
Abstract
Objective:
To identify factors associated with receiving electroconvulsive therapy (ECT) for serious psychiatric conditions.
Methods:
Retrospective observational study using hospital administrative data linked with death registrations and outpatient mental health data in New South Wales (NSW), Australia. The cohort included patients admitted with a primary psychiatric diagnosis between 2013 and 2022. The outcome measure was receipt of ECT.
Results:
Of 94,950 patients, 3465 (3.6%) received ECT. The likelihood of receiving ECT was higher in older (hazard ratio [HR] = 1.03), female (HR = 1.24) patients. Compared to depression, patients with schizophrenia/schizoaffective disorder (HR = 0.79), schizophrenia-related disorders (HR = 0.37), mania (HR = 0.64) and other mood disorders (HR = 0.45) had lower odds of receiving ECT. Patients with depression and one other serious psychiatric condition had higher odds of receiving ECT than depression alone. Bipolar disorder likelihood of ECT did not differ from depression. A higher number of mental health outpatient visits in the prior year and an involuntary index admission with depression were also associated with receiving ECT. Likelihood of receiving ECT increased with year of admission (HR = 1.32), private patient status (HR = 2.06), higher socioeconomic status (HR = 1.09) and being married (HR = 1.25).
Conclusions:
ECT use for depression and bipolar disorder in NSW aligns with clinical national guidelines. Patients with schizophrenia/schizoaffective, schizophrenia-related disorders, mania and other mood disorders had lower likelihood of ECT than depression, despite ECT being recommended by clinical guidelines for these diagnoses. Variations in ECT were strongly associated with healthcare access, with private patients twice as likely to receive ECT than their public counterparts, suggesting a need to explore ECT accessibility.
Introduction
Serious depressive and psychotic illnesses contribute to high rates of hospitalisation and suicide, functional impairment, extended illness, loss of productivity and reduced quality of life (Espinoza and Kellner, 2022; Simon, 2003). In Australia, depressive disorders are ranked as the fourth leading cause of burden of disease (World Health Organization, 2020), and mental illness and suicide are estimated by the Productivity Commission to cost Australians $180 billion per year (Productivity Commission, 2020). The prevalence of serious mental illness and psychotic disorders in Australia is 3% and 0.5%, respectively, (Australian Institute of Health and Welfare, 2023).
Electroconvulsive therapy (ECT) is an effective treatment for patients with serious mood and psychotic disorders (Espinoza and Kellner, 2022), with an estimated 1.4 million people worldwide treated annually with ECT (Kirov et al., 2021). ECT involves the delivery of a small, pulsed electrical current to induce a seizure under general anaesthesia with the therapeutic intent to rapidly reduce symptoms of psychiatric disorders (The Royal Australian and New Zealand College of Psychiatrists (RANZCP), 2019). ECT yields a more potent anti-depressive effect than standard medication therapies (Lisanby, 2007) and has been consistently demonstrated to be superior to both placebo and pharmacotherapy (Janicak et al., 1985; UK ECT Review Group, 2003). In meta-analyses, ECT effectiveness was 32%, 41%, 20%, and 45% higher than sham ECT, placebo, tricyclic antidepressants (TCAs), and monoamine oxidase inhibitors (MAOIs), respectively (Janicak et al., 1985). ECT is generally reserved for patients who do not benefit from multiple trials of different medications (Weiss et al., 2019).
Australian and New Zealand clinical guidelines for the use of ECT (Weiss et al., 2019) are consistent with international consensus guidelines (Espinoza and Kellner, 2022; Pinna et al., 2018). They recommend that ECT is indicated as a first-line treatment for serious melancholic depression, high suicide risk, depression with psychotic or catatonic features, and patients with a previous response or specific preference. It is a second-line treatment for patients who are unresponsive to several levels of medications, including TCAs and MAOIs. ECT is also indicated as a treatment for bipolar disorder and schizophrenia (Weiss et al., 2019).
Studies from different countries have found considerable patient, health care provider or geographical variations of ECT use (Lecarpentier et al., 2022; Leiknes et al., 2012; Luccarelli et al., 2020; Ma et al., 2019). Some of this variation may be unwarranted, reaching beyond differences in individual patient needs or preferences due to the gap between evidence-based medicine and clinical practice (Buchan et al., 2016). Both clinical and non-clinical demographic patient characteristics are understood to contribute to ECT variation, including age, sex, race, socioeconomic, education, private health insurance status and geographic locale, such as urbanicity or rurality (Jørgensen et al., 2020; Kaster et al., 2021; Knight et al., 2018). Studies from the United States, Canada, Denmark and France have shown that ECT use is associated with increased age (Kaster et al., 2021; Lafrenière et al., 2023), being female (Luccarelli et al., 2020), higher income and education level (Kaster et al., 2021), diagnosis of major depressive disorder (MDD) (Slade et al., 2017), increased illness severity (Lecarpentier et al., 2022; Peltzman et al., 2020), increased prescriptions, service use and comorbidities (Peltzman et al., 2020; Wilkinson et al., 2018). A recent study found that ECT was used for a different patient cohort in China compared to the United States, with the receipt of ECT independently associated with being younger, employed, fewer previous hospitalisations and involuntary admissions, with the variation suggested to be attributable to associated agitated behaviour (Ma et al., 2019).
Current epidemiological literature on ECT utilisation in Australia has significant limitations. Existing studies have relied on small sample sizes drawn from individual hospitals or localised geographic areas (Das et al., 2019; Lee et al., 2020; Stormont et al., 2016). In addition, with data in prior studies ranging from 1998 to 2016 (Das et al., 2019; Doessel et al., 2006; Lee et al., 2020; Plakiotis et al., 2012; Stormont et al., 2016; Teh et al., 2005; Wood and Burgess, 2003), the generalisability and currency of findings become less relevant. This study aimed to determine the factors associated with receiving ECT, using linked administrative data on a state-wide scale in New South Wales (NSW), within the last decade.
Methods
Data sources
This study is a retrospective cohort analysis that utilised linked administrative inpatient, outpatient and mortality data from NSW, Australia. Information about psychiatric hospitalisations was obtained from the NSW Admitted Patient Data Collection (APDC), which documents all inpatient separations, including discharges, transfers and deaths, from both public and private hospitals in NSW. The APDC captures information on up to 50 procedures coded using the Australian Classification of Health Interventions (ACHI) and up to 51 diagnoses coded using the International Classification of Diseases, 10th Revision, Australian Modification (ICD-10-AM). Mortality data were obtained from the NSW Registry of Births, Deaths & Marriages (RBDM). Data related to psychiatric outpatient care were extracted from the NSW Mental Health Ambulatory Minimum Data Set (MH-AMB). The NSW Ministry of Health Centre for Health Record Linkage performed the data linkage and reports rates of false-positive and false-negative links of 0.5% (Centre for Health Record Linkage, 2023). Ethics approval was granted for this study by the NSW Population and Health Services Research Ethics Committee (2020/ETH02539/2020.84). A waiver of consent for the linkage of study participants’ data was granted by the NSW Population and Health Services Research Ethics Committee.
Study cohort
The cohort included all adult patients admitted with a primary diagnosis of a psychotic disorder or mood disorder (ICD-10-AM codes F20-F39) between July 2013 and February 2022, including unipolar and bipolar depression, schizophrenia and manic or psychotic symptoms. Exclusion criteria included (1) prior admission with a psychotic disorder or mood disorder (ICD-10-AM codes F20-F39) in any diagnosis field in a 1-year look-back period from index admission; (2) patients under 18 years of age at the time of index admission; (3) patients who had received prior ECT in the look-back period. The look-back period serves as a window of time used to define the study population under consideration. When eligibility criteria for an individual were met at multiple times throughout the study period, two unbiased choices for study entry are: (1) choosing a single eligible time, which could be the first, the last or a random eligible index admission; or (2) considering all eligible times (Hernán and Robins, 2016). In this study, we opted for choosing a random eligible index admission, since it represents a simple and patient-centric solution. Where multiple episodes of care comprised a single hospitalisation, all diagnosis codes, procedure codes and length-of-stay data were aggregated from these episodes, while the initial episode was retained to extract information for all other fields.
Two sensitivity analyses were conducted. The first sensitivity analysis extended the look-back period from 1 year to 3 years to assess its influence on the study outcomes. The second sensitivity analysis tested whether the factors associated with ECT varied following the cohort definition used in prior studies (Kaster et al., 2021; Knight et al., 2018) outside of Australia. The second sensitivity analysis modified our cohort definition by (1) adding an inclusion criterion of restricting hospital admissions to those with a length of stay of 3 days or more, as these patients would have had sufficient time for detailed clinical assessment of ECT suitability (Kaster et al., 2021) during that hospital admission, and (2) restricting follow-up to the index admission (Kaster et al., 2021; Knight et al., 2018).
Outcomes and covariates
The primary outcome was the first receipt of ECT (ACHI codes 14224-00–14224-06) during index admission and all available follow-up. Medical history and comorbidities were determined by examining diagnosis codes (primary and otherwise) in the index admission and prior admissions in the look-back period. Patient age and sex were obtained from the APDC record for the index admission. Diagnostic group variables included depression (ICD-10-AM: F32, F33), bipolar disorder (ICD-10-AM: F31), manic episode (ICD-10-AM: F30), schizophrenia and schizoaffective disorders (ICD-10-AM: F20, F25), schizophrenia-related disorders (schizotypal, delusional and other psychotic disorders, ICD-10-AM: F21-24, F28-29) and other mood disorders (ICD-10-AM: F34-39). We chose depression as the reference mental health diagnosis and included interaction terms accounting for patients with depression and any of the other psychotic or mood disorders to determine how depression in combination with other serious psychiatric conditions impacts receipt of ECT.
Rather than using all comorbidities from all available diagnosis codes in the cohort, we selected comorbidities based on the standardised Charlson Comorbidity Index (CCI) following prior work (Wilkinson et al., 2018). Substance abuse was identified through the Major Diagnostic Category (MDC) code 20 (Alcohol/Drug Use and Alcohol/Drug-Induced Organic Mental Disorders). Health service utilisation characteristics measured from the look-back period included the number of days in a psychiatric unit, emergency department visits and outpatient mental health visits (calculated from MH-AMB as service days where the patient was present). From the index admission, we included involuntary patient admission to a psychiatric unit and those with a diagnosis of depression who were involuntarily admitted.
Sociodemographic factors included year of index admission, marital status (married vs other), patient payment status and socioeconomic status (SES) of their area of residence. Australia operates a mixed public and private healthcare system. Patients were categorised as public or private patient according to their patient payment status, which was determined at the index admission. Patients affiliated with workers’ compensation, veteran affairs and defence force were classified as private patients. SES was measured using the Statistical Area Level 2 (Australian Statistical Geography Standard 2016 classification), corresponding to the patient’s local residential area, utilising the Australian Bureau of Statistics Index of Relative Socio-economic Advantage and Disadvantage (IRSAD) (Australian Bureau of Statistics, 2016). This index was stratified into quintiles, with the first quintile denoting the lowest relative SES, and the fifth quintile denoting the highest SES.
Statistical analysis
We constructed cause-specific Cox proportional hazard models to determine the risk factors associated with receiving ECT (dependent variable), with associations expressed as hazard ratios (HR) with 95% confidence intervals. The time to event of receiving ECT was determined by calculating the number of months from the discharge date of index admission until the earliest event among (1) the first occurrence of ECT (including those at index admission), (2) the end of the follow-up window (1 March 2022) and (3) death. The date of discharge was used as the date of ECT to ensure that patients who received ECT during index admission had non-zero event times.
Multiple multivariable models were used – the base model was limited to patient demographics such as age and sex, while the adjusted model incorporated all covariates. The second sensitivity analysis fitted multivariate logistic regression models to the outcome of receiving ECT during index admission in patients with a length of stay of at least 3 days. The models’ goodness-of-fit was evaluated using the concordance index (for the Cox models) and the area under the receiver operating characteristic curve (AUC, for the logistic regression model) with 10-fold cross-validation. Univariate hazard analysis using Nelson-Aalen was estimated using the entire dataset to calculate the cumulative probability of receiving ECT, and similarly for death.
Results
Baseline characteristics
Among 119,763 patients with at least one psychiatric admission between 2012 and 2022, 94,950 met our inclusion criteria after excluding those who met the exclusion criteria (Figure 1). In our cohort (Table 1), 91,485 (96.4%) patients did not receive ECT during follow-up, 6112 (6.6%) died before the end of follow-up and 3465 (3.6%) received ECT. Patients who died during follow-up were older (median 64.5; interquartile range [IQR] 48.2–79.4 years) and had more medical comorbidities (higher CCI score, median 3.0; IQR 1.0–4.0).
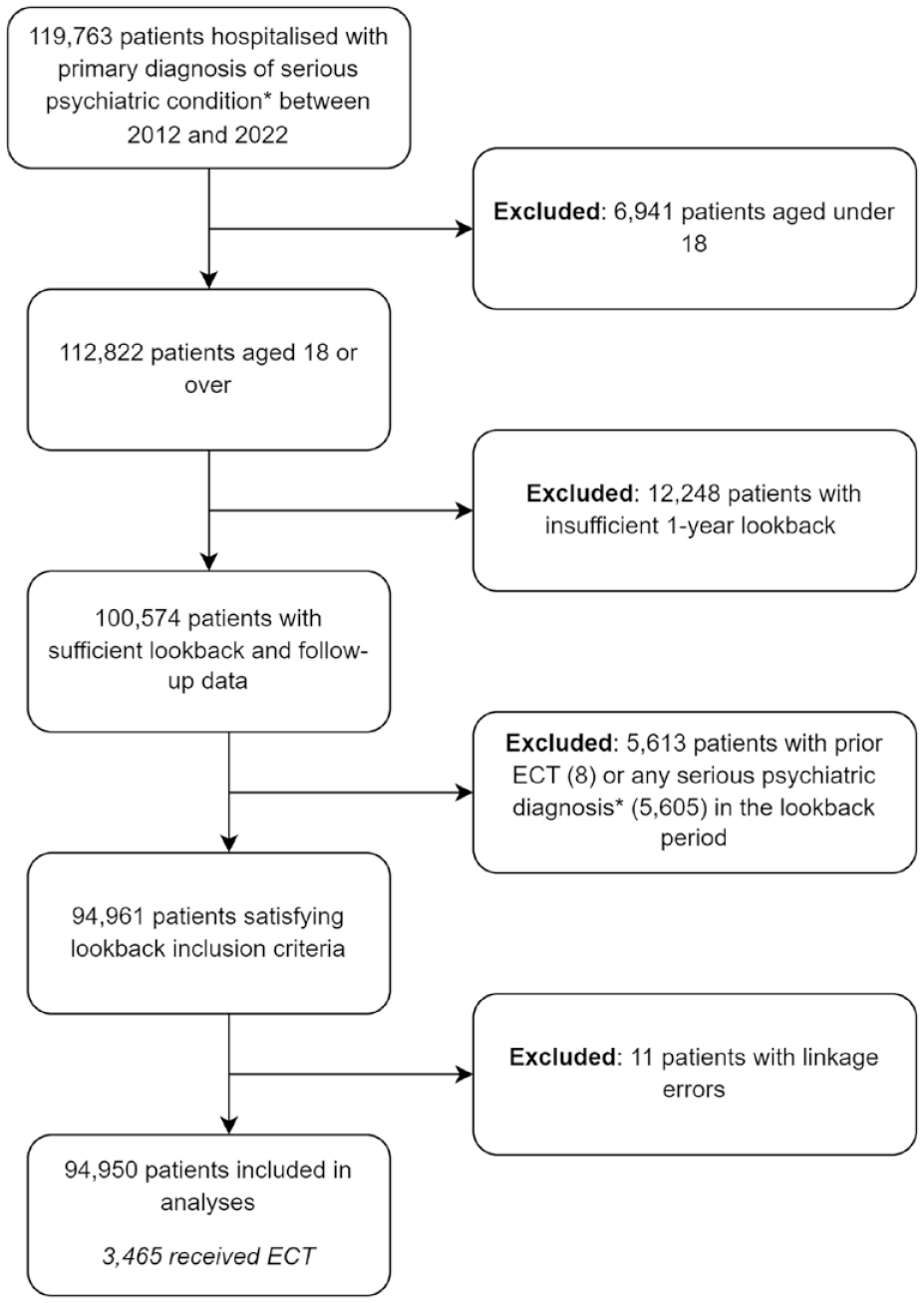
Flowchart of the selection of the 1-year look-back study population.
Summary of baseline characteristics of the 1-year look-back study population at the time of index psychiatric admission to a public or private hospital in New South Wales, Australia.
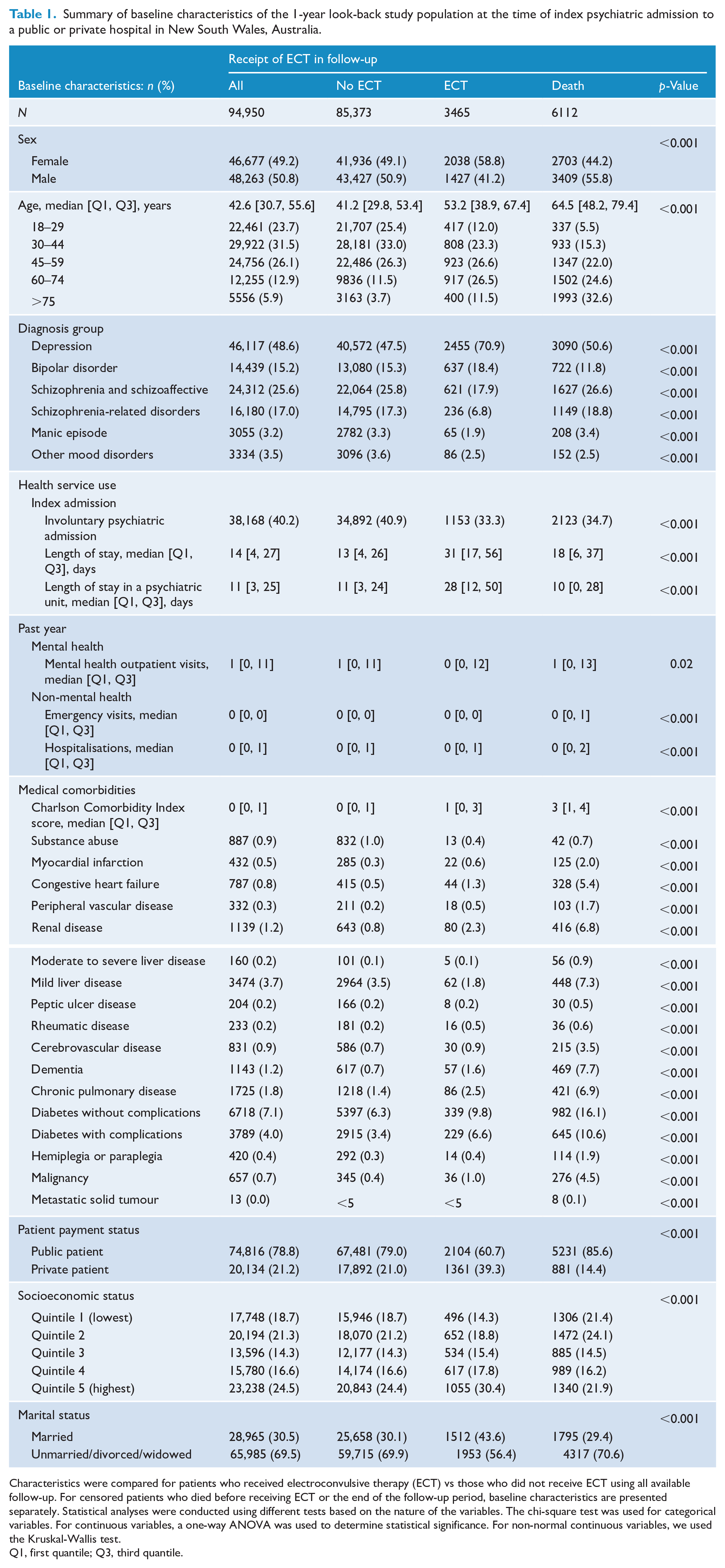
Characteristics were compared for patients who received electroconvulsive therapy (ECT) vs those who did not receive ECT using all available follow-up. For censored patients who died before receiving ECT or the end of the follow-up period, baseline characteristics are presented separately. Statistical analyses were conducted using different tests based on the nature of the variables. The chi-square test was used for categorical variables. For continuous variables, a one-way ANOVA was used to determine statistical significance. For non-normal continuous variables, we used the Kruskal-Wallis test.
Q1, first quantile; Q3, third quantile.
Patients who received ECT during follow-up had higher rates of depression (70.9% vs 47.5%) and bipolar disorder (18.4% vs 15.3%) and lower rates of schizophrenia and schizoaffective disorder (17.9% vs 25.8%), schizophrenia-related disorders (6.8% vs 17.3%), manic episodes (1.9% vs 3.3%) and other mood disorders (2.5% vs 3.6%). Patients receiving ECT had higher CCI scores (IQR 0-3 vs IQR 0-1) and lower rates of substance abuse diagnosis (0.4% vs 1.0%). Patients who received ECT were also more likely to have depression combined with other psychotic or mood disorders, including bipolar disorder, schizophrenia and schizoaffective disorder and other mood disorders (Supplemental Table 1).
Various indicators of service utilisation for mental health reasons showed higher service utilisation among ECT recipients: more days spent in a psychiatric unit during index admission (median 28 days, IQR 12–50 days vs median 11 days, IQR 3–24 days) and longer inpatient lengths of stay (median 31 days, IQR 17–56 days vs median 13 days, IQR 4–26 days). A smaller proportion of ECT patients were involuntarily admitted to a psychiatric unit at their index admission (33.3% vs 40.9%). Those diagnosed with depression and who had an involuntary psychiatric admission had significantly higher rates of ECT (17.9% vs 9.1%, Supplemental Table 2).
Patients who received ECT were older (median age 53.2, IQR 38.9–67.4) than those who did not receive ECT (median age 41.2, IQR 29.8–53.4) and were more likely to be female (58.8% vs 49.1%) and married (43.6% vs 30.1%). ECT patients were more often private patients in their index admission (39.3% vs 21.0%) and socioeconomically advantaged, with higher rates in the highest income quintile (30.4% vs no 24.4%) and lower rates in the lowest income quintile (14.3% vs no 18.7%). Rates of ECT were substantially greater among private patients with depression (32.8% vs 16%), bipolar disorder (7.1% vs 3.2%) and schizophrenia and schizoaffective disorder (1.7% vs 1%, Supplemental Table 3).
Factors associated with ECT
Our cohort had a median follow-up period of 4.04 years (IQR 1.96–6.28), with cumulative hazard rates of receiving ECT or dying shown in Figures 2 and 3. Older age was associated with an increased likelihood of receiving ECT (Table 2), with the likelihood increasing for each additional year of age (adjusted HR [aHR]= 1.03; 95% CI = [1.03, 1.03]). Females had an increased likelihood of receiving ECT (aHR = 1.24, 95% CI = [1.15, 1.32]). Relative to those with a diagnosis of depression at index admission, those with a diagnosis of schizophrenia and schizoaffective disorder (aHR = 0.79, 95% CI = [0.70, 0.89]), schizophrenia-related disorders (aHR = 0.37, 95% CI = [0.31, 0.44]), mania (aHR = 0.64, 95% CI = [0.49, 0.84]) and other mood disorders (aHR = 0.45, 95% CI = [0.33, 0.61]) had lower likelihood of receiving ECT. Patients with depression and at least one other serious psychiatric condition had higher likelihood of receiving ECT (aHR = 1.41, 95% CI = [1.25, 1.58]) than those who only had depression. Bipolar disorder was not associated with an increased or decreased likelihood of ECT compared to depression. Patients with depression and involuntary admission to a psychiatric unit during index admission were associated with a higher likelihood of receiving ECT, but an involuntary admission without a depression diagnosis did not increase odds of receiving ECT. A larger number of mental health outpatient visits in the previous year were associated to a higher likelihood of receiving ECT. A medical history of renal disease and complicated diabetes was associated with receiving ECT, while mild liver disease was associated with reduced likelihood of ECT.
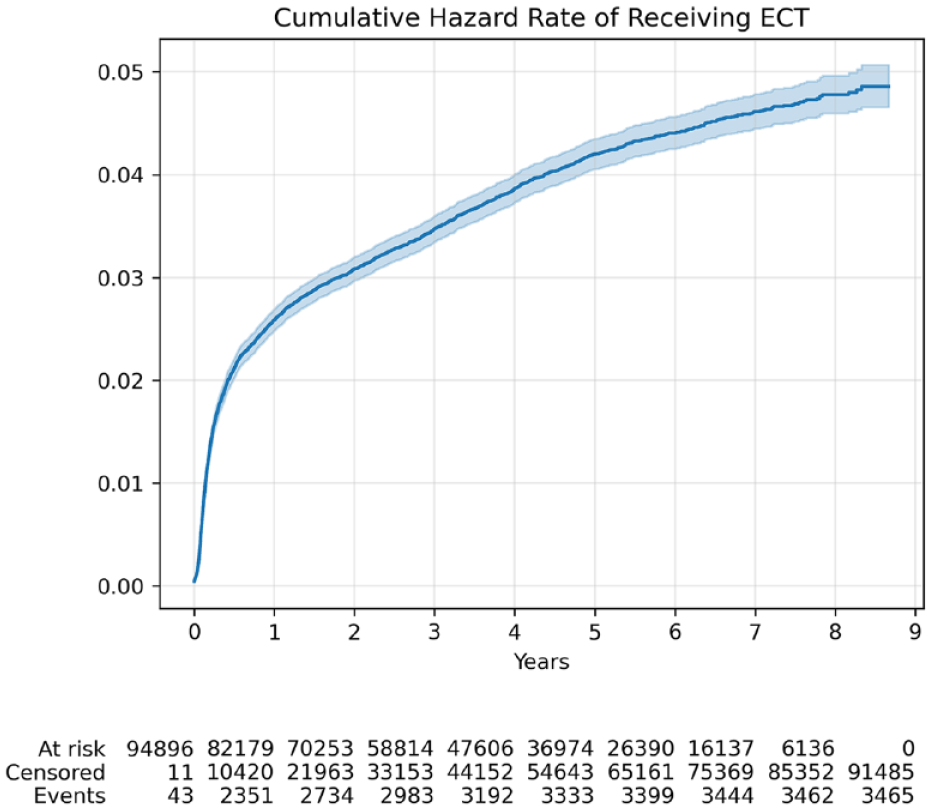
Nelson-Aalen hazard curve showing the cumulative hazard rate of receiving electroconvulsive therapy (ECT) after index psychiatric admission in the 1-year look-back study population. The likelihood of receiving ECT is highest in the first year after index admission.
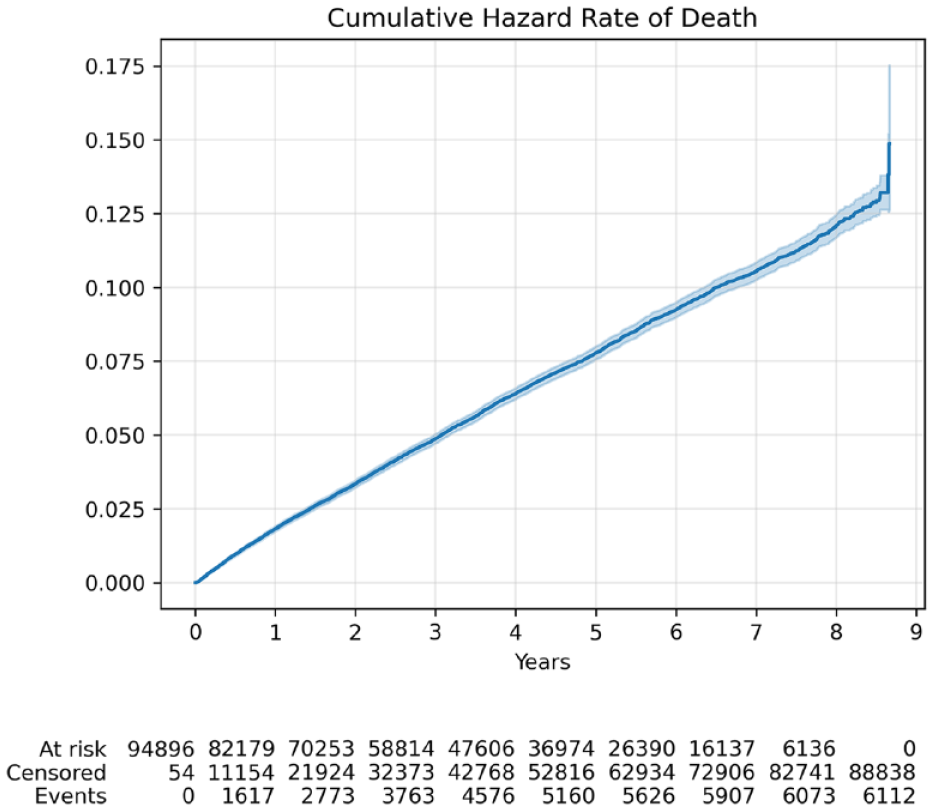
Nelson-Aalen hazard curve showing the cumulative hazard rate of death (censoring) occurring after index psychiatric admission in the 1-year look-back study population. The risk of death in the cohort was constant over the follow-up period.
Hazard ratios derived from Cox regression to determine risk factors associated with receiving ECT in the 1-year look-back study population.
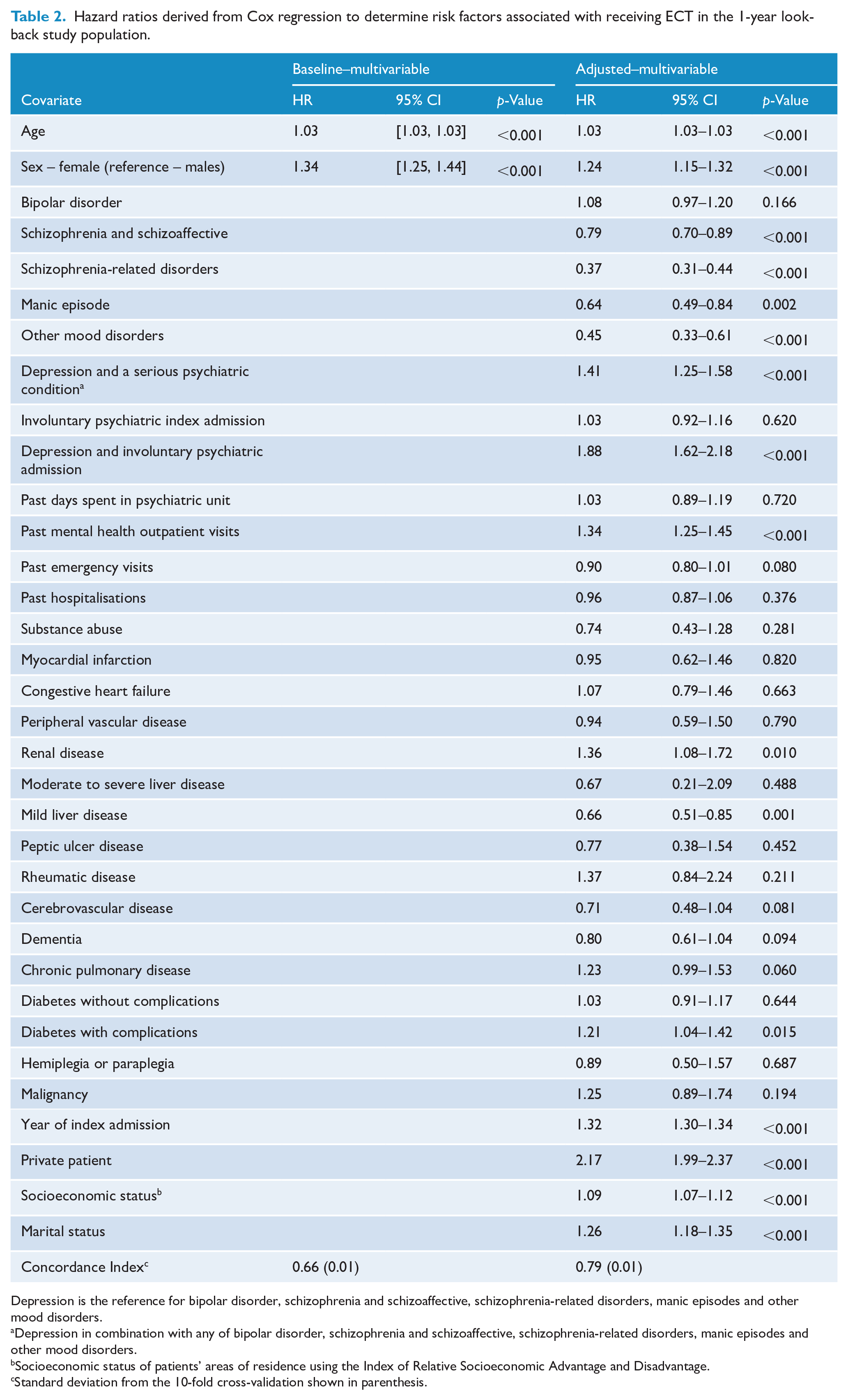
Depression is the reference for bipolar disorder, schizophrenia and schizoaffective, schizophrenia-related disorders, manic episodes and other mood disorders.
Depression in combination with any of bipolar disorder, schizophrenia and schizoaffective, schizophrenia-related disorders, manic episodes and other mood disorders.
Socioeconomic status of patients’ areas of residence using the Index of Relative Socioeconomic Advantage and Disadvantage.
Standard deviation from the 10-fold cross-validation shown in parenthesis.
The year of admission (advancing year) was associated with receiving ECT (aHR = 1.32, 95% CI = [1.30, 1.34]), with a breakdown of ECT per year in our cohort presented in Supplemental Table 4. All sociodemographic factors were linked to an increased likelihood of receiving ECT: private patient status, higher SES of the area of residence and being married.
Sensitivity analysis
Sensitivity analyses conducted on the cohort with a 3-year look-back period (Supplemental Tables 5 and 6) demonstrated similar associations in directionality and magnitude to those presented in Table 2 (1-year look-back period). Additional factors that reduced the likelihood of receiving ECT in the 3-year look-back period cohort included a higher number of emergency visits in the 3 years prior to index admission and a medical history of myocardial infarction and dementia.
Supplemental Table 4 presents the summary patient characteristics for the second sensitivity analysis with the cohort having a minimum length of stay of 3 days at the time of index psychiatric admission and follow-up limited to the index admission (see Supplemental Figure 3 for a flow diagram of inclusion/exclusion criteria). Compared to the main cohort (Table 1), patients with a length of stay of at least 3 days at the time of index admission were older (median age 57.7 vs median age 53.2), had higher rates of depression (77.0% vs 70.9%), lower rates of bipolar disorder (17.6% vs 18.4%) and other mood disorders (1.7% vs 2.5%). Patients with a length of stay of at least 3 days also had higher rates of involuntary psychiatric admissions and longer lengths of stay. They had similar rates of private patient status (38.1% vs 39.3%) but higher rates in the three highest income quintiles. The directionality of the associations (Supplemental Table 8) of factors with receiving ECT in patients with a length of stay of at least 3 days (Appendix Table 5) was consistent with the main results (Table 2). Additional factors that reduced the likelihood of receiving ECT during the index admission in patients with a length of stay of at least 3 days were bipolar disorder, past emergency visits and past hospitalisations. All sociodemographic factors (private patient status, SES and being married) were consistent with the main results in increasing the odds of receiving ECT.
Discussion
Main findings
In our study population of NSW psychiatric inpatients admitted for mood or psychotic disorders, 3.6% received ECT. As an intervention for psychiatric patients, ECT increased in NSW from 2013 to 2018, and then decreased from 2019 to 2021 (during the COVID-19 pandemic). Patients with schizophrenia and schizoaffective disorder, schizophrenia-related disorders, mania and other mood disorders had lower likelihood of receiving ECT than those with depression, consistent with a prior study (Jørgensen et al., 2020; Lecarpentier et al., 2022), with schizophrenia-related disorders having the lowest odds of all psychiatric conditions. Patients with depression and at least one other serious psychiatric condition had higher odds of receiving ECT than patients only with depression, consistent with prior work (Jørgensen et al., 2020). The effect of bipolar disorder was not statistically different from depression. These results suggest that ECT in NSW is being used for depression and bipolar disorder in accordance with established national clinical practice guidelines (Malhi et al., 2015; Weiss et al., 2019). ECT is being used in accordance with guidelines for patients who present with manic episodes, other mood disorders, schizophrenia and schizoaffective disorder (without depression) and schizophrenia-related disorders, though at lower rates than for depression. The strong association of private patient status with receiving ECT suggests the need to further investigate the variation in ECT supply or accessibility.
Clinical predictors
Recipients of ECT were more likely to be older and female, consistent with previous work in Australia (Teh et al., 2005; Wood and Burgess, 2003), Europe (Jørgensen et al., 2020; Lecarpentier et al., 2022; Schweder et al., 2011) and North America (Kaster et al., 2021; Knight et al., 2018; Lafrenière et al., 2023; Luccarelli et al., 2020; Slade et al., 2017; Wilkinson et al., 2018). Increasing age may be appropriately associated with ECT use, as the efficacy of ECT is greater in older adults (Spaans et al., 2015), with increased response rate and quality of life improvement, particularly for late-life depression in which ECT is safe and well-tolerated (Weiss et al., 2019). Stronger representation of the elderly may also be due in part to depression being more difficult to treat in this age group (Lemasson et al., 2018). However, the reasons for demographic differences in gender, although also found in multiple prior studies, are less clear. Although depression disproportionately affects women (Lemasson et al., 2018), we found that independent of psychiatric diagnoses, females received more ECT than males. This may reflect a gender bias where providers are more inclined to consider ECT an appropriate treatment option in female patients, or female patients may have increased awareness of or be more receptive to undergoing ECT treatment (Wood and Burgess, 2003).
ECT was associated with patients with a diagnosis of depression and involuntary psychiatric index admissions, which is likely a proxy for severe depression, which would appear to be in keeping with guideline recommendations of ECT treatment for more severe disease (Malhi et al., 2015; Weiss et al., 2019). This finding may also reflect clinicians’ perceptions of ECT utility in chronic, treatment-refractory illness. Other studies have supported similar findings of ECT being associated with greater psychiatric care utilisation (Kaster et al., 2021; Knight et al., 2018; Lafrenière et al., 2023; Wilkinson et al., 2018; Wilkinson and Rosenheck, 2017) and involuntary admission (Kaster et al., 2021).
Non-clinical predictors
Recipients of ECT were more likely to be married, private patients at their index admission and more socioeconomically advantaged. Being a publicly funded patient, unmarried and living in a socioeconomically disadvantaged area (lower IRSAD score) each independently reduced the odds of receiving ECT. The findings raise concerns over inequitable access to ECT in NSW, consistent with studies from the United States, Canada and Denmark (Case et al., 2013; Jørgensen et al., 2020; Kaster et al., 2021; Patel et al., 2019; Slade et al., 2017; Wilkinson et al., 2018). Patient insurance status represented the strongest non-diagnosis independent predictor in our analyses, in line with American studies (Case et al., 2013; Patel et al., 2019; Slade et al., 2017) and an Australian study (Teh et al., 2005) reporting academic and private hospitals as administering the majority of ECT treatments in WA – this trend is also consistent with American studies (Hermann et al., 1995; Patel et al., 2019). With declining availability of hospital mental health beds in Australia (Australian Medical Association [AMA], 2022), hospital financial pressures concerning the cost of inpatient psychiatric units (Allison et al., 2018; Degli Esposti et al., 2022) may provide a disincentive to offer ECT treatment for publicly funded patients. Furthermore, private patients in Australia enjoy greater access to elective procedures, including individual provider selection and shorter waiting times, potentially increasing their demand for ECT.
More socioeconomically advantaged patients with greater health literacy may exercise a higher demand for ECT due to greater understanding and acceptance of ECT and greater satisfaction following treatment (Goodman et al., 1999), while physicians may accede or face less barriers in prescribing to such patients (Hendryx et al., 2002). Concurrently, patients who are married or more advantaged may have greater enabling resources to effectively navigate the complexities of the healthcare system (Hendryx et al., 2002), with this conceptualisation enabling them to receive ECT treatment.
Limitations
Our study focused on ECT treatment for patients who were admitted to a hospital with psychotic or mood disorders (ICD-10-AM codes F20-F39), but future research should explore ECT utilisation across a broader range of psychiatric conditions and the general population in NSW. No direct conclusions on causality can be drawn from the estimates presented in our results, which should be interpreted as associations. Our survival analysis used cause-specific hazard models to simplify the interpretation of the analysis. By including all covariates in a single model in conducting risk analysis, confounding of effect estimates potentially occurred, whereby some variables estimate the total effect, while other effect estimates may be complicated by mediating features estimating the direct effect (Westreich and Greenland, 2013).
Constraints pertaining to data availability inevitably resulted in the omission of various factors that may affect ECT use in our analyses. Unmeasured but possibly significant characteristics include provider training and attitudes and patient-specific features such as medication data, history of pharmacological psychiatric treatment failure and illness severity. No ECT parameters were available, such as the electrode electric charge, placement and dosing schedules.
Conclusion
ECT use in NSW follows clinical guidelines for diagnosis of depression and bipolar disorder. Diagnoses of mania, schizophrenia, schizoaffective, schizophrenia-related disorders and other mood disorders decreased odds of receiving ECT compared to depression, despite being supported by RANZCP guidelines. Non-clinical predictors revealed socioeconomic disparities, particularly in ECT receipt between public and private patients. Further research to identify mechanisms and interventions for addressing these disparities are required to ensure equitable access to ECT.
Supplemental Material
sj-docx-1-anp-10.1177_00048674241266067 – Supplemental material for Factors associated with electroconvulsive therapy treatment for adults with serious psychiatric conditions in Australia
Supplemental material, sj-docx-1-anp-10.1177_00048674241266067 for Factors associated with electroconvulsive therapy treatment for adults with serious psychiatric conditions in Australia by Timothy Chen, Colleen Loo, Luis Salvador-Carulla, Louisa R Jorm, Preeyaporn Srasuebkul, Grant Sara, Juan C Quiroz and Blanca Gallego in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors wish to thank the NSW Centre for Health Record Linkage (CHeReL) for linking the datasets: NSW Admitted Patients Data Collection and the NSW Registry of Births, Deaths & Marriages; the NSW Ministry of Health for providing access to population health data and Malcolm Gillies and Mark Hanly for feedback on the statistical analysis.
Author Contributions
All authors contributed to the conception and design of the study. TC performed the data analysis and wrote the first draft. All authors contributed to critical revisions of the manuscript. All authors approved the final draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Health and Medical Research Council (NHMRC), project grant No. APP1184304. CL is supported by a National Health and Medical Research Council (NHMRC) Investigator Grant No.1195651.
Data Availability Statement
The datasets for this study were obtained from the NSW Centre for Health Record Linkage (CHeReL). The datasets cannot be publicly shared due to ethical, governance and confidentiality agreements.
Supplemental Material
Supplemental material for this article is available online.