
Abstract
Background:
Evidence suggests that externalizing and internalizing symptoms are expressed early in life and are associated with problematic drinking in young adulthood. However, few studies have examined their role during childhood and adolescence in predicting alcohol problems later in life.
Objectives:
To examine the role of childhood and adolescent externalizing and internalizing symptoms in predicting alcohol use disorders in young adulthood.
Methods:
We searched five electronic databases (PubMed, Scopus, PsycINFO, Web of Sciences and Embase) for studies which diagnosed alcohol use disorders through either the International Classification of Diseases or American Psychiatric Association – Diagnostic and Statistical Manual of Mental Disorders criteria and followed up children or adolescents into the transition to young adulthood. We performed a meta-analysis and obtained pooled odds ratio estimates with 95% confidence intervals using random-effects models.
Results:
A total of 12 longitudinal studies met eligibility criteria and were included in the meta-analysis. All measured the outcome using Diagnostic and Statistical Manual of Mental Disorders criteria. The majority were of good quality and were conducted in the United States. A total of 19,407 participants (50% female) were included in this meta-analysis. Of these, n = 2337 (12%) had diagnoses of alcohol use disorders/alcohol dependence. Participant ages ranged from birth to 36 years. Internalizing symptoms increased the risk of young adult alcohol use disorders by 21% (odds ratio = 1.21; 95% confidence interval = [1.05, 1.39]), with no strong evidence of publication bias. Subgroup analysis suggested significantly lower heterogeneity than for externalizing studies. Externalizing symptoms increased the risk of alcohol use disorders by 62% (odds ratio = 1.62, 95% confidence interval = [1.39, 1.90]). We found some evidence of publication bias and significant heterogeneity in the studies.
Conclusion:
Our findings highlight the contribution of early behavioural problems to the development of alcohol use disorders in young adulthood and the need for timely scrutiny of and intervention on early behavioural problems.
Introduction
Alcohol use disorders (AUD) are a severe form of alcohol use problems which commonly develop during late adolescence and young adulthood (Sher et al., 2005). AUD are associated with a range of adverse outcomes such as poor education and occupational attainment, and serious social and medical problems across the lifespan including high morbidity and mortality (World Health Organization, 2014).
A large body of evidence has consistently shown that externalizing symptoms correlate with substance use disorders (SUD) and predict AUD (Iacono et al., 1999; Krueger et al., 2002; Sher and Gotham, 1999). Behavioural disinhibition has been suggested as the core driver for the externalizing pathway (Krueger et al., 2002). Current evidence points to interactions between underlying vulnerability for behavioural disinhibition and high-risk environments, where the latter is reflected by deviant peer networks, impaired parenting and disruptive contexts (Hussong et al., 2011). Externalizing symptoms have a high heritability factor, varying from 81% (Krueger et al., 2002) to 84% (Young et al., 2000), and a shared vulnerability between antisocial behaviour and SUD has been suggested (Slutske et al., 1998).
On the other hand, the role of internalizing problems is less clear, possibly due to the dominance of the externalizing pathway (Hussong et al., 2011). Evidence suggests that the internalizing pathway may be relevant for a subset of individuals, who drink to cope with negative affect (Kuntsche et al., 2005) or believe that drinking can help relieve stress or tension (Schuckit et al., 2006). Others have reported that high levels of negative affectivity may not be sufficient to motivate drinking behaviour by itself, raising concerns about its causal link with AUD (Sher and Gotham, 1999).
Problematic alcohol consumption during adolescence is common in western countries such as Australia (Degenhardt et al., 2013), the United States (Johnston et al., 2013) and North European regions (Kuntsche et al., 2004). In a high proportion of adolescents, this drinking pattern persists into young adulthood with associated chronic consequences including AUD (McCambridge et al., 2011). Therefore, it is important to understand the factors that lead to persistence of this drinking pattern into young adulthood, given that interventions to prevent these problems in adolescence may have impact in young adulthood. This understanding can also help guide preventive measures targeted at early developmental stages.
Research from the field of developmental psychopathology emphasizes the existence of early risk factors in the aetiology of alcohol use and AUD in young adulthood (Hussong et al., 2011). Given that both externalizing and internalizing symptoms are expressed early in life, their role in adolescence in predicting alcohol problems later in life warrants examination. While a large body of evidence suggests an important role for externalizing symptoms, there are inconsistencies with respect to whether internalizing symptoms early in life predict alcohol initiation and alcohol use problems in young adults (Crum et al., 2008; Kjeldsen et al., 2018; Mayzer et al., 2009).
In this study, we perform a meta-analysis of data from longitudinal studies, estimating the separate pooled effects of internalizing and externalizing symptoms in childhood or adolescence to provide a better understanding of their roles in the development of AUD in young adulthood. This adds to the scarce longitudinal evidence on the mental health predictors of AUD tracked in these two important development life periods. Our approach is unique in that it thus allows us to separately quantify the relative roles of internalizing and externalizing symptoms, and to look specifically at AUD in a defined developmental period in which these often manifest. To increase our rigour, we focus on examining longitudinal studies which are the best source of evidence for temporal associations between mental health symptoms across childhood and adolescence and AUD in young adulthood. In addition, we limit the outcomes measured to those assessed clinically using a structured interview, either through the International Classification of Diseases (ICD) or through Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria.
Methods
This meta-analytic review was conducted in accordance with the preferred reporting items for systematic review and meta-analysis (PRISMA; Liberati et al., 2009). The protocol was registered in the International Prospective Register of Systematic Reviews (www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018088841).
Eligibility criteria
We included longitudinal studies that examined predictors of AUD or alcohol dependence (AD) among young adults, and followed up children or adolescents during the transition to young adulthood. Our study had an exclusive focus on longitudinal studies as these provide stronger evidence in support of temporal associations between specific exposures and outcomes. Studies in which the outcome was not assessed by structured clinical interview, using either ICD or DSM criteria, were excluded.
Given that young adulthood is most often defined as ranging from age 21 to the early 30s (Kosterman et al., 2014), studies for which the final follow-up age was in this range were included in this analysis. In addition, in order to ensure that the results were as widely generalizable as possible, we focused on population-based studies (see Figure 1).
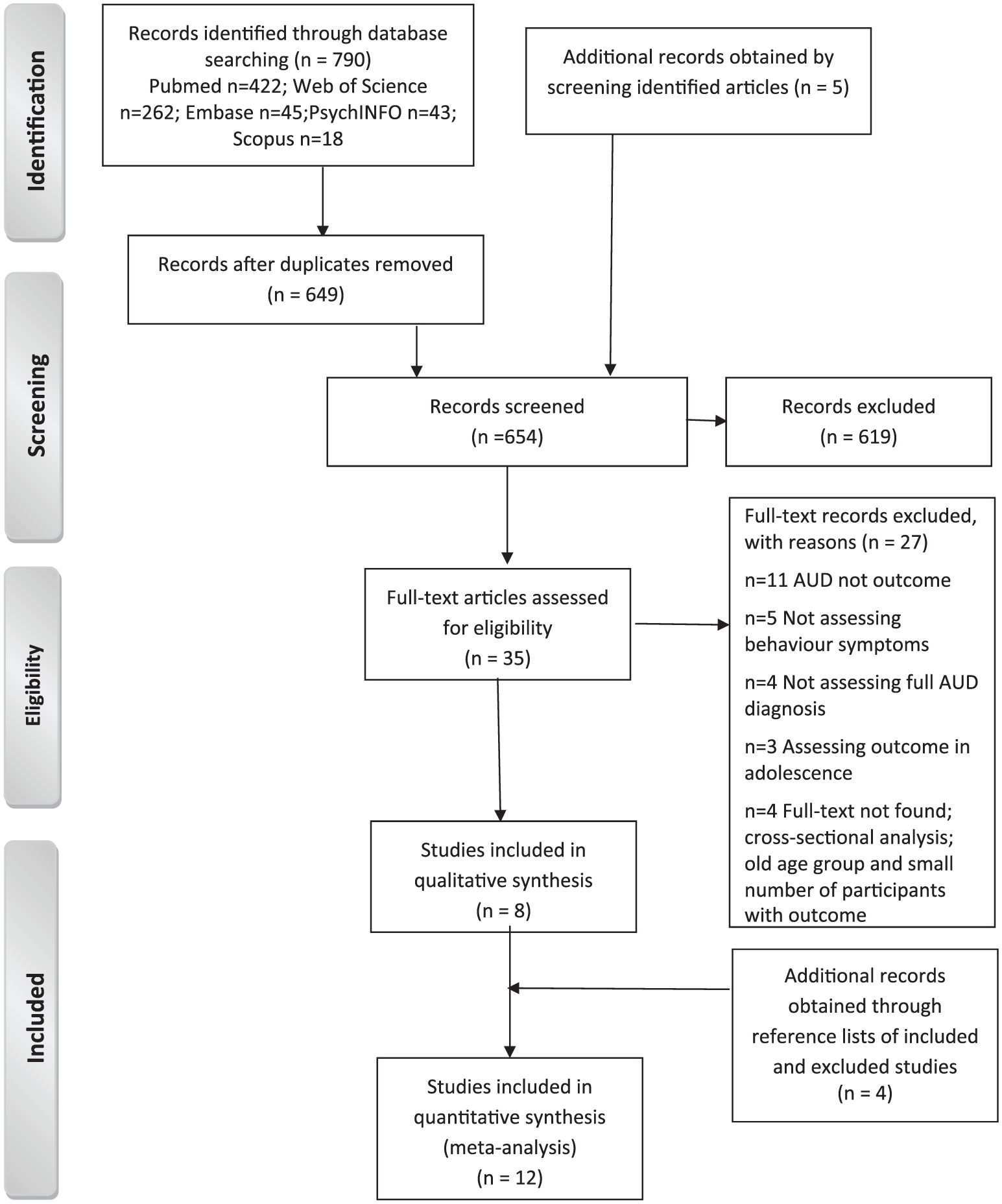
Flow diagram of the literature search.
Search strategy
We searched five electronic databases (PubMed, Scopus, PsycINFO, Web of Science and Embase) for studies published from database inception to January 2018. The search strategy combined the following four sets of terms. Internalizing search strategy: ‘internali* symptoms’ OR ‘internali* behavi*’ OR ‘anxiety’ OR ‘depressi*’ ‘depressive symptoms’ OR ‘mood disorder*’. Externalizing search strategy: ‘externali* symptoms’ OR ‘externali* behavi*’ OR ‘aggressive behavi*’ OR ‘antisocial behavi*’ OR ‘delinquen*’ OR ‘conduct disorder*’. Alcohol disorder search strategy: ‘alcohol disorder*’ OR ‘alcohol use disorder*’ OR ‘alcohol abuse*’ OR ‘alcohol dependence’ OR ‘problem* drinking’ OR ‘problem* alcohol use’ OR ‘drinking behavi*’. Young adult search strategy: ‘young adult*’ OR ‘youth’ OR ‘early adult*’. Only published articles were included. Language was restricted to English. Additional articles were found by screening the reference lists of eligible and excluded studies and forward searching for subsequent citations of these papers.
Study selection
Pertinent studies were identified by screening titles and abstracts. Articles were excluded unless the title or abstract focused on externalizing and internalizing symptoms as predictors of AUD among young adults. Where this was not clear, the full text of the article was screened. Screening, selection, data extraction and narrative synthesis were performed independently by two reviewers. Differences in article selection and quality were resolved by consensus.
Data synthesis and analysis
We converted all extracted estimates to odds ratios (ORs). Pooled ORs with 95% confidence interval (CI) were calculated using random-effects meta-analysis, as considerable between-study heterogeneity was expected (Berkey et al., 1995). Forest plots were constructed to show the study-specific and pooled estimates. Given that most of the included studies assessed more than one externalizing or internalizing symptom, the list of studies for each forest plot varied. Where studies assessed both externalizing and internalizing symptoms, they were included in the forest plot assessing each symptom set. Between-study heterogeneity was evaluated using Cochran’s Q statistic and I2 test statics (Higgins and Thompson, 2002). I2 statistics were calculated to describe the percentages of total variation across studies caused by heterogeneity. A zero value indicated no heterogeneity, 25% low, 50% moderate and 75% high level of heterogeneity (Higgins and Thompson, 2002). Subgroup analyses were also performed by exposure status, developmental stage of exposure, year of publication, country, outcome type, the tool used to assess internalizing and externalizing symptoms and study quality, as possible sources of heterogeneity between studies. Sensitivity analysis was also performed by stepwise exclusion of each study and calculating a pooled estimate for the remaining studies. The presence of publication bias was examined using Egger’s test (p < 0.05; Egger et al., 1997). All statistical analyses were performed using STATA14 metan package.
Quality assessment
We used the Newcastle-Ottawa Quality Assessment tool for cohort studies (Wells et al., 2016) to assess the quality of the included studies against Selection, Comparability and Outcome criteria. Studies received a maximum of 1 star for each numbered item within the Selection and Outcome components and a maximum of 2 stars for Comparability. Quality scores were assigned by summing scores across the three components. Results were summarized in three categories: good (3 or 4 stars in Selection domain AND 1 or 2 stars in Comparability domain AND 2 or 3 stars in Outcome domain); fair (2 stars in Selection domain AND 1 or 2 stars in Comparability domain AND 2 or 3 stars in Outcome domain) or poor (0 or 1 star in Selection domain OR 0 stars in Comparability domain OR 0 or 1 star in Outcome domain) quality. Quality assessments were carried out by two authors independently (I.M. and C.S.) and any discrepancies were resolved through discussion.
Results
Eligible studies
Figure 1 shows the PRISMA flowchart summarizing phases of the search. The electronic searches identified 790 articles. Five additional articles were selected from the reference lists of the identified studies. After duplicate removal and screening, 35 potentially relevant articles were retrieved for full-text assessment. A total of 27 articles were excluded, leaving 8 articles which met the eligibility criteria. Four studies were added from reference lists of included and excluded studies, giving a final total of 12 studies for the meta-analysis, of which 5 assessed externalizing symptoms and 7 assessed internalizing symptoms. AUD not being the outcome under study was the most frequent reason for exclusion.
Study characteristics
All 12 eligible studies featured prospective cohorts and were published between 2001 and 2015. A summary of the characteristics of the included studies is presented in Supplemental Table S1. Nine were assessed to be of good quality and three of fair quality (Supplemental Table S2). The majority of studies had high retention rates across waves. The studies were predominantly conducted in the United States (n = 8; Buckner and Schmidt, 2009; Farmer et al., 2016; Grant et al., 2001; Guo et al., 2001; Hill et al., 2011; Jackson and Sher, 2003; Palmer et al., 2013; Pardini et al., 2007) with the remaining studies in Australia (n = 2; Alati et al., 2005; Bonomo et al., 2004), New Zealand (n = 1; Fergusson et al., 2007) and Germany (n = 1; Behrendt et al., 2011). All eligible articles were written in English and sample sizes ranged from 378 (Jackson and Sher, 2003) to 5792 (Grant et al., 2001). A total of 19,407 participants (49.9% female; n = 9688 women and n = 9719 men) were included in this meta-analysis. Of these, n = 2337 (12%) had diagnoses of AUD/AD. The populations were either school/university, community or birth cohorts. Participant ages ranged from birth to 36 years.
All studies measured the outcome using American Psychiatric Association (APA) – DSM diagnostic criteria, either DSM-III, DSM-III-R, DSM-IV or DSM-V. The outcome was measured during young adulthood only (Alati et al., 2005; Bonomo et al., 2004; Buckner and Schmidt, 2009; Fergusson et al., 2007; Guo et al., 2001; Hill et al., 2011; Palmer et al., 2013; Pardini et al., 2007), or in adolescence and young adulthood (Behrendt et al., 2011; Farmer et al., 2016; Grant et al., 2001; Jackson and Sher, 2003).
Study findings
Externalizing symptoms and the risk of AUD
Of the included studies, 10 assessed externalizing symptoms, as reflected by antisocial behaviour, conduct disorders, delinquency, attention and hyperactivity problems during adolescence, against the risk of AUD (Alati et al., 2005; Farmer et al., 2016; Guo et al., 2001; Hill et al., 2011; Jackson and Sher, 2003) or AD (Bonomo et al., 2004; Fergusson et al., 2007; Grant et al., 2001; Guo et al., 2001; Palmer et al., 2013; Pardini et al., 2007) in young adulthood. Four studies assessed externalizing symptoms using DSM diagnostic criteria (Farmer et al., 2016; Hill et al., 2011; Palmer et al., 2013; Pardini et al., 2007), and the remaining studies used well-established, validated, self-report scales. One study assessed the mediating role of behavioural undercontrol in the relationship of family history of problematic drinking with AUD (Jackson and Sher, 2003).
Overall, most studies found positive associations of externalizing symptoms with AUD and/or AD in young adulthood. However, associations of attention and hyperactivity problems with AUD and AD were mixed. After accounting for early substance use (including alcohol), two studies failed to find an association (Palmer et al., 2013; Pardini et al., 2007). Hill et al. (2011) found positive associations, but the level of adjustment in this study was limited to gender and familial risk status.
The pooled effect of studies included in the meta-analysis showed that externalizing symptoms are associated with an increased risk of AUD in young adulthood (OR = 1.62; 95% CI = [1.39, 1.90]). There was evidence of publication bias (coefficient = 1.99, p = 0.001) and significant heterogeneity among studies measuring this association (Q = 111.10, p < 0.001, I2 = 80%) (Figure 2). Sensitivity analysis suggested similar pooled associations when each of the estimates was excluded from the model (results not shown).
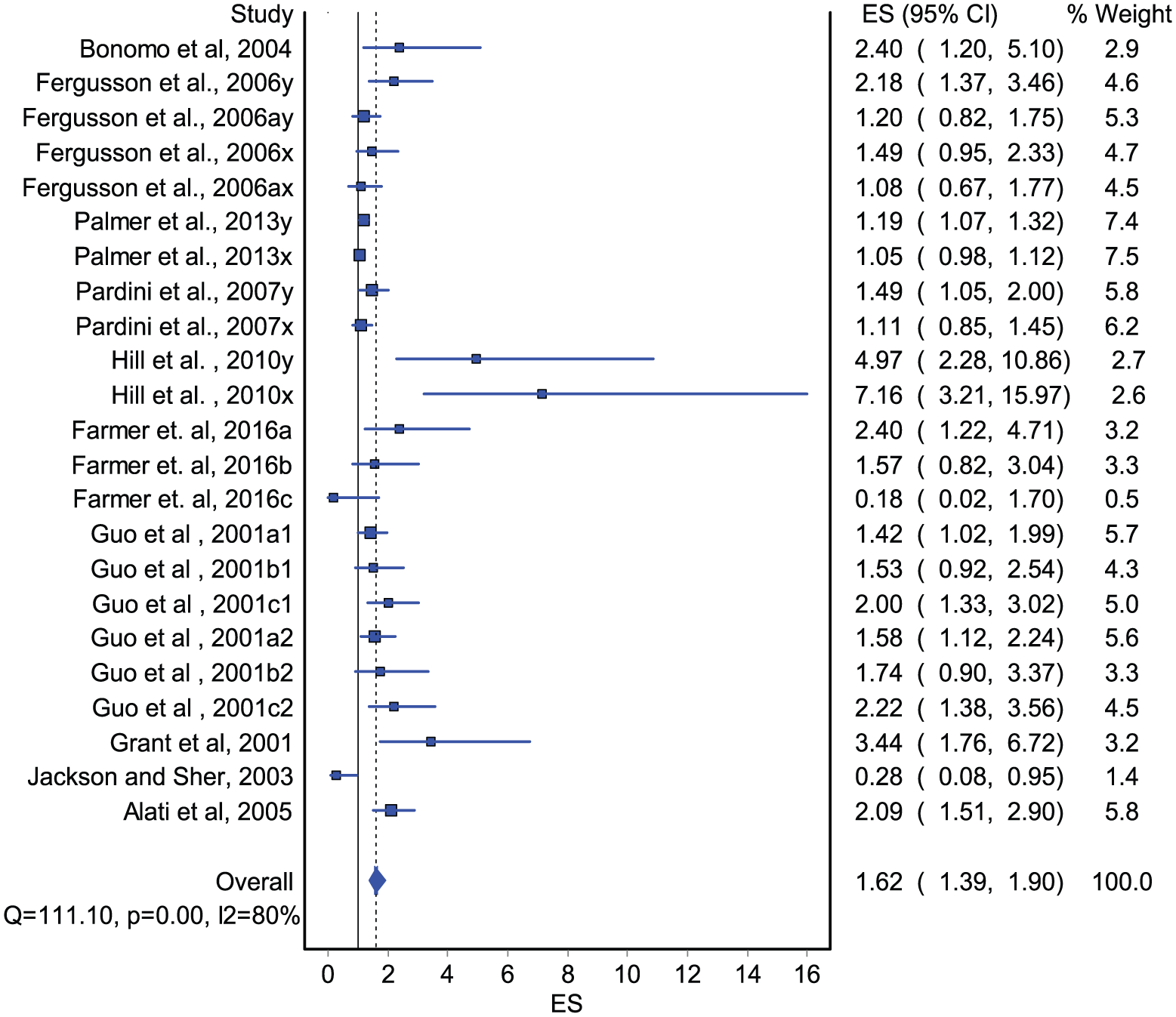
Forest plot assessing externalizing symptoms in adolescence and AUD or AD in young adulthood (pooled OR, 95% confidence intervals).
We conducted subgroup analyses by exposure type, age of exposure, exposure screening tool, type of outcome, country and year of study publication. This analysis showed stronger effect estimates among those who had antisocial symptoms (OR = 1.80, 95% CI = [1.51, 2.16]). No between-study heterogeneity was noted among these studies (Q = 8.04, p = 0.33, I2 = 13%; Table 1). The risk of AUD was also higher among those who had conduct disorders (OR = 1.72, 95% CI = [1.26, 2.35]), although we noted a high degree of heterogeneity among these studies (Q = 27.86, p < 0.001, I2 = 76%).
Subgroup analysis of externalizing symptoms and the risk of AUD or AD.
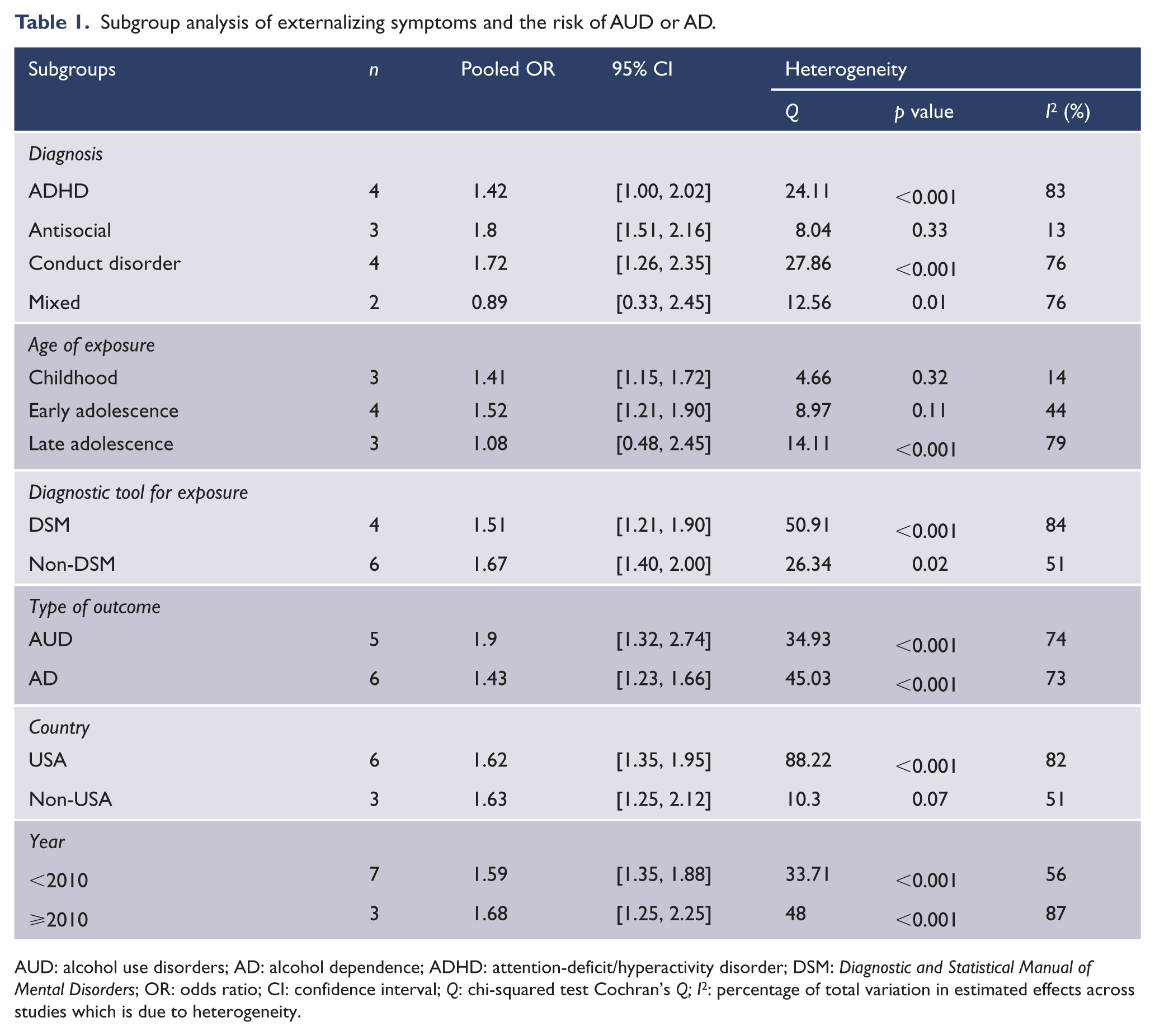
AUD: alcohol use disorders; AD: alcohol dependence; ADHD: attention-deficit/hyperactivity disorder; DSM: Diagnostic and Statistical Manual of Mental Disorders; OR: odds ratio; CI: confidence interval; Q: chi-squared test Cochran’s Q; I2: percentage of total variation in estimated effects across studies which is due to heterogeneity.
Subgroup analysis by age of exposure suggested that externalizing symptoms in childhood increased the risk of young adult AUD by 41% and in early adolescence by 52%. No heterogeneity was detected between groups (Table 1). The effect of externalizing symptoms was higher for AUD (OR = 1.90, 95% CI = [1.32, 2.74]) than for AD (OR = 1.43, 95% CI = [1.23, 1.66]) (Table 1). Regarding the screening instruments used, lower estimates were found among studies that used DSM (OR = 1.51, 95% CI = [1.21, 1.9]) than non-DSM (OR = 1.67, 95% CI = [1.40, 2.00]) instruments. We opted not to perform subgroup analysis by quality as all studies had been assessed as having fair or good quality.
Internalizing symptoms and the risk of AUD
Seven studies examined internalizing symptoms (comprising anxiety and depression), and inconsistent associations were found. Two studies found positive associations of anxiety with AUD and AD after adjustment for prior alcohol use (Pardini et al., 2007) and depression (Buckner and Schmidt, 2009). However, when internalizing symptoms were analysed in combination (i.e. depression and anxiety symptoms together), results were mixed. After accounting for externalizing symptoms, one study found a positive association (Behrendt et al., 2011) and two (Alati et al., 2005; Farmer et al., 2016) found none. Depression alone, assessed using either self-reported scale or DSM criteria, was not associated with AUD (Hill et al., 2011) or AD (Pardini et al., 2007).
The pooled effect for studies included in the meta-analysis suggested that internalizing symptoms in childhood and adolescence are associated with an increased risk of AUD in young adulthood (OR = 1.21, 95% CI = [1.05, 1.39]; Figure 3). We found significant between-study heterogeneity, but no publication bias (coefficient = 0.96, p = 0.089).
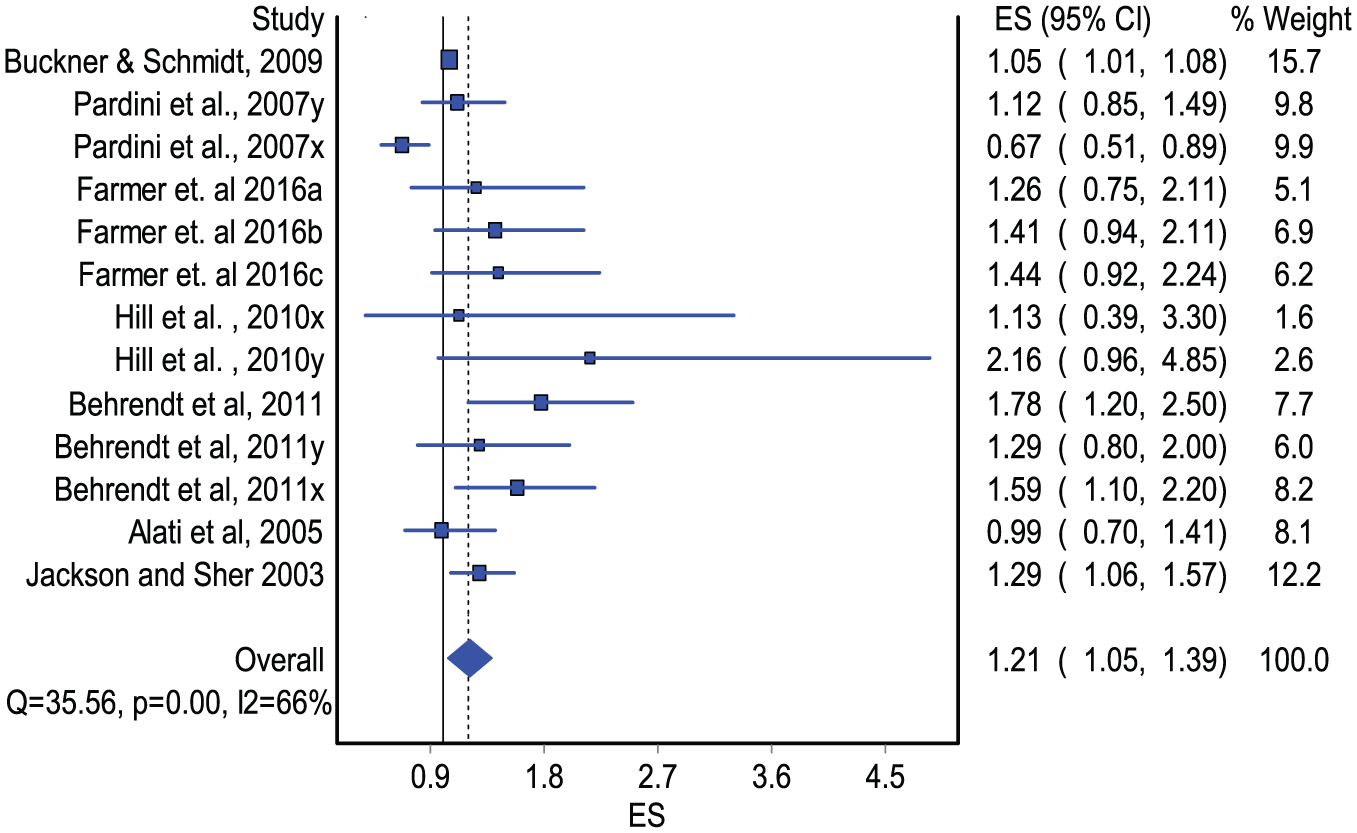
Forest plot of studies assessing internalizing symptoms in adolescence and AUD or AD in young adulthood (pooled OR with 95% confidence intervals).
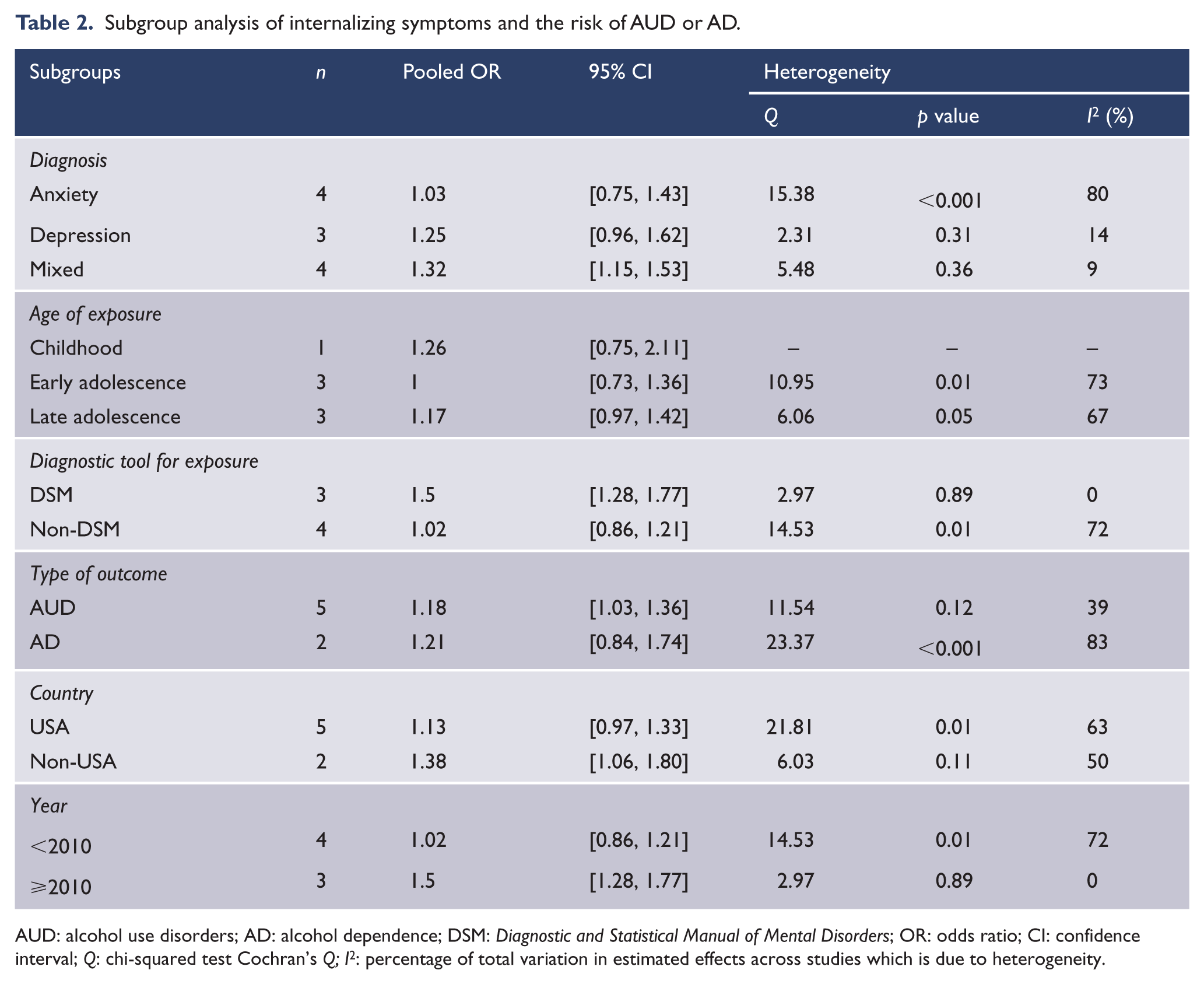
We again conducted subgroup analysis (see Table 2) and found significantly less heterogeneity among those studies published after 2010 (OR = 1.50, 95% CI = [1.28, 1.77], I2 = 0%) and outside the United States (OR = 1.38, 95% CI = [1.06, 1.80], I2 = 50%). In addition, we found lower heterogeneity among studies which used AUD as their outcome (OR = 1.18, 95% CI = [1.03, 1.36], I2 = 39%), used DSM criteria to measure internalizing symptoms (OR = 1.50, 95% CI = [1.28, 1.77], I2 = 0%), and studies measuring depression only (OR = 1.25, 95% CI = [0.96, 1.62], I2 = 14%) or depression and anxiety in combination (OR = 1.32, 95% CI = [1.15, 1.53], I2 = 9%) (Table 2). Sensitivity analysis again suggested similar pooled associations when each of the estimates was excluded from the model (results not shown).
Subgroup analysis of internalizing symptoms and the risk of AUD or AD.
AUD: alcohol use disorders; AD: alcohol dependence; DSM: Diagnostic and Statistical Manual of Mental Disorders; OR: odds ratio; CI: confidence interval; Q: chi-squared test Cochran’s Q; I2: percentage of total variation in estimated effects across studies which is due to heterogeneity.
Discussion
This is the first meta-analysis that assesses the role of early internalizing and externalizing symptoms in the aetiology of AUD in young adulthood. Findings from this meta-analysis suggest that both internalizing and externalizing symptoms increase the risk of AUD, by 21% and 62%, respectively. Our findings are consistent with those from a meta-analysis of prospective studies assessing the risk of mental health disorders with subsequent substance-related disorders (Groenman et al., 2017), where childhood attention-deficit/hyperactivity disorder, oppositional defiant disorder, conduct disorder and depression all increased the risk of developing substance-related disorders (including AUD). Our meta-analysis suggests that both internalizing and externalizing symptoms in childhood or adolescence can also lead to AUD later in life.
Our pooled analyses point to an effect of internalizing symptoms on AUD. This partly supports existing evidence. Groenman et al.’s (2017) findings described above suggested a link between childhood depression and subsequent SUD. There is also evidence of an association between internalizing symptoms and adolescent alcohol use even when controlling for externalizing symptoms (Merikangas et al., 1998; Sung et al., 2004). However, there are also conflicting findings, where no associations or positive associations were found between internalizing symptoms and adolescent alcohol use after accounting for externalizing symptoms (Fleming et al., 2008; Kaplow et al., 2001; Maslowsky et al., 2014; Scalco et al., 2014). Because of this mixed evidence, both risk and protective mechanisms for the association of internalizing symptoms and problematic drinking have been proposed. One of the most commonly proposed risk mechanisms for the internalizing pathway is self-medication of negative emotional experiences such as anxiety and depression, in which substance use is motivated by a desire to reduce emotional distress (Hussong et al., 2011; McCarthy et al., 2010). A recent study that investigated the direct and indirect temporal associations of internalizing and externalizing symptoms with alcohol use problems offered some support for this mechanism but suggested that these associations may be multi-directional and so more complex (Foster et al., 2018).
Evidence from studies showing positive associations of a range of externalizing symptoms with problematic drinking is well replicated (Englund et al., 2008; Miller et al., 2016). The mechanisms behind these associations are still unclear, as is our understanding of the diverse characteristics that comprise the behaviours of the externalizing domain. One main proposed mechanism involves a vulnerability to behavioural disinhibition that is exacerbated by social environmental factors such as exposure to stress and family conflict and possibly by precocious alcohol and other drug use (McGue et al., 2001; Zucker et al., 2011). Similarly, others suggest that externalizing symptoms are likely to exclude youth from prosocial peer groups and encourage them to select and engage with deviant peers who provide opportunities and reinforcement for alcohol and drug use (Dodge et al., 2009; Hawkins et al., 1992). In addition, an earlier study among twin pairs indicated the existence of substantial genetic links between antisocial behaviour and SUD (Slutske et al., 1998). In that study, the authors showed that both childhood conduct disorder and AD were substantially heritable, with genetic influences accounting for 76% and 71% of the conduct disorder and AD phenotypes, respectively.
In general, we found that mental health symptoms that predict clinically diagnosed AUD can also predict the development of binge/risky drinking and problematic drinking (Miller et al., 2016; Mushquash et al., 2013). From this, we can conclude that either there is no pathway that specifically distinguishes AUD from other forms of problematic drinking, or binge/risky drinking or problematic drinking may be on the causal pathway of developing AUD in young adults. Thus, given the complexity of AUD aetiology, more studies are needed to clarify its distinctive pathways from risks experienced early in life.
It is worth noting that some characteristics of the included studies may have affected our analysis. First, studies did not clearly distinguish the temporality between adolescent alcohol use and symptoms of externalizing and internalizing problems. Accounting for prior adolescent alcohol use may have allowed this issue to be addressed. Although the majority of the studies included in this meta-analysis assessed adolescent alcohol use, only one (Pardini et al., 2007) accounted for it in the modelling and found that early conduct disorder symptoms strongly predict AUD symptoms and AD in young adulthood. Thus, prospective studies that make this distinction are needed. Second, we found a moderate degree of heterogeneity among studies measuring both symptoms, mostly among those measuring externalizing symptoms. It is possible that methodological issues are the origin of heterogeneity for studies of both sets of symptoms. It may be that measures of internalizing symptoms were less reliable and may show lower rates of inter-reporter agreement than those of externalizing symptoms (De Los Reyes and Kazdin, 2008). For instance, we noted that, among studies measuring internalizing symptoms, depression and mixed diagnoses were assessed using DSM criteria, whereas anxiety was assessed using self-report subscales.
Third, the included studies did not directly assess the comorbidity of internalizing and externalizing problems in the aetiology of AUD, although a few included studies investigated both problems (Alati et al., 2005; Farmer et al., 2016; Jackson and Sher, 2003; Pardini et al., 2007). AUD commonly co-occurs with other psychopathologies (Jones et al., 2018; Mewton et al., 2011). It has been estimated that 20–65% of alcohol-dependent patients also suffer from other mental health disorders (El-Guebaly, 1990). Evidence also suggests the co-occurrence of both externalizing and internalizing symptoms in the developmental pathway of AUD (Colder et al., 2013; Kessler et al., 2011; Lilienfeld, 2003). Given that the comorbidity of these behaviours can lead to weaker but statistically significant association with substance disorders (Colder et al., 2013), there is a possibility that the pooled positive estimates of studies assessing internalizing symptoms may have resulted from the comorbidity with externalizing symptoms. In fact, we found that most studies showed that early externalizing symptoms predicted AUD later in young adulthood when these symptoms co-occurred with internalizing symptoms. However, most studies that investigated the role of internalizing symptoms while adjusting for externalizing symptoms found no effects (Alati et al., 2005; Farmer et al., 2016). Our overall findings are thus partly consistent with those from a longitudinal study (Foster et al., 2018) which suggests that co-occurrence of internalizing and externalizing symptoms may obscure the impact of internalizing symptoms on alcohol problems. Thus, there is a need to better clarify the role of internalizing symptoms in the aetiology of AUD, while taking into account the heterogeneity of internalizing conditions, the type of diagnostic tools and the comorbidity with externalizing symptoms.
Finally, we were not able to test the gender interactions of both symptoms on AUD. Only one study provided separate risk estimates for boys and girls (Alati et al., 2005). This is important because evidence shows that symptoms are unequally prevalent among boys (more likely to externalize; Leadbeater et al., 1999) and girls (more likely to internalize; Bor et al., 2014). Addressing these gaps will contribute to a better understanding of the role of these early-life behavioural problems in the aetiology of AUD in young adulthood.
Findings from this study have clinical relevance and implications for prevention. They highlight the need for timely scrutiny of and intervention in early behavioural problems, given their potential to contribute to later drinking problems. Interventions aiming to prevent and manage these behavioural problems early in life may reduce the likelihood of AUD in young adulthood. These may include screening for and treatment of mental health problems in children and adolescents who may present externalizing and internalizing symptoms characteristic of behavioural disinhibition or affective problems. Interventions in the specific social environments (including peers and family) aimed at reducing family conflict and early involvement with substances may also be helpful (Jones et al., 2018). Interventions are also needed to increase awareness of the risk of AUD later in life among those with problem behaviours.
Strengths of this meta-analysis include its ability to provide quantitative estimates of the associations of both internalizing and externalizing symptoms with AUD. The exclusive focus on longitudinal studies attempted to track predictors across developmental periods of childhood and adolescence and investigate the magnitude of their association with AUD, thus providing evidence of temporal associations. The majority of included studies were of good quality as assessed by the Newcastle-Ottawa Quality Assessment tool for cohort studies, with high retention rates. Importantly, we found no publication bias among studies measuring internalizing symptoms, which strengthens our clarification of previously inconsistent findings.
This meta-analysis also has limitations. We found some publication bias in studies assessing externalizing symptoms. This may be due to a general tendency to publish positive findings, or it may be that the well-replicated nature of associations between externalizing symptoms and AUD may have influenced the publication bias noted in our meta-analysis among studies measuring externalizing symptoms. Some studies were included more than once because they have reported separate analyses, by gender, for different development periods (childhood, adolescence and young adulthood) or for different outcomes (AUD, AD). The latter two may have biased our results if the same participants were counted more than once. Our findings may not be generalizable to other populations, given that all included studies were conducted in western countries and relevant studies published in a language other than English may have been missed. Another limitation is that our meta-analysis only included 12 studies and thus especially the subgroup analyses are likely to be statistically underpowered to detect any real differences between the subgroups. Last, we only included studies that have clinically diagnosed AUD. This may have excluded potential relevant studies from our analysis.
Despite these limitations, our meta-analysis adds to the growing but still limited literature on the effects of early internalizing symptoms on AUD in young adulthood, as well as aligning with established evidence for externalizing symptoms.
Conclusion
The presence of early internalizing symptoms predicts young adult AUD. Externalizing symptoms in childhood and adolescence are also predictors of AUD in young adulthood. Identification of problem behaviours in childhood and adolescent and early interventions may reduce the development of AUD during young adulthood. Further longitudinal studies are needed to address the methodological issues raised in this study.
Supplemental Material
Supplementary_Tables – Supplemental material for Externalizing and internalizing symptoms in childhood and adolescence and the risk of alcohol use disorders in young adulthood: A meta-analysis of longitudinal studies
Supplemental material, Supplementary_Tables for Externalizing and internalizing symptoms in childhood and adolescence and the risk of alcohol use disorders in young adulthood: A meta-analysis of longitudinal studies by Ivete Meque, Berihun Assefa Dachew, Joemer C Maravilla, Caroline Salom and Rosa Alati in Australian & New Zealand Journal of Psychiatry
Footnotes
Author Contributions
I.M. designed the search strategy, synthesized findings and wrote the first draft of the manuscript. I.M. and C.S. screened and extracted data from papers. J.C.M. and B.A.D. synthesized findings and revised the first draft. All authors contributed to conceptual discussions and revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
I.M. and J.C.M. were funded by the University of Queensland International Scholarships. B.A.D. was supported by the International Postgraduate Research Scholarship (IPRS) and Australian Postgraduate Award (APA).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.