
Abstract
Introduction
In recent years, the role of electroconvulsive therapy (ECT) as a psychiatric treatment modality has been challenged by an increasing range of pharmacological and psychotherapeutic treatments, as well as newer brain stimulation techniques such as transcranial magnetic stimulation (TMS) (Merkl et al., 2009). This increase in treatment options for severe mental illness raises questions regarding current patterns of ECT use and whether ECT use has remained stable or changed over time. Few population-level epidemiological studies examining these questions have been published. Availability of Australian population-level data would be helpful in informing clinicians’ and policymakers’ understanding of this field and allow comparison of local practices with those in other places.
A few previous studies from the United States (US) examined ECT service delivery at a geographical aggregation higher than a single hospital, health service or city (Hermann et al., 1995; Olfson et al., 1998; Rosenbach et al., 1997). Rosenbach et al. (1997) examined trends and variations in ECT utilisation rates, expenditures and treatment patterns in the Medicare population from 1987 to 1992 using a 5% nationally representative data sample. An increase in use was documented, both in terms of absolute patient numbers (12,000–15,560) and rate of use per 10,000 population (4.2–5.1). Increased use was noted among women, whites and people with disabilities under 65 years, but not among men, non-whites or older adults. The share of outpatient ECT expenditure also increased (7–16%). Patients received eight ECT treatments on average.
Two additional population-level US studies provided useful cross-sectional ECT utilisation data, but no information on patterns of use over time (Hermann et al., 1995; Olfson et al., 1998). Hermann et al. (1995) studied variation in ECT use across 317 metropolitan statistical areas, using data from the American Psychiatric Association’s 1988–1989 Professional Activities Survey, with 17,729 psychiatrists treating 4398 patients with ECT. Utilisation rates varied highly among the 202 statistical areas reporting ECT use, ranging from 0.4 to 81.2 patients annually per 10,000 population. Psychiatrist, primary care physician and private hospital bed numbers per capita were the strongest predictors of variation, along with regulatory stringency.
Olfson et al. (1998) examined ECT use among adult inpatients with recurrent major depression, and whether prompt ECT affected length and cost of inpatient care, using the 1993 Healthcare Cost and Utilization Project data. ECT was used in 9.4% of patients in this category, with 59.2% commencing treatment within 5 days of admission. ECT recipients were more likely to be older, white, privately insured and residing in affluent areas. Although ECT was related to longer and costlier admissions, prompt ECT administration was associated with shorter and less costly hospital stays after accounting for patient selection.
Despite being used in Australia since 1941 (Birch, 1942; Goldney and Adams, 2009), population-level studies regarding Australian ECT use are similarly limited, with only two studies examining changes in use over time (Doessel et al., 2006; Teh et al., 2005). Teh et al. (2005) studied ECT practice in Western Australia from 1988 to 2001 using a partially complete data set derived from the State Mental Health Information System and psychiatric hospital records. Most ECT recipients were adult women (65% of 1469 ECT patients) diagnosed with mood disorders (> 82%). The average age at the first ECT admission was 50 years for both genders. The number of ECT recipients rose markedly each year (particularly adults aged 18–64 years), increasing by 73% compared to only a 5% increase in the State’s resident population during the same 5 years. However, the proportion of ECT use within psychiatric services remained constant due to a parallel increase in psychiatric inpatient admissions over this time.
Doessel et al. (2006) examined private ECT service provision in Australia from 1984 to 2004 using Medicare data, in terms of absolute numbers and utilisation rates. Private sector ECT use varied considerably, falling from 1984 to 1991 but subsequently rising even in the context of declining use of other private psychiatric services. Variations between different states and territories were also demonstrated, with a U-shaped pattern of use in five states (consistent with a decrease in use early in the study period, followed by a subsequent increase) and a linear pattern in South Australia and The Northern Territory. Utilisation rates were highest in Queensland, South Australia, The Northern Territory and Victoria, and particularly low in Western Australia.
Two further population-level Australian studies provided a cross-sectional picture of ECT use, but did not examine changes in use over time (Jorm and Henderson, 1989; Wood and Burgess, 2003). ECT formed a larger percentage of private psychiatric services provided to older rather than younger Australians in the 1985–1986 financial year, based on an analysis of national Medicare data by Jorm and Henderson (1989). Overall, older adults received ECT 1.84 times the per capita rate for younger adults. The trend towards rising ECT use with age was particularly strong among women.
Wood and Burgess (2003) used Victorian statutory ECT data from the 1998–1999 financial year to study population-based utilisation rates, attributes of ECT recipients and factors related to differential use. Across public and private sectors, crude treated-person and administration rates were 39.9 persons and 330.3 ECT treatments per 100,000 population/annum, respectively. Corresponding age-adjusted rates were 44.0 persons and 362.6 ECT treatments per 100,000 population/annum, respectively. Age/sex-specific rates generally increased with age and female sex, with 75.2% of recipients having depression, 32.9% aged over 64 and 62.8% being women. Public sector ECT was independently predicted (in decreasing order of importance) by diagnosis, age and sex.
In this paper, we examine ECT delivery in the state of Victoria, Australia, one of eight Australian states and mainland territories, with an estimated resident population at 30 June 2007 of 5.2 million people (Australian Bureau of Statistics, 2007). We report ECT provision to adults aged 25 years and over from 1998 to 2007, focusing particularly on changes in utilisation rates over this period. We also compare our results to existing population-level utilisation studies; offer possible explanations for our findings based on clinical experience of ECT service delivery; and provide recommendations for future research. This paper is unique in the ECT literature in presenting 10-year, population-adjusted ECT utilisation rates across all public and private treatment settings within an entire statutory region.
Methods
In Victoria, ECT is provided in both the public and private hospital sectors. In June 2011, there were more public than private acute psychiatry inpatient beds in the State (approximately 921 and 532 respectively, with a 1.7:1 ratio); we expect this ratio to have been comparable during the study period. Voluntary or involuntary treatment under the Mental Health Act (MHA) of Victoria is possible, but the latter is only permitted in the public sector. Acute ECT is usually administered to inpatients, but outpatient treatment also occurs (representing both acute and continuation/maintenance ECT) (O’Connor et al., 2010a; O’Connor et al., 2010b).
Analyses are based on statutory ECT data collected from mental health services across Victoria by the Office of the Chief Psychiatrist, Victorian Department of Health. Individual patient and service level data, containing details of every public and private sector ECT treatment administered in the State, are regularly forwarded to the Department by service providers in a structured format. ECT-related information collected by the Department includes patient demographic data; treatment setting (public or private); whether treatments are administered voluntarily or under the MHA; and the type of electrode placement used. ECT data for the 1998–2007 period were extracted from departmental data and made available to researchers in a de-identified format. Ethics approval was provided by the Department of Health Human Research Ethics Committee (Victoria).
In providing data to investigators, an attempt was made to preserve as much original information as possible while presenting it in a format amenable to analysis using Predictive Analytics Software (PASW) Statistics version 18 (SPSS Inc., Chicago, Illinois, USA). The data aggregation required to achieve this balance limited the types of analyses possible. For example, any individual patient was included only once as a single case in any one year and other variables were organised accordingly. Thus, a single annual treatment count was recorded for each patient, with no provision to determine whether this represented one or more acute courses or a series of continuation/maintenance treatments. Similarly, only one centre type (public or private) was recorded annually for each patient, according to the first centre type at which ECT was administered in that year. Most patients likely received all their ECT at the same centre in any one year, but some may have been treated at more than one location. Reported findings for public versus private sector treatment are thus approximate. We recoded diagnoses as either ‘depression’, ‘psychosis’ (incorporating schizophrenia and schizoaffective disorder) or ‘other’ (incorporating mania) and divided patients into three groups for age-related analyses (25–44, 45–64 and 65 years and over). Patients aged less than 25 years were not studied as too few received ECT for population-level analysis to be meaningful.
The primary demographic and clinical variables examined were as follows:
gender (male, female);
diagnosis (depression, psychosis, other);
age group (25–44, 45–64, 65+);
treatment setting (public, private);
MHA status (voluntary only, involuntary only, mixed status);
electrode placement (unilateral only, bilateral only, mixed placement).
Tables 1–3 show descriptive statistics and preliminary analyses for primary demographic and clinical categories and selected subcategories of interest. The tables are primarily organised to illustrate differences in the percentage of patients and percentage of treatments for related primary categories or subcategories from 1998 to 2007 (contained within the same table row and, in the case of subcategories, arranged according to age group or diagnosis). Patients have been counted only once in deriving the given percentages, even if treated more than once in separate years. For the 2007 data, the number of patients and number (mean; SD) of treatments are also provided as a basis for undertaking ANOVAs using OpenEpi (Dean et al., 2011) to look for differences in the number of treatments administered to patients in related primary categories or subcategories.
Electroconvulsive therapy in Victoria (1998–2007): descriptive statistics and preliminary analyses for primary clinico-demographic categories.
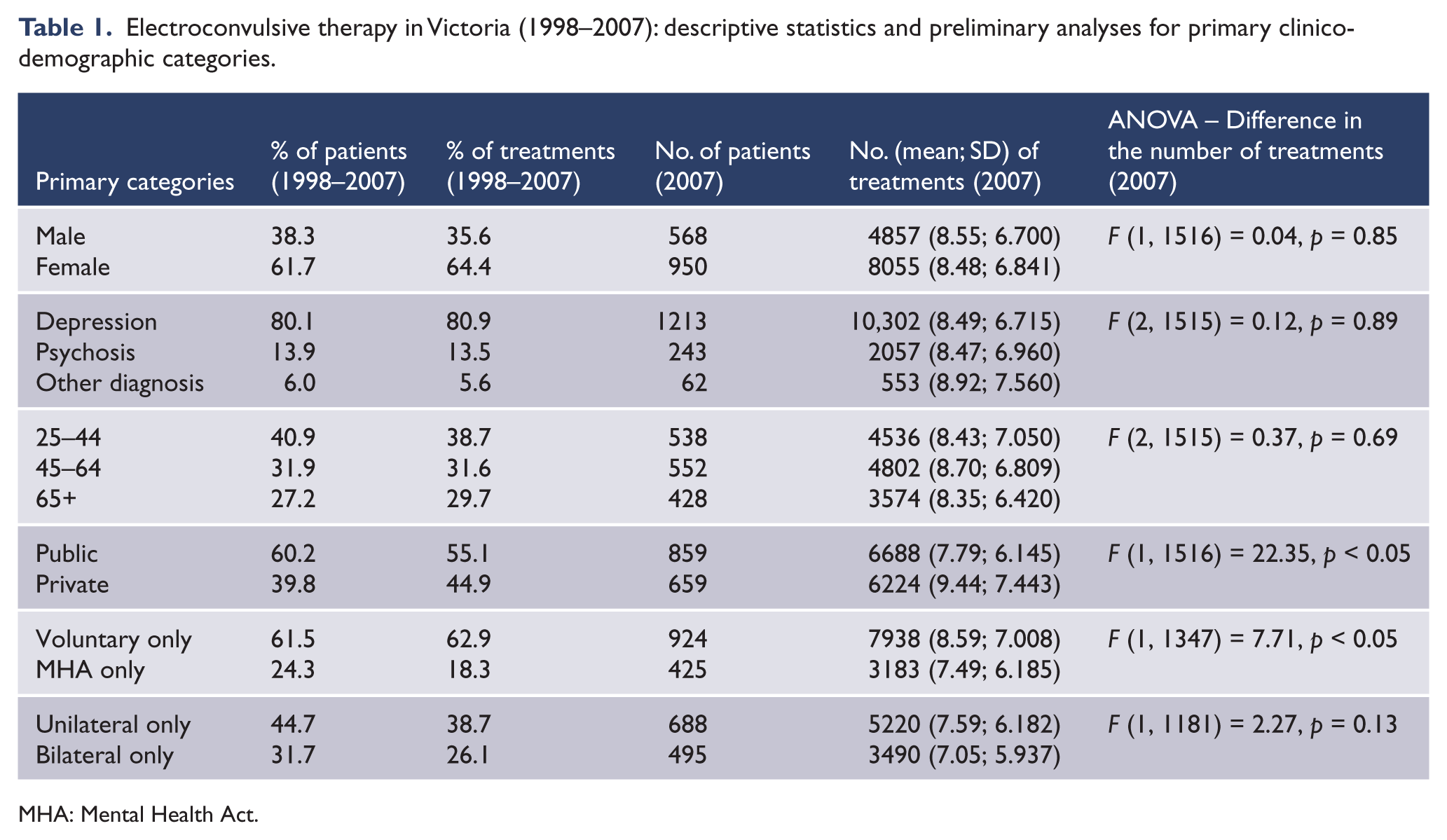
MHA: Mental Health Act.
Electroconvulsive therapy in Victoria (1998–2007): descriptive statistics and preliminary analyses for selected clinico-demographic subcategories according to age group.
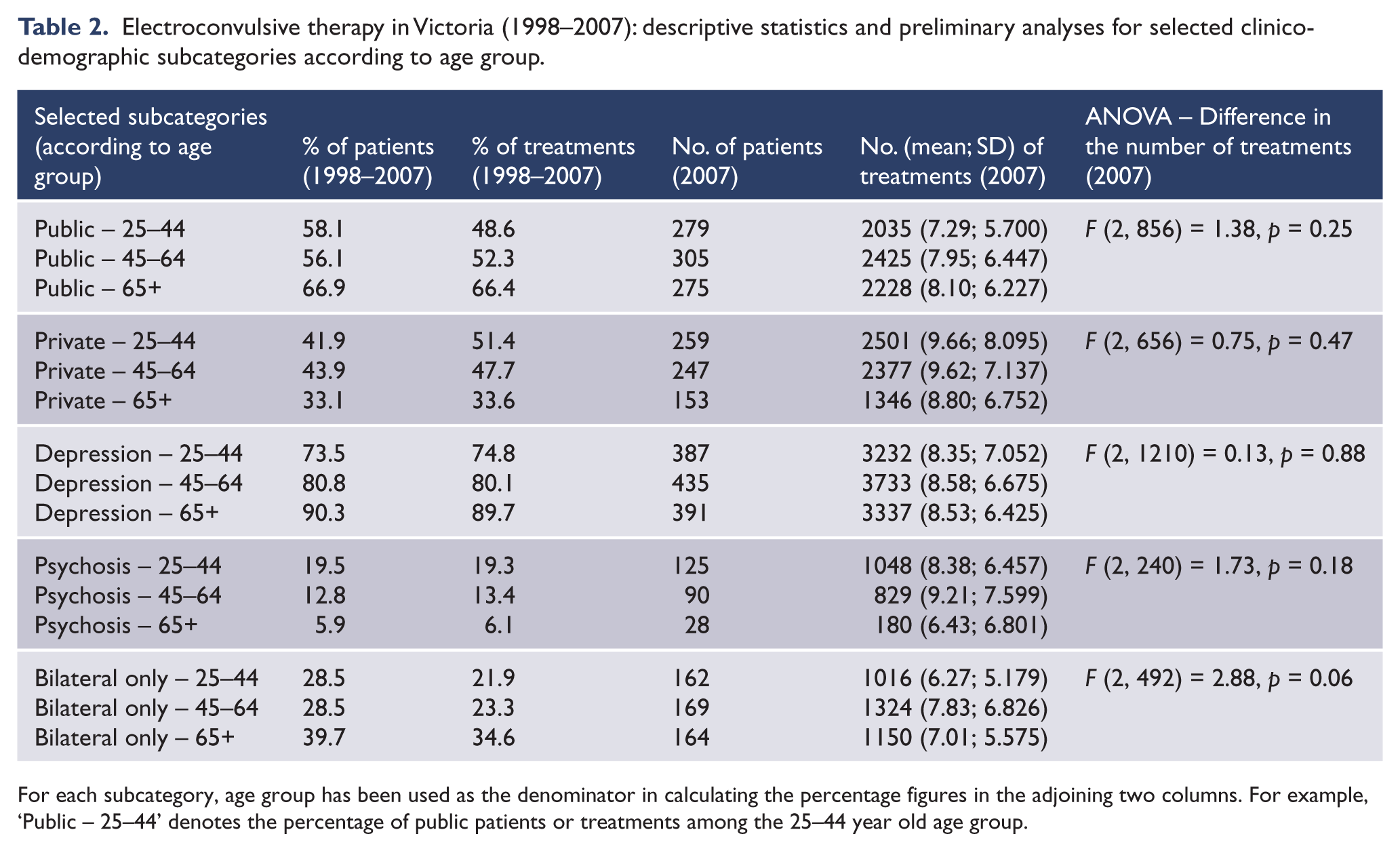
For each subcategory, age group has been used as the denominator in calculating the percentage figures in the adjoining two columns. For example, ‘Public – 25–44’ denotes the percentage of public patients or treatments among the 25–44 year old age group.
Electroconvulsive therapy in Victoria (1998–2007): descriptive statistics and preliminary analyses for selected clinico-demographic subcategories according to diagnosis.
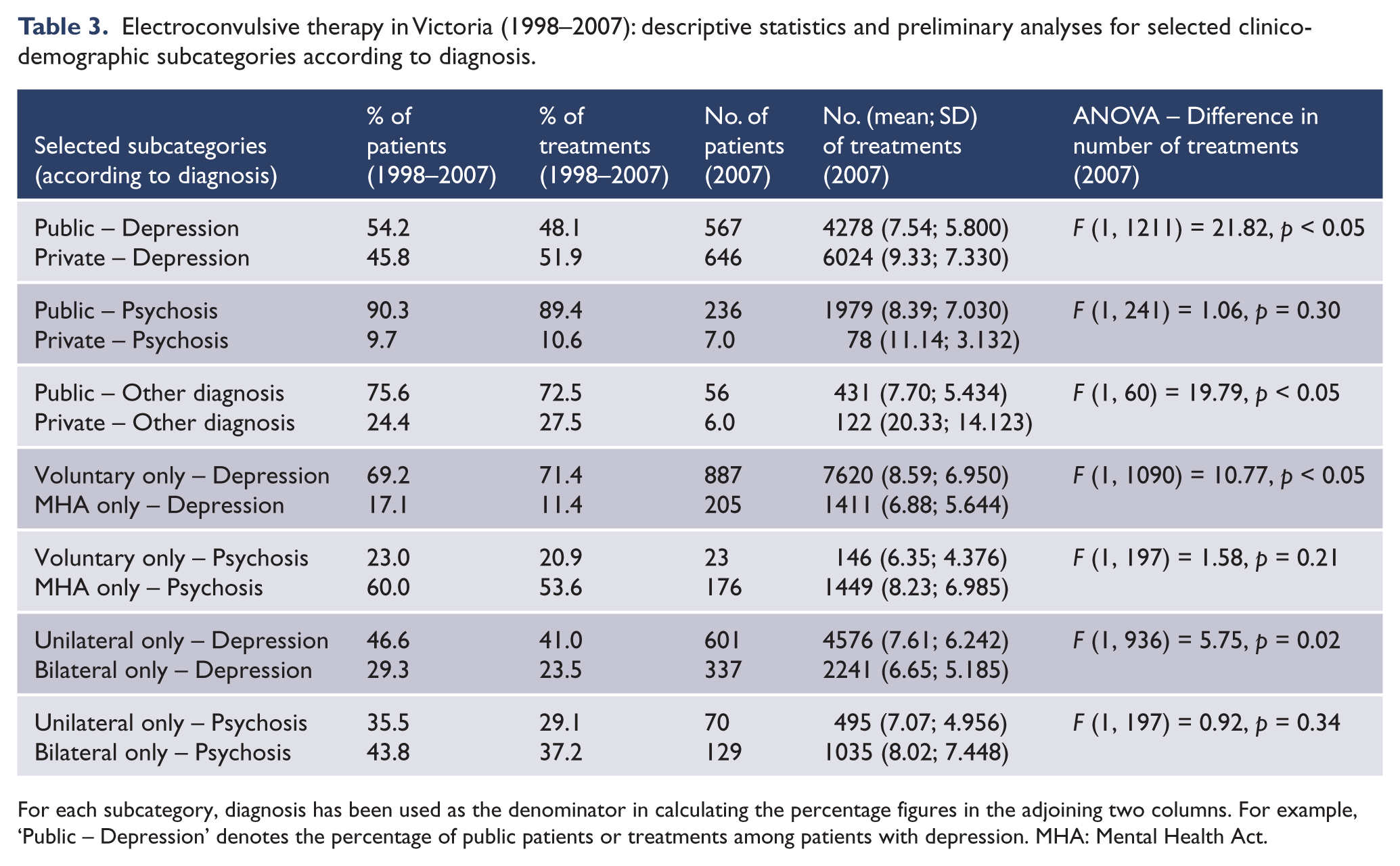
For each subcategory, diagnosis has been used as the denominator in calculating the percentage figures in the adjoining two columns. For example, ‘Public – Depression’ denotes the percentage of public patients or treatments among patients with depression. MHA: Mental Health Act.
As the centrepiece of this paper, crude annual ECT data were converted into utilisation rates per 100,000 population, using a time series spreadsheet of Victoria’s population by year of age (Australian Bureau of Statistics, 2010), and results presented graphically for primary demographic and clinical categories (Figures 1–6). Population adjustment was performed to account for the growth in Victoria’s population from 4,660,900 in June 1998 (Australian Bureau of Statistics, 1998) to 5,205,200 in June 2007 (Australian Bureau of Statistics, 2007).
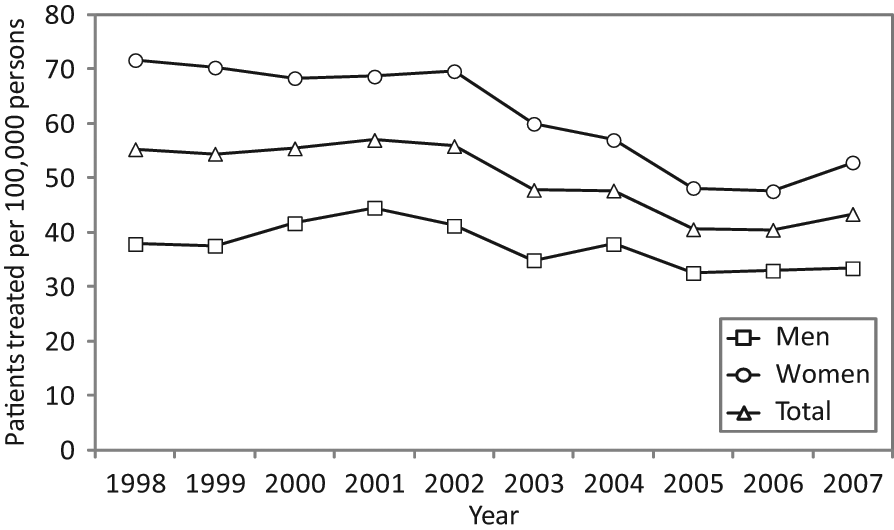
Patients treated with electroconvulsive therapy per 100,000 men, women and total population (Victoria, 1998–2007).
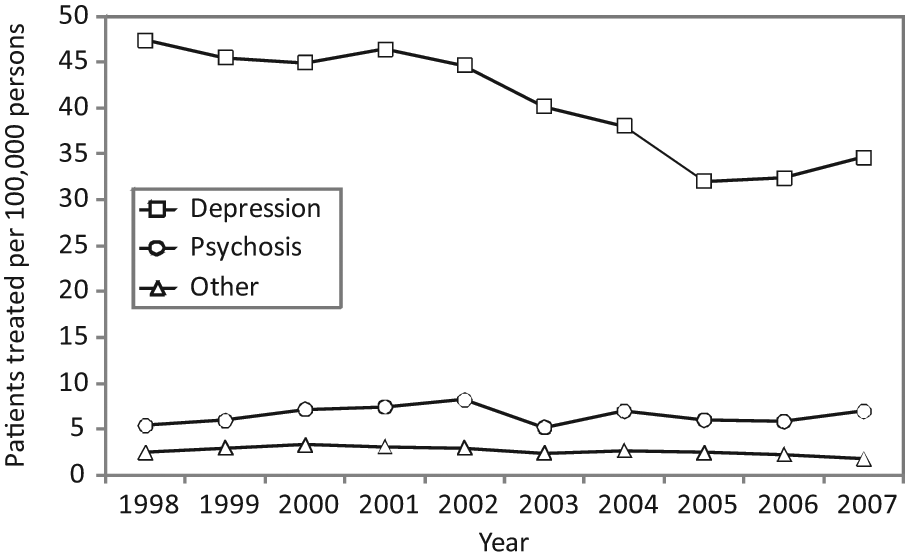
Patients treated with electroconvulsive therapy for depression, psychosis or other diagnoses per 100,000 population (Victoria, 1998–2007).
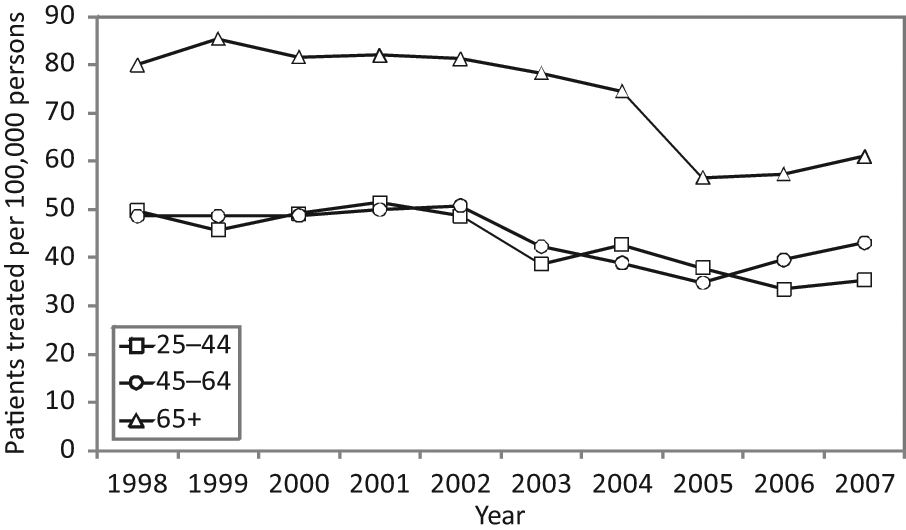
Patients treated with electroconvulsive therapy per 100,000 age-specific population (Victoria, 1998–2007).
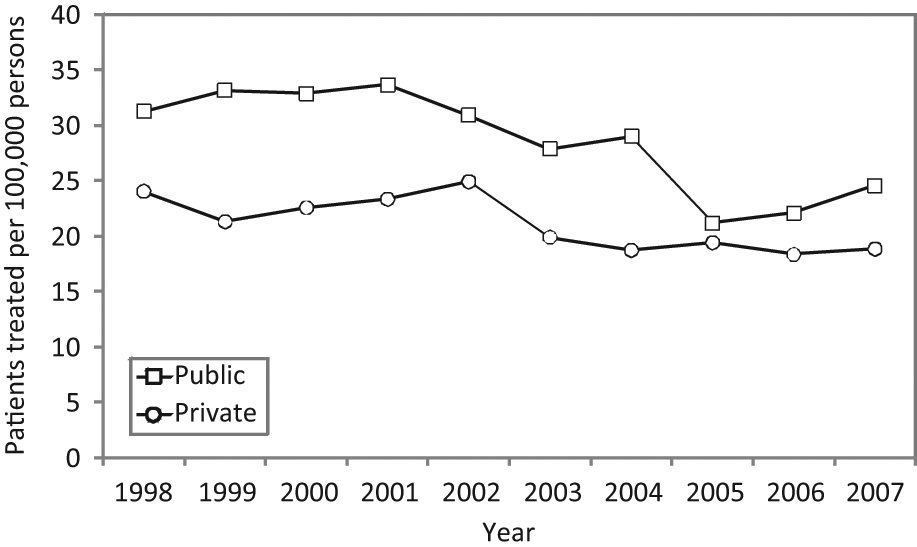
Public and private patients treated with electroconvulsive therapy per 100,000 population (Victoria, 1998–2007).
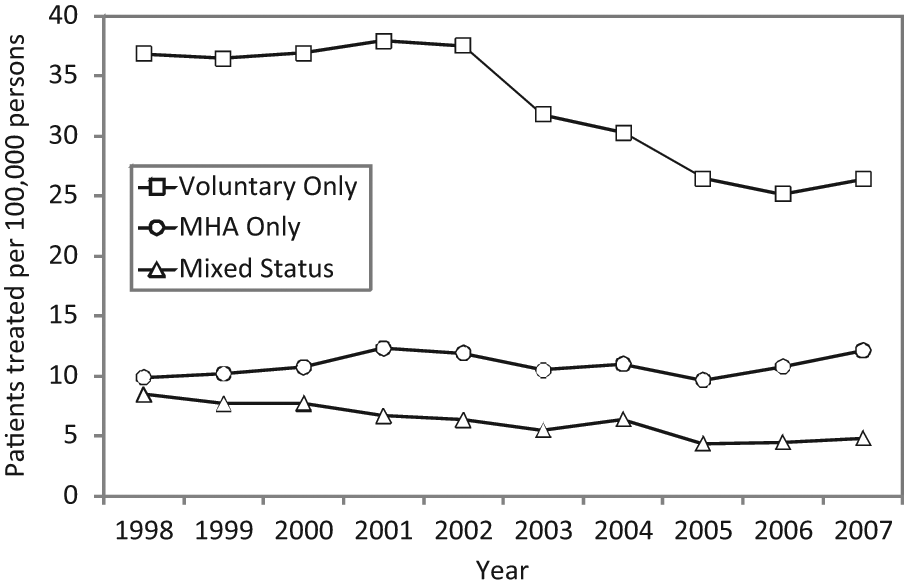
Patients treated with electroconvulsive therapy per 100,000 population, according to Mental Health Act (MHA) status (Victoria, 1998–2007).
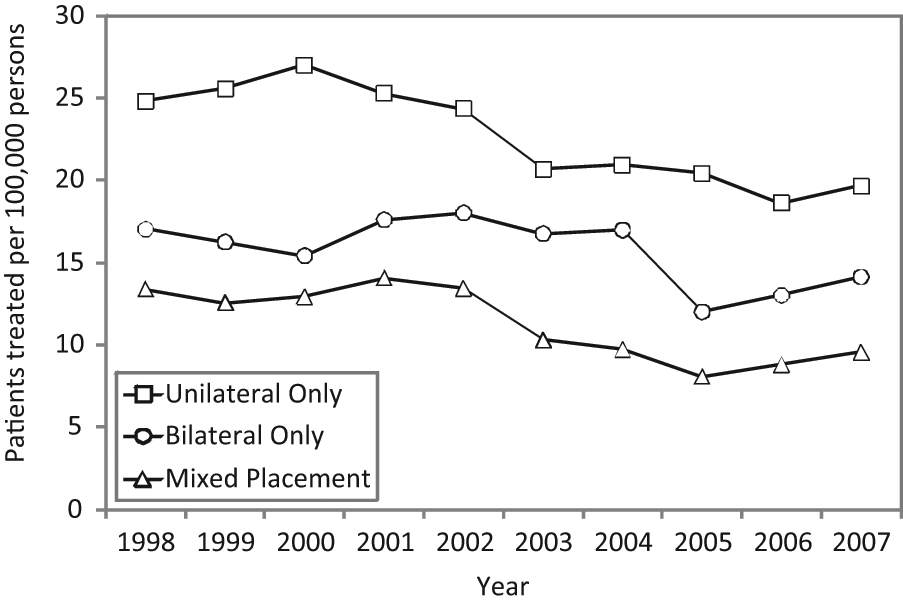
Patients treated with electroconvulsive therapy per 100,000 population, according to electrode placement (Victoria, 1998–2007).
Results
Descriptive statistics and preliminary analyses
Inspection of the second and third columns of Table 1 (percentage of patients and treatments, 1998–2007) allows the following conclusions to be drawn regarding primary demographic and clinical categories. Most ECT recipients were women. The vast majority of patients were treated for depression, followed in decreasing order by psychosis and other diagnoses (in much smaller numbers). The greatest percentage of patients (and treatments) was in the 25–44 years age group, followed in decreasing order by the 45–64 and 65+ age groups. Most ECT recipients were treated in the public sector. The majority of patients received treatment on a voluntary basis only. Patients treated with only a unilateral electrode placement exceeded those treated with only a bilateral placement.
ECT use differed according to age group (Table 2). There was a greater gap between public-private sector ECT service provision among older adults (aged 65+), who were treated in smaller numbers in the private sector than their younger counterparts. With increasing age, the percentage of patients receiving ECT for depression increased whereas the percentage receiving ECT for psychosis decreased. Bilateral treatment only was used in a higher percentage of patients aged 65+ years, compared to their younger counterparts.
ECT use also differed according to diagnosis (Table 3). Patients with depression were treated in the public and private sectors in roughly equal numbers, whereas a clear majority of patients with psychosis or other diagnoses were treated publicly. The majority of patients with depression received voluntary treatment only, whereas the majority of those with psychosis received involuntary treatment only. An exclusively unilateral electrode placement was most common among patients with depression, whereas an exclusively bilateral placement was most common among those with psychosis.
Only two ANOVAs were indicative of differences in the amount of ECT administered to patients in related primary categories (Table 1). Private patients received significantly more treatments than public patients. Patients receiving ECT on a voluntary basis only received significantly more treatments than those receiving ECT under the MHA (i.e. involuntarily) only.
No ANOVAs reached significance for differences in the amount of ECT administered to patients in related subcategories arranged according to age (Table 2). However, significant differences emerged in the amount of ECT administered to patients in related subcategories arranged according to diagnosis (Table 3). Patients with depression received significantly more treatments:
in the private than public sector;
on a voluntary basis only than under the MHA (i.e. involuntarily) only;
with an exclusively unilateral electrode placement than an exclusively bilateral placement.
Patients with diagnoses other than depression or psychosis also received significantly more treatments in the private than public sector.
Ten-year, population-adjusted utilisation rates
Graphical representation of ECT utilisation data from 1998 to 2007 allows observations about the pattern of use over time to be made. Patients treated with ECT in Victoria from 1998 to 2007 per 100,000 men, women and total population are shown in Figure 1. An overall decline in ECT use from 2001 onward is evident, followed by a small increase in 2007.
Patients treated with ECT for depression, psychosis or other diagnoses in Victoria from 1998 to 2007 per 100,000 population are shown in Figure 2. This figure demonstrates that much of the decline in ECT use during the study period was for depression, whereas utilisation rates for psychosis and other diagnoses remained relatively stable over time.
Patients treated with ECT in Victoria from 1998 to 2007 per 100,000 age-specific population are shown in Figure 3. Although crude data were indicative of relatively small numbers of patients aged 65+ years receiving ECT, age adjustment of data as presented in this figure reveals higher rates of ECT use among older adults compared to the two younger age groups. Furthermore, there was a particularly sharp decline in ECT use among patients aged 65+ years from 2004 to 2005.
Public and private sector patients treated with ECT in Victoria from 1998 to 2007 per 100,000 population are shown in Figure 4. The rate of ECT use was consistently higher in public than private settings. A notable decline in public sector use from 2004 to 2005 (perhaps partially reflecting the decline among patients aged 65+ years over the same period) resulted in almost equal use between sectors in 2005, with rates subsequently diverging again.
Patients treated with ECT in Victoria from 1998 to 2007 per 100,000 population according to MHA status are shown in Figure 5. Most patients were treated on a voluntary basis only and it was among this group that much of the decline in ECT use during the study period occurred. Utilisation rates among patients treated under the MHA (i.e. involuntarily) only or with a mix of voluntary and involuntary treatment were more stable over time.
Patients treated with ECT in Victoria from 1998 to 2007 per 100,000 population according to electrode placement are shown in Figure 6. The previously noted sharp declines in ECT use among patients aged 65+ years and in public sector treatment from 2004 to 2005 are paralleled here by a reduction in exclusively bilateral electrode placement over the same period.
Discussion
Our findings have important limitations, many stemming from aggregation of information in the research data set. For example, the total annual treatment count available for each patient precluded differentiation of acute from maintenance ECT. Reported public-private use is approximate, as only the initial treatment setting was recorded annually for each patient. The research data set included limited demographic information and was restricted to ECT alone rather than psychiatric service delivery in general, impeding the conduct of meaningful regression analyses for the prediction of ECT use. Despite these limitations, documentation of ECT use across Victoria for an entire decade allows comparison of local with interstate and overseas practice, and hypothesis generation from observed findings to guide future research.
Population-adjusted ECT utilisation data from 1998 to 2007 (Figure 1) indicates a gradual overall decline in use over time, with a slight increase again in 2007. Availability of selective serotonin reuptake inhibitors (SSRIs) and serotonin–noradrenaline reuptake inhibitors (SNRIs), which are safer and better tolerated than tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs) (Papakostas, 2010; Thase and Denko, 2008), may help explain this pattern. Figure 2 further supports this hypothesis, with much of the decline in ECT use during this period being for depression, whereas use for psychosis and other diagnoses remained relatively constant. Alternatively, the treatment of fewer patients with non-psychotic mood disorders in the public sector over time due to resource constraints may have contributed to this finding. It is nevertheless clear that significant numbers of patients continued receiving ECT during the study period. This pattern of decreasing use (apparent even prior to population adjustment of data) is in contrast with the finding by Teh et al. (2005) of a marked increase in ECT recipients from 1988 to 2001 in Western Australia. Our population-adjusted utilisation rates of 54.4 patients treated and 529 treatments administered per 100,000 population in 1999 are slightly higher than, but comparable to, previously published figures by Wood and Burgess (2003) for the 1998–1999 financial year. Methodological factors are likely to account for this difference.
Our findings that 61.7% of patients were women and 80.1% had depression are consistent with depression occurring more commonly among females (Parker and Brotchie, 2010) and being the predominant indication for ECT (Baghai and Möller, 2008). These figures are comparable to those reported by Wood and Burgess (2003) for Victoria (62.8% female, 75.2% depression) and Teh et al. (2005) for Western Australian (64.9% female, > 82% affective disorders).
Although patients aged 65 years and over accounted for only 27.2% of ECT recipients, age adjustment of the data was indicative of these patients consistently receiving ECT at a higher rate than those in the 25–44 and 45–64-year-old age groups (Figure 3), for a diagnosis of depression in 90.3% of cases. Our findings concur with those of Wood and Burgess (2003) (25% aged 65 years and over, rising use with increasing age except in the 85+ age group), Teh et al. (2005) (27% aged 65 years and over and treated at a higher rate than younger adults) and Jorm and Henderson (1989) (older adults received ECT 1.84 times the per capita rate for younger adults).
One possible explanation is that older adults may experience severe forms of medication-resistant mental illness (Mulsant and Pollock, 1998). Psychiatric hospital separations for psychotic depression have been shown to peak in men aged 70–74 and women aged 75–79 (Draper and Low, 2009). The combination of depressive psychosis and objective signs of melancholia (psychomotor agitation and retardation, either together or alone) is particularly predictive of ECT response (Buchan et al., 1992). Such illness can be life-threatening, as in the case of decreased oral intake of food and fluids accompanying depression, necessitating urgent intervention and response as afforded by ECT (Baghai and Möller, 2008; Gangadhar et al., 1982). Historically, ECT may have been used as a better tolerated alternative to TCAs and MAOIs in older adults with multiple medical comorbidities (Christopher, 2003; Kelly and Zisselman, 2000). The introduction of SSRIs and SNRIs may have attenuated concerns regarding medication tolerability, but SSRIs may be less effective than TCAs among inpatients (Anderson, 2000; Anderson, 2001), potentially also contributing to ongoing ECT use among older adults.
ECT was administered predominantly in the public sector (60.2% of patients), although population-adjusted administration rates were almost equal between sectors in 2005 (Figure 4). Figure 4 also reflects a previously reported peak (turning point) in private sector ECT use in Victoria in 2001–2002 (Doessel et al., 2006). Public-private ECT use differed notably according to diagnosis, with 90.3% of patients with psychosis receiving ECT in public rather than private settings. Impairments in reality testing and insight accompanying severe schizophrenia (Baier, 2010; Osatuke et al., 2008) are often more practically managed in the public sector and may necessitate involuntary treatment. This concurs with our finding that 60% of patients receiving ECT for psychosis were treated on an involuntary basis only. Psychosocial decline (Menezes et al., 2006; Van Os and Kapur, 2009) may also limit these patients’ ability to afford the private health insurance required to access private inpatient care. Similar considerations may explain the greater gap between public-private sector ECT service provision among adults aged 65 years and over, 66.9% of whom were treated publicly. Although older adults are more likely to be treated with ECT for depression than schizophrenia, inability to provide consent due to depressive psychosis and melancholia (Buchan et al., 1992) may necessitate public treatment under the MHA.
The finding that private patients received significantly more ECT treatments than public patients (despite a smaller number of private acute psychiatric beds) is suggestive of differences in practice between the two sectors. However, questions regarding whether ECT administration is more or less adequate in one or the other sector or whether any differences in practice are of clinical relevance cannot be answered with certainty based on this data alone.
The majority of patients (61.5%) were treated on a voluntary basis only. However, much of the decline in use from 2002 onwards occurred in this group, whereas patients receiving involuntary treatment only remained consistent in number (Figure 5). One possible explanation is that severe mental illness may be more likely to be treatment-resistant and require involuntary treatment, features which may characterise a consistent patient minority. Alternatively, the decline in ECT use on a voluntary basis only may reflect a broader, less severely ill patient population benefiting from newer pharmacological treatments or fewer patients with mood disorders being treated in the public sector over time. More patients with depression (69.2%) received ECT on a voluntary basis only compared to those with psychosis (23.0%), probably due to the impaired reality testing and poor insight more likely to accompany the latter.
The finding that 44.7% of patients received right unilateral treatment only and 31.7% bilateral treatment only suggests many psychiatrists prescribe right unilateral ECT in the first instance to minimise cognitive side effects, only switching to bilateral treatment where response is suboptimal (Plakiotis and O’Connor, 2009; Plakiotis et al., 2010). Despite the increased risk of ECT-related adverse cognitive sequelae among patients aged 65+ years (Gardner and O’Connor, 2008), 39.7% received bilateral treatment only compared to 28.5% of younger patients. Greater illness severity and treatment resistance may combine with medical comorbidity to increase the life-threatening nature of mental illness among older adults (Kelly and Zisselman, 2000; Prudic et al., 1990). Some psychiatrists may therefore prescribe bilateral ECT to older adults from treatment outset to achieve a rapid, efficient response while minimising unnecessary exposure to repeated anaesthesia, although the benefits of this approach are not proven.
Comparable factors may explain why most patients with depression received unilateral ECT only (46.6%), whereas most with psychosis received bilateral ECT only (43.8%). Although availability of antipsychotic medication has seen ECT for psychosis decline (Fink and Sackeim, 1996), a perception of psychosis as particularly treatment-resistant may underlie a preference for bilateral placement where ECT is resorted to. Comparison of bilateral with unilateral ECT in the treatment of schizophrenia has been identified as an under-researched area, although the limited available data to date suggest both modalities to be equally effective in terms of global improvement (Tharyan and Adams, 2005).
Conclusions
This paper provides a broad overview of ECT use in Victoria from 1998 to 2007. The scope of the available data is unique in ECT research, covering both public and private sector treatment across an entire jurisdiction over 10 years. Some of our findings reinforce conventional clinical impressions regarding patterns of ECT use. For example, the findings that most ECT recipients are women and have depression or that more patients with psychosis receive ECT in the public sector will likely come as no surprise to most practising clinicians. Other findings warrant closer attention as they may not be readily apparent in clinical practice. The finding of a higher age-adjusted utilisation rate among older adults is such an example that may be obscured by the relatively small (absolute) number of older patients with mental illness encountered clinically. The greater use of bilateral ECT among older adults – despite the potential for more adverse cognitive effects with this modality – is also notable, but may reflect clinicians’ need to take medical comorbidity into account in making complex risk–benefit decisions. While utilisation rates gradually declined over the decade studied, patients continued to receive ECT in significant numbers, suggesting that its role in treating severe mental illness is far from superseded.
The present population-level research cannot explain on its own the causative factors underlying the patterns that emerged, nor can it demonstrate the effectiveness (or adverse cognitive effects) of ECT as practised in Victoria. However, the findings raise interesting questions for further investigation. To facilitate future research endeavours, it may be worth reviewing the present generic system of mental health statutory data collection to see whether ECT data can be recorded in a manner making it even more amenable to research applications. As part of this process, possibilities for linking State ECT data to other State and national health databases can be explored, while ensuring all steps are taken to preserve the confidentiality of sensitive health-care information. In the meantime, there is scope to explore additional questions using our existing data set – such as ECT use for more specific diagnoses, including mania and schizophrenia – despite the identified limitations.
Footnotes
Acknowledgements
We thank Joyce Goh for assisting us in accessing the ECT database.
Funding
We thank the John Cockayne Memorial Aged Care Research Fund for supporting this study.
Declaration of interest
The authors report no conflicts of interest and are alone responsible for the content and writing of this paper.