to participate in the research. An attempt was made to record which clients were approached using the existing service contact record sheets; however, this information was not reliably collected.
The MP participants were male clients of MA, aged 18 years and over. In total, 253 men participated: 156 in the short-medium sample and 97 in the outreach/emergency sample. All participants were experiencing primary homelessness (without conventional accommodation, such as sleeping rough) or secondary homelessness (in transient accommodation, including supported accommodation) when they were first interviewed. Individuals were ineligible to participate if they were intoxicated, if they were not oriented to time and place (Mini Mental State Examination; Folstein et al., 1975), or if their English level was very poor.
Examination of participants recruited via the different pathways revealed that there were several significant differences between the short-medium sample and the outreach/emergency sample at W1. Compared to the short-medium sample, the outreach/emergency sample had a significantly higher proportion of Indigenous participants (13.8% vs 6.0%, p=0.036), was significantly less likely to have completed a post-school qualification (37.2% vs 52.4%, p=0.022), but more likely to be employed (12.4% vs 4.5%, p=0.022) and to meet criteria for current drug dependence (40.9% vs 23.5%, p=0.004). Regarding the high number of Indigenous participants in the outreach/emergency sample, there was an Indigenous outreach worker employed as part of the outreach team, specifically to address the low access to MA’s accommodation services in this population. The Indigenous outreach worker contributed to the recruitment and administration of the baseline survey and, as such, the higher number of Indigenous participants in the outreach/emergency sample relative to the short-medium sample was attributed to this.
At the 12-month follow-up, 42.3% of participants (n=107) were successfully followed up and re-interviewed: 47.4% (n=74) of participants from the short-medium sample, and 34.0% (n=33) of participants from the outreach/emergency sample. Comparison of the total follow-up sample to the original W1 sample revealed no significant differences on any of the variables investigated in this paper.
Materials
The MP client survey collected information on the backgrounds, needs, and outcomes of homeless men receiving support through MA’s Sydney services. The survey incorporated an extensive range of questions and instruments related to homelessness history, mental health, quality of life, service utilisation, and criminal justice contact. The survey took approximately 60–90 minutes to administer. A shorter version of the survey, which took approximately 45–60 minutes to administer, was administered to the outreach/emergency sample. This decision addressed the ethical concerns of undertaking a lengthy survey with clients in highly tenuous accommodation circumstances, and because the outreach/emergency services had a short duration of contact with clients.
The current study utilised an array of mental health and housing measures, as follows.
Psychological distress was measured using the 10-item Kessler Psychological Distress Scale (K10; Kessler et al., 2003). The K10 is a validated instrument and has Australian normative data (Slade et al., 2011).
Self-reported mental disorder diagnoses were measured by a single question that asked participants whether they had ever been diagnosed by a medical practitioner or psychologist as experiencing any of the following mental disorders: mood disorder, anxiety disorder, personality disorder, psychotic disorder, dissociative disorder, substance use disorder, eating disorder, or impulse-control disorder.
Substance dependence was assessed for all substances used in the previous month using the 5-item Severity of Dependence Scale (SDS). The scale has been shown to have good psychometric properties and has been used to assess dependence on different classes of drugs and alcohol (Gossop et al., 1997). Based on the research literature, different cut-off scores were used for each substance (for example, Cuevas et al., 2000; Kaye and Darke, 2002; Lawrinson et al., 2007; Topp and Mattick, 1997). This information was then categorised into two variables: alcohol dependence and drug dependence.
Traumatic stress response (past month) was measured using the 17-item PTSD Checklist–Civilian Version (PCL-C; Weathers et al., 1993). The PCL-C has demonstrated strong psychometric properties (Ruggiero et al., 2003). Participants were given the option to self-complete this measure.
Psychosis was measured using the 10-item Psychosis Screener (PS; Degenhardt et al., 2005), developed specifically for the National Survey of Mental Health and Wellbeing (NSMHW), which ascertains lifetime and 12-month prevalence of psychosis. The measure is reported to have moderate sensitivity and specificity.
Information on housing and homelessness was collected via a series of questions regarding current and past year accommodation circumstances. Housing outcome was collapsed into a binary variable – housed or not housed in stable, long-term housing. Stable, long-term housing was defined as any option under the long-term tenure category, which included: purchasing/purchased own dwelling, private rental, public housing rental, and long-term community housing accommodation.
The shorter survey used with the outreach/emergency sample did not include the traumatic stress response or psychosis measures.
Procedure
The baseline client survey was administered by caseworkers to new MA clients at the start of their support period, or as soon as appropriate given the client’s needs. To assist with the slow recruitment from the outreach/emergency services, research officers conducted approximately half of the baseline surveys in this sample. All participants were provided with a Participant Information Statement and provided written consent to complete the surveys and to be contacted for the follow-up surveys. Participants were re-administered the survey at 3 and 12 months by a trained research interviewer. Participants were reimbursed in vouchers for each survey attempted, whether or not the survey was completed.
Data analysis
Data were analysed using the statistical software package SPSS (Version 21; IBM Corp., 2012). Analysis of variance (ANOVA) was used for analyses involving continuous outcome variables, while a combination of chi-squared and binary logistic regression analyses were used for categorical outcome variables. McNemar’s test was used to assess changes over time on dichotomous variables for the housed and non-housed groups.
In all multivariate regression analyses, Indigenous status was included as a covariate as Indigenous people are more likely to experience homelessness than other Australians (MacKenzie and Chamberlain, 2008). In addition, age was included to control for greater potential exposure to homelessness. Furthermore, research suggests that older age is associated with greater housing success among homeless people with a mental illness (Lipton et al., 2000).
Results
Demographics
Table 1 presents the demographic and mental illness profile of participants at W1. Participants ranged in age from 19 to 82 years (mean: 41 years). Of the 253 participants, one in 11 (9%) identified as Aboriginal and/or Torres Strait Islander, almost half (46%) had completed a post-school qualification, and one in 13 (8%) were employed at the time of the baseline survey. The mean age that participants had first slept rough was 28 years; however, this ranged from 5 to 60 years.
Demographic and mental illness profile of participants at baseline (n=253).
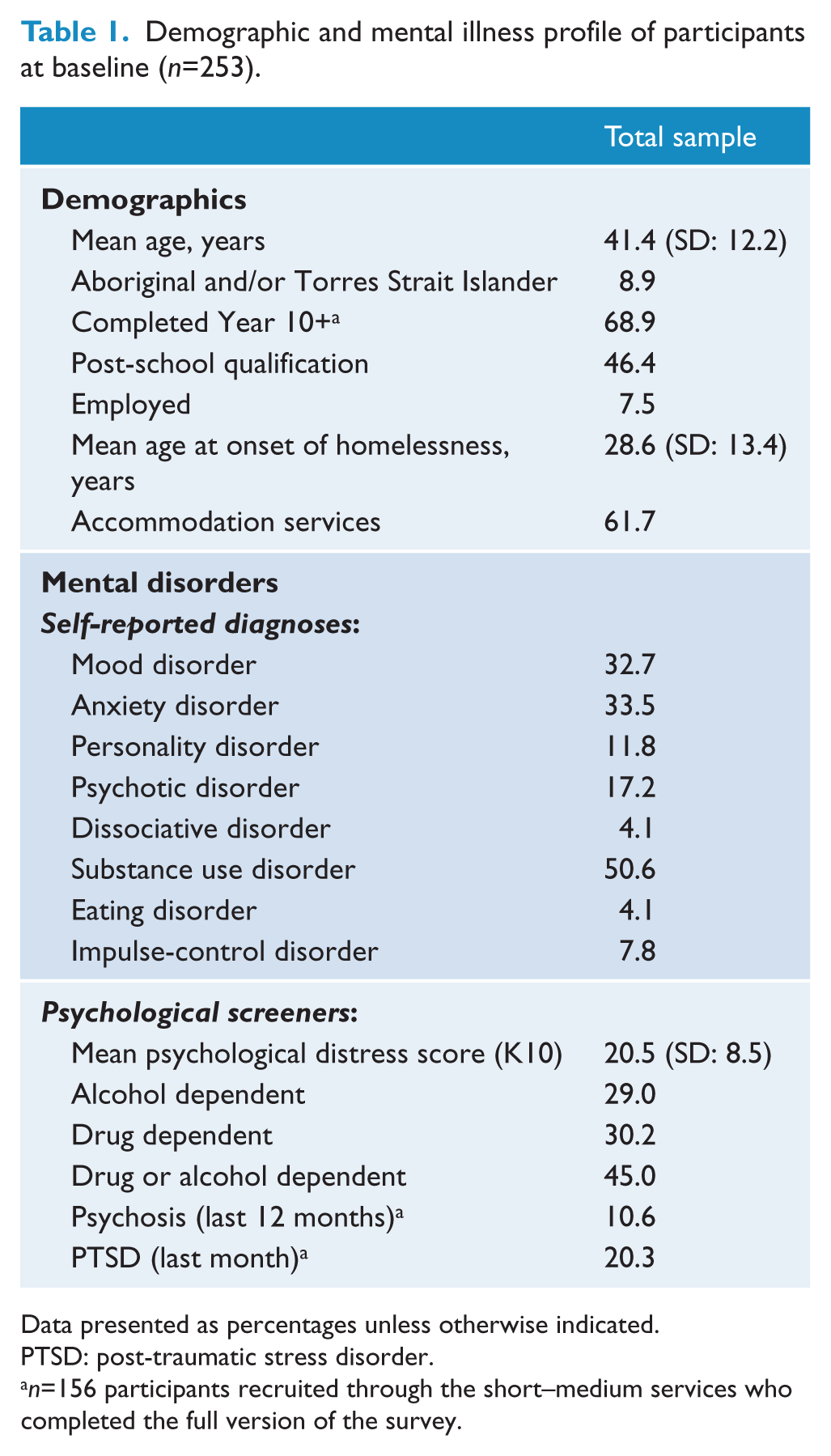
Data presented as percentages unless otherwise indicated.
PTSD: post-traumatic stress disorder.
n=156 participants recruited through the short–medium services who completed the full version of the survey.
Mental health
Almost three-quarters (71%) of participants reported being diagnosed by a mental health practitioner with one or more mental disorders over their lifetime. Specifically, one in four (25%) reported one mental disorder, one in five (21%) reported having two mental disorders, and one in four (26%) reported having three or more mental disorders. Among those who had been diagnosed with a mental disorder, the average number of disorders was 2.3 (range: 1–9 diagnoses). Substance use disorder was the most commonly reported mental disorder (51%). Anxiety (34%) and mood (33%) disorders were the next most commonly reported mental disorders.
Results on the K10 indicated that half of the participants were experiencing high (27%) or very high (22%) levels of psychological distress, with the mean score falling within the moderate range. Based on responses on the SDS and recent substance use, at the time of the W1 interview, almost one in three participants met criteria for drug dependence and alcohol dependence in the last month, respectively. Further analysis indicated that poly-substance dependence was common: half (50%) of the participants who were alcohol dependent were also drug dependent. Among participants who completed the full version of the survey, one in five (20%) screened positive for PTSD in the last month, and one in 10 (11%) screened positive for having experienced psychosis in the last 12 months.
Health service utilisation
Among all participants, one in nine (11%) had accessed the AOD counsellor through the MP. Of those who accessed this service, the median number of contacts was two (range: 1–14). Similarly, one in nine (11%) participants had accessed the MP psychologist. Of those who had accessed this service, the median number of contacts was 2.5 (range: 1–27). One in 17 (6%) participants had accessed both the AOD counsellor and psychologist at least once. There was a significant correlation between number of contacts with the AOD counsellor and number of contacts with the psychologist (r=0.261, p<0.001).
Housing and mental illness at the 12-month follow-up
To compare participants accommodated in stable, long-term housing at the 12-month follow-up (n=48) to those not accommodated in stable housing (n=59), ANOVA and chi-squared analyses were conducted for continuous and categorical variables, respectively (Table 2). Overall, the two groups did not differ significantly on any of the reported demographics. Type of support service provided at baseline was found to be associated with housing status at W3, wherein participants recruited through the short-medium services were significantly more likely to be in stable housing at the 12-month follow-up than those recruited through the outreach/emergency services. Specifically, 52% of participants in the short-medium sample were stably housed at follow-up, compared to 27% of participants in the outreach/emergency sample. In addition, participants who met criteria for drug dependence at baseline were significantly less likely to be housed at follow-up. There were no other significant differences between the housed and non-housed groups in regard to mental illness at the univariate level. Examination of the service utilisation data also indicated that there was no significant difference between the groups in terms of number of contacts with the MP psychologist or AOD counsellor.
Predictors of housing at W3 (n=107).
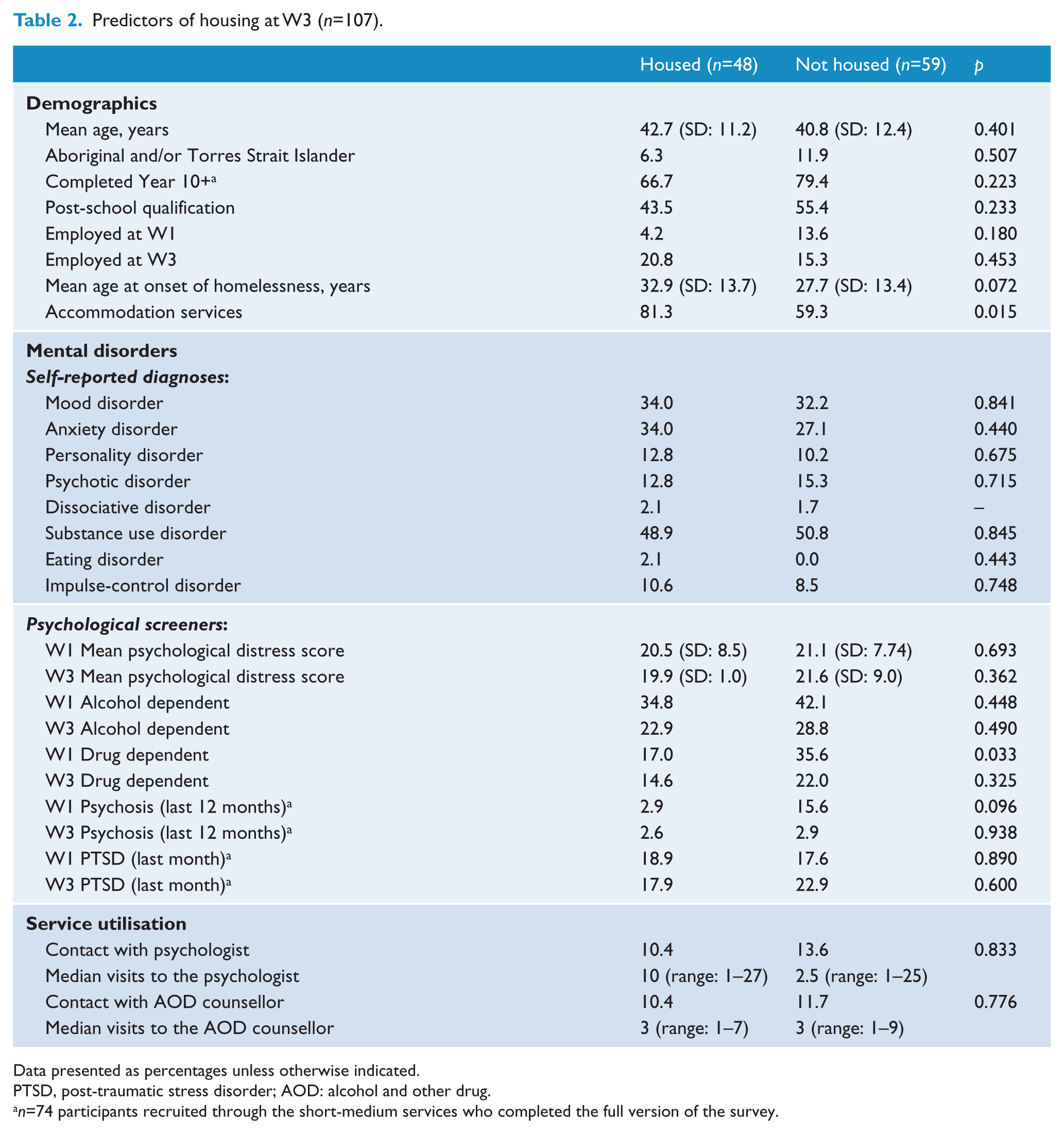
Data presented as percentages unless otherwise indicated.
PTSD, post-traumatic stress disorder; AOD: alcohol and other drug.
n=74 participants recruited through the short-medium services who completed the full version of the survey.
Predicting housing outcome at 12-months
In order to examine which factors best predicted housing outcome at the 12-month follow-up, multivariate binary logistic regression analysis was conducted. The first model included variables with p-values below 0.1 at the univariate level, including support service, W1 drug dependence, and age at onset of primary homelessness (and controlling for the covariates of Indigenous status and age). Recent psychosis was included in a second model as not all participants completed this instrument. In this model, which demonstrated overall significance (p=0.026), participants recruited through the short-medium services remained significantly more likely to be in stable housing at the 12-month follow-up, compared to the outreach/emergency sample (p=0.023). No other variables were significant at the multivariate level.
A second multivariate regression was conducted using the same variables outlined above but also including recent psychosis (p<0.1) and excluding support service (which was redundant given the psychosis screener was only administered to participants in the short-medium sample). This model was not found to be significant overall (p=0.093).
Predictors of mental health at 12-months
Further analysis was conducted to examine whether there were any changes in mental illness from baseline to follow-up for the housed and non-housed participants, respectively. For both the housed and non-housed groups, from W1 to W3 there was no overall change in psychological distress (p=0.539 and p=0.645, respectively), with the mean for both groups remaining in the moderate range of distress. While alcohol dependence among both groups decreased from W1 to W3, this did not reach significance (McNemar’s test for matched subject pairs; p=0.070 and p=0.057 for the housed and non-housed groups, respectively). Similarly, while there was a reduction in the proportion of participants screening positive for drug dependence among the non-housed group, this did not reach significance (p=0.115); there was no overall change in drug dependence for the housed group. Finally, among both groups, there was no significant change from W1 to W3 in the proportion of participants who screened positive for either psychosis in the previous 12 months or PTSD in the last month.
Discussion
This study supports existing Australian and international research showing that mental health problems are more prevalent among people experiencing homelessness than the general population. Consistent with other samples in Sydney (Teesson et al., 2004), almost three-quarters of the male participants in this study had been diagnosed with a mental disorder over their lifetime. Compared to the 2007 NSMHW (Slade et al., 2009), the current sample had a significantly higher prevalence of substance use (51% vs 25%; p<0.0001), anxiety (34% vs 26%; p=0.011), and mood (33% vs 15%; p<0.0001) disorders. These differences are reflected in the high levels of psychological distress in the sample, with half of the men in this study scoring in the high or very high range of psychological distress, a finding consistent with previous research (Wong, 2002).
Several explanations have been put forward to account for this, including the extreme physical and social deprivation endured by people experiencing homelessness. In addition, mental illness itself has been identified as a pathway into homelessness (Johnson and Chamberlain, 2011). Regardless of whether mental illness pre-dates or is a consequence of homelessness, individuals need to be assessed properly and treatment matched to their specific mental health needs (Clark and Rich, 2003). Given effective treatments are now available, particularly for affective disorders, further research should be undertaken to determine how they may best be delivered to this group. Previous research suggests that an integrated approach is gold standard, where stable accommodation is provided whilst simultaneously engaging individuals in treatment for mental health and substance use issues (Milby et al., 2005). While the MP adopted an integrated approach to homelessness and mental health, utilisation of the psychologist and AOD counsellor was minimal, despite an assertive case management approach. Hence, this study suggests that simply providing services is not sufficient for complex clients presenting with comorbidity. This underutilisation of mental health services has similarly been observed in other research involving homeless men (Fichter and Quadflieg, 2005).
One potential reason why these services were not accessed in spite of their availability could be the perceived stigma associated with accessing mental health services, as well as the stigma attached to being homeless, both of which have been shown to be barriers to accessing health services (Gelberg et al., 2004; Jezewski, 1995). However, in the case of the MP, the AOD and mental health services were provided on-site in a setting in which only homeless people were present. This study suggests that more innovative ways of engaging individuals into services need to be explored and incorporated into an integrated service delivery model that is appropriate for this heterogeneous population.
We found that mental health status at baseline was not a significant predictor of housing outcome at 12-month follow-up, suggesting other factors are important. This finding is supported by one other longitudinal study (Fichter and Quadflieg, 2005), but is contrary to others, which found that symptoms of depression and anxiety, and substance use were associated with poorer housing outcomes at follow-up (Lee et al., 2009; O’Connell et al., 2008). This may be due to methodological differences, including the nature of the services provided – the latter studies included access to housing, which was not the case in the MP.
As expected, participants recruited through the short-medium term services were significantly more likely to have achieved stable housing at the 12-month follow-up than participants recruited via the outreach/emergency services. There are several explanations for this finding. First, most specialist services had a waiting list and some only occurred once per fortnight. This meant that the short-medium sample participants could be reminded of their appointments and assisted to attend them. In comparison, participants from the outreach/emergency sample had typically left the service before the date of their appointment. Second, caseworkers had more opportunity to work with participants in the short-medium services relative to the outreach/emergency services, potentially providing a greater level of support and social engagement. Individuals could only stay at the emergency accommodation service for a maximum of 3 nights at a time, many of whom then slept rough on the streets. Support through the outreach service was more complex, particularly as this relied on the outreach workers being able to locate the homeless men. Thus, while the emergency/outreach participants were able to access the full set of services, the practicalities of their circumstances may have precluded them from realising all opportunities.
While mental health was not a predictor of housing, the stability and support offered through the accommodation services may have been sufficient to allow participants to seek and achieve long-term housing, regardless of mental illness and AOD issues. Half of the participants from the accommodation services who were followed up had achieved stable, long-term housing, compared to a quarter of participants in the outreach/emergency sample. However, it is important to note that only 34% of participants from the outreach/emergency services were successfully followed up, nine of which were housed in stable accommodation. Hence, the small number of housed participants in the outreach/emergency sample makes it difficult to make inferences from the data with confidence. Further work is required on this issue.
This study found no significant change in housed participants’ mental health presentation with respect to level of psychological distress, substance use, or recent psychosis or PTSD symptoms. Research by Wong (2002) investigating psychological distress amongst people experiencing homelessness found that for participants with no mental disorder who obtained their own apartment, psychological distress significantly reduced, whereas for participants with a severe mental illness or substance use disorder, there was no significant change in psychological distress. In the current study, this level of analysis was not possible given the small sample size for participants who were housed at the 12-month follow-up (n=48). Furthermore, given the current study did not examine the length of time that participants were stably housed, a participant may have only been housed for a day to meet the criteria of being housed. Thus, it is difficult to ascertain the specific impact of stable accommodation on mental health. Previous longitudinal research found that mental health improved over a 3-year period, which the authors argued may be because of an improved housing situation, as well as increased medical/psychiatric support (Fichter and Quadflieg, 2005).
There are several limitations associated with the present study. First, given the MP was conducted only among males experiencing homelessness, the results of this study cannot, therefore, be generalised to females. Second, whether these prevalence estimates, drawn from an urban centre, are representative of homeless people in other urban regions around Australia requires further investigation. Third, owing to the difficulties experienced following up this transient group, a smaller sample size was re-interviewed at the 12-month follow-up, which limited the analyses that could be conducted. Nevertheless, this remains one of the largest longitudinal studies completed to date on a sample of people experiencing homelessness in Australia. Fourth, owing to a shorter duration of contact with clients of the outreach and emergency accommodation services, ethical concerns dictated an abridged version of the client survey should be provided, which excluded two of the psychological screeners used in the present study: the psychosis and PTSD screener. As such, it is possible that the prevalence of PTSD and/or psychosis differed between the short-medium and outreach/emergency samples, which could have contributed to the significant difference in housing outcomes. Fifth, while it would have been ideal to administer structured clinical interviews to ascertain precise diagnostic information, this was impractical for the purposes of this study. Arguably, the prevalence of mental disorders in this sample may be an underestimate given that not all individuals may have accessed a mental health professional to receive a diagnosis and, furthermore, participants may not have been forthcoming with information about mental health and AOD issues with caseworkers when signing up for support.
In summary, this study contributes to the evidence base in Australia examining the relationship between housing, homelessness, and mental health. Despite a high level of mental health issues in people who are homeless, access to supported accommodation and specialist services can improve housing outcomes.
Footnotes
Acknowledgements
We acknowledge the Michael Project staff and participants who have enabled this nationally significant research to be undertaken. We also acknowledge the contributions of Tim Marchant, Kathryn Di Nicola, Alicia Bauskis, Marina Athanassios, Karen Larsen, Anne Hampshire, Shelley Mallett, Kathryn Taylor, Richard Bryant, Emma Black and Sean Lappin, who contributed to the study to ensure its success.
Funding
This study was funded through philanthropic donation to Mission Australia, which was then used to fund the Michael Project and its associated research component.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.