
Abstract
Objective:
Acute course of electroconvulsive therapy is effective in inducing remission from depression, but recurrence rate is unacceptably high following termination of electroconvulsive therapy despite continued pharmacotherapy. Continuation electroconvulsive therapy and maintenance electroconvulsive therapy have been studied for their efficacy in preventing relapse and recurrence of depression. The purpose of this meta-analysis was to examine the efficacy of continuation electroconvulsive therapy and maintenance electroconvulsive therapy in preventing relapse and recurrence of depression in comparison to antidepressant pharmacotherapy alone.
Methods:
We searched MEDLINE, Embase, PsycINFO, clinicaltrials.gov and Cochrane register of controlled trials from the database inception to December 2016 without restriction on language or publication status for randomized trials of continuation electroconvulsive therapy and maintenance electroconvulsive therapy. Two independent Cochrane reviewers extracted the data in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines for systematic reviews and meta-analyses. The risk of bias was assessed using four domains of the Cochrane Collaboration Risk of Bias Tool. Outcomes were pooled using random effect model. The primary outcome was relapse or recurrence of depression.
Results:
Five studies involving 436 patients were included in the meta-analysis. Analysis of the pooled data showed that continuation electroconvulsive therapy and maintenance electroconvulsive therapy, both with pharmacotherapy, were associated with significantly fewer relapses and recurrences than pharmacotherapy alone at 6 months and 1 year after a successful acute course of electroconvulsive therapy (risk ratio = 0.64, 95% confidence interval = [0.41, 0.98], p = 0.04, risk ratio = 0.46, 95% confidence interval = [0.21, 0.98], p = 0.05, respectively). There was insufficient data to perform a meta-analysis of stand-alone continuation electroconvulsive therapy or maintenance electroconvulsive therapy beyond 1 year.
Conclusion:
There are only a few randomized trials of continuation electroconvulsive therapy and maintenance electroconvulsive therapy. The preliminary and limited evidence suggests the modest efficacy of continuation electroconvulsive therapy and maintenance electroconvulsive therapy with concomitant pharmacotherapy in preventing relapse and recurrence of depressive episodes for 1 year after the remission of index episode with the acute course of electroconvulsive therapy.
Keywords
Introduction
Depressive disorders often recur with substantial morbidity and mortality (Frank et al., 1990; Keller et al., 1983; Kessler and Walters, 1998; Maj et al., 1992; Roy-Byrne et al., 1985). In fact, longitudinal follow-up over 15 years has shown an 85% cumulative recurrence rate in major depressive disorder (Mueller et al., 1999). Electroconvulsive therapy (ECT) is the most effective form of treatment to induce remission from depression (Pagnin et al., 2004; UK ECT Review Group, 2003), but 40%–60% of patients suffer from relapse or recurrence of depression even with continued antidepressant therapy in the year following termination of acute course of ECT (Jelovac et al., 2013; Rasmussen et al., 2009; Sackeim et al., 2001).
The continuation electroconvulsive therapy (c-ECT) refers to continued treatment for the next 6 months beyond remission from major depression, whereas maintenance electroconvulsive therapy (m-ECT) denotes treatment that is continued beyond those 6 months (American Psychiatric Association (APA), 2000a). The aim of c-ECT is to prevent relapse and that of m-ECT is to avert recurrence. The c-ECT was a practice that emerged soon after the introduction of ECT. With the arrival of pharmacotherapy its use faded, but re-emerged in 1980s, and has become a focus of ECT research more recently. Randomized controlled trials, non-randomized prospective studies, retrospective studies and several case reports have suggested that c-ECT and m-ECT have been well tolerated and effective in preventing relapse and recurrence (Brown et al., 2014; Rabheru, 2012). Duration of reported m-ECT varied from 6 months up to 12 years (Brown et al., 2014; Elias et al., 2014; Rabheru, 2012). The APA (2000a) and Royal Australian and New Zealand College of Psychiatrists (2014) recommend m-ECT for selected patients with recurrent depressive disorder, but other guidelines differ in recommendations. For example, National Institute for Health and Care Excellence (NICE, 2003) guideline does not recommend continued ECT due to lack of controlled trial evidence for efficacy. With the knowledge of relapse and recurrence of depression after a successful course of acute ECT, researchers have investigated the usefulness of continued ECT over the past few decades. Systematic reviews (Brown et al., 2014) support the view that m-ECT has a distinct role in the management of mood disorder, but some randomized trials provided inconsistent results. After the latest systematic review appeared more than a year ago, another randomized controlled trial of c-ECT was published recently (Kellner et al., 2016). Moreover, a meta-analysis of randomized trials of c-ECT and m-ECT has not been reported. In this paper, we report the first meta-analyses of randomized trials of c-ECT and m-ECT in depressive disorders.
Methods
Search strategies
We collected the data for this review with a protocol in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Figure 1). The search covered the MEDLINE database through PubMed, Embase, PsycINFO, clinical trials registered with clinicaltrials.gov and Cochrane Register of controlled trials. We initially searched the database using the key words ‘electroconvulsive therapy’ ‘depressive disorder’ in order not to miss the studies that did not use the key words ‘continuation’ or ‘maintenance’ ‘electroconvulsive therapy’. We repeated the search with ‘continuation electroconvulsive therapy’ ‘depressive disorder’ and ‘maintenance electroconvulsive therapy’ ‘depressive disorder’. The filters included human studies, clinical trials, date up to 31 December 2016 and the age above 18 years. There was no restriction on language or publication bias applied to searches. Two reviewers (A.E. and V.H.P.) independently searched and extracted the data. Both reviewers had previous experience of completing meta-analysis with Cochrane. We resolved disagreements through discussion and when required we consulted the statistician (S.C.) and senior author (J.P.). We contacted trial authors for incomplete data.
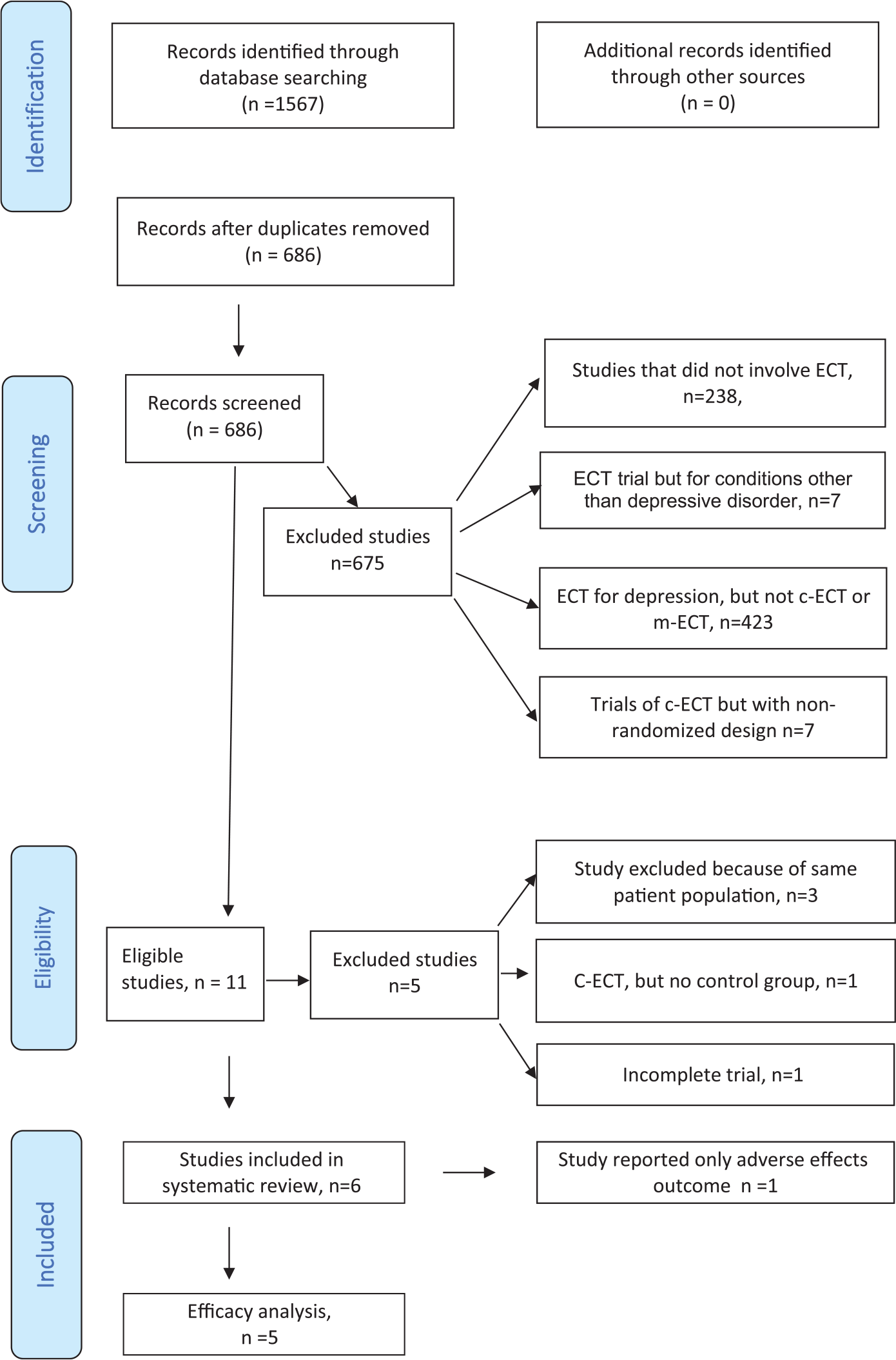
PRISMA flow diagram.
Eligibility criteria
The inclusion criteria were as follows: (1) randomized controlled trials, (2) age group 18 years and older, (3) major depressive disorder, (4) remission or response following acute ECT, (5) continuation of ECT for duration of 6 months or more. Both unipolar and bipolar depressions were included. Continuation ECT administered for schizophrenia and schizoaffective disorder were excluded. Diagnostic criteria according to International Classification of Diseases, tenth edition (ICD-10); Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV); Diagnostic and Statistical Manual of Mental Disorders, the text revision of DSM-IV (DSM-IV-TR); and Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-V) were accepted for the diagnosis of depression (APA, 2000b, 2013; World Health Organization, 1992). Continuation or maintenance ECT with or without antidepressant therapy was the experimental intervention studied against the comparator intervention of post-ECT continuation pharmacological antidepressant therapy alone. Trials with intention-to-treat (ITT) analysis were included, and the primary analysis was restricted to ITT studies, the preferred method to reduce bias. Trials with no summary data were not included in the meta-analyses.
Outcomes measured
The efficacy outcomes used were recurrence or relapse of a depressive episode as defined by the ICD-10, DSM-IV, DSM-IV-TR or DSM 5 diagnostic criteria or a depression rating scale, admission to a hospital because of a depressive episode or dropout from the study because of recurrence or relapse. The adverse events outcomes included adverse cognitive function as measured by Mini-Mental State Examination (MMSE) or any other validated tool to measure cognitive side effects; cardiovascular complications (hypertension, hypotension, arrhythmias, asystole); complications related to anaesthesia (e.g. prolonged apnoea); and other adverse reactions related to ECT (headache, muscular and joint pain, generalised body ache, delirium, post-ictal agitation and prolonged seizure). Mortality arising from a cause directly attributable to ECT or anaesthesia for ECT was also included under adverse outcomes. Acceptability to patients was evaluated by dropout rate.
Assessment of risk of bias
We assessed the risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins and Green, 2008). We estimated the risk of bias according to the following domains: whether randomization was adequate; whether the allocation sequence was concealed until participants were assigned to their groups; whether knowledge of the allocated treatment was adequately masked for patients, clinicians, assessors of the outcome and statisticians during the study; whether there were incomplete data; and whether there was any selective reporting of outcomes. We judged each potential source of bias as high, low or unclear. Trials are given weightage in proportion to the level of bias. Cochrane Review Manager 5 (RevMan 5) software was used to perform the analysis.
Data analysis and assessment of heterogeneity
The primary analysis, based on the proportion of patients in both groups who experienced relapse or recurrence during the study period, calculated the risk ratio (RR) to evaluate the difference in effect size between the treatment groups. The data were pooled according to the weighted averages. We assessed heterogeneity using a p value; this was read in conjunction with visual inspection of forest plot and I2 value. The studies on m-ECT were conducted by researchers working independently, with different populations of patients and methodologies varying in terms of frequency of the intervention (e.g. fortnightly m-ECT against monthly m-ECT), electrode placement and pulse width. For these reasons, a common effect size could not be assumed and a random effects meta-analysis was performed. Asymmetry of the funnel plot was used to judge the reporting bias.
Results
Selection of studies
The search identified 1567 abstracts. Further results are shown in the PRISMA flow diagram (Figure 1). There were 11 trials that met all inclusion criteria, five of which were excluded because one was incomplete (Sarachaga, 2015); one studied c-ECT, but there was no control group without c-ECT (Yildiz et al., 2010); and three involved the data from the same patient population from which complete trials were published (Bajbouj, 2015; Rasmussen et al., 2007; Serra et al., 2006). The complete trials were included in the analysis. Of the remaining six studies found to be eligible for meta-analysis, only five studies were included in the efficacy analysis because one study exclusively reported cognitive outcome and was from the same patient population from which efficacy results and cognitive outcomes were reported (Smith et al., 2010).
Characteristics of included studies
There were five trials involving 436 patients (Brakemeier et al., 2014; Kellner et al., 2006, 2016; Navarro et al., 2008; Nordenskjöld et al., 2013). The duration of m-ECT varied among the studies from 6 months to 2 years. Three studies reported 6-month outcomes (Brakemeier et al., 2014; Kellner et al., 2006, 2016) and one trial reported 1-year outcomes (Nordenskjöld et al., 2013). There was only one 2-year trial (Navarro et al., 2008). The authors of the latter two studies provided 6-month data upon request. Two studies included only elderly patients (Kellner et al., 2016; Navarro et al., 2008), and the others had patients at least 18 years of age. The largest trial ran for six months, and it compared c-ECT as monotherapy against antidepressant therapy, nortriptyline, and lithium (Kellner et al., 2006). All other studies compared c-ECT or m-ECT with concomitant pharmacotherapy against pharmacotherapy alone. All studies suffered from lack of participant blinding, but reported that assessors were blind to the treatment status. The procedures that are indicative of concealment of allocation were adequately described in one study (Nordenskjöld et al., 2013). All studies used ITT analysis; one study used modified ITT because of post-randomization dropout (Kellner et al., 2006).
Efficacy outcomes
Continuation ECT compared to continuation pharmacotherapy
There was only one study that compared c-ECT as monotherapy against pharmacotherapy, nortriptyline and lithium (Kellner et al., 2006); all others compared c-ECT along with pharmacotherapy against pharmacotherapy alone (Brakemeier et al., 2014; Kellner et al., 2016; Navarro et al., 2008; Nordenskjöld et al., 2013). In the study that compared the c-ECT as a monotherapy against pharmacotherapy (n = 184), 184 subjects were randomized into c-ECT (n = 89) or continuation pharmacotherapy (n = 95) on a modified ITT basis following post-randomization dropout of 17 patients. A total of 33 (37.5%) subjects relapsed with c-ECT and 30 (31.6%) relapsed on c-pharmacotherapy; there was no significant difference between the two groups regarding relapse or dropout rates even after adjusting for variables, namely, age, gender and psychosis status (hazard ratio: 1.1; 95% confidence interval [CI = 0.7, 1.9]; p = 0.63). However, the relapse rate in both groups was significantly lower than that of a historical placebo group (84%) (Sackeim et al., 2001). The samples represented severe depression resistant to first-line treatments. The c-ECT followed a strict schedule rather than a flexible model. We did an exploratory analysis of pooled data from all c-ECT trials regardless of whether c-ECT was accompanied by c-pharmacotherapy or not. Meta-analysis with random effects did not show any significant difference between the two treatment conditions, c-ECT or m-ECT, with and without pharmacotherapy and pharmacotherapy alone (RR = 0.84, 95% CI = [0.59, 1.19], p = 0.30) with minimal heterogeneity (χ2 = 4.85, I2 = 17%, p = 0.3) (Figure 2). Sensitivity analysis using fixed effects model did not change the results significantly (RR = 0.87, 95% CI = [0.65, 1.16], p = 0.35). Since we did not find a significant difference between the c-ECT with or without pharmacotherapy against pharmacotherapy alone, we performed a subgroup analysis c-ECT with pharmacotherapy against pharmacotherapy alone.

Forest plot: 6-month outcomes of continuation ECT with and without pharmacotherapy vs pharmacotherapy alone.
Continuation ECT with pharmacotherapy against pharmacotherapy alone: 6-month outcomes
Four trials reported data of c-ECT and c-pharmacotherapy against c-pharmacotherapy alone for 269 patients (Brakemeier et al., 2014; Kellner et al., 2016; Navarro et al., 2008; Nordenskjöld et al., 2013). One study had three arms: c-ECT and c-pharmacotherapy, c-pharmacotherapy and cognitive behavioural psychotherapy (CBT) and c-pharmacotherapy alone (Brakemeier et al., 2014). The cognitive behavioural arm was excluded for the purposes of this meta-analysis. Across the four trials, 252 patients who remitted with or responded to acute ECT were randomized to c-ECT + pharmacotherapy (n = 122) or c-pharmacotherapy (n = 106). One trial randomized responders rather than remitters (Brakemeier et al., 2014). Response was defined as 50% decrease in depression rating score. This study defined sustained response rate as the primary outcome, and it was calculated by eliminating those who relapsed and dropped out from the original ITT samples. The pooled analysis of subjects from all four trials favoured c-ECT + c-pharmacotherapy over c-pharmacotherapy alone in preventing relapse in the 6 months following response/remission after an acute course of ECT (RR = 0.64, 95% CI = [0.41, 0.98], p = 0.04) (Figure 3). Heterogeneity was insignificant (χ2 = 0.67, I2 = 0, p = 0.88). We performed a sensitivity analysis with three studies (Kellner et al., 2016; Navarro et al., 2008; Nordenskjöld et al., 2013) that recruited patients with the criterion of remission rather than response following acute ECT. The results were stronger than combining response with remission and in favour of c-ECT (RR = 0.57, 95% CI = [0.34, 0.96], p = 0.03).

The 6-month outcomes of continuation ECT plus pharmacotherapy vs pharmacotherapy alone.
Maintenance ECT with pharmacotherapy against pharmacotherapy alone: 1-year outcomes
A total of 89 subjects were randomized to m-ECT and pharmacotherapy (n = 44) versus pharmacotherapy alone (n = 45) (Navarro et al., 2008; Nordenskjöld et al., 2013). One trial did not report analysis of 1-year data, but the authors supplied the raw data for the 1-year observation, and it was entered in the meta-analysis. Meta-analysis showed superior efficacy of m-ECT along with pharmacotherapy over pharmacotherapy alone (risk ratio = 0.46, 95% confidence interval = [0.21, 0.98], p = 0.05, respectively) (Figure 3). Heterogeneity was present although insignificant (χ2 = 1.14, I2 = 17, p = 0.29) and sensitivity analysis with fixed effect model showed significance difference favouring m-ECT + pharmacotherapy over pharmacotherapy alone (RR = 0.44, CI = [0.24, 0.80], p = 0.007).

The 6-month outcomes of continuation ultrabrief ECT plus pharmacotherapy vs pharmacotherapy alone.
Maintenance ECT with pharmacotherapy against pharmacotherapy alone: 2-year outcome
Only one study extended to 2 years of m-ECT (Navarro et al., 2008). It was bifrontotemporal electrode placement for both acute and continuation course. The continuation regimen started as weekly treatment for the first month, fortnightly for the following month and then monthly. This study showed significantly lower relapse rate in m-ECT + c-pharmacotherapy arm compared to c-pharmacotherapy alone (nortriptyline with a maximum dose of 100 mg; hazard ratio = 8.12, CI = [1.5, 44.7], p = 0.009). Given that there were no similar studies, meta-analysis was not performed for 2-year data.
Ultrabrief ECT
Three trials that used ultrabrief ECT were pooled separately (Brakemeier et al., 2014; Kellner et al., 2016; Nordenskjöld et al., 2013). Across the three studies, 114 patients were randomized to c-ECT + c-pharmacotherapy group and 105 patients were allocated to c-pharmacotherapy (Figure 4). The frequency of c-ECT varied: in one study, treatment was administered weekly for 6 weeks followed by fortnightly for 46 weeks (Nordenskjöld et al., 2013); second study involved treatment weekly for 4 weeks, fortnightly for 8 weeks and then monthly for 3 months (Brakemeier et al., 2014); and the third study followed flexible Symptom-Treated Algorithm-Based Longitudinal ECT (STABLE) algorithm. The results were inconsistent across the three studies; two of them supported c-ECT while one favoured c-pharmacotherapy + CBT. In the pooled analysis, the superior efficacy of c-ECT + c-pharmacotherapy remained with ultrabrief treatment (RR = 0.64, CI = [0.41, 0.99], p = 0.05, heterogeneity p = 0.44, I2 = 0%).
Completers’ analysis
A sensitivity analysis was performed with completers’ data. The data for completers were available from the three studies that reported 6-month outcomes for c-ECT (Brakemeier et al., 2014; Navarro et al., 2008; Nordenskjöld et al., 2013). Analysis with random effect model showed significantly better outcome with c-ECT + pharmacotherapy compared to pharmacotherapy alone (RR = 0.61, CI = [0.38, 0.96], p = 0.03, heterogeneity p = 0.49, I2 = 0%).
Adverse effects
Cognitive functions
None of the studies reported any significant difference in measured cognitive functions among the treatment groups. MMSE was the most consistently used cognitive measure. Brakemeier et al. did not use MMSE; instead they used neuropsychological tests to assess cognitive functions. Original MMSE data were available from four studies for 6-month outcomes (Kellner et al., 2006, 2016; Navarro et al., 2008; Nordenskjöld et al., 2013). The pooled data from studies that compared continuation ECT with pharmacotherapy against pharmacotherapy alone did not show a significant difference in the MMSE score at the conclusion of trials (mean difference: 0.31, CI = [–0.17, 0.78], p = 0.21). Heterogeneity among the studies was insignificant (p = 0.81, I2 = 0%).
Other side effects
Patient acceptance of continuation therapies, as reflected in dropout rates, was not significantly different among the treatment groups (RR = 1.28, CI = [0.17, 6.67], p = 0.62). Navarro et al. (2008) used Udvalg for Kliniske Undersøgelse (UKU) side effects scale, blood pressure monitoring and electrocardiography (ECG) and found no difference in QTc interval or heart rate between the combination (m-ECT and nortriptyline) treatment group and nortriptyline alone group. The authors found that both m-ECT and nortriptyline were well tolerated, and adverse effects were mild to moderate. The side effects reported included headache and memory loss in two patients and myocarditis in one patient receiving c-ECT. In the pharmacotherapy group, dry mouth (27.4%), tremor (17.9%), drowsiness and fatigue (14.7%), and constipation (13.7%) were reported in patients taking nortriptyline and lithium. In another study, three patients (11%) on the pharmacotherapy attempted suicide with lithium and were admitted with lithium intoxication (Nordenskjöld et al., 2013). Kellner et al. (2016) reported suicidal ideations in three patients (5%) in the medication plus ECT group.
Publication bias
We did not examine a funnel plot because of small number of studies. Examination of funnel asymmetry is recommended only if there are at least 10 studies and visual inspection of the plot can be misleading (Higgins and Green, 2008).
Discussion
Methodological issues
This review has identified small number of randomized trials with designs that varied in terms of inclusion criteria – age group; interventions, including electrode placement; duration of trials – and tools used to measure outcomes. None of the trials had participant blinding to intervention assignment. Considering previously established evidence of the efficacy of ECT from sham vs real ECT studies and the risks associated with anaesthesia, participant blinding is not usually expected in ECT trials (Pagnin et al., 2004; UK ECT Review Group, 2003). The blinding of assessors was maintained in all trials. Concealment of allocation is a method where the sequence of random allocation of groups is not disclosed to either participants or those involved in recruiting participants until randomization is completed. For an ECT trial, it is important that participants are randomized after they have completed baseline assessments and provided informed consent in order to avoid post-randomization dropout once patients know their treatment assignment, especially where there is no blinding. This is crucial in preventing selection bias. Allocation concealment was adequately described in only one study (Nordenskjöld et al., 2013). All trials used ITT analysis, and three of them reported missing data and the number of completers.
Efficacy
The summary measures indicate that c-ECT and m-ECT trials along with continued pharmacotherapy showed better efficacy than pharmacotherapy alone in preventing relapse and recurrence at 6 months and 1 year after termination of acute ECT. There was only one study that compared c-ECT alone to c-pharmacotherapy, and this study failed to demonstrate a difference between the two groups (Kellner et al., 2006). One reason for the lack of better efficacy of stand-alone c-ECT over c-pharmacotherapy may be lack of flexibility of c-ECT schedule. For example, the Prolonged Remission in Depressed Elderly (PRIDE) study used a specific algorithm, STABLE, to determine the frequency of supplemental c-ECT and found superior efficacy of c-ECT + c-pharmacotherapy over c-pharmacotherapy alone (Kellner et al., 2016). This suggests that ongoing clinical evaluation and optimization of c-ECT frequency may be crucial in maintaining remission. Second, trials that showed superior efficacy of c-ECT and m-ECT over c-pharmacotherapy alone featured ECT combined with pharmacotherapy as the comparison treatment, not convulsive therapy alone. This implies a possible synergistic role for ECT and psychotropic medications in the maintenance treatment of depression. The best data have come from combination of nortriptyline and lithium or venlafaxine and lithium. Whether m-ECT alone, perhaps using a flexible schedule of treatment, would be able to prevent relapse or recurrence remains to be investigated. There were only two trials that completed 1 year of m-ECT. Both showed superior efficacy of m-ECT + pharmacotherapy compared to pharmacotherapy alone. One of these studies administered m-ECT for 2 years showing significantly better outcome with m-ECT, but there were no similar studies to pool the data for a meta-analysis. Ultrabrief ECT has become the focus of recent research, and its role in the treatment of acute symptoms has been well studied and debated (Tor et al., 2015). Subgroup analysis with ultrabrief ECT showed that for continuation and maintenance treatments, this mode of treatment was efficacious (RR = 0.64, CI = [0.41, 0.99], p = 0.05, heterogeneity p = 0.44, I2 = 0%).
The frequency and the dose of continuation and maintenance ECT varied from study to study and within the study (Brakemeier et al., 2014; Kellner et al., 2006, 2016; Navarro et al., 2008; Nordenskjöld et al., 2013). The gradual transition from acute course of ECT to continuation phase can be challenging as patients may show early signs of relapse. The studies included in this meta-analysis mostly used a treatment algorithm of weekly ECT for a month, then fortnightly ECT for a month or more, followed by monthly ECT in some instances (Table 1). The schedule for c-ECT and m-ECT has been derived from both theoretical propositions and evidence derived from other studies. For example, increased seizure threshold, one of the proposed therapeutic mechanisms of ECT, returns to baseline in months following termination of ECT (Sackeim, 1999). Studies of seizure duration in m-ECT did not show progressive lengthening of seizure in responders (Jarvis et al., 1993), but demonstrated prolongation in non-responders (Di Pauli and Conca, 2009). These findings are replicated by another study that observed seizure prolongation with loss of efficacy when the interval between treatments exceeded 2 months (Wild et al., 2004). In a separate line of evidence, a non-randomized prospective trial demonstrated that patients with bipolar disorder continued to remain in remission with bimonthly maintenance ECT (Minnai et al., 2011). As noted earlier, the majority of randomized trials included in this meta-analysis used monthly ECT. Combining the data from randomized trials included in this meta-analysis, non-randomized prospective trials and retrospective studies, it appears that 1- to 2- month interval may be optimal for m-ECT. As far as electrical stimulus dosing is concerned, the dose may be determined at the commencement of c-ECT by re-titration, and the same dose may be continued as long as patients maintain clinical remission. Some authors recommend re-titration if the interval exceeds 2 months (Wild et al., 2004). Kellner et al. (2016) developed the STABLE algorithm, a flexible regimen with demonstrated efficacy in remitted geriatric patients for the first 6 months after ECT. This highlights the importance of psychiatrists’ knowledge of their individual patients and supplemental ECT as indicated.
Characteristics of included studies.
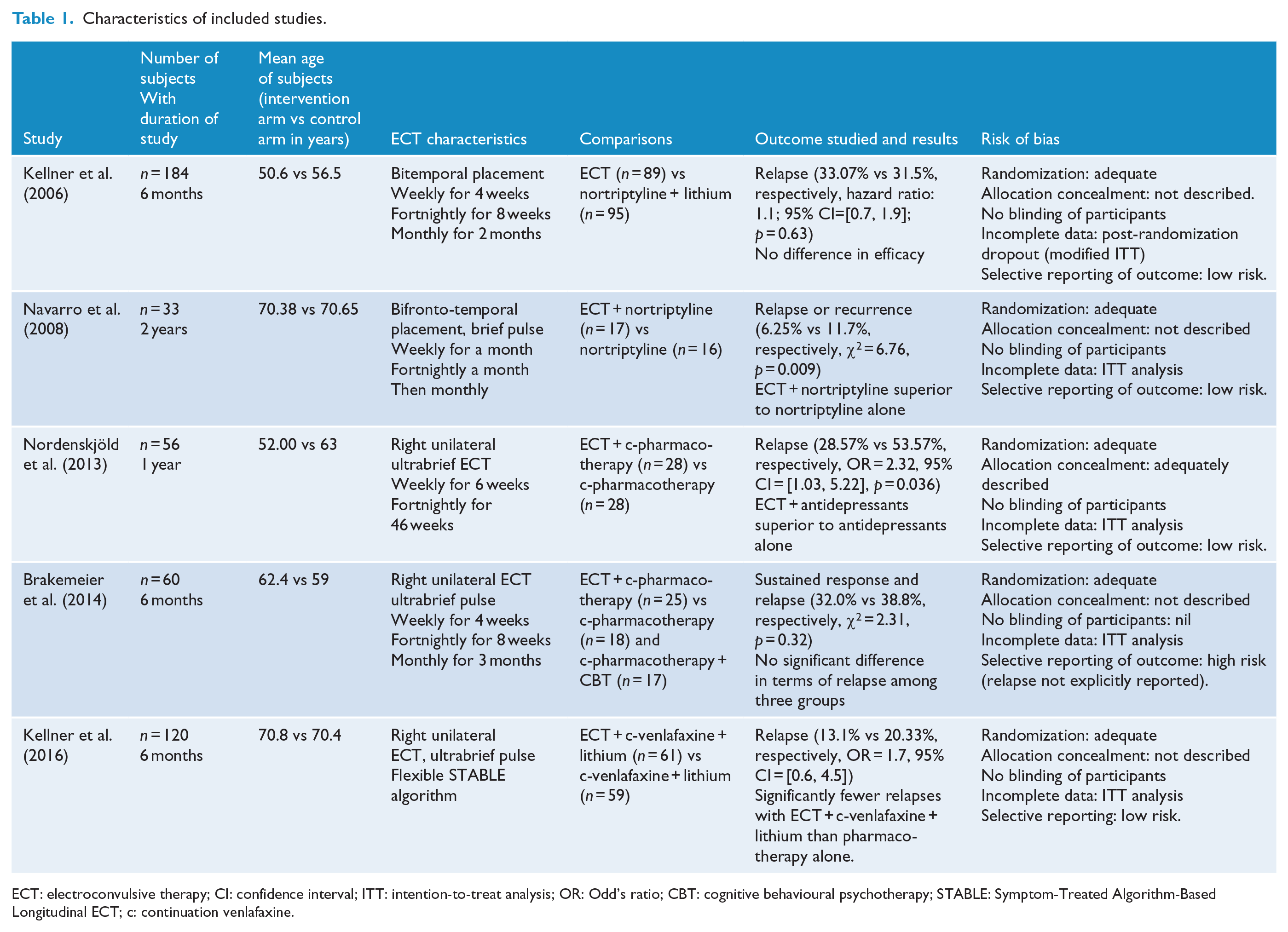
ECT: electroconvulsive therapy; CI: confidence interval; ITT: intention-to-treat analysis; OR: Odd’s ratio; CBT: cognitive behavioural psychotherapy; STABLE: Symptom-Treated Algorithm-Based Longitudinal ECT; c: continuation venlafaxine.
Adverse effects
The available data suggest tolerability of c-ECT and m-ECT. The dropout rate was not significantly different between c-ECT + continued pharmacotherapy and c-pharmacotherapy alone. The fact that cognitive functions were not significantly different in the c-ECT and m-ECT group compared to pharmacotherapy groups is consistent with the previous findings of lack of cognitive deterioration with continued or repeated course of ECT (Kirov et al., 2016; Russel et al., 2003; Trevino et al., 2010; Vothknecht et al., 2003). The major cognitive side effects usually occur with acute ECT; the cognitive impact of c-ECT and m-ECT with wider intervals between treatments appears to be negligible with the assessment instruments used in these studies. Cognitive functions were assessed mostly by MMSE, a tool that does not assess retrograde memory impairment, an adverse effect of significant interest with ECT (Folstein et al., 1975). This meta-analysis did not find a significant difference in the MMSE score at the end of included trials.
Limitations of the evidence
The most important limitation was small number of randomized trials with limited duration, 6 months to 2 years. However, this meta-analysis provides practitioners the nature of evidence for c-ECT and m-ECT and important information about some of the technical aspects of continued ECT: appropriate criteria (see below), concomitant pharmacotherapy, frequency and dosing, role of ultrabrief ECT in the maintenance treatment and safety. ECT remains as an underutilized treatment, and this is particularly the case with c-ECT and m-ECT even though recurrence rate is sizeable. The first randomized trial of c-ECT was published in 2006 and the last one in 2016. At the same time, the literature is replete with retrospective studies and case reports of c-ECT and m-ECT (Brown et al., 2014; Rabheru, 2012). This probably reflects renewed interest in the field of c-ECT and m-ECT, but the challenges in conducting well controlled trials: logistics, stigma, ethics approval and patients’ adherence. In view of the small number of trials, the data were initially pooled in an exploratory way with c-/m-ECT as a class regardless of concurrent pharmacotherapy, electrode placement, pulse width and frequency of treatment sessions. However, each treatment characteristic may have potential impact on the outcome and future direct comparison may be useful. The findings of this meta-analysis may change when enough data emerge for differential meta-analysis, i.e. meta-analyses that can examine the role of individual treatment factors. The current meta-analyses have identified some design issues that may be considered for future trials. The studies by Navarro et al. (2008) and Kellner et al. (2016) have limited generalizability because of age selection. Pharmacotherapy used in the included trials was mostly restricted to venlafaxine and nortriptyline in combination with lithium: role of other drugs as concomitant treatment with m-ECT needs to be explored. Brakemeier et al. (2014) examined subjects for response rather than remission in a c-ECT trial and found no significant difference between c-ECT + c-pharmacotherapy and c-pharmacotherapy alone. Other trials that used remission as the outcome criterion showed benefits of c-ECT and m-ECT over c-pharmacotherapy alone. This observation warrants further study as to the appropriate criterion to be examined in future study of the continuation and maintenance treatment of patients after an acute course of ECT. Information regarding m-ECT from controlled trials beyond 2 years is non-existent: prospective non-randomized trials and retrospective chart reviews form the database for extended m-ECT over several years (Brown et al., 2014; Rabheru, 2012). There is little evidence to support superior efficacy of stand-alone continuation ECT over antidepressant pharmacotherapy. Randomized trials show 30%–39% relapse rate with a combination of nortriptyline and lithium, a rate comparable to stand-alone continuation ECT but superior to placebo (Kellner et al., 2006; Sackeim et al., 2001).
Conclusion
Meta-analyses of the available but limited data show that both c-ECT and m-ECT along with concomitant pharmacotherapy have superior efficacy in reducing the risk of relapse and recurrence of depression for 1 year after remission from an acute course of ECT in comparison to pharmacotherapy alone. The evidence is modest and derived from a small number of randomized trials suggesting the need for more trials of maintenance ECT with longer duration.Acknowledgment
Footnotes
Acknowledgements
The authors would like to acknowledge Cochrane for their Review Manager 5 (RevMan 5) software.
Correction (May 2025):
This article has been updated online to correct Figure 3 and a sentence in the section: Maintenance ECT with pharmacotherapy against pharmacotherapy alone: 1-year outcomes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.