
Abstract
Objective:
The relationship between Indigeneity, social adversity status and externalizing symptoms is complex and unclear. This study investigates how Indigeneity, social adversity status and externalizing symptoms are related in young people.
Methods:
A total of 132 Indigenous and 247 non-Indigenous young people aged 6–16 years were recruited from a hospital mental health outpatient service. Normality plots with statistics for social adversity status and parent-reported externalizing symptoms were completed for the two groups, matched for age, gender, mental disorder symptom severity, symptom-linked distress and impairment. Standard multiple regression was used to examine how Indigeneity moderates the relationship between social adversity status and parent-reported externalizing symptoms. A scatterplot investigated the association between Indigeneity and social adversity status in young people with parent-reported externalizing symptoms.
Results:
The distributions of the two groups and (1) social adversity status and (2) parent -reported externalizing symptoms were non-normal but acceptable for a moderator analysis. Indigeneity and social adversity status made independent significant positive contributions to externalizing symptoms. In contrast the interaction between Indigeneity and social adversity status made a nonsignificant negative trend to externalizing symptoms. A scatterplot revealed Indigeneity moderated the link between social adversity status and externalizing symptoms.
Conclusions:
High social adversity status is linked to externalizing symptoms in non-Indigenous young people but despite higher social adversity, Indigenous young people don’t necessarily externalize. Potential protective resilience factors for externalizing symptoms in the Indigenous young people need to be ascertained and nurtured. Future systematic investigations of the contribution of these protective factors to Indigenous referral pathways and management are needed. It is also crucial that increased social adversity status is addressed and managed in all young people, regardless of Indigeneity.
Introduction
Higher social adversity status (SAS) is associated with increased mental health conditions including externalizing symptoms in non-Indigenous young people. Bradley and Corwyn (2002) noted that the effects of increasing SAS begin before birth, extend into adult life and are associated with decreased material and social resources and increased stress inducing conditions affecting young people and/or their parents. Importantly, the deleterious effects of higher SAS are moderated by each child and family’s characteristics and available external support systems. Currie (2009) extends the association of increasing SAS with worsening mental health in young people to emphasize its pivotal role in future higher SAS later in life and transgenerational higher SAS. Diez Roux and Mair (2010) expounded the important roles housing and local neighborhood play in mediating the relationship between increased SAS and increased mental health conditions in young people. Two major mechanisms have sought to explain this link: The social causation model outlines how increased social adversity may then lead to increased mental health conditions. Dohrenwend et al. (1992) noted the importance of social causation for women with depressive disorders and men with substance abuse/dependence disorders. In contrast, the health selection model emphasizes that increased mental health conditions may then cause sufferers to experience greater social adversity. Dohrenwend et al. (1992) explained that this model may be important for people with psychotic disorders. Link and Phelan (1995) found that both models are crucial for understanding higher SAS being linked with increased mental health conditions in young people.
In contrast, the links between SAS and mental health conditions including externalizing symptoms in Indigenous young people are complex and unclear. Shepherd et al.’s (2012) findings in a large sample of 4- to 17-year old Indigenous young people in Western Australia supported higher SAS being linked with increased mental health conditions, including externalizing symptoms. Young et al. (2017) similarly reported that Indigenous young children’s mental health and wellbeing is adversely affected by increased social adversity and they share the same risk and protective psychosocial factors for mental health as for non-Indigenous children. Other authors focus on the particular adverse effects of colonization as a major determinant of increased mental health conditions in Indigenous young people (King et al., 2009) and specifically intergenerational trauma (Atkinson, 2002; Czyzewski, 2011). Silburn et al. (2006) expounded that increased stress experienced by Indigenous young people as a result of colonization regardless of SAS may limit the mental health benefits linked with lower SAS. However, Sarche and Spicer (2008) explored unique cultural protective factors that may ameliorate colonization’s effects, specifically extended family networks and traditional parenting and child-rearing beliefs as a few of the cultural strengths American Indian and Alaska Native young people can draw on. Similarly, Andrade et al. (2006) emphasized the importance of sociocultural factors that confer protection from psychopathology for Indigenous Hawaiian young people.
A number of authors specifically explore how Indigenous young people may experience lower rates of mental health conditions including externalizing symptoms despite having increased SAS: LaFromboise et al. (2006) investigated American Indian young people with moderate to high SAS and found that higher engagement, knowledge of and immersion in traditional cultural practices, perceived community support, a warm supportive mother and absent perceived discrimination were linked with lower rates of mental health conditions, including externalizing problems. Galliher et al. (2011) similarly reported that in Navajo adolescents affirmation, belonging and exploration of traditional cultural practices, and for some young people identification with Settler culture, protected against perceived discrimination’s association with increased mental health conditions, including externalizing behaviors and substance abuse. Mileviciute et al. (2013) noted that an optimistic explanatory style moderated the relationship between negative life events (increased SAS) and mental health conditions such as depression in American Indian young people. Hopkins et al. (2014) outlined that for high-risk Indigenous families, prosocial friendships and increased SAS conferred protection for better psychosocial functioning (and lower externalizing symptoms). Recently, Fatima et al. (2022) analyzed data from the Longitudinal Study of Indigenous Children (LSIC) and noted that Indigenous children with strong cultural identity and knowledge have less social and emotional difficulties, including externalizing problems.
To date, Indigeneity, SAS and externalizing symptoms have not been investigated in clinically referred children and adolescents. Therefore, 379 young people aged 6–16 years (Indigenous 132; non-Indigenous 247) were recruited from a hospital mental health outpatient service. The two groups were matched for age, gender, mental disorder symptom severity, symptom-linked distress and impairment. Standard multiple regression was used to examine how Indigeneity moderates the relationship between SAS and parent-reported externalizing symptoms.
Method
Participants
A total of 132 Indigenous children and adolescents, aged 6–16 years, were recruited from consecutive referrals to the Wadja Aboriginal Family Place and their tertiary hospital-based Indigenous mental health team over a 4-year period. The Indigenous young people, their families and community were cared for by the Victorian Aboriginal Health Service or Victorian Aboriginal Community Controlled Health Organisations and/or the Victorian Aboriginal Child Care Agency. They were referred for a range of difficulties that overlapped but can be grouped as follows: oppositional defiant rule breaking behaviors (59%), impulse control problems (20%), depression and anxiety difficulties (16%) and other (namely learning problems (6%); 71% of these children were medicated with stimulant medication being most common (84%).
An age, gender, mental disorder symptom severity, symptom-linked distress and impairment (Rutter et al., 1975) matched clinic referred group of non-Indigenous young people (N = 247), aged 6–16 years, from 50 local primary and secondary schools was recruited as a clinical control group over a 6-year period (see Table 1). These 247 children and adolescents were screened from a total sample of 596 children and adolescents identified by teachers and/or school support staff as having coping difficulties who then referred them to specialized university clinics in metropolitan Melbourne (Australia), over a 6-year period. All 596 young people were assessed but only 247 were age, gender, mental disorder symptom severity, symptom-linked distress and impairment matched to the Indigenous group. They were referred for a range of difficulties that overlapped but can be grouped as follows: oppositional defiant rule breaking behaviors (62%), impulse control problems (23%), depression and anxiety difficulties (13%) and other (namely learning problems (8%); 68% of these children were medicated with stimulant medication being most common (85%).
Key demographic and clinical factors in the (1) Indigenous clinical (I) and (2) non-Indigenous clinical (NI) groups.
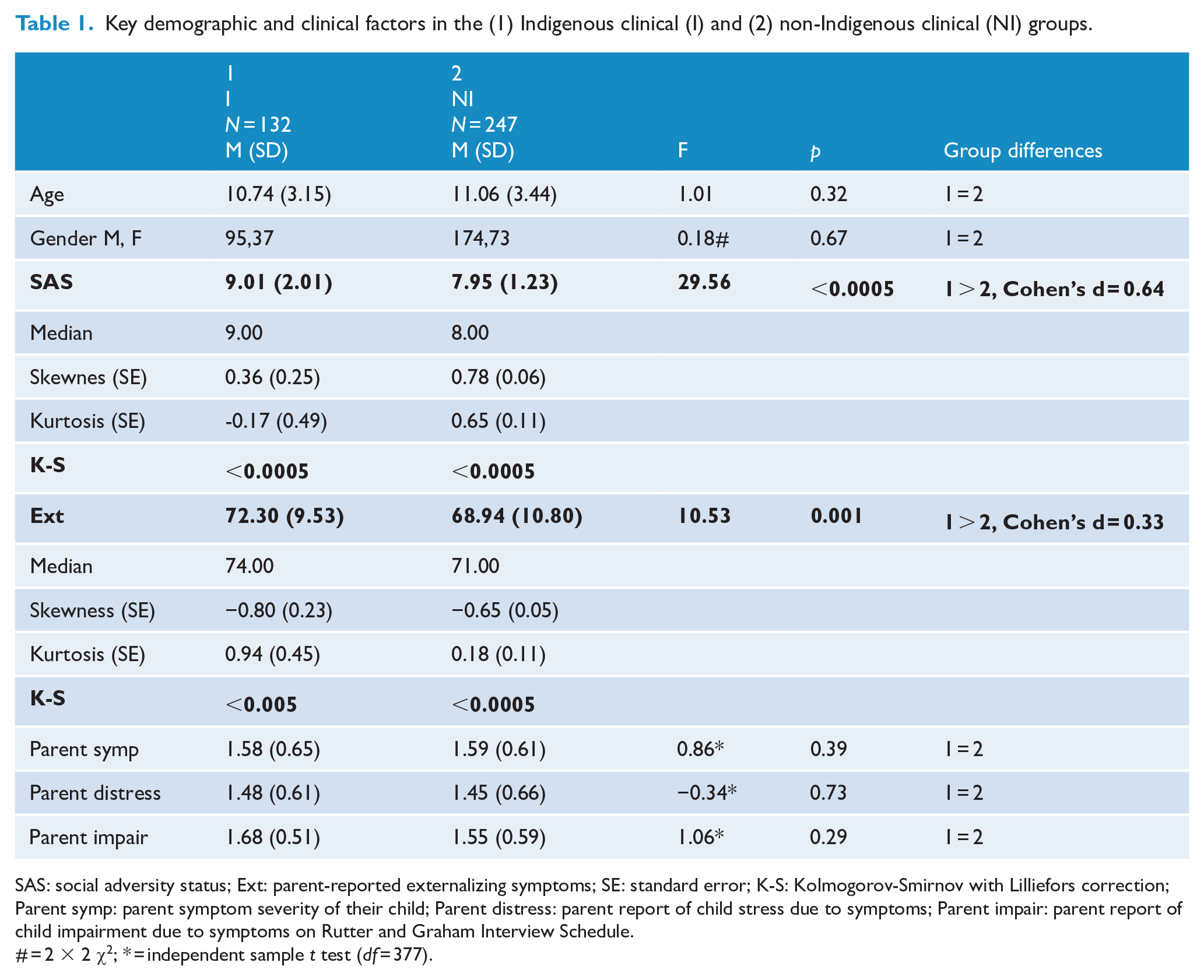
SAS: social adversity status; Ext: parent-reported externalizing symptoms; SE: standard error; K-S: Kolmogorov-Smirnov with Lilliefors correction; Parent symp: parent symptom severity of their child; Parent distress: parent report of child stress due to symptoms; Parent impair: parent report of child impairment due to symptoms on Rutter and Graham Interview Schedule.
# = 2 × 2 χ2; * = independent sample t test (df = 377).
The two groups did not differ with respect to their referring problems, their medication status or the community-based psychosocial interventions that had been trialed. All the children and adolescents met the inclusion criteria of living in a family home (and not in an institution) and attending normal primary and secondary schools. All had non-age corrected Intelligence Quotients of 70 or above (Wechsler, 2003) and none had neurological disease, endocrine disease, substance abuse/dependence disorders, personality disorders, bipolar or psychotic disorders. There was no refusal to participate. The cultural validity and reliability of the impairing patterns of symptoms in the Indigenous group were carefully and systematically determined by Indigenous mental health staff or AHLOs ensuring that each carer-identified pattern of symptoms and associated functional impairment was correctly interpreted. Trained interviewers (mental health staff) interviewed all the remaining caregivers of the non-Indigenous young people.
Measures
The Achenbach Child Behavior Checklist (CBCL) (Achenbach and Rescorla, 2001) consists of 112 behavior problem items which are rated by a parent on a 3-point scale as to how applicable each is to the child (scale: 0 = not true, 2 = very/often true). The externalizing subscale is ascertained and includes the aggressive and delinquent behaviors subscales comprised relevant symptoms. The CBCL is well researched, has adequate psychometric properties (inter-rater reliability κ
The Schedule for Affective Disorders and Schizophrenia for school age children-present and lifetime version (K-SADS-PL) (Kaufman et al., 2000) is a structured diagnostic interview schedule based on Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV criteria (0 = no information, 3 = threshold), with a parent version. It was used to determine DSM-IV mental disorders from a structured clinical interview with each child’s caregiver. It has proven clinical utility, reliability (inter-rater reliability kappa > 0.75 [kappa = 0.87 current sample]) and validity.
The Rutter and Graham Interview Schedule (Rutter et al., 1975) is a semi-structured clinical interview originally developed to ascertain mental disorders presence or absence from a parent perspective. It ascertains overall mental disorder symptom severity, symptom-linked distress and impairment rated on a 0—absent, 1—mild and 2—severe, Likert-type scale. The Rutter and Graham Interview Schedule has good test–retest reliability (κ = 0.85), consistency (Cronbach’s α= 0.92) and concurrent validity.
The Parental Account of Childhood Symptoms (PACS) (Taylor et al., 1986) is a semi-structured clinical interview which was originally developed as an instrument for the measurement of children’s behavior problems as experienced at home. A trained interviewer administered the demographic section of the interview. A SAS scale (range 3–) was formed from adding a total of family income level (1–2), mother’s educational level (1–2), single parent status (0–1), sibling size (0–) and broken home status (1–2). The PACS has been demonstrated to have adequate inter-rater reliability (κ = 0.69–0.96) and Cronbach’s coefficient alphas ranged from 0.87 to 0.89.
The fourth edition of the Wechsler Intelligence Scale for Children (WISC-4) (Wechsler, 2003) was used. This provides verbal comprehension, perceptual reasoning, working memory, processing speed, and full-scale scores of measured intelligence via 10 core subtests of known intelligence domain features. The WISC-4 is well established with valid and reliable (Cronbach’s α > 0.80) normative data.
Procedure
The clinical research protocol was Hospital Ethics Committee approved (2019.207/56941). All participants and their caregivers were given verbal and written information and written informed consent was obtained from each participant’s caregiver before entering the study. Testing occurred over one session (90 minutes maximum duration) with breaks as needed. Each parent and their child were assessed in separate rooms by different trained clinical researchers (a child and adolescent psychiatry Fellow; a probationary psychologist—both under approved supervision; an Indigenous child and adolescent psychiatrist; an Indigenous clinical psychologist; and AHLOs). During the session, the parent completed the CBCL and was interviewed using the PACS demographic section, Rutter and Graham Interview Schedule overall mental disorder symptom severity, symptom-linked distress and impairment scales, and K-SADS-PL while his or her child completed the WISC-IV. The WISC-IV (10 core subtests) was administered by a probationary psychologist under the supervision of a registered psychologist. Paper versions of the psychometric measures were used.
Statistical analysis
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS/SC). The two groups and (1) SAS and (2) parent-reported externalizing symptoms distributions were investigated for normality (Mishra et al., 2019) (see Table 1 and Figures 1 and 2). Missing data were filled by contacting the participants in question. Participant demographic and key clinical characteristics were compared across the two groups using one-way analysis of variance (ANOVA) or independent sample t-tests for continuous variables and chi-square tests for categorical variables (see Table 1). Standard multiple regression was performed between parent-reported externalizing symptoms (z score) in their child—dependent variable, parent-reported SAS (z score)-independent variable and Indigeneity as the moderator variable. Preliminary assumption testing was performed to ensure there were no violations of normality, linearity, outliers, missing data, multicollinearity and homoscedasticity of residuals. A scatterplot of parent-reported SAS (z score) and parent-reported externalizing symptoms (z score) was composed with linear regression lines for Indigenous and non-Indigenous participants (see Figure 3).
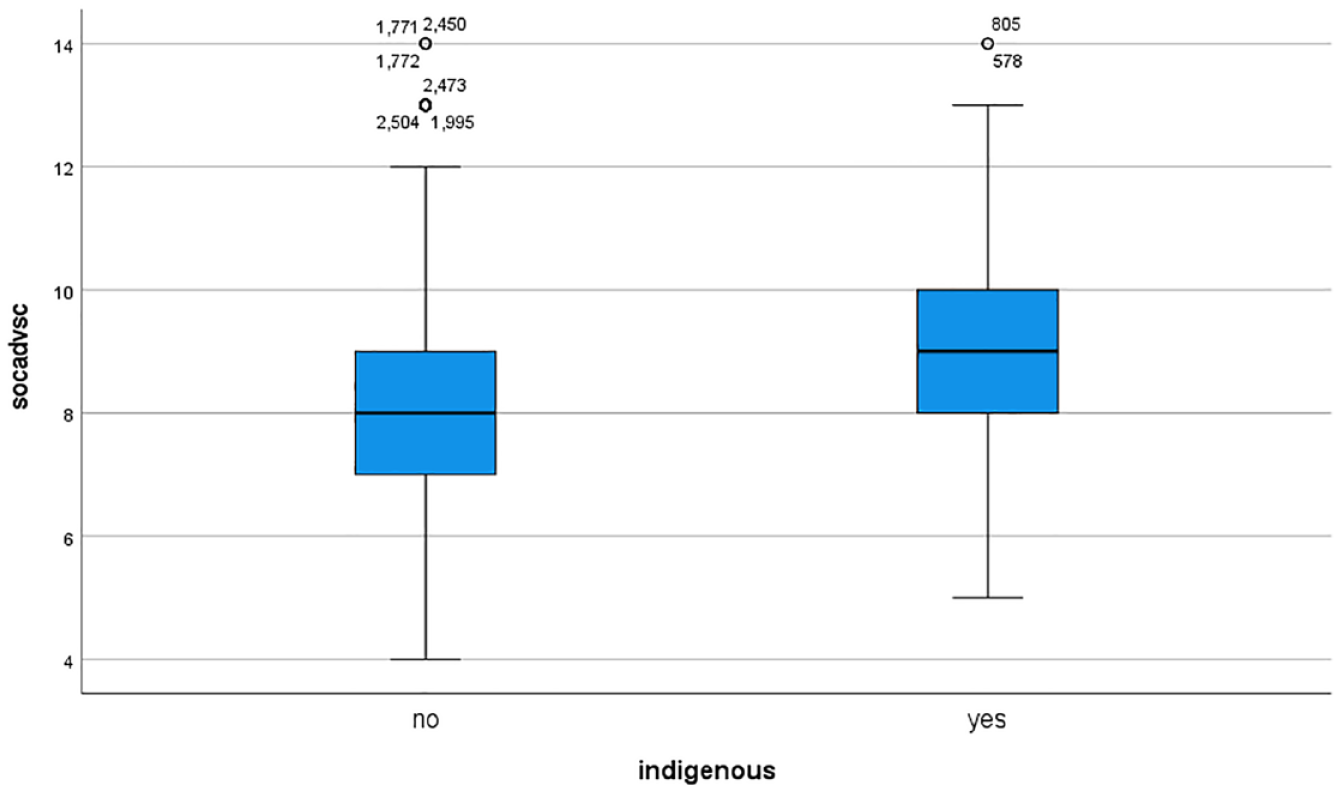
Boxplot of social adversity status (raw score) for Indigenous (yes) and non-Indigenous (no) participants.
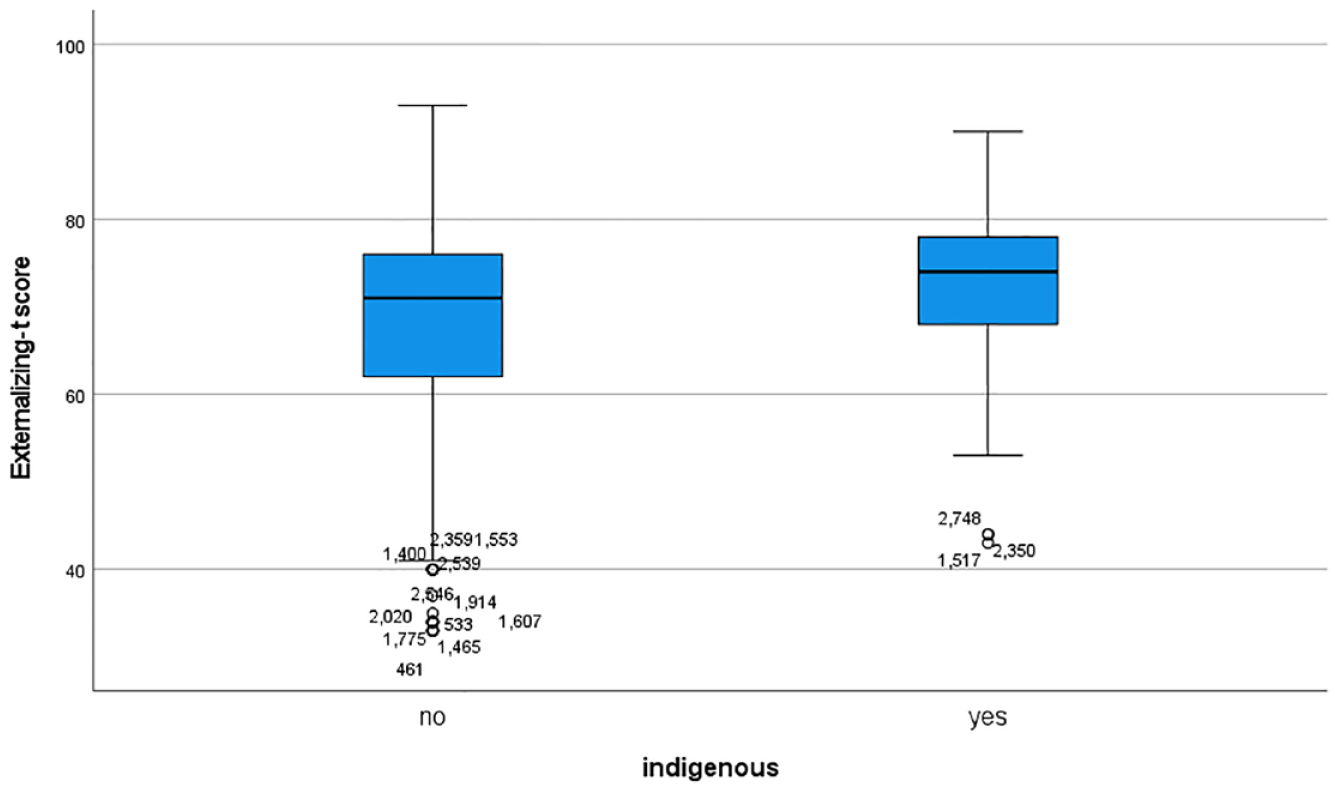
Boxplot of parent-reported externalizing symptoms (T score) for Indigenous (yes) and non-Indigenous (no) participants.
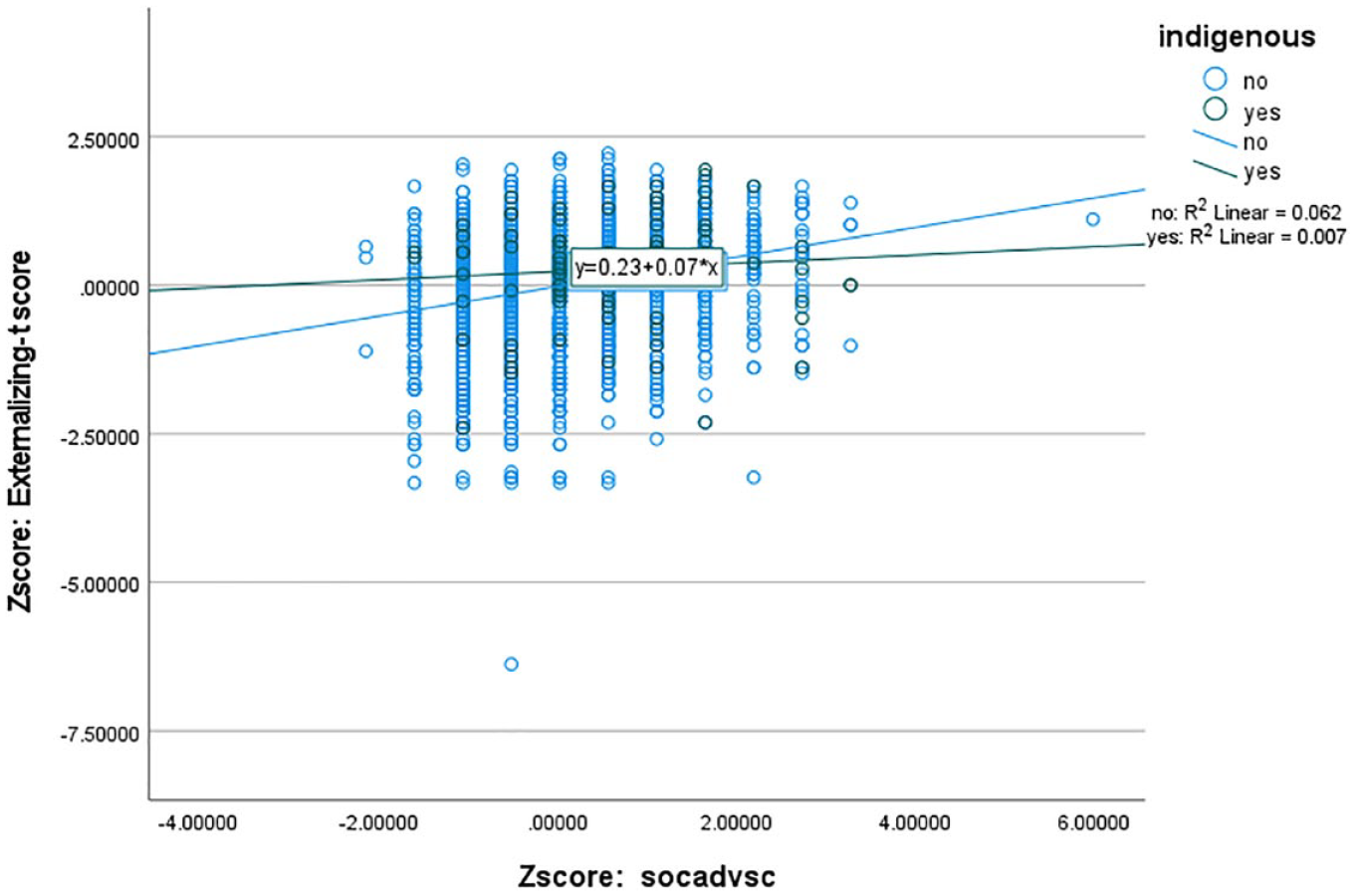
Scatterplot of social adversity status (z score) and parent-reported externalizing symptoms (z score) with linear regression lines for Indigenous and non-Indigenous participants.
Results
The Indigenous clinical group had higher parent-reported externalizing symptoms—small effect size difference—and SAS—medium effect size difference—than the non-Indigenous clinical group (see Table 1). DSM mental disorders and Intelligence quotients for these two groups are reported in Vance et al. (2022). Normality plots with statistics for the two groups with (1) SAS and (2) parent-reported externalizing symptoms revealed that none of the groups were normally distributed for either variable (Kolmogorov–Smirnov with Lilliefors correction—p < 0.05; see Table 1). However, relevant median values, Skewness and Kurtosis values (within ±1.0), and box plot graphs revealed all the distributions were acceptable for moderator analysis (see Table 1, Figures 1 and 2; Baron and Kenny, 1986; Mishra et al., 2019).
The findings revealed that Indigeneity, SAS and externalizing symptoms had small positive correlations with each other (see Table 2). Moreover, Indigeneity (B = 2.72 [95% CI = 0.24–5.20], p < 0.05) and SAS (B = 2.69 [95% CI = 2.22–3.16], p < 0.0005) made independent significant positive contributions to externalizing symptoms. In contrast, the interaction between Indigeneity and SAS (B = −1.94 [95% CI = −3.97 to −0.09], p = 0.06) had a nonsignificant negative trend to externalizing symptoms (see Figure 3). The non-Indigenous participants appeared to manifest a trend of increasing externalizing symptoms with increasing SAS but this was not evident to the same extent in the Indigenous group (see Figure 3).
Bivariate correlations for parent-reported externalizing symptoms (z score), social adversity status (z score), Indigeneity, and interaction between Indigeneity and social adversity status.
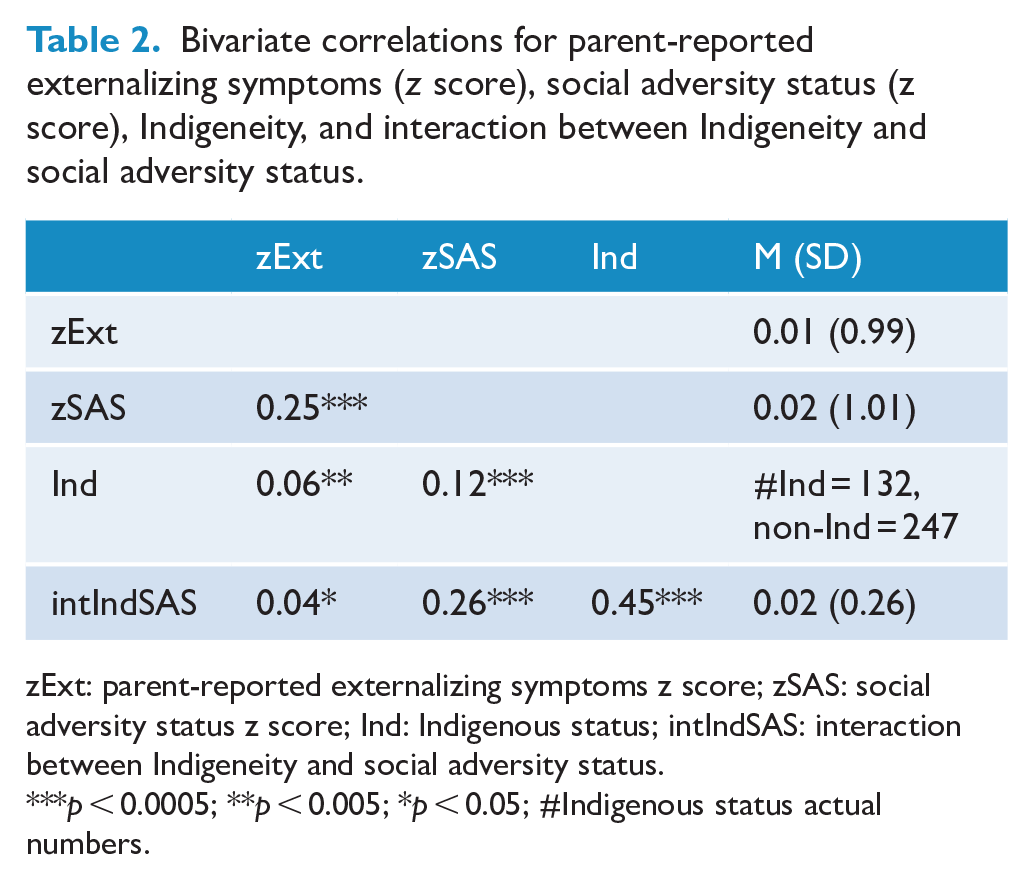
zExt: parent-reported externalizing symptoms z score; zSAS: social adversity status z score; Ind: Indigenous status; intIndSAS: interaction between Indigeneity and social adversity status.
p < 0.0005; **p < 0.005; *p < 0.05; #Indigenous status actual numbers.
Discussion
The Indigenous group manifest increased parent-reported externalizing symptoms and higher SAS than the non-Indigenous clinical group, consistent with the extant epidemiological literature (AIHW, 2018, 2020; Australian Bureau of Statistics (ABS), 2016) and clinical literature (Vance et al., 2022; 2023). However, these factors have not led to worse clinical impairment as the two clinical groups were matched for parent-reported mental disorder symptom severity, symptom-linked distress and the degree of impairment due to the mental disorder symptoms. Their clinical homogeneity was further evident given they did not differ in the main types of clinical problems leading to their referral to mental health services, the psychological management and/or the medications trialed at the time of their referral. Increased externalizing symptoms in Indigenous young people are crucial to recognize and appropriately manage, given the potential to promote more adaptive behaviors and prevent development of conduct disorder (Rowe et al., 2010), antisocial personality disorder and future imprisonment (Olino et al., 2010).
Higher SAS is associated with externalizing symptoms in non-Indigenous young people consistent with the extant literature (Adler and Stewart, 2010; Elgar et al., 2015; Piotrowska et al., 2015). In contrast, despite higher social adversity, Indigenous young people do not necessarily externalize. This finding is consistent with a wide ranging literature noting the possible protective factors aiding Indigenous young people in their communities and potentially decreasing externalizing symptoms (Calma et al., 2017; Dudgeon et al., 2016; Hawthorne, 2018; Prehn and Ezzy, 2020; Zubrick et al., 2010). Social and emotional wellbeing is directly proportional to the network of relationships Indigenous young people have with their family, kinship network and community (Calma et al., 2017; Dudgeon et al., 2016; Zubrick et al., 2010). Their connections to Country, Cultural practices, Ancestral Spirits and Spirits of Country are also crucial (Dudgeon et al., 2016; Hawthorne, 2018; Prehn and Ezzy, 2020). Increased number of carers for Indigenous young people may be a direct result of the extended family, kinship and community networks available for them (Calma et al., 2017; Zubrick et al., 2010). These carers frequently provide deep secure attachments and add unique culturally deep life skills for Indigenous young people (Dudgeon et al., 2016; Hawthorne, 2018).
This stands in direct contrast to a western perspective that often emphasizes the attendant risks of multiple carers associated with insecure attachment and ad hoc internalization of life skills (Claessens and Chen, 2013). A similar argument can be made for increased numbers of siblings in the home—a common finding in Indigenous households (Vance et al., 2023). Similarly, a western viewpoint often sees an increased regional location for the home address for Indigenous young people as linked to limited to access to welfare, health and educational services and employment opportunities. In contrast, such regional locations are often linked to Indigenous enclaves (‘villages’) where there are many culturally safe and appropriate resources implicitly available for young people to learn from (Vance et al., 2023). Indeed Hopkins et al. (2014) and Gennetian et al. (2012) note that Indigenous young people that move from absolute and relative poverty into socioeconomically advantaged areas may experience substantial stresses linked to relative isolation from extended family, community and cultural supports, and possibly from smaller family size with decreased sibling number. This may then be linked with increasing parent-reported externalizing symptoms, although no extant research to date verifies this change.
It is therefore crucial that Indigeneity is identified early as part of the clinical mental health assessment of young people and their families. Targeted holistic management can follow a comprehensive cultural and bio-psycho-social formulation that ensures SAS features are addressed (Bhat et al., 2020; Twizeyemariya et al., 2017). This may involve social work, welfare/legal professionals, and other health and mental health professionals working together in a culturally safe and appropriate way so all the factors outlined in a young person’s comprehensive formulation may be managed and/or advocated for. Clearly, managing SAS is imperative for all young people regardless of Indigenous status. But potential protective factors for Indigenous young people need to be ascertained and nurtured by multidisciplinary teams. From a research perspective, future systematic investigations of the contribution of key SAS factors of different magnitude to mental health referral pathways, presenting symptoms, diagnoses, psychosocial management strategies and effective medications are needed. Then, the relative contribution of particular SAS features of a young person’s presentation can guide societal resource allocation to address those factors of greatest import.
The main limitation of this study is the narrow definition of SAS factors examined. Although defined through clinical interview in a culturally valid and reliable manner, there remain many further factors in this domain to be carefully and systematically investigated in future studies. It is clear that the primary strength is our Indigenous young people being assessed by Indigenous mental health staff or AHLOs, ensuring that each impairing pattern of symptoms and associated functional impairment were correctly interpreted in the Indigenous group. Also there are no ceiling or floor effects for our measures of externalizing symptoms and SAS affecting our statistical analysis.
In conclusion, this study finds that Indigeneity is associated with increased parent-reported externalizing symptoms and higher SAS. While non-Indigenous young people appear to manifest worse externalizing problems with increasing SAS, Indigenous young people do not necessarily externalize despite higher SAS. There are a wide range of potential cultural protective factors that may help ameliorate the effect of increasing SAS. It is crucial that SAS factors of greatest magnitude are dealt with first and are managed and/or advocated for as part of treatment plans for all young people, regardless of Indigeneity. It also remains imperative to not disrupt those features that provide protection and enhance resilience for Indigenous young people and their communities and for health policy to take these into account. Future systematic investigations of the contribution of these protective factors to mental health referral pathways, assessment and management are needed.
Footnotes
Acknowledgements
We thank our Elder’s board, especially Uncle Herb Patten and Aunty Esther Kirby for the counsel and leadership, Karen Dally for her administrative support and Janice Dally for her data entry.
Author’s Note
Aboriginal Heritage, Alasdair Vance matrilineal Northern Wathaurung Mt Emu people; Jo Winther matrilineal Wadi Wadi Wemba Wemba people. Aboriginal Heritage, Janet McGaw by marriage to Alasdair Vance Northern Wathaurung Mt Emu people. Aboriginal Heritage, Angel O’Meara matrilineal Iman/Ghungalu and patrilineal Wiradjuri people. Joseph Gone is an enrolled member of the Aaniiih-Gros Ventre Tribal Nation of Montana, USA. Sandra Eades is a Noongar woman from Mount Barker, WA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project was funded by the Medical Research Future Fund Million Minds Program Grant (1179461). The funder of this study had no role in the study design, data collection, data analysis, data interpretation, and writing of the manuscript.
Data Sharing
All Indigenous data are under the control of our governing Victorian Traditional Custodian Elder’s board. Reasonable requests made to the corresponding author will be presented to the Elder’s board, and if approved, data will be made available.