
Abstract
Objective:
To systematically investigate the scope and nature of discrimination and positive treatment experienced by adults with mental health problems when using health services in an Australian population-based survey.
Methods:
Australian adults (n = 1381) who reported a mental health problem or scored high on a screening questionnaire were interviewed about their experience of discrimination and positive treatment from healthcare professionals. Descriptions of experiences were content-analysed to identify key characteristics.
Results:
In all, 11.8% of respondents reported discrimination from a health professional in the past 12 months. The most common types of discrimination included being treated dismissively, being judged and not being listened to, particularly regarding personal history and treatment needs. In contrast, 40.4% reported being treated more positively by their health professional because of their mental health problem. Key types of positive treatment by health professionals were being supportive and understanding and being a good listener. Good quality care approaches were also appreciated, including making a referral, being engaged in the treatment process, regularly checking the status of the person’s mental health and providing information.
Conclusion:
A minority of respondents with mental health problems had experienced discrimination from their healthcare professional, potentially interfering with recovery. Anti-stigma education interventions for healthcare professionals should address how to increase knowledge and understanding of mental health problems, reduce negative attitudes and encourage supportive behaviours.
Background
Mental health stigma is a complex concept and can be conceptualised as including three components: ignorance or misinformation, negative attitudes or prejudice, and negative behaviours or discrimination (Thornicroft et al., 2007). Stigma and discrimination disadvantage people with mental health problems in many areas of life by reducing opportunities for employment and safe housing, impeding treatment seeking and adherence, interfering with self-esteem and personal relationships and increasing risk of suicide (Clement et al., 2015; Corrigan, 2004; Livingston and Boyd, 2010; Pompili et al., 2003).
It would seem reasonable to assume that health professionals hold non-stigmatising attitudes, as they have elected to care for people with mental health problems and possess greater knowledge and familiarity. A review of 19 studies found that the majority of mental health professionals have positive attitudes and hold less stigmatising views than members of the public (Wahl and Aroesty-Cohen, 2010). However, some studies have found predominantly negative attitudes among professionals, and even in studies where the majority had positive attitudes, there were still substantial minorities holding stigmatising views. These views tended to relate to pessimism about treatment and recovery, the belief in dangerousness or unpredictability and the desire for social distance (e.g. reluctance to live next door to someone with a mental health problem or have them marry into the family). Most research has focused on schizophrenia and severe mental illness, and interpreting the research literature is complicated by the multi-dimensional nature of stigma (Yap et al., 2014) and different findings across types of professions and mental health problems. For example, research with Australian health professionals found that general practitioners (GPs) held more stigmatising views than psychiatrists or psychologists, and stigma was higher for schizophrenia than for depression or anxiety disorders (Reavley et al., 2014).
Evidence of stigmatising attitudes among health professionals is supported by research that directly asks consumers about their experience in the healthcare system. Surveys of mental health service users consistently show a significant minority reporting discrimination from healthcare professionals. International studies using the Discrimination and Stigma Scale (DISC) show substantive rates of discrimination by mental health staff: 19% (depression, Lasalvia et al., 2013), 34% (mix of disorders, Corker et al., 2013; Thornicroft et al., 2014) and 39% (schizophrenia, Harangozo et al., 2014). Discrimination related to people with mental health problems getting help for a physical health problem ranges from 17% (depression, Lasalvia et al., 2013; schizophrenia, Harangozo et al., 2014) to 26–30% (mix of disorders, Corker et al., 2013; Thornicroft et al., 2014). Surveys of mental health consumers in Australia also show significant stigma and discrimination among health professionals (Mental Health Council of Australia [MHCA], 2011). Nearly one-third reported being shunned or avoided, and one-fifth believed that they had been treated unfairly by their health professional. This discrimination tended to be higher in those with diagnoses of borderline personality disorder, post-traumatic stress disorder (PTSD) or schizophrenia.
Despite an increased research focus on consumer reports of discrimination rather than the attitudes of health professionals, there are a limited number of studies that report in-depth information about the types of discrimination experienced in healthcare settings. A review of qualitative studies investigating stigma experienced by patients with schizophrenia found that stigma in the healthcare system was a major theme across studies (Mestdagh and Hansen, 2014). Common stigmatising experiences included not being treated with respect, not receiving information about potential treatments and exclusion from taking part in treatment decisions, being treated in a paternalistic or overprotective manner and having physical health problems ignored or dismissed. Structural discrimination experiences included inadequate mental health treatment facilities that had an impersonal focus on efficiency and a lack of continuity of care across services. Among those with borderline personality disorder, common experiences of discrimination by health professionals include having diagnoses and treatment withheld and experiencing psychological abuse (Bonnington and Rose, 2014).
A major limitation of the existing literature is that it has predominantly employed samples of convenience and clinical populations that may not be representative, potentially biasing estimates of discrimination. No population-based studies have systematically reported on the nature of discrimination by health professionals across a range of mental health problems. Nor has there been much investigation into the types of experiences people with mental health problems experience as positive interactions with health professionals. This is an important research gap as positive relationships with health professionals are highly valued, can reduce the experience of stigma and help build confidence and encourage recovery (Knox et al., 2014; Mestdagh and Hansen, 2014). Therefore, the aim of this study was to investigate the prevalence and explore the nature of discrimination and positive treatment experienced by adults with mental health problems when using health services, in a national population-based survey.
Methods
The data in this paper are part of a larger study surveying Australians with mental health problems about their personal experiences of discrimination in a variety of domains (e.g. friends, family, the workplace and health care) as well as observed discrimination against other adults with a mental health problem. For detailed survey methodology, see Reavley and Jorm (2015). Briefly, the survey involved computer-assisted telephone interviews (CATIs) with a national sample of 5220 members of the general community aged 18 years and over. The sample was contacted by random-digit dialling of both landlines and mobile phones. Interviews were conducted between October and December 2014 by the Social Research Centre survey company. Ethical approval was obtained from the University of Melbourne Human Research Ethics Committee.
Survey interview
Figure 1 provides an overview of the process of sampling and case selection for interview. Initial questions covered socio-demographic information, including age, gender, marital status, postcode, country of birth, language spoken at home, level of education and Aboriginal and Torres Strait Islander status. Respondents completed the 12-month version of the Kessler 6 (K6) mental health symptom screening questionnaire (Kessler et al., 2010) and were asked whether they had experienced any sort of mental health problem in the last 12 months. Respondents who answered ‘yes’ to this question were then asked what they thought the problem was. For the purposes of this study, respondents were considered to have a mental health problem if they either scored in the high range on the K6 (⩾19) or specified any of the following mental health problems: depression/major depression, attempted suicide or self-harm, anxiety/anxiety disorder, PTSD, agoraphobia, panic disorder, obsessive–compulsive disorder (OCD), social phobia, generalised anxiety disorder (GAD), eating disorder/anorexia/bulimia, schizophrenia/paranoid schizophrenia, schizoaffective disorder, psychosis/psychotic, bipolar/bipolar disorder/manic-depressive disorder, mental illness, personality disorder/borderline personality disorder, attention-deficit hyperactivity disorder (ADHD), autism/Asperger’s and nervous breakdown.
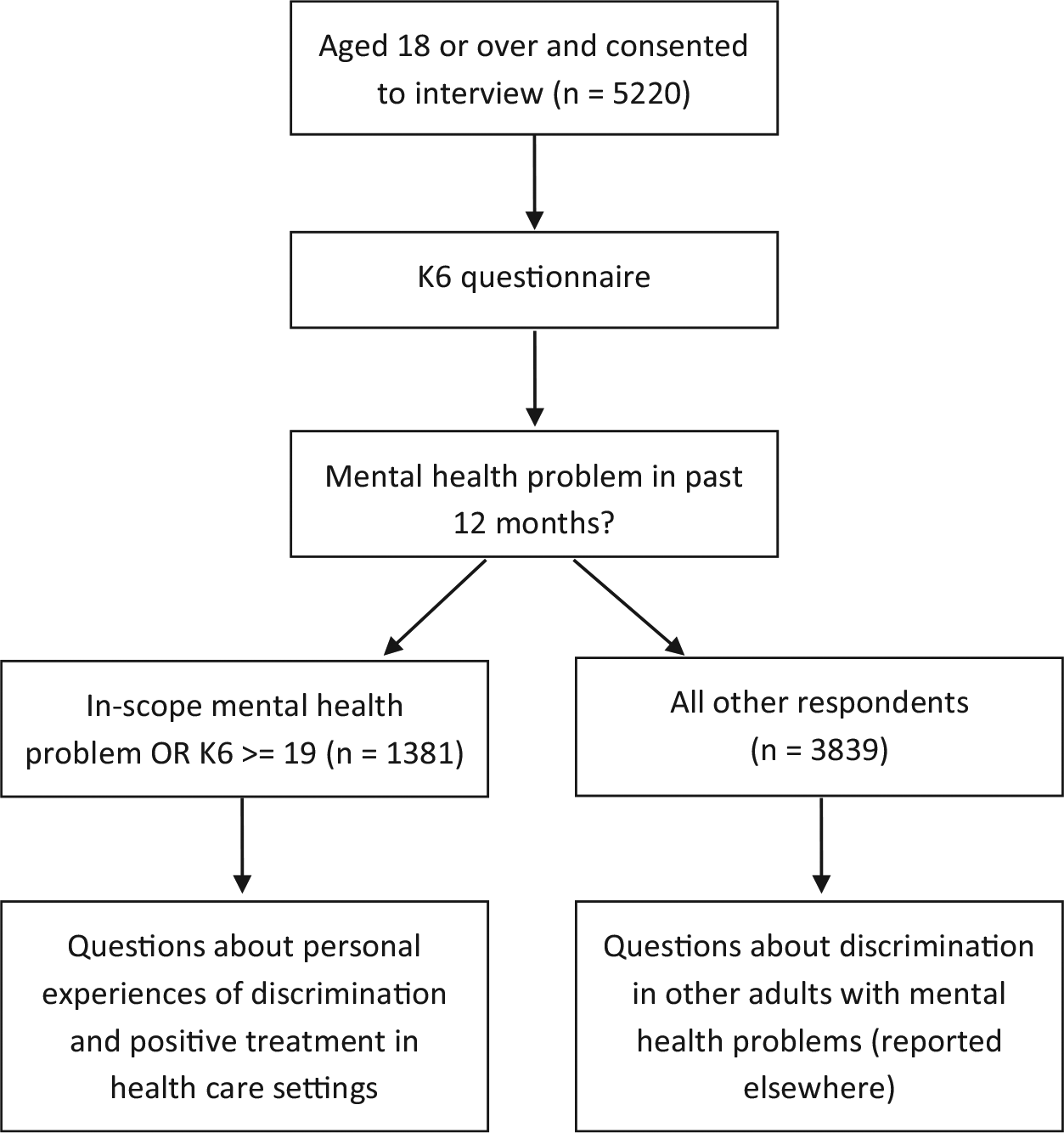
Flow chart of the process of sampling and case selection for interview.
These respondents were then asked a series of questions about their experiences of discrimination and positive treatment over the past 12 months in a range of domains, including treatment by health professionals. Respondents were told, ‘discrimination occurs when people are treated unfairly because they are seen as being different from others’. For the health professionals domain, respondents were asked, ‘Have you been discriminated against by a health professional because of the emotional or mental health problems that you told me about, for example, by a GP, counsellor, dentist, or nurse?’ and ‘Have you been treated more positively by a health professional because of these problems?’. If respondents answered ‘yes’, they were then asked, ‘What sort of professional was this?’ (with multiple responses allowed) and ‘Can you please describe what happened?’ Answers were directly transcribed verbatim by interviewers.
Content analysis
The verbatim descriptions of discrimination and positive treatment by health professionals underwent a content analysis (Crowe et al., 2015) to identify key characteristics of these experiences. One author (A.J.M.) read through the responses to develop an initial coding system, informed by previous descriptions of discrimination experiences involving health professionals (Henderson et al., 2014). The coding framework included instructions with examples and counter-examples. More than one category could be used to describe a single response. A sample of responses was then double-coded by a second author (R.B., N.J.R.) in order to refine the coding system. Any coding discrepancies were discussed until consensus was reached for both the coding system and the response in question. Once the coding framework was finalised, a single author (A.J.M., R.B.) coded the remaining discrimination and positive treatment responses. Discussion with a second author was necessary for some responses. Responses that could not be interpreted, did not make sense or required very strong assumptions about the respondent’s meaning were not coded. Responses were also not coded if they related to a physical health problem (e.g. cancer, surgery and diabetes). Only categories with at least 5% frequency are presented. A few respondent quotes were then selected to provide examples for each category.
Statistical analysis
A pre-weight was applied to adjust for the dual frame design and the respondent chance of selection. The achieved sample was close to the Australian national population in terms of geographic distribution; however, there was an under-representation of males and younger adults and an over-representation of university-educated individuals and people with an English-speaking background. These biases were adjusted for by ‘raking’ (also known as rim weighting or iterative proportional fitting) to account for known population proportions of gender, age, education level, region and telephone status. All analyses were performed using Intercooled Stata 13 (StataCorp LP, TX, USA).
Results
Overall, 5220 interviews were completed, with a response rate of 37.5%. In total, 1381 (28.8%) respondents were classified as having a mental health problem and were asked the questions about their experiences of discrimination and positive treatment. Of these, 732 respondents had K6 scores of 19 or above and 1159 respondents had a mental health problem considered to be in scope. Table 1 describes the clinical and socio-demographic characteristics of the sample classified as having a mental health problem. As described in Reavley and Jorm (2015), more respondents reported experiencing positive treatment by health professionals (40.4%) than discrimination (11.8%). GPs were the most common type of health professional reported to have discriminated against respondents and treated them more positively. There was significant overlap, with half (50.2%) of the respondents who reported being discriminated against also reporting being treated more positively by a health professional.
Clinical and socio-demographic characteristics of respondents classified as having a mental health problem.
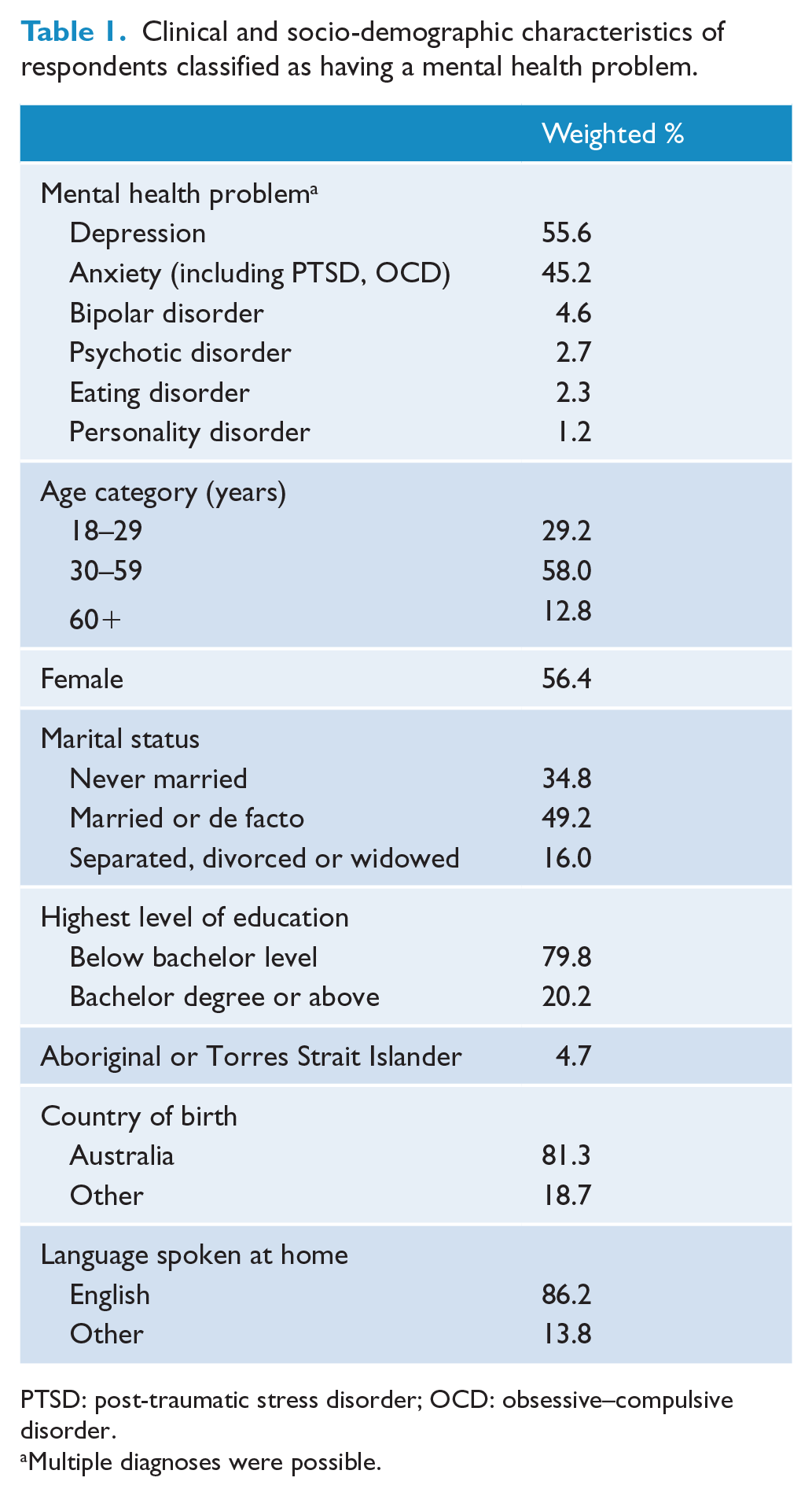
PTSD: post-traumatic stress disorder; OCD: obsessive–compulsive disorder.
Multiple diagnoses were possible.
Discrimination experiences
Of the 177 respondents reporting discrimination by a health professional, 146 provided a description of the experience and 134 responses were able to be coded. Examples from each category are provided for illustration, with the respondent’s gender, age group, diagnosis and health professional given after each quote.
Dismissive and sceptical
The most common experience of discrimination was the respondent’s health professional being dismissive of their mental health problem and that it was real or needed treatment (n = 35, 26.1%). Respondents reported being spoken to in a dismissive manner: They were not helpful – said ‘well that’s life, get over it’. (Female, 60–64 years, depression, GP) When I went to the GP with yours anxiety and was told the GP that I should toughen up mentally, or get mentally better, or not think too much. (Male, 30–34 years, anxiety disorder, GP)
Health professionals also did not always believe that the respondent needed treatment for their mental health problem: The first GP I saw when I started experience severe depression. I asked for a mental health plan. He thought I was lying and presented as being very sceptical. (Male, 30–34 years, bipolar, GP) When I went in after a work incident, I went to see a local doctor his actual words were ‘there is nothing wrong with you, get over it, you just want drugs’. (Male, 30–34 years, stress, GP)
Being judged
A total of 31 (23.1%) respondents reported that the health professional was ‘judgemental’ or they provided specific examples of being judged: As soon as a doctor finds out you’ve been on antidepressants, their attitude changes, like ‘here we go again, a neurotic woman’. (Female, 65–69 years, depression, anxiety disorder, panic disorder, GP) I went to a local GP and told him my full medical history and he didn’t believe that I was a doctor myself, that I could have these issues and also be smart and successful. (Female, 25–29 years, depression, anxiety disorder, eating disorder, GP)
Not willing to listen
A total of 19 (14.2%) respondents reported discrimination involving their health professional not listening to them, particularly regarding the nature of the problem and its treatment: Not really listening to me, with regards to my treatment I feel like I’ve just been along for the ride. (Female, 35–39 years, panic disorder, generalised anxiety disorder, GP, psychiatrist) The last visit I felt I had questions to ask on a couple of occasions she didn’t listen, the answer she gave showed she didn’t listen. (Female, 60–64 years, anxiety disorder, GP)
Not supportive or caring
A total of 17 (12.7%) respondents reported discrimination by health professionals who were not supportive or caring towards them: The Doctor that I see is from another country, he doesn’t show much empathy. I don’t know if it is a cultural difference. (Male, 55–59 years, anxiety disorder, GP) They said that you need a miracle, was not really supportive at all. (Male, 45–49 years, depression, GP, counsellor, psychologist)
Lack of understanding
Some respondents reported that their health professional lacked knowledge or understanding about their mental health problem (n = 14, 10.4%). This included ignorance about treatment and not understanding difficulties involved in recovery: They have a careless attitude towards people with depression they haven’t had the training. Ignorance of the problem or a very slight sort of knowledge. (Male, 50–54 years, depression, GP) My GP didn’t understand my problem well enough and gave me what I thought was poor advice. (Female, 40–44 years, eating disorder, GP) They don’t believe I put in enough effort to try to recover. They don’t believe I take it seriously enough. I’m not positive enough. (Male, 50–54 years, depression, GP)
Ignoring physical health problems
A total of 14 (10.4%) respondents reported their health professional did not provide treatment for physical health concerns because these problems were misattributed to the mental health problem: I have weird recurrent hernia – all in different pages – a congenital condition – when they realized I had a mental health condition they said I must be making it up for attention – demanded to be seen by someone else and then I got my surgery. (Female, 30–34 years, depression, anxiety disorder, nurse, surgeon) Well I went there because I thought I had a concussion because I fell. I had a previous mental health issue at the hospital, and he didn’t look into it concussion. He immediately send someone from the mental health department to see me. (Female, 20–24 years, depression, anxiety disorder, emergency medical doctor) Well, I think that he had a interpretive bias towards me. He assumed I was irrational – when I was informing him of my physical symptoms he would put it down to anxiety and told me to meditate. (Female, 45–49 years, depression, anxiety disorder, GP)
Medication only
Respondents also described discrimination when health professionals prescribed medication without adequate explanation, information, consultation or attempt to discuss alternatives (n = 12, 9.0%): His bedside manner wasn’t great and didn’t explain what was going on and why I would need to go on anti-depressants, he just gave me a script and sent me on my way so I didn’t take them because I didn’t know what it was for. (Female, 35–39 years, PTSD, post-natal depression, GP) They were too quick to prescribe medication, like a quick fix for the issue, but I would much rather try counselling first than getting straight into heavy medication. (Female, 20–24 years, depression, anxiety disorder, GP)
Refused medication
Some professionals refused to provide medication that the respondent requested or they withheld their medication from them (n = 11, 8.2%): Pharmacist – they questioned me in depth about my mental health and refused to give me my medication. (Female, 20–24 years, depression, psychosis, bipolar disorder, GP, pharmacist) The nurse wouldn’t give me my Xanax. (Female, 20–24 years, depression, attempted suicide or self-harm, nurse)
Barriers accessing treatment
Difficulties accessing treatment in a timely manner were described by 11 respondents (8.2%). These barriers included delays at emergency, premature discharge from hospital, a lack of follow-up after discharge from hospital and not being able to consult a health professional when requested: She kicked me out of emergency when I came to from my overdose. She kicked me out with a blanket and no support. (Female, 50–54 years, depression, nurse) I was taken to the hospital by an ambulance and in very depressed state and I was left in the waiting room for 8 hours in the hospital and then I just left/if it was someone who is really suicidal they would probably kill themselves that day and no one seemed to care/they told a mental health person was going to come/I was very agitated and no one came. (Female, 40–44 years, depression, attempted suicide or self-harm, emergency medical doctor)
Avoidance
Respondents also reported that health professionals either avoided or tried to avoid dealing with them or the mental health problem itself (n = 11, 8.2%): My GP told me to go see another GP because they felt like he couldn’t help me with my issues. (Male, 35–39 years, depression, attempted suicide or self-harm, GP) Because it wasn’t a physical issue, they refused to acknowledge the issue, which led to a misdiagnosis and I was given the wrong medication. (Female, 20–24 years, borderline personality disorder, GP)
Positive treatment
Of the 607 respondents who reported being treated more positively by a health professional because of their mental health problems, 568 provided a description of the experience and 512 were coded.
Supportive/understanding
By far the most common type of positive treatment reported was that the health professional was supportive or understanding (n = 335, 65.4%). Responses in this category described the health professional as ‘supportive’ in general terms or provided specific examples of supportive behaviour: Being very supportive in terms of what they say through the words they use … She always greets me with a big hug, she is very positive and very understanding. (Female, 60–64 years, anxiety disorder, GP) More positive support, encouraging me to keep doing what I’m doing, telling me how well I’m doing, noticing the positive changes. (Female, 40–44 years, bipolar disorder, GP, nurse) Understanding and giving me respect, not stigmatising. (Female, 20–24 years, depression, psychosis, bipolar disorder, psychologist, psychiatrist) My GP and psychologist said that they were there for me whenever I needed them. (Female, 40–44 years, anxiety disorder, GP, psychologist) Compassionate and caring. (Male, 75+ years, depression, GP) They’ve been more sympathetic. (Female, 45–49 years, anxiety disorder, counsellor)
Good listener
The next most common positive experience involved health professionals listening or being willing to listen to respondents talk about their issues (n = 87, 17.0%): He listens to what I have to say. (Female, 65–69 years, depression, GP) They’re happy to discuss my problems and issues with me. (Female, 55–59 years, depression, GP, dentist, psychiatrist, emergency medical doctor) She just talks to you and ask you the right things so you can get it off your chest. (Female, 45–49 years, depression, GP)
Treatment effort
Respondents described health professionals who were engaged in the treatment process and made a concerted effort to help them improve (n = 59, 11.5%). This included a willingness to try different approaches and treatments to get a good result: Just putting a lot of effort into the consultations I’ve had with them to help me get a better outcome. (Female, 40–44 years, eating disorder, GP, psychologist) He just makes sure he’s in contact with the psychiatrist and makes sure he knows what the psychiatrist is doing so when I turn up at his doorstep he knows how to help me. (Female, 45–49 years, bipolar disorder, GP) Asking lots of questions, trying different things and medications, coming up with some solutions. (Female, 45–49 years, depression, anxiety disorder, GP)
Referral
Making a referral or encouraging the respondent to seek further help was also seen as positive treatment (n = 59, 11.5%): He set me up to see a counsellor. (Female, 55–59 years, no disorder, GP) Just gave me some advice and options and referred me to the psychologist and was very professional. (Female, 45–49 years, depression, anxiety disorder, GP)
Checking on them
Respondents described health professionals who checked on them to see whether they were okay (n = 51, 10.0%): They would give me regular phone calls to see how I was and checking up on me. (Female, 18–19 years, depression, anxiety disorder, GP, psychiatrist) He always just asks how I am and makes and extra check to see if I’m ok. (Female, 30–34 years, post-natal depression, GP)
Gave information
Respondents also reported that being given information or explanation about mental health problems and treatments was positive (n = 40, 7.8%): She helps me understand and gives me printouts to help me understand depression. (Female, 55–59 years, depression, psychologist) I asked for help, and he explained some things. Explained some of my behaviours and what might be causing them, things I didn’t understand. (Female, 40–44 years, depression, anxiety disorder, GP) Spoke about the support services available, the mental health initiative of getting free psychology sessions. (Male, 35–39 years, depression, anxiety disorder, GP)
Treatment was effective
Some respondents reported that the help or treatment they received from the health professional was effective (n = 25, 6.8%): He got me onto the right medication. (Female, 60–64 years, depression, GP) I had the best help, that’s the only reason I’m back at work. (Male, 50–54 years, depression, anxiety disorder, psychologist, psychiatrist)
Encouraged coping strategies
Encouraging coping strategies or suggesting coping skills was also reported as positive treatment by respondents (n = 33, 6.4%): She gave me strategies to cope. (Female, 50–54 years, anxiety disorder, GP) She gave me tips (like mindfulness) which I still rely on every day. (Female, 50–54 years, depression, anxiety disorder, GP) He gave me ideas for me to get me out of the major depression and suicidal situation, gave me clues to help me focus on things other than my own illness. (Female, 65–69 years, PTSD, psychologist)
Spent more time
Respondents also reported health professionals spending more time than usual with them as positive treatment (n = 28, 5.5%): She’s really given me a lot of her time. (Female, 45–49 years, depression, anxiety disorder, GP) The GP gave more time, normally it’s a real rush job but he given me more time. (Female, 50–54 years, depression, shy or social problem, GP, psychologist)
Discussion
This nationally representative study found that over 11% of respondents with a mental health problem in the previous 12 months reported discrimination by a health professional. Discrimination was most commonly related to being treated dismissively, being judged and not listening to the person, particularly regarding their personal history and treatment needs. In contrast, 40% reported positive treatment from their health professional because of their mental health problem. Positive treatment was characterised most strongly by a supportive and understanding approach and good listening skills. Good quality care approaches were also appreciated, including making a referral, being engaged in the treatment process, regularly checking the status of the person’s mental health and providing information.
Efforts to improve community mental health literacy and encourage help-seeking for mental health problems are impeded when sub-optimal care is provided by some health professionals. Dismissive and judgemental attitudes from health professionals may perpetuate stigma, particularly self-stigma, adding to the burden experienced by those with mental health problems and interfering with recovery (Corrigan, 2004; MHCA, 2011). Furthermore, experiencing discrimination from a health professional may prevent or delay seeking help for mental health problems in the future. Evans-Lacko et al. (2015) found that previous experiences of discrimination in a healthcare setting were associated with higher health services costs, even controlling for socio-demographics, disorder type and level of symptoms and functioning. As the largest difference in cost was due to psychiatric inpatient care, they hypothesised that past stigma may lead to an avoidance of services until the person’s worsening symptoms necessitate more expensive inpatient care.
This study found lower rates of discrimination in healthcare settings than studies conducted in other countries (Corker et al., 2013; Harangozo et al., 2014; Lasalvia et al., 2013; Thornicroft et al., 2014). Several factors may account for this difference, including the use of a different interview measure (which had a focus on discrimination in the past 12 months only) and different sampling methods. Furthermore, our population sample included a high proportion of depression and anxiety disorders, and few respondents reported psychotic illnesses or personality disorders. Alternatively, the large-scale anti-stigma initiatives undertaken in Australia over the last 15 years and the improved training and support of GPs may be factors (Dunt et al., 2011; Pirkis et al., 2005; SANE Australia, 2013).
A dismissive attitude from family members is a common experience of discrimination (Hamilton et al., 2014), but other research has not identified dismissiveness as a key experience of discrimination from health professionals. Other studies have also reported more overt or blatant forms of discrimination, such as physical and sexual abuse (Rose et al., 2011) or withholding treatment (Bonnington and Rose, 2014). In this study, respondents tended to describe more subtle forms of discrimination, such as feeling that they were being judged. However, some common themes of discrimination are similar to those identified in other studies. For example, a lack of respect, similar to not being supportive or caring, has previously been identified (Mestdagh and Hansen, 2014). People with schizophrenia have also reported a lack of understanding of their condition, particularly from GPs, as discriminatory (Rose et al., 2011). Failures on the part of health professionals to listen and discuss treatment options that are personalised to the patient’s particular problem and history have also been identified as common forms of discrimination (Henderson et al., 2014; Mestdagh and Hansen, 2014; Schulze and Angermeyer, 2003). Although not frequent in this study, reports of ‘diagnostic overshadowing’ as a type of discrimination are consistent with previous research (Schulze and Angermeyer, 2003). This misattribution of physical symptoms to mental health problems may contribute to the greater risk of premature death in people with severe mental illness (Henderson et al., 2014).
Some of the types of positive experiences with health professionals could be seen as the inverse of the discrimination experiences – being supportive and understanding rather than dismissive or sceptical, for instance. These positive experiences could be expected to be delivered as part of standard care. This mirrors the finding from Rose et al. (2011) which found positive examples of ‘discrimination’ towards people with schizophrenia were being treated well and with kindness and respect – experiences which could be expected as standard in a civil society. Alternatively, although interviewers asked respondents to describe how they had been treated more positively by a health professional because of their mental health problem, respondents may have misunderstood and answered regarding positive treatment in general.
Recognising that mental health stigma exists in healthcare professionals, anti-stigma interventions targeted towards healthcare professionals and students have been developed. Evaluations of these have primarily been conducted with students rather than professionals already practising, and only a handful of randomised controlled trials have focused on mental health professionals (Mehta et al., 2015; Stubbs, 2014). These interventions have included education as well as direct and indirect interactions with people with mental health problems or their carers. While there is some evidence for short-term reductions in stigma, it is unclear how long the effects last, and widespread implementation may be premature (Stubbs, 2014). The results from this study can inform these interventions, particularly with respect to the need to increase knowledge and understanding of mental health problems, reduce negative (judgemental) attitudes, increase awareness of diagnostic overshadowing and highlight the important skills of listening and including patients in discussions around treatment. These skills are particularly important for GPs, who are typically the first point of contact in Australia’s healthcare system and were the most common type of health professional reported by respondents to have discriminated against them.
A strength of this study is the population-based sampling, which may have reduced the likelihood of recruiting respondents who wanted to participate due to experiencing particularly bad discrimination. However, study findings should be considered in light of the relatively low response rate, which may limit the generalisability of the results. Additionally, not all descriptions of discrimination experiences were clear and follow-up questions to clarify respondents’ answers were not possible.
In conclusion, this study suggests that a minority of Australian adults with mental health problems are treated by their health professionals in a manner perceived to be discriminatory. This suggests that ongoing anti-stigma education for health professionals is required, and the findings from this study can inform the content of these interventions. In addition to improving knowledge and attitudes, these interventions can include messages about positive behaviours that health professionals can engage in to best support people with mental health problems towards recovery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the National Health and Medical Research Council.