
Abstract
Objective:
Emergency departments the world over have seen substantial increases in the number of individuals presenting for mental health reasons. However, we have a limited understanding of their experiences of care. The aim of this review was to systematically examine and synthesise literature relating to the experiences of individuals presenting to emergency department for mental health reasons.
Methods:
We followed Pluye and Hong’s seven-step approach to conducting a systematic mixed studies review. Studies were included if they investigated adult mental health experiences in emergency department from the users’ perspective. Studies describing proxy, carer/family or care provider experiences were excluded.
Results:
Sixteen studies were included. Thematic synthesis identified three themes and associated subthemes. Theme 1 – ED staff can make-or-break and ED experience – comprised: Feeling understood and heard; Engaging in judgement-free interactions; Receiving therapeutic support; Being actively and passively invalidated for presenting to the ED; and Once a psych patient, always a psych patient. Theme 2 – Being in the ED environment is counter-therapeutic – comprised: Waiting for an ‘extremely’ long time; and Lacking privacy. Theme 3 was Having nowhere else to go.
Conclusions:
The experiences described by individuals presenting to emergency department for mental health reasons were mostly poor. The results illustrate a need for increased mental health education and training for all emergency department staff. Employment of specialist and lived experience workers should also be prioritised to support more therapeutic relationships and emergency department environments. In addition, greater investment in mental health systems is required to manage the current crisis and ensure future sustainability.
Keywords
Introduction
Mental illness is a significant contributor to the global burden of disease (Ferrari et al., 2022). Although the Organisation for Economic Cooperation and Development (OECD) reports that some countries are making progress towards strengthening mental healthcare systems, there are still significant gaps in all countries when it comes to mental health system performance (Organisation for Economic Cooperation and Development, 2021). In particular, there is a disproportionate burden on emergency departments (EDs) globally to provide care for individuals with mental illness (Brathwaite et al., 2022; Ferro et al., 2023; Lavergne et al., 2022; Ramadan et al., 2022; Villas-Boas et al., 2023). For example, mental health–related ED presentations in the United States increased by 40.8% between 2009 and 2015, accounting for more than 10% of all ED presentations in individuals 15–64 years old (Santillanes et al., 2020). The growth in presentations was even greater in England at 200% between 2010 and 2020 (Wardrop et al., 2023). These individuals were also twice as likely to spend 12 hours or more in ED compared to people presenting for other reasons (Royal College of Emergency Medicine, 2022).
Despite the emphasis for health services and systems to provide person-centred care, there is currently limited understanding of the experiences of individuals presenting to ED for mental health reasons. These experiences are a critical component of quality and safety (Australian Commission on Safety and Quality in Health Care, 2014; Luxford et al., 2010; Marsh et al., 2019; Sargent and Waldman, 2019) and form the bedrock of safe, high-quality healthcare (Anhang Price et al., 2014; Kruk et al., 2018). Moreover, improved experiences have been linked to improved health outcomes (Cathal et al., 2013; Prang et al., 2019). Person-centred care requires active collaboration, communication and shared decision-making between healthcare providers, services and people (Delaney, 2017; Sharma et al., 2015). Yet, if we do not understand the experiences of some of our most vulnerable ED users, it becomes challenging to respond to their preferences, needs and values. Thus, the aim of this study was to systematically examine and synthesise the literature relating to the experiences of individuals presenting to ED for mental health reasons.
Methods
Study design
This was a systematic mixed studies review (SMSR) that followed the seven-step approach described by Pluye and Hong (2014). Reporting was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Page et al., 2021). The SMSR was registered with the international prospective register of systematic reviews (PROSPERO; ID: CRD42023458916). There was no patient and/or public involvement.
Step 1: formulate a review question
The aim was to systematically review literature relating to mental health experiences in ED. In addressing this aim, we sought to answer the following research question: How do individuals presenting to ED for mental health reasons describe their experiences of care?
Step 2: define eligibility criteria
Studies were included in the SMSR if they met the criteria detailed in Table 1. An experience was defined as ‘what’ happened during an episode of care, and ‘how’ it happened from the service user’s perspective (Bull et al., 2019). We did not include studies that described service user’s satisfaction. This is because experiences and satisfaction differ conceptually and operationally (Bull, 2021), and experiences are considered to provide more actionable information for quality improvement (Ahmed et al., 2014).
Eligibility criteria.
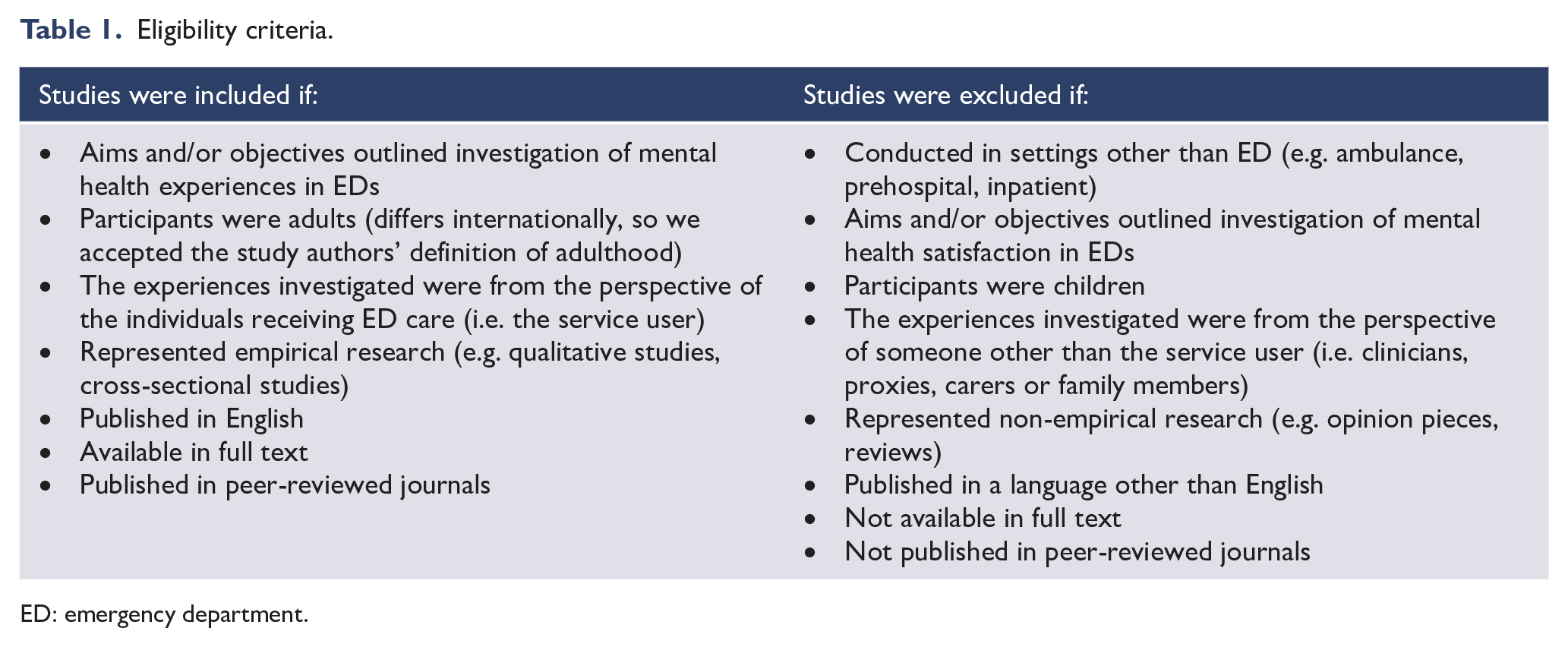
ED: emergency department.
Presentations to ED for mental health reasons were defined broadly as to not limit the inclusion of studies based on the severity or type of mental illness described. As such, we defined mental illness as a principal diagnosis of mental or behavioural disorder (e.g. depression, anxiety, schizophrenia, psychosis, post-traumatic stress, personality and substance use disorders), poisoning, self-harm or suicide ideation. This aligns with how mental illness has been defined in other reviews (Mao et al., 2023; Newton et al., 2010).
Step 3: apply an extensive search strategy
The following electronic databases were searched from inception to 1 September 2023: Embase (via Elsevier), Cumulative Index to Nursing and Allied Health Literature (CINAHL) Complete (via EBSCOhost), PubMed (via the National Library of Medicine), Medline (via EBSCOhost) and Scopus (via Elsevier). Supplemental Appendix 1 details the search strategies employed. Search terms were structured around the central concepts of ‘patient experience’, ‘mental health’ and ‘emergency department’. Medical Subject Headings (MeSH) and key word searches were used, as were Boolean operators (e.g. AND, OR) and proximity searching.
Steps 4 and 5: identify and select potentially relevant studies
Results were exported from electronic databases and imported into Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia). All duplicate records were automatically removed upon import. Two authors (C.B. and J.Y.G.) undertook title and abstract screening, and full-text screening. Where there was ambiguity around the inclusion of an article, the two authors reached a consensus-based decision on inclusion. Where consensus could not be reached, N.W. was consulted to make the final decision. The reference lists of included articles were hand-searched by C.B. to identify additionally relevant studies for inclusion.
Step 6: appraise the quality of included studies
To evaluate the quality of the included studies in the SMSR, we used the 2018 version of the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018). The MMAT appraises five different types of research design, including qualitative research, randomised controlled trials, non-randomised studies, quantitative descriptive studies and mixed-methods studies. Each research design is appraised against two screening questions and five methodological questions. Responses are either ‘yes’, ‘no’ or ‘can’t tell’. To ensure consistency and reliability in our approach, two authors (C.B. and J.Y.G.) independently appraised the included studies using MMAT. Discrepancies that arose were discussed between the two authors and resolved through consensus-based decision-making. As per MMAT scoring guidance, quality appraisal of each study was described in table form; an overall score was not calculated (Hong et al., 2018).
Step 7: synthesise included studies
Data extraction was undertaken by C.B. and J.Y.G. with each cross-checking the others’ extraction for accuracy and comprehensiveness. Using a bespoke data extraction template, the following information was extracted from the included studies:
Publication details including title; author names; publication year; and the country where research was conducted.
Study details including aims/objectives; study design; definitions or frameworks of service user experience underpinning the study design (if applicable); study population, intervention control and outcomes (PICO, if applicable); and the methods/instruments used to investigate mental health experiences.
Study sample characteristics including a general sample description; sample size and response rate (if applicable); and the mental health condition under investigation/reason for ED presentation.
Study findings (this was dependent on the study design, i.e., verbatim themes and subthemes were extracted from qualitative studies, whereas survey domains and associated quantitative results were extracted from quantitative survey studies).
To synthesise the findings of all included studies, a convergent qualitative thematic approach was employed (Pluye and Hong, 2014). This type of results synthesis addresses research questions such as what, how and why by transforming data from identified studies – be they qualitative, quantitative or mixed methods in design – into qualitative findings such as themes (Pluye and Hong, 2014). Qualitative transformation of study findings occurred during the first phase of data coding. Using the Thomas and Harden (2008) thematic synthesis approach, qualitative data were then developed into descriptive subthemes and themes to describe mental health patient experiences in the ED. This entailed line-by-line coding using NVivo 14 (QSR International, 1999–2023), followed by organising codes into groups, and subsequently the development of descriptive subthemes and themes. This process was led by C.B. and reviewed by the co-author team.
Results
Figure 1 illustrates that there were 1885 studies identified through electronic databases and an additional two through handsearching reference lists. After the removal of duplicates, and title and abstract screening, 45 studies underwent full-text review. Of these, 16 studies were included. Supplemental Appendix 2 details the studies excluded with reasons. Nearly all studies (14/16, 87.5%) were of qualitative design and semi-structured interviews were employed most frequently (10/14, 71.4%). Over one-third (6/16, 37.5%) of the included studies were conducted in Canada. The most common reasons for ED presentation included opioid use disorder (OUD), self-harm and severe mental illnesses. A description of each study is provided in Table 2.
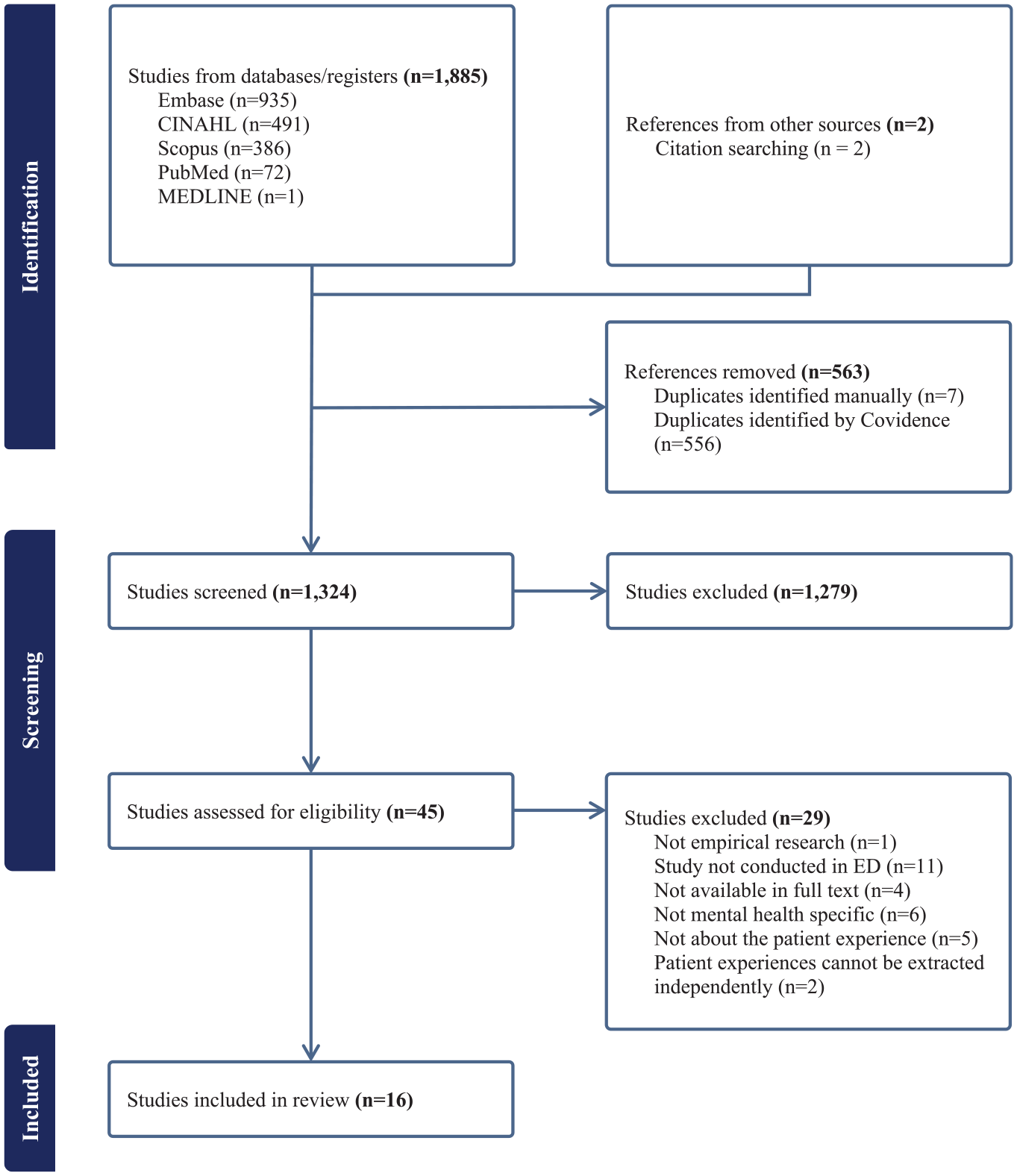
PRISMA flow diagram.
Details of the included studies.
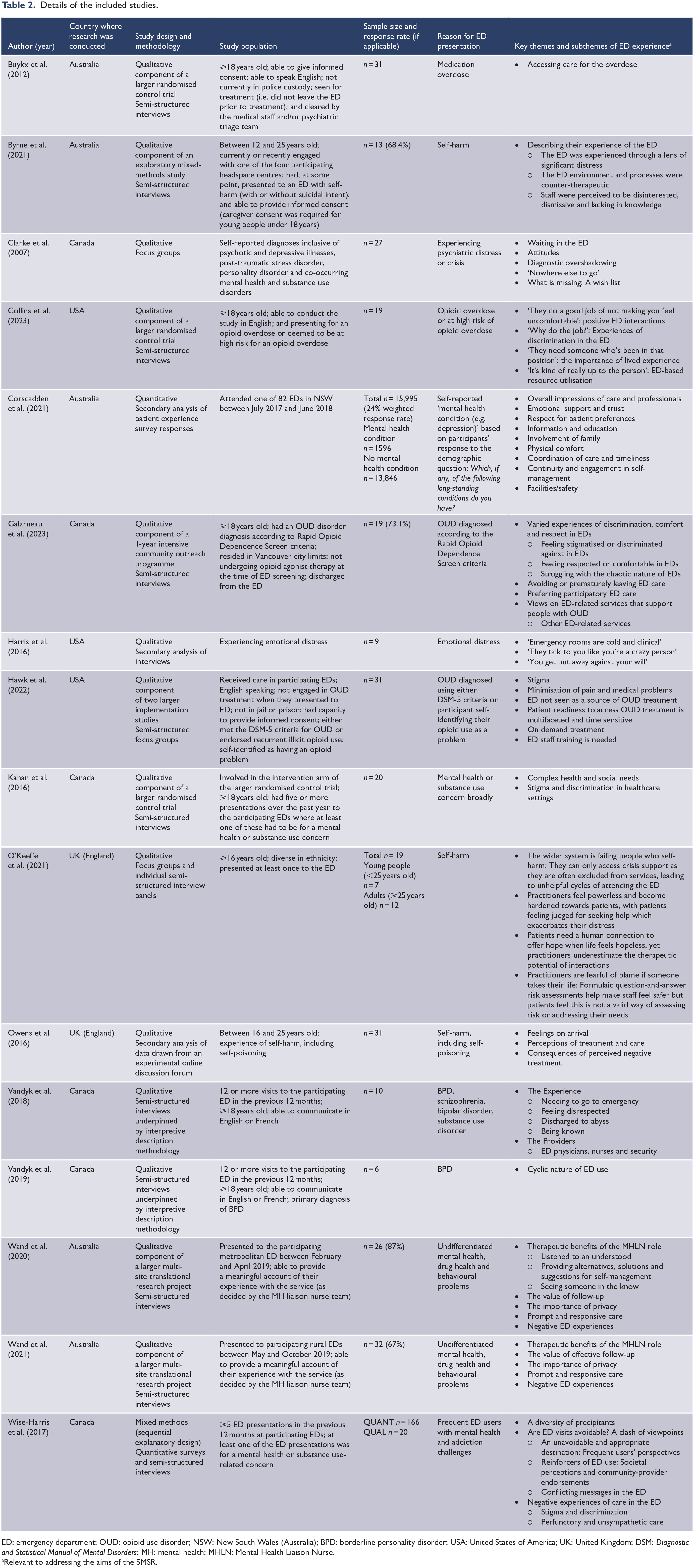
ED: emergency department; OUD: opioid use disorder; NSW: New South Wales (Australia); BPD: borderline personality disorder; USA: United States of America; UK: United Kingdom; DSM: Diagnostic and Statistical Manual of Mental Disorders; MH: mental health; MHLN: Mental Health Liaison Nurse.
Relevant to addressing the aims of the SMSR.
Supplemental Appendix 3 provides the MMAT results. Overall, most qualitative studies were appraised as high quality. There were only two studies where it was difficult to discern whether: (1) the findings were adequately derived from the data; (2) the interpretation of the results was sufficiently substantiated by data; and (3) there was coherence between qualitative data sources, collections, analysis and interpretation (Buykx et al., 2012; Clarke et al., 2007). The single quantitative descriptive study was appraised as high quality (Corscadden et al., 2021). The single mixed-methods study was appraised moderately as there was no apparent rationale for using this study design, nor were we able to confidently suggest that both the comprising qualitative and quantitative components adhered to their respective appraisal criteria (Wise-Harris et al., 2017).
Thematic synthesis results
ED staff can make-or-break an ED experience
It was clear in all studies that the way individuals presenting for mental health reasons were treated by ED staff was the most important determinant of a positive or negative experience. When shown genuine care and concern, individuals were put at ease and ‘actually believe[d] that things would be okay’ (Byrne et al., 2021). When treated in a cold and unempathetic manner, individuals felt stigmatised, shameful and burdensome on ED staff and the others around them. The dismissal of their complex mental health issues and life situations led several to believe that the next time they attempted suicide or self-harm, a fatal outcome or more serious injury was necessary to convey that their distress warranted attention (Table 3) (Byrne et al., 2021; Owens et al., 2016; Vandyk et al., 2018; Wand et al., 2020).
Quotes supporting the theme and subthemes of ED can make-or-break an ED experience.
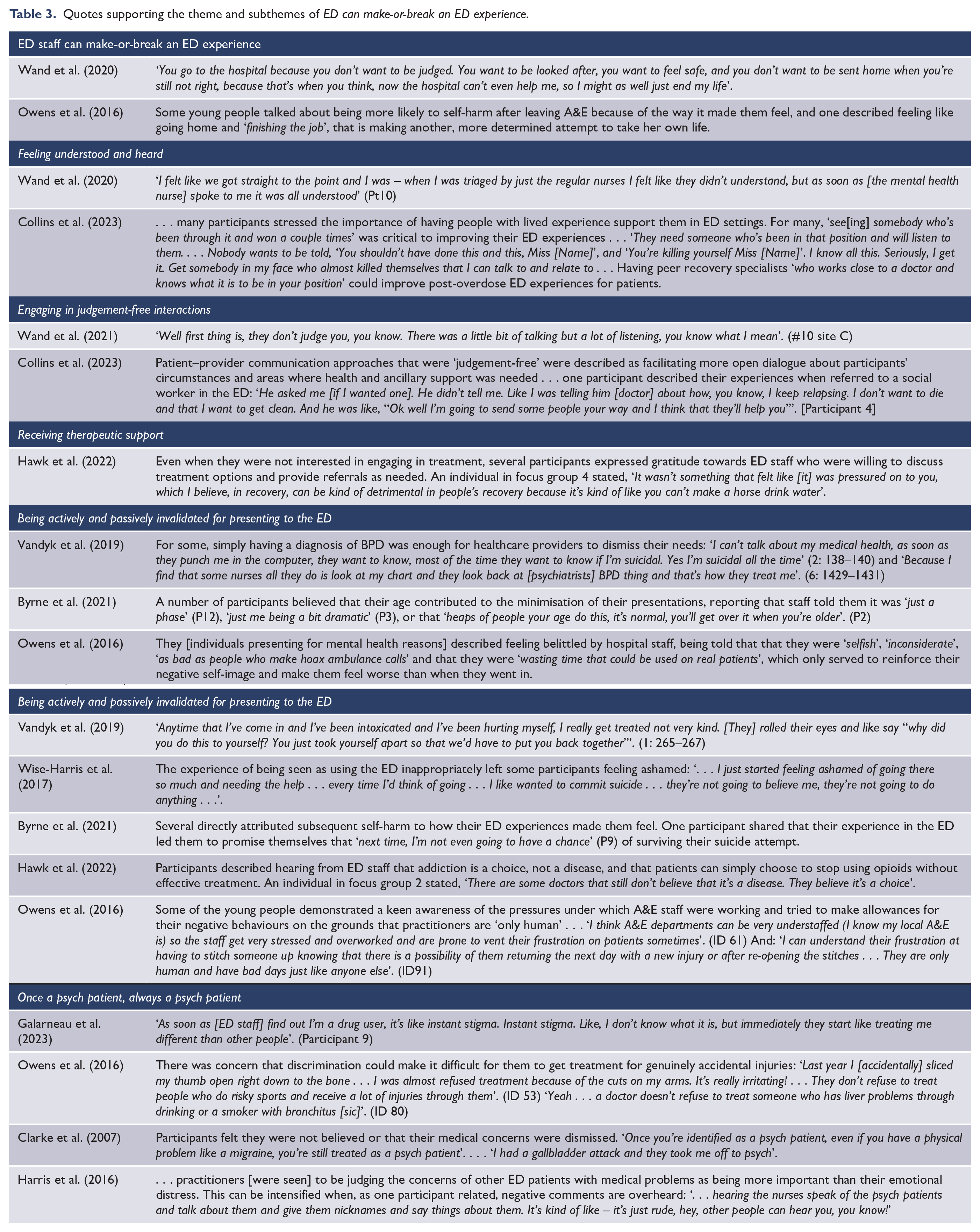
This overarching theme was further explored through the following positive and negative experiential subthemes. Positive subthemes included: (1) ‘Feeling understood and heard’, (2) ‘Engaging in judgement-free interactions’ and (3) ‘Receiving therapeutic support’. Negative subthemes included: (1) ‘Being actively and passively invalidated for presenting to the ED’ and (2) ‘Once a psych patient, always a psych patient’.
Feeling understood and heard
Individuals presenting for mental health reasons noted that they felt understood and heard particularly when engaging with specialist mental care practitioners, lived experienced workers and peer recovery workers in the ED. This was because their interactions with these providers were personalised and considerate of their overall life circumstances (e.g. housing, criminal history, trauma) (Vandyk et al., 2018; Wand et al., 2021). Patients felt that due to their lived experience or specialist training, these care providers really understood them, were easier to talk to than non-specialist care providers, and treated them with respect and an appreciation for what they were going through (Table 3) (Collins et al., 2023; Wand et al., 2020, 2021).
While considering conversations with specialist providers and workers particularly ‘meaningful’ (O’Keeffe et al., 2021), some non-specialist ED nurses and doctors also made individuals presenting for mental health reasons feel safe, reassured and cared for by giving them time of day (Byrne et al., 2021; Galarneau et al., 2023; Hawk et al., 2022).
Engaging in judgement-free interactions
Few individuals presenting for mental health reasons described judgement-free interactions with ED staff where they did not feel stigmatised. Indeed, they were shown ‘empathy, compassion and reassurance that it was right to seek help’ in ED (O’Keeffe et al., 2021). Again, this type of experience was more common when individuals engaged with specialist mental care practitioners, lived experienced workers and peer recovery workers (Table 3) (Collins et al., 2023; Wand et al., 2020, 2021).
Judgement-free interactions allowed individuals to feel safe in the ED and reinforced a sense of agency in their care (Collins et al., 2023; Galarneau et al., 2023).
Receiving therapeutic support
Individuals presenting for mental health reasons felt therapeutically supported in the ED when they received ‘the care they were seeking’, adequate psychological and physical comfort, and personalised mental health support (Galarneau et al., 2023; Owens et al., 2016; Vandyk et al., 2018). Examples of ‘good practice’ were described as: . . . asking before taking blood ‘because the process is triggering for some people’; not requiring them to roll up sleeves when having blood pressure taken ‘because she was sensitive to the fact that I probably didn’t want to have scars showing’; asking whether the patient was comfortable with a doctor of the opposite sex; chatting with them in a relaxed way about ‘random stuff’ as well as about their emotional well-being . . . (Owens et al., 2016)
Many people highlighted that the personalised nature of this type of care allowed for more collaborative discussions about their treatment options where they felt like an active participant (Galarneau et al., 2023; Hawk et al., 2022; Vandyk et al., 2018). They also described not feeling rushed or pressured by ED care providers to engage in treatment, particularly if this was not something they were ready to undertake (Table 3).
Being actively and passively invalidated for presenting to the ED
The legitimacy of individuals’ reasons for presenting to ED were often actively brought into question by ED staff (Table 3). In particular, people with borderline personality disorder (BPD), trauma histories, substance abuse disorders and self-harm were most likely to feel unwelcome as these were ‘not perceived as legitimate reason[s] to attend the emergency department’ (Clarke et al., 2007; Corscadden et al., 2021; O’Keeffe et al., 2021; Owens et al., 2016; Vandyk et al., 2019; Wise-Harris et al., 2017). In addition, people presenting with self-harm injuries were told that they were ‘not that bad’ or that their injuries were ‘just superficial’ (Byrne et al., 2021). Young people were particularly targeted by this mentality (Table 3) (Byrne et al., 2021).
Other individuals described more veiled invalidation approaches by staff. In particular, being triaged as low priority, being left to wait for hours in the waiting room and being left alone in a room without anyone checking in on them (Byrne et al., 2021; Clarke et al., 2007; Wand et al., 2021). Not only did these responses leave people feeling ‘abandoned’, ‘not worthy of attention’ and as though they were ‘not a priority’ (Clarke et al., 2007), but it also gave them the opportunity to continue engaging in self-harm in the ED (Byrne et al., 2021; Owens et al., 2016).
Having the legitimacy of their ED presentation questioned left individuals presenting for mental health reasons feeling guilty and like a burden to ED staff, other patients and society more broadly. They were made to feel that they were wasting everyone’s time, ‘wasting taxpayers’ money’ and ‘wasting a bed’ (Table 3) (Byrne et al., 2021).
Ultimately, being invalidated exacerbated individuals’ feelings of self-loathing, shame, embarrassment and worthlessness (Byrne et al., 2021; O’Keeffe et al., 2021; Owens et al., 2016; Vandyk et al., 2019; Wise-Harris et al., 2017). Being treated this way deterred them from wanting to seek help in the future and encouraged them to double-down on their attempts to self-harm and take their own lives (Table 3) (Byrne et al., 2021; Owens et al., 2016; Vandyk et al., 2018; Wand et al., 2020).
Some individuals suggested that ED staffs’ negative attitudes towards them was propagated by a lack of mental health training and awareness (Clarke et al., 2007; Hawk et al., 2022; Vandyk et al., 2018; Wand et al., 2021). Others recognised that the busyness of EDs, the pressures on staff, and staff powerlessness to change an under-resourced system were also likely contributors to this negative attitude (Table 3) (Byrne et al., 2021; Galarneau et al., 2023; O’Keeffe et al., 2021; Owens et al., 2016; Wand et al., 2020, 2021).
Once a psych patient, always a psych patient
Many individuals presenting to ED with mental health concerns described feeling stigmatised and judged by ED staff due to having a mental illness. Even when presenting to ED for physical problems, they felt unfairly discriminated against and believed they received slower and poorer care than other patients (Table 3) (Clarke et al., 2007; Galarneau et al., 2023; Owens et al., 2016).
Some individuals – particularly those who presented to ED after attempting suicide and with substance use disorders – also reported interactions where they were treated as less than human (Clarke et al., 2007; Harris et al., 2016; Wand et al., 2020). Minimal eye contact, staff failing to ask them how they were feeling and being held against their will were all examples of the stigma these individuals felt as a consequence of having a mental illness (Harris et al., 2016).
Derogatory name calling was another form of stigma experienced. Individuals presenting for mental health reasons described how ED staff would use the following nicknames to refer to them: ‘frequent flyer’ (O’Keeffe et al., 2021; Vandyk et al., 2018); ‘the attention-seeking type, the dramatic type, the crazy one’ (O’Keeffe et al., 2021); ‘drug seeker’ (Hawk et al., 2022); ‘dope fiend’ (Hawk et al., 2022); and ‘psych case’ (Table 3) (Wise-Harris et al., 2017).
Stigmatising experiences led individuals to feel they ‘need[ed] to calculate carefully what they say and do not say’ to avoid disclosing their previous mental illness history, despite the medical risks that could potentially arise when omitting this information (Clarke et al., 2007; Collins et al., 2023; Harris et al., 2016).
Being in the ED environment is counter-therapeutic
The ED environment was described by many individuals as ‘scary’ (Byrne et al., 2021; Harris et al., 2016; Wand et al., 2020), ‘frightening’ (Buykx et al., 2012; Clarke et al., 2007; Harris et al., 2016), ‘overstimulating’ (Clarke et al., 2007), ‘chaotic’ (Galarneau et al., 2023; Harris et al., 2016; O’Keeffe et al., 2021) and ‘unwelcoming’ (Galarneau et al., 2023). They noted how the bright lights (Byrne et al., 2021; Harris et al., 2016), loud noises (Byrne et al., 2021; Harris et al., 2016) and ‘smothery-like’ smells (Harris et al., 2016) of the ED intensified their existing distress and anxiety. The situation was further complicated by their vulnerable emotional state and the means of self-harm they had engaged in (e.g. attempted substance overdose) (Table 4) (Byrne et al., 2021; Harris et al., 2016).
Quotes supporting the theme and subthemes of Being in the ED environment is counter-therapeutic.
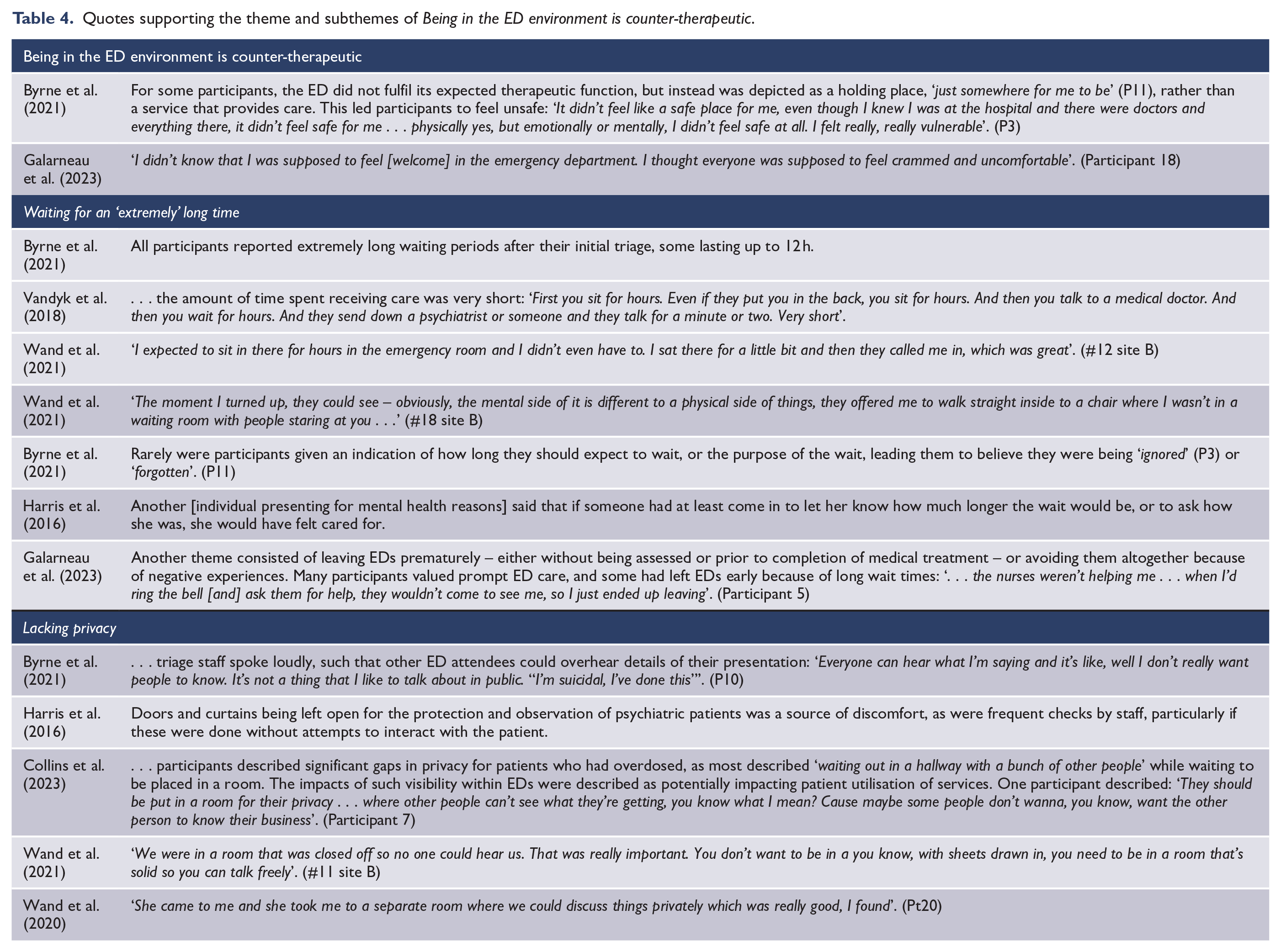
This overarching theme is further explored through the following subthemes: (1) ‘Waiting for an “extremely” long time’ and (2) ‘Lacking privacy’.
Waiting for an ‘extremely’ long time
The counter-therapeutic nature of the ED environment was reinforced in how long individuals presenting for mental health reasons spent waiting. First in the waiting room, then waiting to talk to care providers, and finally, waiting to be admitted or discharged (Clarke et al., 2007; O’Keeffe et al., 2021; Wand et al., 2020). This exacerbated their feelings of distress and gave them an opportunity to ‘think the worst things’ (Table 4) (Harris et al., 2016).
The only time individuals presenting for mental health reasons described prompt responses after triage was when mental health liaison nurses were involved in their care (Table 4) (Wand et al., 2020, 2021).
Individuals also described feeling forgotten about when they were not informed about how long they might be waiting (Table 4) (Byrne et al., 2021; Harris et al., 2016; Wise-Harris et al., 2017). As a result of long waits, several people described simply giving up and leaving ED without being seen or prior to the completion of their medical treatment (Clarke et al., 2007; Galarneau et al., 2023; Wise-Harris et al., 2017). Such experiences deterred them from wanting to seek help in the future (Table 4) (Byrne et al., 2021; Collins et al., 2023; Galarneau et al., 2023).
Lacking privacy
Further adding to peoples’ distress was the lack of privacy afforded to them in the ED, particularly in the waiting room. There were two key facets to this: (1) the lack of privacy experienced when disclosing information to staff (Byrne et al., 2021; Galarneau et al., 2023; Wand et al., 2020, 2021) and (2) the lack of spatial privacy (Collins et al., 2023; Corscadden et al., 2021; Galarneau et al., 2023; Harris et al., 2016; Wand et al., 2020). Individuals presenting for mental health reasons recounted how triage nurses spoke loudly, allowing other patients to overhear the details of their presentation. Some highlighted that, as it was, telling staff their story was inherently hard and scary (Byrne et al., 2021; Harris et al., 2016; O’Keeffe et al., 2021). Not only because of how emotionally distressing it was for themselves (i.e. to acknowledge that they had tried to kill themselves) (Byrne et al., 2021; Hawk et al., 2022), but also because of their previous experiences in ED and other healthcare settings where this type of information typically caused a stigmatising, discriminatory or unhelpful response (Byrne et al., 2021; Galarneau et al., 2023; Kahan et al., 2016; Vandyk et al., 2018). Add in the lack of privacy afforded by the ED environment, and several individuals found the whole experience detrimental to their already fragile mental state.
In the few instances where privacy was prioritised by care providers, individuals presenting for mental health reasons recognised how important this was for them, as it enabled them to engage in free and unfiltered conversation with their care providers (Wand et al., 2020, 2021). It also promoted feelings of calm and reassurance. However, this was only reported in studies where mental health liaison nurses were involved in the care process (Table 4) (Wand et al., 2020, 2021).
Having nowhere else to go
This final theme describes how people with mental health problems presented to the ED because they felt they had nowhere else to go. This was attributed to the time of day they needed help (e.g. weeknights and weekends); a lack of alternative and accessible community support services, including where the wait list was too long (i.e. there was no immediate capacity to help them); and lacking familial and social structures that could help them in times of crisis (Clarke et al., 2007; Hawk et al., 2022; O’Keeffe et al., 2021; Vandyk et al., 2018; Wise-Harris et al., 2017). When in crisis, these individuals said that presenting to ED was unavoidable and necessary (Table 5).
Quotes supporting the theme Having nowhere else to go.
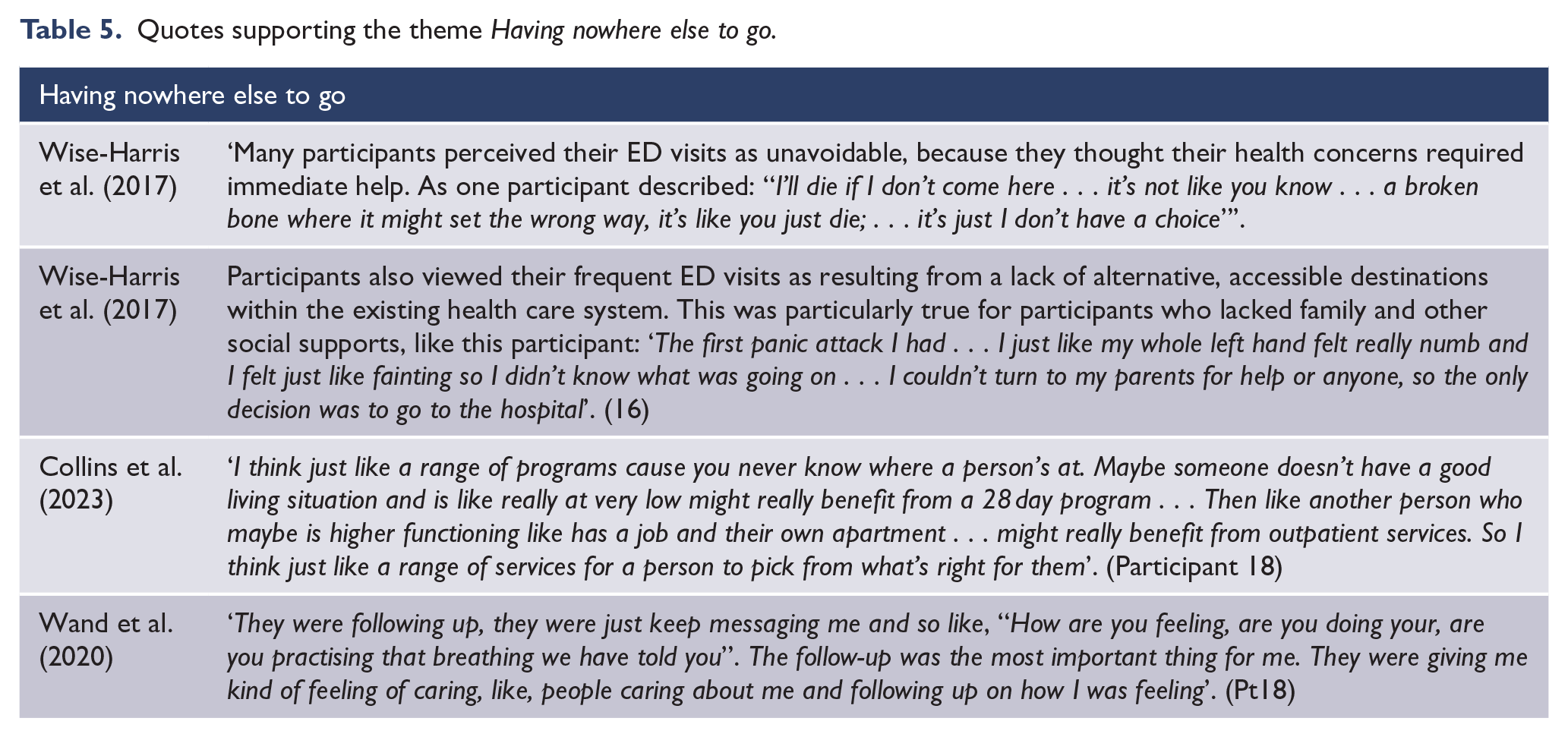
They also described re-presenting to ED because the referrals to support they received were not useful or missing altogether. Some individuals described receiving a ‘. . . “sheet of paper” which often contained outdated or unhelpful information, programs that did not match [their] needs, or were inaccessible to patients based on insurance status or waitlists’ (Hawk et al., 2022). In their quantitative cross-sectional survey study, Corscadden et al. (2021) reported that only 60% of people presenting to ED with mental health conditions reported ‘definitely’ receiving enough information to manage their care outside of the ED. Indeed, people described needing more guidance on how to access follow-up care (Hawk et al., 2022), and more options for community services because a ‘one-size-fits-all approach’ fails to recognise the expansive complexity of their lives (Table 5) (Collins et al., 2023).
While the ED was not a supportive gateway to long-term mental healthcare for most, there was a great appreciation among several individuals for the follow-up phone calls, texts and emails they received after being discharged from ED (Byrne et al., 2021; Wand et al., 2020, 2021). The gestures were viewed as supportive and encouraging, and provided an opportunity for their care providers to reiterate strategies and suggestions discussed in the ED (Table 5) (Wand et al., 2020).
Discussion
The aim of this SMSR was to systematically review literature relating to the experiences of individuals presenting to ED for mental health reasons. Our results described three main themes: ED staff can make-or-break an ED experience; Being in the ED environment is counter-therapeutic; and Having nowhere else to go. The results show that though some ED care providers were respectful and supportive of individuals presenting in acute mental health crisis – particularly those with lived experience or specialist training – the overwhelming majority of individuals reported experiences characterised by stigma, judgement and invalidation. Moreover, the ED was described as unwelcoming, unsafe and therapeutically hostile, but tended to be the only option for many individuals due to a lack of alternative community and social support services. Albeit considering the views of heterogeneous population groups and contexts, these results illustrate several generalisable areas for enhancing the treatment of people with mental illness in the ED.
The current SMSR illustrates overlapping and disparate ED experiences to previous research in more ‘generic’ adult populations (without mental health conditions) (Bull et al., 2021). A 2021 review described two overarching and interrelated experiential themes: Relationships between ED patients and care providers and Spending time in the ED environment (Bull et al., 2021). Relational power imbalances were described by many people who felt they had to compete for care providers’ time by adopting passive and compliant behaviours (Bull et al., 2021). Relational imbalances were also evident in the current review, but were distinctively illustrative of epistemic injustice; the injustice that occurs when an individual’s authority as a ‘knower’ through life experience is ignored, dismissed or doubted due to prejudice (Fisher, 2023). This was particularly noted by individuals who described having the validity of their presentation questioned by care providers and consistently being stigmatised as a ‘psych case’ even when presenting for a physical problem. Despite significant shifts in society’s attitudes towards talking about and supporting mental health (NRS Healthcare, 2019; Venters, 2018), the current review suggests that discriminatory treatment of people with mental illnesses is still common in EDs.
Staff cite that a combination of departmental and hospital-wide issues, as well as negative individual attitudes, contribute to the epistemic injustice individuals with mental illness face in the ED (Koning et al., 2018; McHale and Felton, 2010; Pawaskar et al., 2022; Rayner et al., 2019). A lack of education about mental health, particularly self-harm and substance abuse, is also a large contributor (Hsiao et al., 2015; Koning et al., 2018; McHale and Felton, 2010; Pawaskar et al., 2022; Rayner et al., 2019). ED staff describe the challenges of caring for people with mental health needs in the ED because some individuals display aggressive behaviours which can provoke fear and anger responses from ED staff, and many will re-present leading to a sense of hopelessness and a ‘why bother’ attitude (Clarke et al., 2014). In addition, some ED staff view individuals presenting with mental health issues as manipulative and ingenuine, reducing their desire to want to help them (Clarke et al., 2014). At the opposite end of the spectrum, knowledge about mental illness and a focus on therapeutic relationships supports positive attitudes towards individuals with mental illness (McHale and Felton, 2010). Growth in the lived experience and peer recovery workforces have also improved attitudes towards this group of ED users (Byrne et al., 2019; Carstensen et al., 2017; Sacre et al., 2022). In the current review and other research, the value of mental health clinical liaison nurses in ED has been highlighted; both from the perspective of improving users’ experiences, and supporting flow and efficiency by providing timely, specialist mental health support (Brinkman et al., 2009; Burian et al., 2014; Carstensen et al., 2017; Sacre et al., 2022; Sinclair et al., 2006). Thus, there is a clear need for increased mental health education and training for all ED staff, as well as the employment of specialist and lived experience workers to foster more therapeutic relationships and ED environments. In addition, a greater understanding of the factors that influence staff attitudes (both positive and negative) towards people presenting to ED for mental health reasons is needed, particularly through a lens of moral psychology to clarify psychological processes underlying the judgements, attitudes and behaviours ED staff exhibit towards individuals with mental illness.
The poor experiences described in this review are not exclusively a consequence of negative staff attitudes. It is important to recognise the systemic challenges that EDs and mental healthcare systems the world over are facing, which, in turn, impact on the user experience. EDs are increasingly overcrowded (Attwooll, 2022; Kelen et al., 2021; Savioli et al., 2022); the workforce is quickly becoming burnt out and demoralised (Elder et al., 2020); and dated funding mechanisms mean services are required to do more with less (Kelen et al., 2021; Turner et al., 2020). Moreover, patients face longer waits and ED lengths of stay; particularly individuals presenting for mental health reasons (Brazel et al., 2023; Duggan et al., 2020; Royal College of Emergency Medicine, 2022). Yet, the availability of other services to support individuals in mental health crisis are limited. For example, a 2022 Australian study examining wait times for community-based treatment of anxiety and depression in adolescents showed that the median wait time for treatment with a psychologist was 91.3 days, and 124 days for a psychiatrist (Subotic-Kerry et al., 2023). Similar findings have been echoed in the United Kingdom (Frith, 2017) and the United States (Sun et al., 2023). Moreover, while crisis line services (e.g. call, text and chat) are readily available to most people, systematic review evidence suggests they have limited effectiveness (Hoffberg et al., 2019). While the Nordic countries have been widely praised for the sustainability of their universal mental healthcare systems and 30-day wait time targets (Nordentoft et al., 2022; Organisation for Economic Cooperation and Development, 2021), it is clear that greater funding across other countries is required to boost current, inefficient systems (Duggan et al., 2020; Organisation for Economic Cooperation and Development, 2021). That is, funding will need to focus on both the backlog of individuals who need mental health support immediately, and ensure system sustainability into the future for the growing number of individuals with mental illness.
Limitations
This review has some limitations. First, despite systematic searching of numerous electronic databases supplemented by reference list handsearching, some studies may have been missed. Second, grey sources of literature were not included due to their potential risk of bias. Finally, the experiences of marginalised and disadvantaged populations were poorly represented in the current review due to the dearth of literature related to these individuals. Thus, the conceptual understanding of mental health ED experiences derived from the current evidence base needs to be considered in light of this limitation.
Conclusion
This SMSR described the experiences of individuals presenting to ED for mental health reasons as generally poor. While some individuals reported experiences where their engagement with care providers was judgement-free and they felt understood and heard, most described being actively and passively invalidated for presenting to the ED. Indeed, poor experiences were characterised by stigma and discrimination. The ED environment itself was unwelcoming and left some individuals feeling unsafe. However, it was often also recognised as the only place for people to go, due to a lack of accessible community and social supports. Based on these findings, several recommendations have been posited: first, increased mental health education and training for all ED staff; second, employment of specialist and lived experience workers to support more therapeutic relationships and ED environments; and finally, greater investment in mental healthcare systems globally to ensure sustainability into the future.
Supplemental Material
sj-docx-1-anp-10.1177_00048674241259918 – Supplemental material for Experiences of individuals presenting to the emergency department for mental health reasons: A systematic mixed studies review
Supplemental material, sj-docx-1-anp-10.1177_00048674241259918 for Experiences of individuals presenting to the emergency department for mental health reasons: A systematic mixed studies review by Claudia Bull, Jia Yin Goh, Nicola Warren and Steve Kisely in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-2-anp-10.1177_00048674241259918 – Supplemental material for Experiences of individuals presenting to the emergency department for mental health reasons: A systematic mixed studies review
Supplemental material, sj-docx-2-anp-10.1177_00048674241259918 for Experiences of individuals presenting to the emergency department for mental health reasons: A systematic mixed studies review by Claudia Bull, Jia Yin Goh, Nicola Warren and Steve Kisely in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-3-anp-10.1177_00048674241259918 – Supplemental material for Experiences of individuals presenting to the emergency department for mental health reasons: A systematic mixed studies review
Supplemental material, sj-docx-3-anp-10.1177_00048674241259918 for Experiences of individuals presenting to the emergency department for mental health reasons: A systematic mixed studies review by Claudia Bull, Jia Yin Goh, Nicola Warren and Steve Kisely in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: N.W. is an Associate Editor for ANZJP. N.W. and S.K. are on the Advisory Board for ANZJP. C.B. and J.Y.G. declare no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: C.B. was funded by an NHMRC Special Initiative in Mental Health Grant (GNT2002047).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.