
Abstract
Flinders Medical Centre (FMC) is a large teaching hospital in the southern suburban area of Adelaide, South Australia. The emergency department (ED) manages approximately 50 000 presentations per year. The ED caters for all patients with either physical/medical problems or mental health concerns. As with many large hospitals, a major problem for the ED is access to inpatient beds for patients requiring admission to the hospital. Thus patients are frequently waiting for extended periods of time prior to admission to an inpatient bed. This is seen for both mental health patients and patients requiring admission for other illnesses.
The mental health component of the ED has traditionally been run by the Psychiatry Department's consultationliaison (C-L) service. No systematic examination had been conducted to confirm whether or not there was an increase in demand but there was a general perception that this was the case. This paper examines the changes in demand for mental health services in the FMC ED over a 10-year period.
Deinstitutionalization and mainstreaming was a central policy of the National Mental Health Plan [1] premised on principles of human rights and equity and the belief that integrated mental health and community services could provide holistic care to clients in a manner that contributed to the prevention of illness and the reduction of stigma. While this approach has provided many benefits to people experiencing mental illness, it appears to have also resulted in increasing numbers of mental health presentations to emergency departments within our general hospitals [2–4]. This phenomenon has also been observed in other countries where deinstitutionalization and mainstreaming has occurred [2], [5], [6].
Mental health presentations in emergency departments
Little has been published about the number of presentations for mental health concerns to general hospital emergency departments in Australia and the authors were unable to locate any that reported over an extended time frame. Reference is frequently made to increasing ED demand but supporting data is usually not presented. The New South Wales ‘Working Group for Mental Health Care in Emergency Departments’ have estimated that between 0.6% and 10% of all ED presentations have a chief psychiatric complaint (cited in) [4]. Holmes et al. [7] reported that 2.1% of ED patients were referred to their psychiatry Consultation-Liaison service and Heslop [2] reported 6.5% of the ED patients were triaged for categories that represented mental health concerns, while discharge diagnosis showed 5% had a primary diagnosis of a mental illness. Studies from other countries show similar rates of mental health presentations in general hospital EDs [6], [8], [9].
Diagnoses
Studies that report comparisons of ED mental health presentations across years are limited. Only one study was located that compared diagnoses of ED mental health patients over time, in this case a four-year period. The major finding was that presentations for suicidal behaviour decreased over that time while the number of patients with psychotic illness increased [6]. However, other studies do detail the range of diagnoses seen in emergency psychiatry settings, although in some cases these are specialist emergency psychiatry services, not general hospital EDs.
Heslop [2] reported that of concerns noted at triage, the most common mental health presentations (more than 50%) were overdose and suicidal behaviour or ideation. A further 10% of patients were thought to have a psychotic illness and 8% depression. Holmes [7] reported the most common diagnoses were personality disorders, psychosis and substance use. Holmes also referred to three studies conducted in other countries that show a wide range of diagnoses with large percentages being diagnosed with psychotic illness, substance-use problems and depression. Hatfield [10] reported data from an emergency psychiatric assessment service in the UK which showed 50% of patients had mood or anxiety disorders, more than twice as many as those with psychosis or personality disorders. Data from a 3-month review of presentations to a London ‘accident and emergency’ facility showed the most common mental health reasons were deliberate self harm (31%), substance abuse (20%), psychosis (17%) and mood disturbance (15%) [11].
Disposition
Some studies have reported on the rates of admission and discharge from the ED for mental health patients. Heslop's [2] study showed that 60% were discharged from the ED and 16% admitted to the psychiatry ward with 7.8% staying overnight in ED and a further 4.7% transferred to another hospital. Of the patients referred from ED to the C-L service 19% required admission to a psychiatric ward [7]. Furthermore, a number of people who present to EDs with mental health problems are subsequently detained. Holmes [7] reported that 10% of patients referred from ED to the liaison team are detained.
Length of stay
One of the difficulties faced by mental health patients in the ED is the amount of time the patients spend there, in an environment that is generally not considered optimal for people with serious psychiatric disorders. Waiting times and duration of stay are influenced by a number of factors including the general workload in the ED, delays due to the problem that often no specialist mental health staff are employed in the ED, and problems with the lack of available beds in psychiatric wards for those patients who need to be admitted. Heslop [2] reported length of stay (LOS) for their first six-month sample as being between one and 30 h with an average of 7–8 h.
In this current study we considered the nature of demand because the ED and psychiatry staff experienced the demands of the emergency mental health patients as an important additional problem to an already pressured ED and Psychiatry team. One factor believed to be contributing to this pressure was the closure in 1996 of the emergency department at the last remaining psychiatric hospital in Adelaide (Glenside Campus) in line with the mainstreaming strategies of the National Mental Health Plan [1]. It was thought that patients who would otherwise have presented to that centre now came to the emergency departments of the other local teaching hospitals. There was considerable discomfort amongst the providers of mental health services who felt that the Glenside ED had been closed without transferring staff from that department to the emergency departments at FMC and the other public teaching hospitals within Adelaide. There was also a perception that there was an increase in the number of patients presenting with psychotic disorders.
Method
The ED at FMC has compiled computerized records about patient presentations since 1993/94. It includes information such as triage categories, discharge diagnoses, patient outcomes and length of stay for all patients who present to the service. The data was examined to describe the change in demand for emergency services from people with mental health problems. Ethics approval was not required as the ED data examined for this study does not include patient identification information.
Patients seen in the FMC ED by mental health staff are triaged on arrival into two broad categories – ‘psychiatric disorder’ or ‘overdose’. The triage staff does not make diagnoses beyond the presumptive assessment of either a psychiatric problem or overdose. (No examination of the accuracy of triage assessments has been conducted, but triage staff are highly experienced in making the initial assessment of presentations to the ED.) The specific diagnoses used in this study were the discharge diagnoses made by psychiatrists or medical staff and coded using ICD-9 diagnostic categories [12]. In this study we have concentrated on the primary diagnosis of the presenting problem and not considered co morbid concerns.
The full range of psychiatric diagnoses of the ICD-9 are used in diagnoses, but for our analyses we grouped together related diagnoses into the following categories:
depression/affective disorders:
major depressive episodes bipolar affective disorder (not mania) reactive depression, dysthymia mania:
manic disorder bipolar disorder – manic hypomania psychotic disorders:
schizophrenia paranoid psychoses schizo-affective disorders psychoneurotic and anxiety disorders:
anxiety disorders panic attacks acute stress reactions adjustment disorders hypochondriasis suicide/self-harm:
suicidal ideation self-inflicted injury self inflicted poisoning (depending on presentation would be coded as overdose) personality disorders:
all groups including borderline personality disorder conduct disorders organic brain syndromes:
delirium dementia acute confusion chronic alcoholic brain syndrome alcohol/drug misuse or abuse:
drug/alcohol induced psychosis drug/alcohol withdrawal acute intoxication alcohol or drug abuse/dependence.
The inclusion of organic brain disorders and alcohol and drug misuse categories is premised on the presenting symptoms that often suggest a problem of a mental rather than physical nature. Triage assessment is often not detailed enough to make the distinction between organic and functional disorders.
Overdose patients are usually assessed and treated initially by the emergency physicians before being transferred to either the intensive care unit, a medical ward or to the mental health staff in the ED for further psychiatric assessment. These diagnoses are not included in the analysis of nominated ‘psychiatric’ presentations as they are usually coded separately as ‘overdoses’ but may become a psychiatric presentation once the issues of overdose are managed.
Within this context we examined the changes in psychiatric presentation, the changes in number of overdoses, and the relative contribution of the different diagnostic groupings over a 10-year period. Results presented are from all presentations over the 10-year period.
Results
Presentations to the ED at FMC for mental health problems have risen significantly over the last 10 years within a context of relatively stable total presentations within a range of 47 000–52 000 per year.
Mental health & overdose presentations
During the 10 years from 1993/94 the percentage of mental health patients has risen from 0.3% to more than 3.5% – a 10-fold increase. The average increase per year was 33%. The biggest increase was in 1997 (66%), which coincided with the closure of the emergency service at the Glenside Psychiatric Hospital at the end of 1996.
The quantitative demand from overdoses is large and the number of presentations is greater than for any single psychiatric diagnosis. The number of patients presenting with overdoses has not changed in any significant manner since 1996. Figure 1 shows the number of presentations for mental health, overdose (based on triage assessment) and all ED patients across the 10 years.
Mental health, overdose and total presentations to the emergency department at Flinders Medical Centre: 1993–1994 to 2002–2003. MH presentations do not include OD.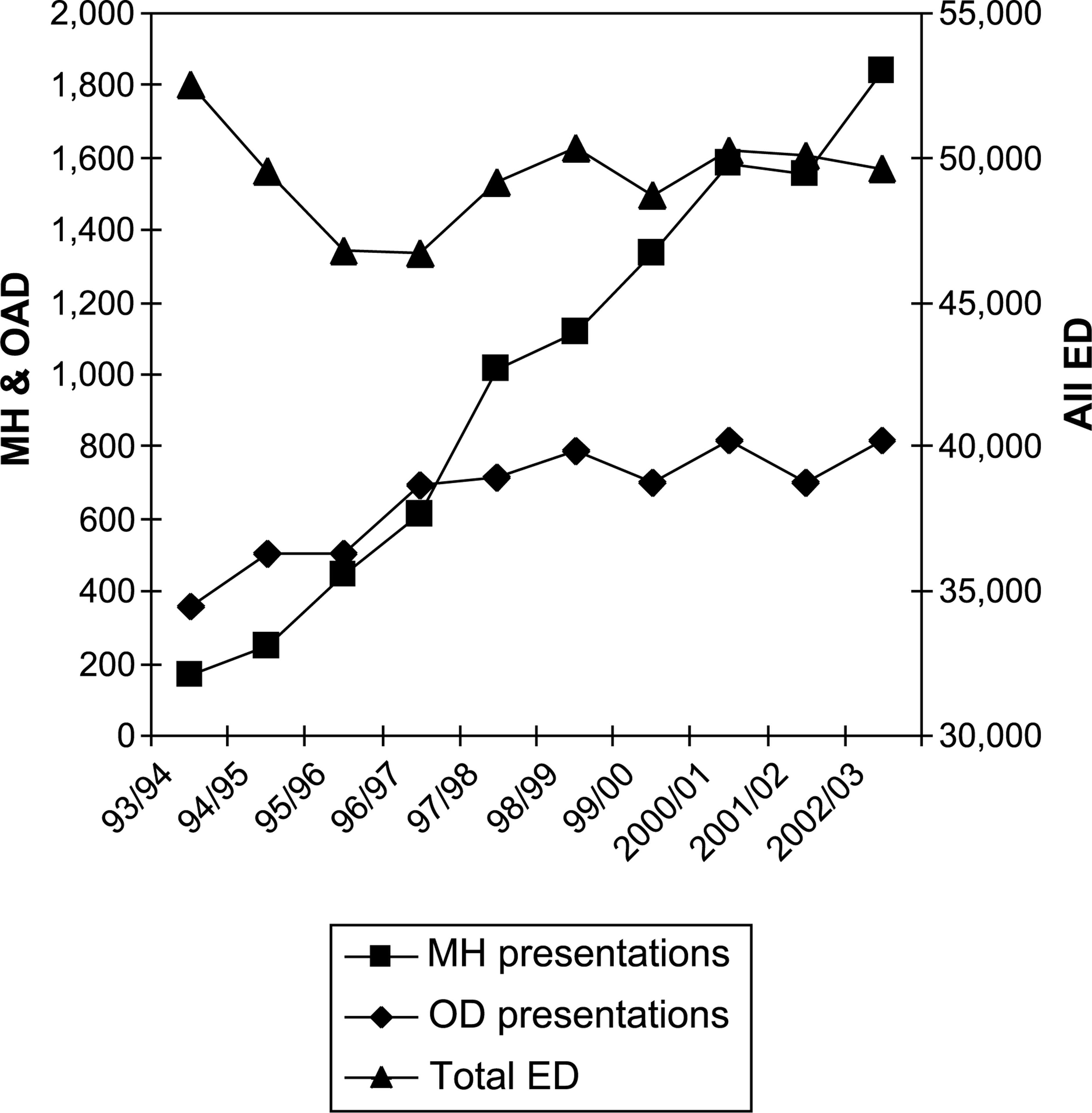
Diagnoses
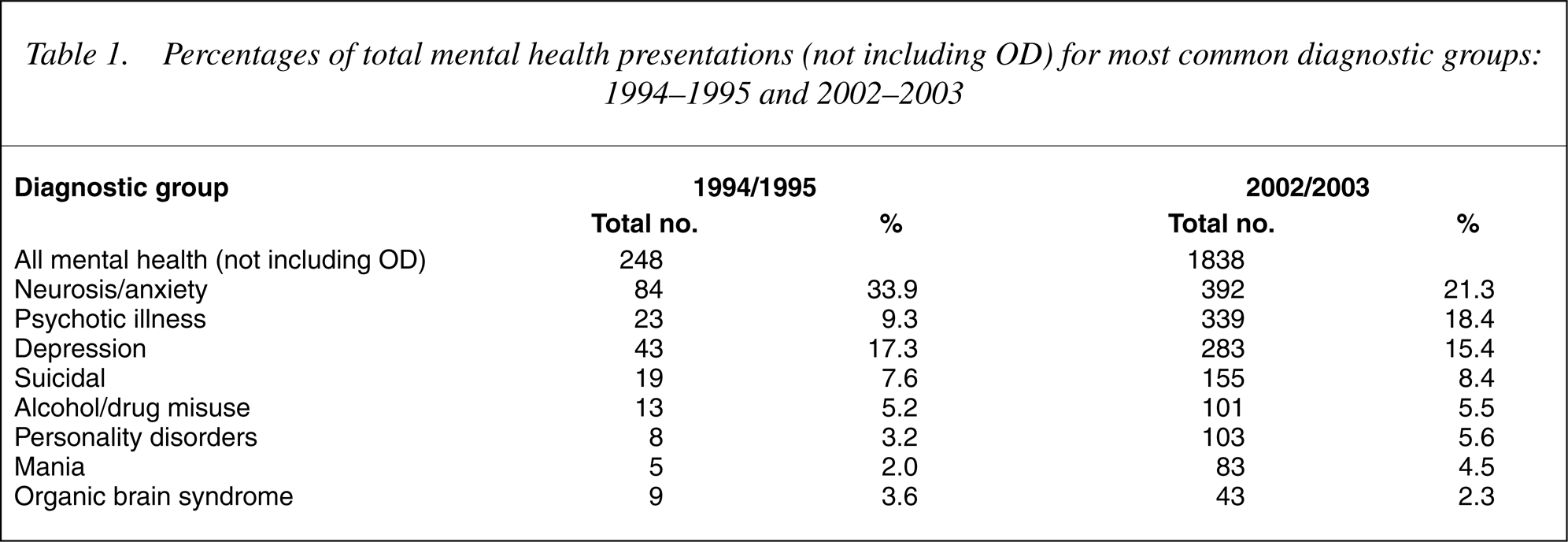
We have examined the discharge diagnoses of patients over 9 years from 1994/95 to 2002/03. The greatest increase in number was seen for affective disorders, psychoneurotic/anxiety related disorders and psychoses. However, an examination of the percentage of patients in each category suggests that the neurosis/anxiety group now represent a smaller proportion of the total, whereas there has been a considerable increase in presentations of psychosis, and while relatively small numbers, mania (see Table 1).
Percentages of total mental health presentations (not including OD) for most common diagnostic groups: 1994–1995 and 2002–2003
Outcomes
There are a number of outcomes for mental health patients who present to the ED. In 2002/03 almost 8% did not wait for full assessment and/or treatment, 36% were discharged directly from the ED, and 22% were transferred to other hospitals, presumably for admission. The remainder, approximately 33%, were admitted to either the ED, the psychiatric ward (including the FMC mental health hospital-at-home service) or to other wards. Those patients categorized as admitted to ED include all patients who wait more than 12 h for inpatient admission.
Detention
Information about the number of detained patients has only been recorded since late 2000, and the data shows that for the 2002/03 years 22.5% of the patients who presented to the ED with psychiatric illness were detained under the Mental Health Act, an increase from 12.3% in 2000/01. Some diagnoses are disproportionately represented in the group of detained patients. For example, mania that has the smallest number of patients (4.5%) represents more than 12% of all detentions whereas the largest group, neurotic/anxious patients (21.3%), account for only 6% of detentions. Psychotic patients, who represent less than 20% of all mental health patients in the ED, account for over 40% of all detentions.
Admissions
As with detentions, some diagnoses are more likely to result in admission than others. The data shows that patients with psychotic illness or mania are much more likely to be admitted than others. In 2002/03, of the patients admitted at FMC or transferred to Glenside for admission, 61% of patients with psychotic illnesses and 57% with mania were admitted as well as 42% of those diagnosed with depression. In comparison, only 18% of patients with neurosis/anxiety problems and 14% with alcohol/drug problems were admitted.
Length of stay
The data shows that at FMC the length of stay (LOS) in the ED, that is from arriving at triage to discharge from ED, admission to a ward or transfer to another hospital, has increased for all patients but more markedly for mental health patients. From 1993/94 through to 1999/ 2000 there had been an increase in LOS for all patients of about 60%. Since then, while there has been an increase in LOS generally of about 20%, the increase for mental health patients has been 300%. Furthermore, detained patients remain in the ED for more than twice as long as voluntary patients. In 2002/03, the average LOS for all patients was 5.77 hours, but for mental health patients this was 16.45 hours. Detained patients stayed an average of 30.86 hours compared to 12.27 hours for voluntary patients.
Discussion
The results from this examination of 10 years of data show that the quantitative demand for emergency psychiatric care at FMC (not including overdoses) has increased 10-fold in as many years, from 0.3% to 3.5% of all presentations to the ED. When overdoses are included the total number has increased from 530 per year to 2657 (5.3% of total) within a context of otherwise stable numbers of presentations.
It is apparent from the data that the reason for this increase is not solely due to the closure of the emergency service at the local stand-alone psychiatric hospital, although in 1 year this may have made a disproportionate contribution. This is an important finding because there was a wide spread belief amongst the staff that this alone accounted for the increased demand. It is clear from the data that other factors must have contributed, as, although there was a marked increase in that year, there was a rise in every year before it and after it.
The introduction of deinstitutionalization and mainstreaming has a longer history and these have most likely contributed to the increase in attendances in the ED at FMC. The very low numbers of presentations 10 years ago may reflect reluctance for people at that time to attend public emergency departments with mental health concerns. Reduced stigma, as a result of public education, as well as changed policy may have contributed to the increases in presentations. Furthermore, people with psychotic illness who were previously institutionalized now live within the community and attend public EDs at times of acute illness. The introduction of these policies has not always been accompanied by sufficient funding of community-based services and it is quite common for the community mental health services to direct patients to the ED.
In comparison to data presented in other studies our records show some similarities and some differences. The percentage of mental health presentations falls within the range suggested by Westwood [4]. The diagnoses attributable to those who present are across the whole spectrum of acute psychiatric disorder. The most common reasons for presentation, following overdose, are for psychoneurotic/stress reaction problems, psychotic disorders, depression and suicidal behaviour and ideation. This pattern of presentation does not closely match those reported by others, apart from overdose being the most common reason in our department. The reason for this difference in diagnostic rates is not known but may be due in part to the method of categorizing patients used in other studies. For example, many studies showed large numbers were classified as substance abuse and suicide attempts, but it is possible that in our records such patients who present may be coded as overdose.
Irrespective of diagnosis, the patients who present are acutely disturbed and could be regarded as subject to a situational crisis. Further investigation is needed to determine the extent to which issues such as drugs and alcohol makes a contribution, and the extent to which the system within which the patient lives makes a contribution.
In terms of admissions, it appears that a greater number are admitted at FMC than reported elsewhere. While only 10.8% are admitted directly to our Psychiatry department (either the inpatient unit or the hospital in the home service) the actual percentage who are ultimately admitted is much higher. In Adelaide the system that operates is such that each public hospital only accepts those patients who reside within its own catchment area. The data reveals that 9.2% were transferred to other general public hospitals (presumably for admission) and that a further 13.2% were transferred to Glenside Psychiatric hospital either due to lack of beds at FMC or because they required a level of supervision and security that could not be offered within our department. Together this means that approximately 55% of the mental health patients who present at the ED are subsequently admitted as only 44% are discharged or do not wait. Admittedly, a large percentage (almost 20%) of those admitted are categorized as ‘admitted to the ED’ which occurs when the patient has been in the ED for more than 12 hours. Thus some of these people may ultimately have quite short admissions, but others may remain in the ED for more than 2 days before being discharged.
The number of patients detained has risen dramatically over the last few years and the latest figure of 22.5% is considerably higher than that reported by Holmes [7]. It is known that a large percentage of the detained patients arrive at the ED already detained by a health care worker in the community but an accurate breakdown of this is not available. Again, this may reflect a shortcoming of community-based care that is not mandated to provide care for patients deemed in need of detention. The average LOS, currently more than 16 h, is much higher than Heslop reported [2]. The factors responsible for this long length of stay are more complex than just bed availability and require further assessment.
The data does support the view of the ED and psychiatry staff that there has been an increase in the number of psychotic patients and other patients who are difficult to manage, such as those with mania. Across the 10 years of this study the percentage of mental health patients presenting with psychotic illness has almost doubled from 9.3% to 18.4% and this group of patients is also most likely to be detained and/or admitted. It is noteworthy that while a large percentage of psychotic patients are detained, almost 60% who present to the ED, presumably with acute symptoms, are managed as voluntary patients. While the actual numbers are much lower, there has also been a similar increase in the number of patients presenting with mania. Prevalence rates of these disorders have remained relatively stable so cannot account for this increase, thus the most likely cause is deinstitutionalization and insufficient community services as mention previously. Together with the increase in the number of presentations for mental health and overdose patients the data reveals a considerable increase in the length of stay (LOS) in the ED experienced by mental health patients. Again, the lack of inpatient beds can contribute to the time patients remains in the ED. The policy of only admitting patients from our own catchment area means that LOS at FMC ED can be affected by bed availability in hospitals in other regions also. Furthermore local practice is that patients with mental health problems are not usually admitted to general wards and this adds to the delay in admission and increased LOS in the ED. A fuller examination of the data is needed to assess what other factors, e.g. total numbers, time of presentation or complexity of problems, impact on LOS. Our intuitive view is that a rise in demand would parallel a rise in the length of stay, but it may be that there is some cut-off point at which an exponential change in LOS, as a function of demand, occurs. Initial indicators from the data over the years suggest that such a cut-off may have occurred at about 110–120 patients per month but currently presentations are above 120 most months. Further investigation of factors that influence LOS is needed.
Within our ED an increase of the magnitude we have experienced is of major significance in terms of the organization of hospital services in general and ED services in particular. A number of initiatives have been implemented to help manage this demand including establishing an ‘emergency mental health unit’ within the ED led by a senior consultant (RSK). A fuller discussion of how the issues of increased demand have been addressed will be presented in future.
The results of this study hopefully provide useful data that other services can use to make comparisons. We have documented patterns of ED use at FMC by patients with mental health problems across a 10-year period of which no similar data has been reported in the Australian literature to date. The increase can be explained largely by changed policies of deinstitutionalization and mainstreaming together with insufficient community mental health services. It is acknowledged that not all other public hospitals (in South Australia or other states) experience such ongoing problems with bed availability and the system of transferring mental health patients to certain hospitals based on where the patient resides may also be particular to South Australia. Thus the issues about LOS stay may not be so pertinent to all services.
Conclusions
This study has examined changes in demand for psychiatry services in the emergency department of FMC over a 10-year period. It also provides data about the number and category of presentation that can be used for comparison by other services. We are currently attempting a more detailed analysis of the causes of the increase in demand and LOS and relative changes in diagnostic groups, which is possibly due to a combination of factors, both within and outside of the mental health system.
The increase in demand in the ED has followed the introduction of mainstreaming and deinstitutionalization. More recently the increased demand experienced at FMC has continued through a period where the capacity of the available local community mental health services to provide consistent and sufficiently lengthy support for patients who were acutely ill has been almost exhausted. In South Australia the government is committed to improving mental health services but addressing the problems must be staged. It may be that if community mental health services are expanded and satisfactory community accommodation is in place that the problem of access-block (for inpatient beds) will improve.