
Abstract
Aims:
Community treatment orders have been introduced in many jurisdictions with increasing use over time. We conducted a rapid umbrella review to synthesise the quantitative and qualitative evidence from systematic reviews and/or meta-analyses of their potential harms and benefits.
Methods:
A systematic search of Medline, PubMed, Embase and PsycINFO for relevant systematic reviews and/or meta-analyses. Where available, participants on community treatment orders were compared with controls receiving voluntary psychiatric treatment. This review is registered with PROSPERO (CRD42023398767) and the Open Science Framework (https://osf.io/zeq35).
Results:
In all, 17 publications from 14 studies met the inclusion criteria. Quantitative synthesis of data from different systematic reviews was not possible. There were mixed findings on the effects of community treatment orders on health service use, and clinical, psychosocial or forensic outcomes. Whereas uncontrolled evidence suggested benefits, results were more equivocal from controlled studies and randomised controlled trials showed no effect. Any changes in health service use took several years to become apparent. There was evidence that better targeting of community treatment order use led to improved outcomes. Although there were other benefits, such as in mortality, findings were mostly rated as suggestive using predetermined and standardised criteria. Qualitative findings suggested that family members and clinicians were generally positive about the effect of community treatment orders but those subjected to them were more ambivalent. Any possible harms were under-researched, particularly in quantitative designs.
Conclusions:
The evidence for the benefits of community treatment orders remains inconclusive. At the very least, use should be better targeted to people most likely to benefit. More quantitative research on harms is indicated.
Keywords
Introduction
Community treatment orders (CTOs) require someone with a diagnosis of mental illness to follow a treatment plan while living in the community. The terminology can differ by jurisdiction. For instance, in Queensland, they are called ‘treatment authorities – community category, while in the United States they are often referred to as ‘assisted outpatient treatment’ or ‘outpatient commitment’ (Brophy et al., 2018). Generally, a serious mental illness must be present and a determination made that the person is at risk of serious harm while in most jurisdictions also lacking the capacity to weigh up the risks and benefits of appropriate treatment (Brophy et al., 2018). The order should also be the least restrictive means of providing the person with treatment and care. The use of CTOs in Australia is high by international standards (Light, 2019). This is despite nationwide reform of mental health legislation intended to improve the human rights of people with mental illness following the country’s adoption of the United Nations Convention on the Rights of Persons with Disabilities (Callaghan and Ryan, 2012). However, legislative changes have had minimal impact on the high rates of CTO use in Australia (Gill et al., 2020).
CTOs are a topic of debate among mental health experts, advocates and people placed on them. There is evidence of increasing use over time in countries such as England and Australia (House of Commons and House of Lords, 2023; Light, 2019). Despite widespread use, there have been relatively few systematic reviews (SRs) and/or meta-analyses of the potential harms and benefits of this approach. The scope of individual reviews has also been limited, quantitative reviews largely being restricted to health service use (Barnett et al., 2018) and particular countries (Kisely et al., 2023). We therefore conducted this rapid umbrella review to meet the time-sensitive needs of the Victorian Independent Review of Compulsory Treatment and Assessment Criteria and Alignment with Decision-Making Laws (Department of Health, 2022). To our knowledge, it is the first to synthesise quantitative and qualitative evidence from SRs of both these study designs worldwide. In particular, we assessed the possible harms and benefits of CTOs and whether these were perceived differently by clinicians, people on CTOs and their families or supporters.
A previous umbrella review of interventions to reduce coercive treatment included CTOs but was restricted to randomised controlled trials (RCTs) and only considered subsequent hospital admissions (Barbui et al., 2021). Because of the challenges of conducting RCTs in this area, it is likely that the participants may not have been typical of people who are placed on CTOs. In addition, it is important to consider a wider range of psychosocial outcomes, including possible harms. We therefore aimed to answer the following questions:
What are the effects of CTOs on health service, clinical and psychosocial outcomes including admissions, bed-days, community contacts, quality of life and interactions with the criminal justice system?
What are the views of clinicians, people on CTOs, families and supporters on the benefits and harms of CTOs including any differences by participant type in how they are perceived?
Method
Search strategy
The protocol for this rapid umbrella review was prospectively registered with the Open Science Framework (https://osf.io/zeq35) and PROSPERO (CRD42023398767) (see online Supplement 1). We followed guidelines from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Moher et al., 2009) and the guidance of the Cochrane Rapid Reviews Methods Group (Garritty et al., 2021). We also followed recommended practice which include the following features: a published protocol with predefined inclusion criteria; a standardised data extraction technique; a description of any overlap in meta-analyses of the same outcomes; estimations of common effect sizes where applicable; and assessments of study quality and heterogeneity (Aromataris et al., 2015; Fusar-Poli and Radua, 2018; Hunt et al., 2018; Pollock et al., 2019).
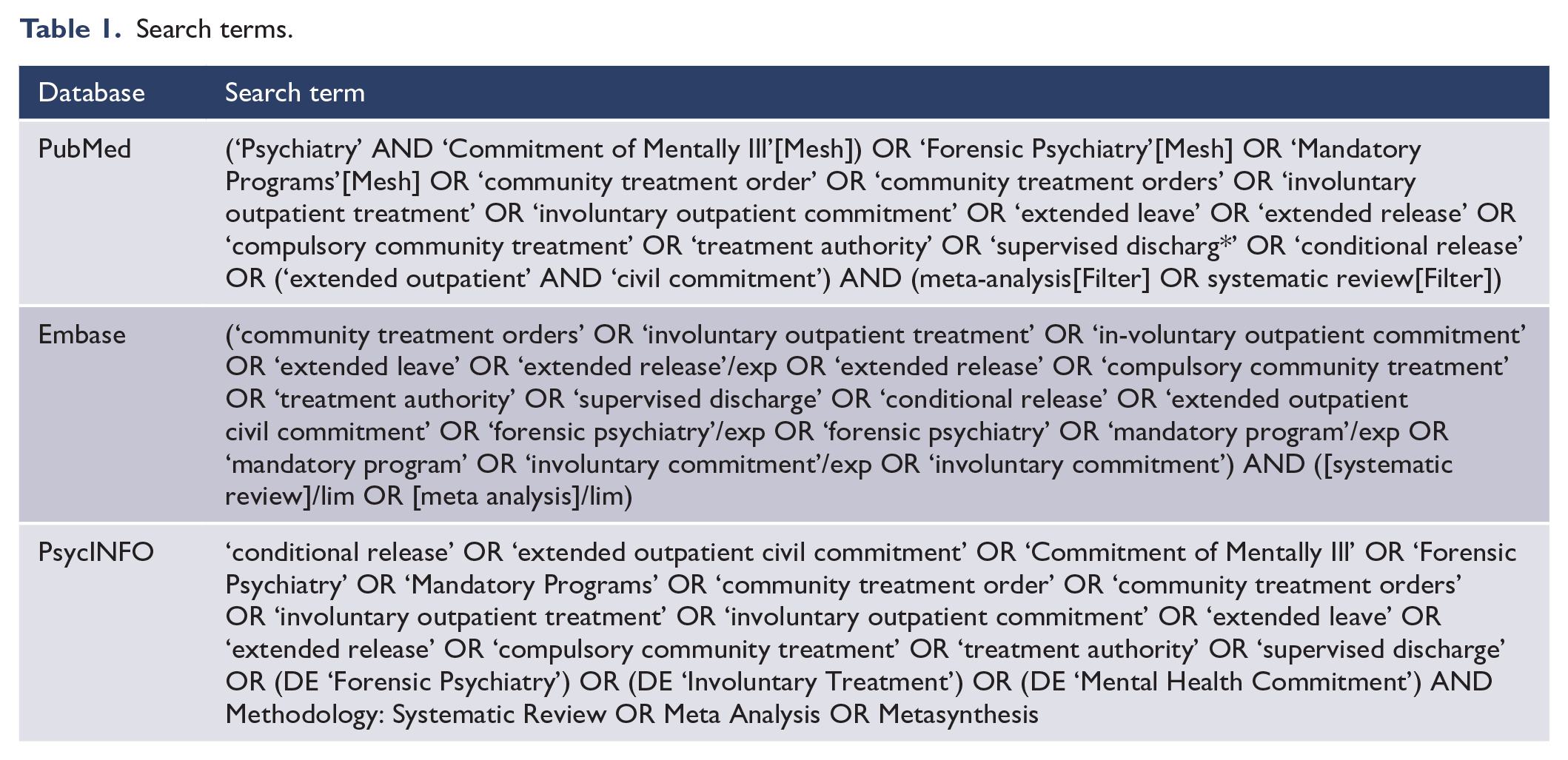
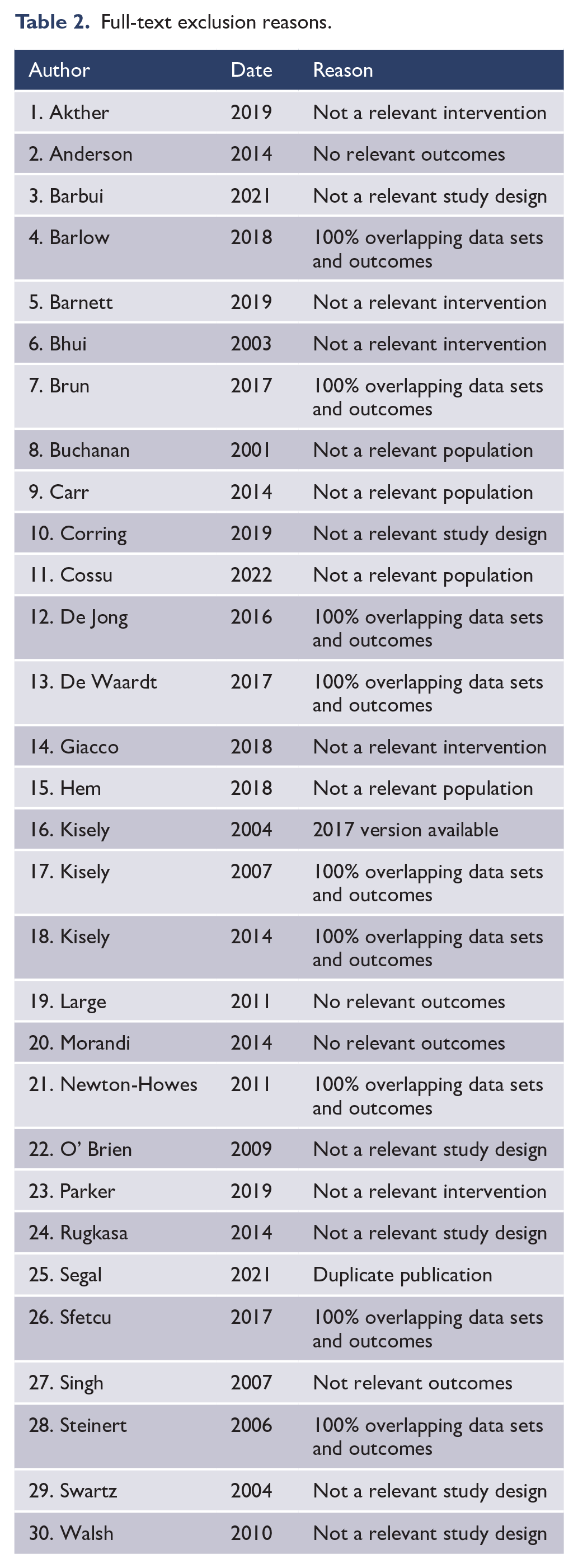
We searched the following databases from inception up to 19 January 2024: PubMed/Medline, Embase and PsycINFO for peer-reviewed research in humans with no language restrictions. Table 1 shows our final search terms following discussion with a professional librarian. Ethical approval was not required as all included primary data had previously been published. Table 2 shows the full-text exclusion reasons.
Search terms.
Full-text exclusion reasons.
Inclusion criteria
We included SRs and meta-analyses of both quantitative and qualitative research on the benefits and harms of CTOs for severe mental illness with, or without, comparisons to controls on voluntary psychiatric treatment. In line with recent guidance, SRs were defined as follows (Krnic Martinic et al., 2019): specific research questions, a reproducible search strategy, inclusion and exclusion criteria, selection methods and a list of included studies. There were no restrictions by language, the electronic versions of any papers in languages other than English being converted into an editable form in Adobe Acrobat Pro and translated using Google.
Exclusion criteria
We excluded studies of compulsory treatment of involuntary treatment in inpatient, forensic or criminal justice settings. We also excluded compulsory treatment for drug or alcohol dependence as these conditions are generally covered by different legislation and not included under the relevant mental health act. For instance, interventions are delivered in residential settings and/or as a result of contact with the criminal justice system (Coleman et al., 2021; Werb et al., 2016). Abstracts, editorials, narrative and scoping reviews were also excluded, as were individual studies of primary data. Finally, we excluded articles if 100% of the results were presented in exactly the same way in another study, giving preference to newer over older reviews.
Study selection and data extraction
Two of the authors (S.K. and T.Z.) independently screened articles by title and abstract, and then by full text for inclusion in the review. The reference lists of selected retrieved papers were screened to identify additional studies that met inclusion criteria. We also used Google Scholar to search forwards for citations of included studies. A third reviewer (L.B.) was consulted in the case of any disagreement and consensus achieved in all cases.
We extracted data as reported in the SRs, not from original studies. The following characteristics were extracted: author, publication year, electronic databases searched, date ranges of the search, study design, number or size of studies, degree of overlap between studies reporting the same outcomes, diagnoses, effect estimates (raw or adjusted), confidence intervals or standard errors, p-values, measures of heterogeneity, publication bias and any critical appraisal. In line with the recommendations of Cochrane Rapid Reviews Methods Group, one reviewer (T.Z.) extracted narrative data from studies, which a second reviewer (S.K.) checked for correctness and completeness (Garritty et al., 2021). However, all quantitative data such as effect estimates, p-values and measures of heterogeneity were independently extracted by both reviewers and disagreements resolved by consensus or consultation with a third author (L.B.). Where possible, data were converted into standardised mean differences to facilitate comparisons across studies. For instance, log odds ratios were divided by 1.81 (Chinn, 2000). Alternatively, results were presented as mean differences for continuous data and the relative risk (R.R.) for any dichotomous outcome.
Outcomes
Our primary outcomes were hospital admissions, bed-days and community contacts in the 12 months following CTO placement. We focused on outcomes at 1 year as this is the most common end-point in the literature and the impact of an intervention on health service beyond 1 year is difficult to ascertain (Kisely et al., 2017).
However, we also assessed for these events up to 10 years from entry into the study. Secondary outcomes included the following as assessed by standardised psychiatric instruments, surveys or qualitative interviews: psychiatric symptoms, psychosocial functioning, quality of life, concordance with psychiatric treatment, criminal justice contacts and all-cause mortality.
Quality assessment and credibility of evidence
SR quality was assessed independently by the same two reviewers (S.K. and T.Z.) using the National Institutes of Health (NIH) Quality Assessment of Systematic Reviews and Meta-Analyses tool. This covers SRs of both quantitative and qualitative data. Conflict was again resolved through discussion with a third reviewer (L.B.). Scores were categorised as good (7–8), fair (4–6) or poor (0–3), in accordance with previous SRs (Firth et al., 2020). We also assessed whether studies used adjusted or raw data as CTOs cases may differ from voluntary controls when not randomly assigned. Finally, we assessed the level of quantitative evidence using criteria adapted from Fusar-Poli and Radua (2018):
Convincing (class I) when the number of cases > 1000, p < 0.00001, I2 < 50% and there are no small study effects in tests for publication bias;
Highly suggestive (class II) when the number of cases > 1000, p < 0.00001, the largest study in the meta-analysis has a statistically significant effect and class I criteria are not met;
Suggestive (class III) when the number of cases > 1000, p < 0.001 and class I–II criteria are not met;
Weak (class IV) when p < 0.05 and class I–III criteria are not met.
Analysis
The findings of the reviews were initially synthesised narratively. Numerical summaries of all relevant outcomes were extracted from each included SR and presented, noting whether these were adjusted or unadjusted effect estimates. Where possible, data were presented using the common effect sizes to allow comparisons across studies. If appropriate, data were combined in a meta-analysis across SRs. This meant only using study-specific data from the SRs, not meta-analysed totals, to avoid the same participants from different SRs being included multiple times in any analysis. Only data from RCTs or adjusted estimates from non-randomised studies could be used and results from the two designs are not combined. Where it was not possible to combine meta-analyses from different SRs, we vote-counted studies to determine the overall direction of findings for each outcome (Campbell et al., 2020).
Results
We found 1470 citations of interest. Of these 37 full-text papers were potentially relevant and assessed for eligibility and an additional 11 through forward and backward searches of their reference lists (Figure 1). As noted above, when there were articles with overlapping results, studies were excluded if 100% of the results were included in another study. We gave preference to newer over older reviews. The full-text screen eliminated 30 studies for reasons outlined in Figure 1, leaving 17 papers from 14 studies to be included in this umbrella review. Allowing for overlap between the studies, there were potentially up to 247,630 participants. Table 3 gives the full list of excluded SRs and the corresponding reasons, while online Supplement 2 contains the full citations.
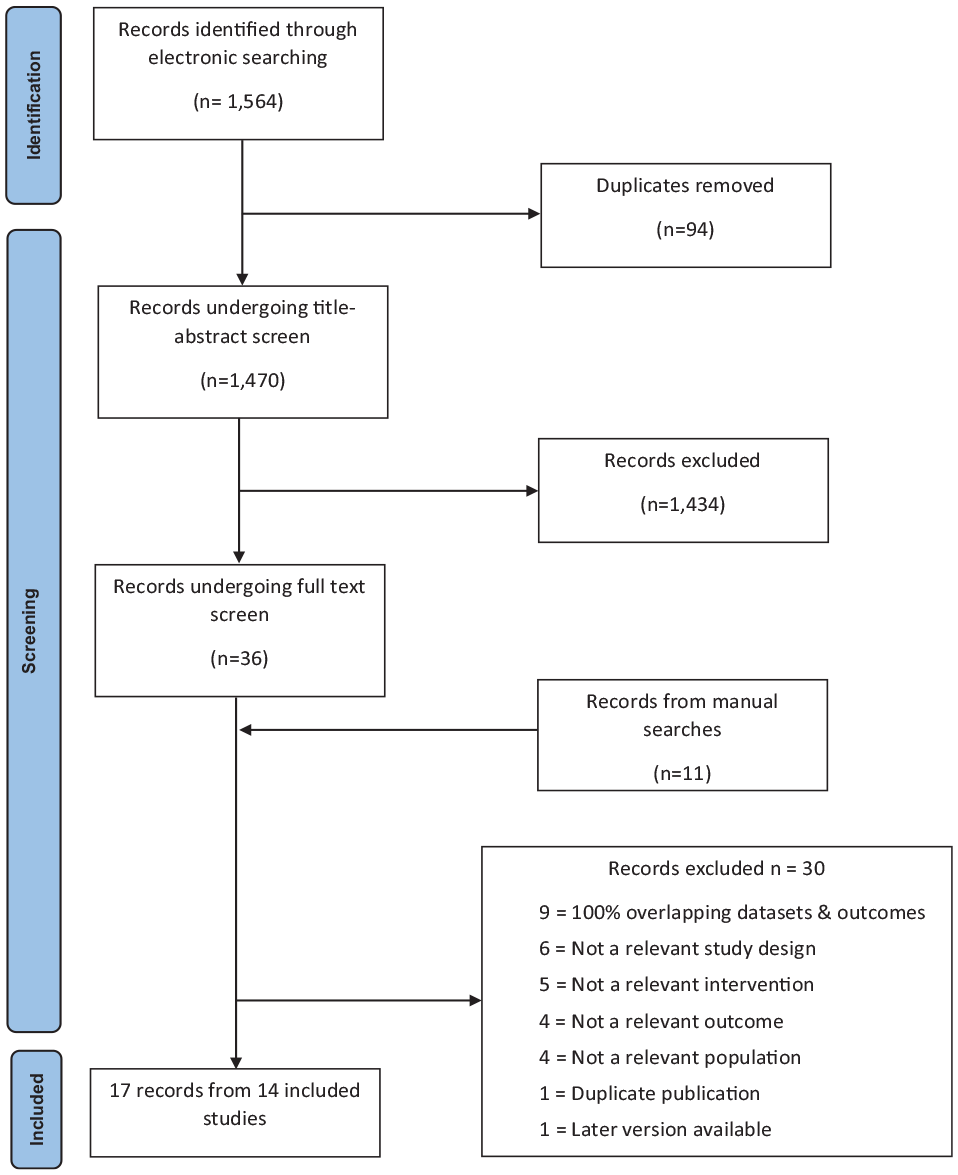
PRISMA diagram.
Quantitative systematic review results.
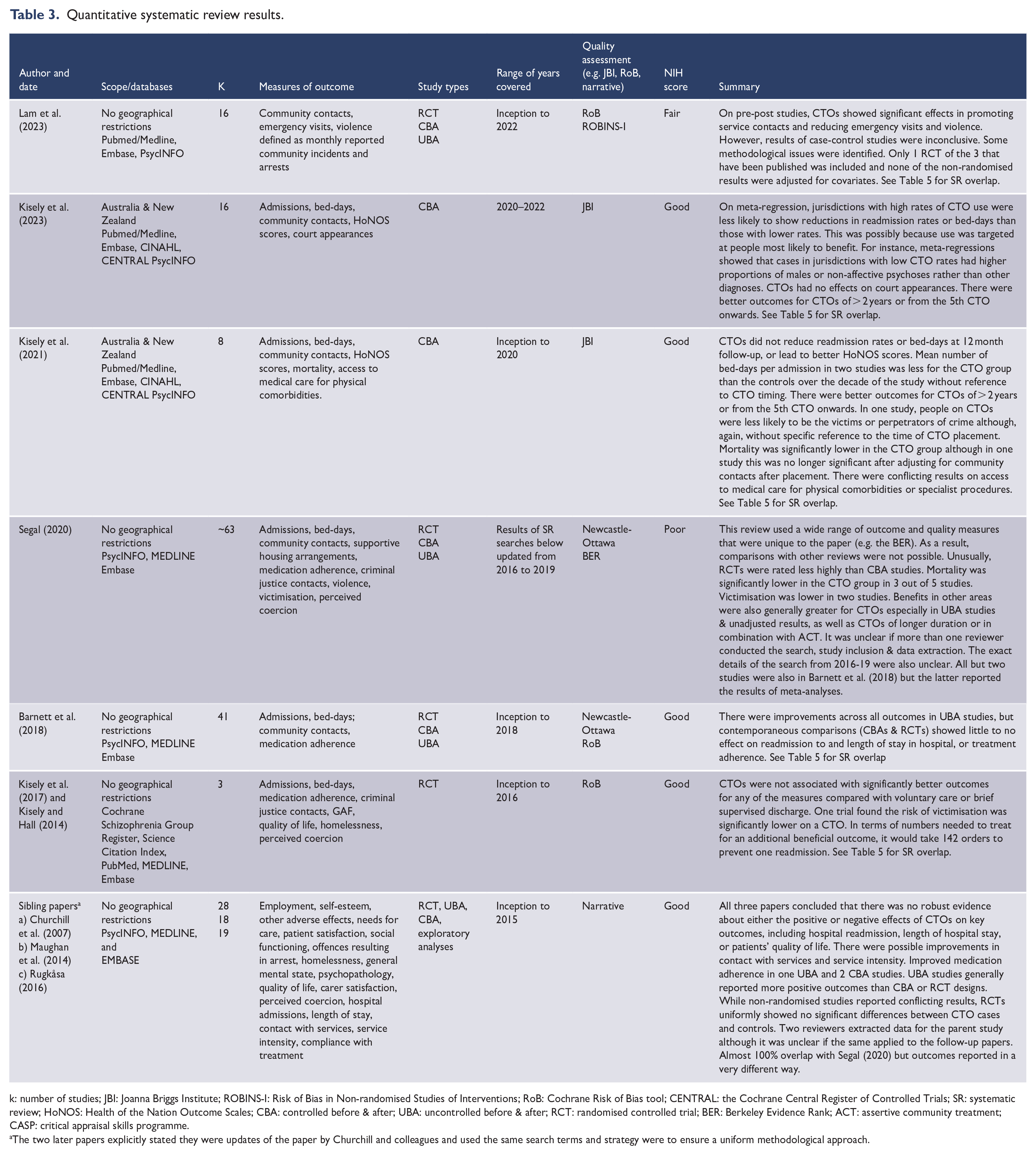
k: number of studies; JBI: Joanna Briggs Institute; ROBINS-I: Risk of Bias in Non-randomised Studies of Interventions; RoB: Cochrane Risk of Bias tool; CENTRAL: the Cochrane Central Register of Controlled Trials; SR: systematic review; HoNOS: Health of the Nation Outcome Scales; CBA: controlled before & after; UBA: uncontrolled before & after; RCT: randomised controlled trial; BER: Berkeley Evidence Rank; ACT: assertive community treatment; CASP: critical appraisal skills programme.
The two later papers explicitly stated they were updates of the paper by Churchill and colleagues and used the same search terms and strategy were to ensure a uniform methodological approach.
There were 10 papers from 7 SRs of quantitative designs (Barnett et al., 2018; Churchill et al., 2007; Kisely and Hall, 2014; Kisely et al., 2017, 2021, 2023; Lam et al., 2023; Maughan et al., 2014; Rugkåsa, 2016; Segal, 2020) (Table 3) and 5 of just qualitative studies (Corring et al., 2017, 2018, 2019; Goulet et al., 2020; Plahouras et al., 2020) (Table 4). Two SRs presented both types of data, although the majority of the studies were qualitative (de Waardt et al., 2022; Pridham et al., 2016) (Table 4). The quantitative studies included uncontrolled before & after (UBA) studies, quasi-experimental or controlled before & after (CBA) designs, and RCTs. Of the SRs of quantitative data, four were meta-analyses that all used random effects models (Table 5) (Barnett et al., 2018; Kisely et al., 2017, 2021, 2023). Two SRs were restricted to Australia and New Zealand, the remainder being worldwide (Table 3). However, of these, only one SR included data from a jurisdiction (Taiwan) that was outside North America, Europe, Australia or New Zealand (de Waardt et al., 2022).
Systematic review results from predominantly qualitative studies.
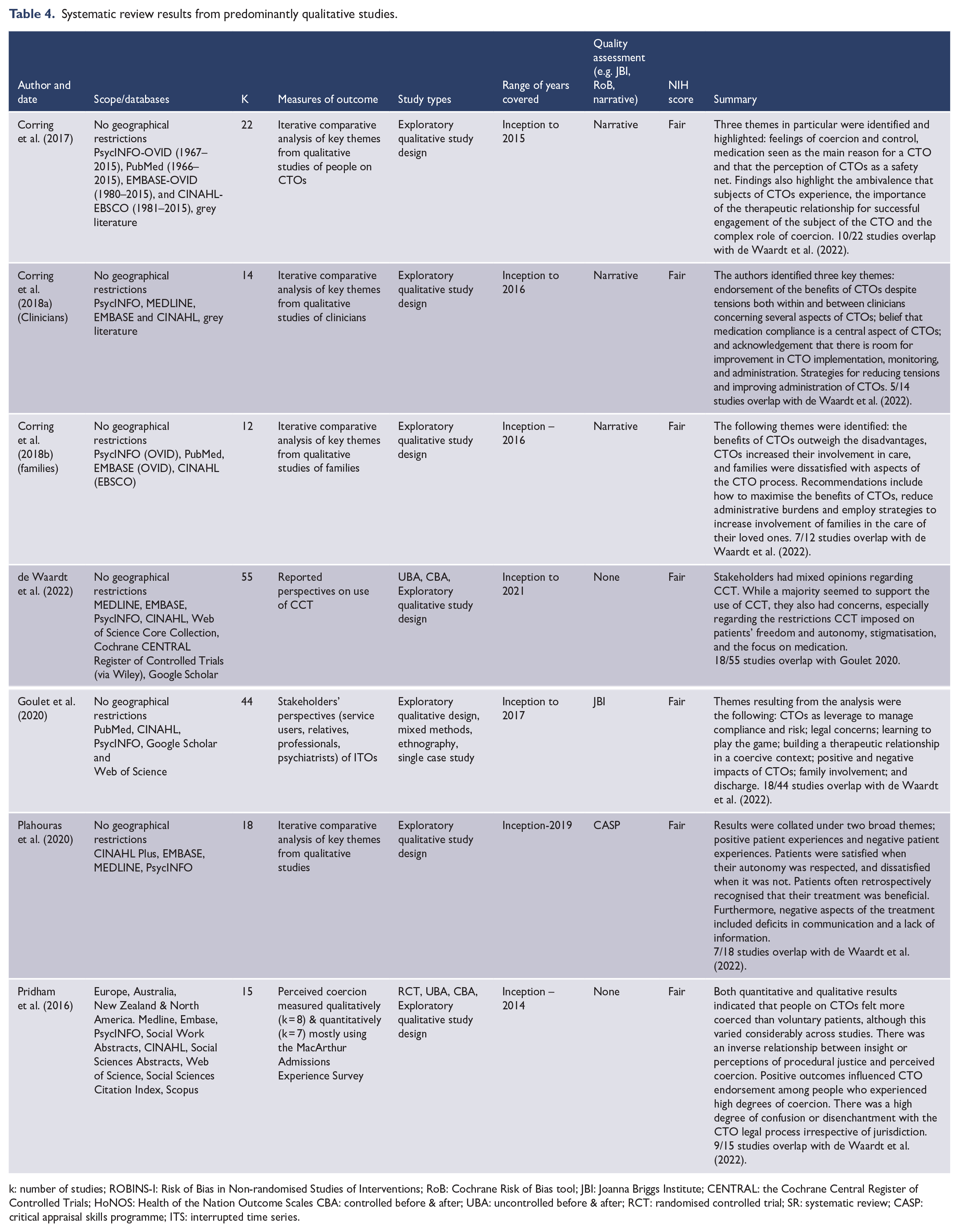
k: number of studies; ROBINS-I: Risk of Bias in Non-randomised Studies of Interventions; RoB: Cochrane Risk of Bias tool; JBI: Joanna Briggs Institute; CENTRAL: the Cochrane Central Register of Controlled Trials; HoNOS: Health of the Nation Outcome Scales CBA: controlled before & after; UBA: uncontrolled before & after; RCT: randomised controlled trial; SR: systematic review; CASP: critical appraisal skills programme; ITS: interrupted time series.
Meta-analyses results.
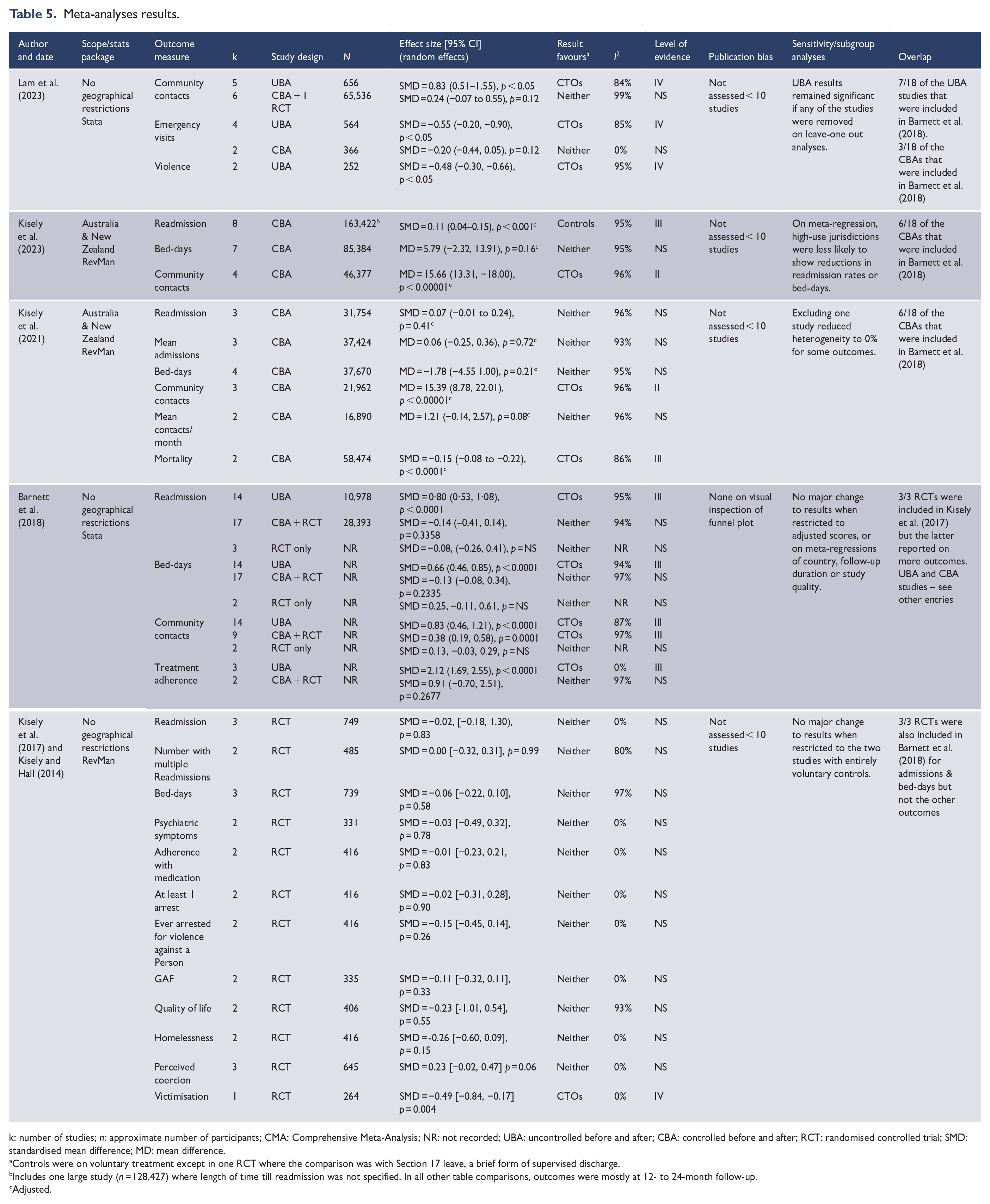
k: number of studies; n: approximate number of participants; CMA: Comprehensive Meta-Analysis; NR: not recorded; UBA: uncontrolled before and after; CBA: controlled before and after; RCT: randomised controlled trial; SMD: standardised mean difference; MD: mean difference.
Controls were on voluntary treatment except in one RCT where the comparison was with Section 17 leave, a brief form of supervised discharge.
Includes one large study (n = 128,427) where length of time till readmission was not specified. In all other table comparisons, outcomes were mostly at 12- to 24-month follow-up.
Adjusted.
Quantitative synthesis of data from different SRs was not appropriate either because of the absence of adjusted study-specific data in the non-randomised studies or because they came from the same three RCTs and therefore replicated meta-analyses that have been previously published (Table 5).
Effects of CTOs on health service, clinical and psychosocial outcomes
Inpatient outcomes
All nine SRs had data on inpatient outcomes from UBA studies, CBA designs or RCTs. The vast majority reported on outcomes at approximately 12 months of follow-up. However, one SR gave greater weight to a range of other measures (Segal, 2020). UBA studies generally reported significant decreases in hospital use in terms of the number of hospital readmissions and accumulated days in hospital for people on CTOs (Tables 3 and 5). However, there more equivocal results in data from CBA designs especially when adjusted. For instance, four out of five SRs reported no significant differences in the use of inpatient services between CTO cases and controls, while in the fifth there were more admissions in the CTO group. Finally, results from the three RCTs uniformly showed no significant differences between CTO cases and controls (Tables 3 and 5).
The Australian SRs also reported on the mean number of bed-days per admission over the 10 years of two Victorian studies without specific reference to when the CTO occurred (1990–2000 and 2000–2010, respectively) (Table 2) (Segal and Burgess, 2006a; Segal et al., 2017a). In both cases, this was less for the CTO group than the controls over the decade of the study (two studies; mean difference = −5.79 days; 95% CI = [−9.18 to −2.40], p = 0.0008, I2 = 42%). However, in a later study from Victoria that was published subsequently to the Australian SRs, this had fallen by 2 days to a saving of only 3.75 bed-days per admission between 2010 and 2017 (Segal et al., 2022).
The two Australian SRs (Kisely et al., 2021, 2023) also reported that there were better outcomes in terms of reduced inpatient health service use for CTOs of greater than 2 years’ duration or from the fifth CTO onwards (Burgess et al., 2006; Harris et al., 2019). By contrast, a third SR reported that people who were discharged to a treatment order immediately following their initial psychiatric admission had better outcomes than those placed on CTOs later in treatment (Segal, 2020). Amongst other findings, the same SR found that there were better outcomes for CTOs of greater than 6 months duration, or in the presence of assertive community treatment (Segal, 2020). One of the SRs from Australia and New Zealand also reported an inverse relationship using meta-regression between state-wide rates of CTO placement and subsequent inpatient use with the result that jurisdictions with low rates of CTO use were more likely to show reductions in readmission rates or bed-days than those with higher rates (Kisely et al., 2023). This was possibly because lower levels of use meant that CTOs were targeted at people who were more likely to benefit (Table 3).
Outpatient/community outcomes including medication adherence
CTOs significantly increased outpatient and community contacts in all the SRs using data from UBA and CBA designs (Tables 3 and 5). However, there were no significant differences in meta-analyses that were restricted to RCTs (Table 5). There was UBA and CBA evidence of improvements to medication adherence although this did not extend to RCTs (Tables 3 and 5).
Other outcomes
There were limited data on other outcomes. There was no CBA or RCT evidence that CTOs resulted in improved quality of life and better scores on either the Health of the Nation Outcome Scales (HoNOS) or Global Assessment of Functioning (GAF). There were conflicting findings in terms of offences or contacts with the criminal justice system (Tables 3), although there were no significant differences in the RCT results (Table 5). However, CTOs did reduce the risk of victimisation in one CBA and one RCT study. In the two RCTs where this was measured, there was no effect on homelessness (Table 5).
Two SRs (Kisely et al., 2021; Segal, 2020) reported that mortality rates were significantly lower in the CTO group compared with controls based on data from one Western Australian (WA) and two Victorian studies (Kisely et al., 2013; Segal and Burgess, 2006b; Segal et al., 2017b). However, there were non-significant findings in two other studies (one unpublished) in the second SR (Segal, 2020). In addition, the WA results were no longer significant following adjustment for community contacts after placement (Kisely et al., 2013). Furthermore, a later Victorian study published after both SRs found no difference in mortality rates between CTO cases and controls in people diagnosed with schizophrenia (Segal et al., 2023). Finally, there were conflicting results on whether CTOs improved access to medical care for physical comorbidities or specialist procedures (Tables 3 and 5).
Only two SRs had quantitative data on potential harms, a Cochrane review and one of predominately qualitative data that is describe more fully below (Kisely et al., 2017; Pridham et al., 2016). Both reported increased levels of perceived coercion in people on CTOs as measured by a standardised scale although this was non-significant in one case (Kisely et al., 2017).
Views of clinicians, people on CTOs, and families and supporters
Most information on the views of clinicians, people on CTOs and their supporters came from surveys or qualitative methods (Table 4). Respondents were generally asked about CTOs in isolation from less coercive alternatives such as advanced directives, for which there is greater evidence of effectiveness (de Jong et al., 2016). Three papers by the same authors reported on the experiences of people on CTOs, clinicians and family, respectively (Corring et al., 2017, 2018, 2019), while two other studies reported on all three groups in the same paper (de Waardt et al., 2022; Goulet et al., 2020). Two studies reported only on the experiences of people on CTOs (Plahouras et al., 2020; Pridham et al., 2016). People on CTOs reported mixed feelings about being on compulsory community treatment in all the studies (Table 3). Benefits included feeling that there was a safety net to prevent them from relapsing or requiring a long-term hospital admission. However, these benefits came at a cost. Most commonly, this was a lack of self-determination and control over treatment for people made subject to CTOs (Corring et al., 2017; de Waardt et al., 2022; Plahouras et al., 2020). Importantly, coercion was a key barrier to building a therapeutic relationship with professionals while the person was on a CTO (Goulet et al., 2020).
In all the SRs, the perceived lack of control prevented people on CTOs from developing positive relationships with clinicians given the power imbalance. One SR highlighted confusion and disenchantment with the CTO legal process irrespective of jurisdiction (Pridham et al., 2016). However, a positive relationship with clinicians could emerge if people on CTOs were able to accept the conditions (Corring et al., 2017).
Clinicians described positive views about CTOs because it allowed for greater control and capacity to intervene to support recovery (Corring et al., 2018; de Waardt et al., 2022). Clinicians also wanted people living with mental illness to get better and saw CTOs as a way to achieve this, identifying the negative aspects of CTOs being a small cost compared with keeping the person well.
Similarly, family members and supporters generally described CTOs as facilitating access to care and felt that they were more frequently recognised by clinicians as having an important role when a person was on a CTO (de Waardt et al., 2022; Corring et al., 2019). Families consequently viewed CTOs as a way to have their thoughts, feelings and perspectives considered (Corring et al., 2019; Plahouras et al., 2020).
All seven SRs of qualitative data discussed the role of medication. Increased medication adherence was reported as a positive outcome of CTOs although this was more likely to be valued by clinicians rather than people on CTOs (Corring et al., 2017; Goulet et al., 2020; Plahouras et al., 2020).
SRs reported on data from standardised instruments less often and these were largely restricted to comparing perceived coercion in people on CTOs with those on voluntary treatment (Kisely et al., 2017; Pridham et al., 2016). In general, CTO cases had higher scores on measures of coercion (Pridham et al., 2016), although this only just failed to reach statistical significance in one meta-analysis of two studies (p = 0.06) (Kisely et al., 2017). There was an inverse relationship between insight, perceptions of procedural justice and perceived coercion (Pridham et al., 2016).
The NIH scores were good for five out of the seven quantitative SRs, with the remaining two rated as either fair or poor, largely because of concerns about the search strategy and/or that only one person conducted the review (Table 3). Other common issues were the absence of any assessment for publication bias or heterogeneity. Table 3 outlines additional limitations in the one SR that was rated poor including areas not covered by the NIH tool (Segal, 2020). The qualitative studies were all rated as fair, but this was largely because meta-analyses are not possible with this methodology (Table 4). The level of evidence for statistically significant results was strongest for community contacts, where it was rated as highly suggestive. For other outcomes (e.g. mortality), it was only weak to suggestive, or non-significant (Table 5).
Discussion
To our knowledge, this is the first umbrella review of both quantitative and qualitative data that specifically examined the benefits and harms of compulsory community treatment in a wide range of countries including the United States, Canada, Taiwan, Great Britain, Norway, Spain, Netherlands, Ireland, Australia and New Zealand. Table 6 summarises the quantitative results. This shows that the evidence for the benefits of CTOs on subsequent health service use was mixed and showed a clear decline with increasing strength of study design. Whereas UBA evidence suggested that CTOs increased follow-up with mental health services and reduced inpatient admissions, more rigorous CBA studies using matching or multivariate analysis reported mixed benefits, and RCTs no effect on inpatient service use. There were similar patterns for clinical, psychosocial and forensic outcomes. The only consistent benefit was an increase in community contacts. However, it could be argued that the latter is a process measure rather than a final result, since the hypothesised method of achieving the outcome is by requiring people to attend community or outpatient services.
Summary of quantitative results.
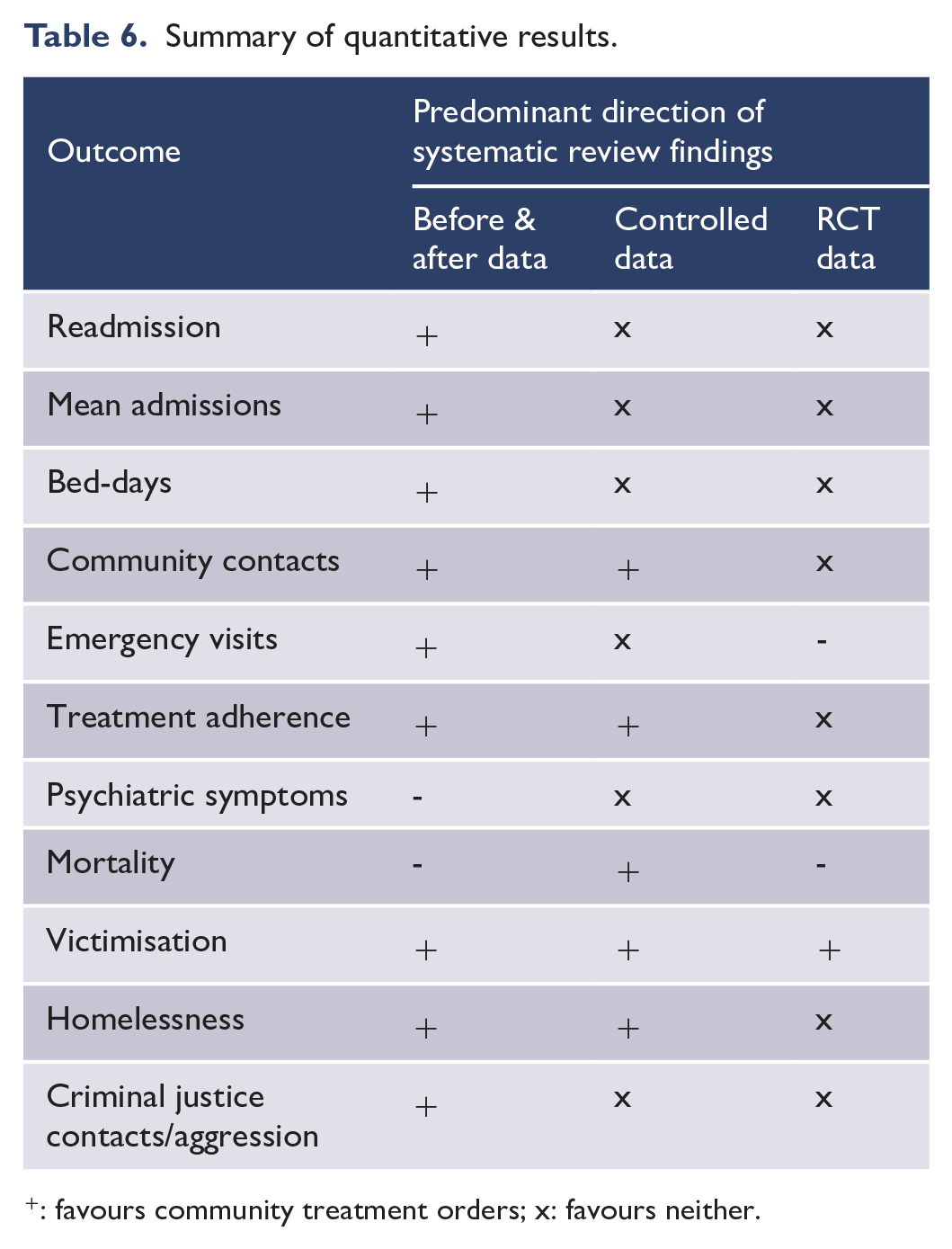
: favours community treatment orders; x: favours neither.
In terms of factors associated with better outcomes, there was a suggestion that a more focused use of CTOs in some jurisdictions was more likely to lead to reductions in readmission rates or bed-days. It may be that in these jurisdictions, CTOs are better targeted towards the people most likely to benefit, such as those with psychosis. These results are consistent with a recent New Zealand-wide epidemiological study where reductions in health service use following CTOs were limited to people with schizophrenia (Beaglehole et al., 2021). There were better outcomes for longer-term CTOs, or from the fifth CTO onwards, although the meaning of this is unclear (Kisely et al., 2020, 2023; Segal, 2020). For instance, a CTO of over 6 months may imply fewer admissions based solely on time at risk in the community, because a CTO of over 6 months means that any psychiatric admission within a 12-month period must occur in the remaining half of the year, while controls have an entire year during which they can be admitted (Segal, 2001). It may also reflect a bias where it was selectively extended when it seemed to be of benefit (Segal, 2001; Szmukler and Hotopf, 2001). CTOs that extend over years and/or multiple treatment orders also raise the question of whether compulsory treatment over such a prolonged period is really less coercive than shorter periods of involuntary hospitalisation. Finally, greater benefit from prolonged CTO placement seems inconsistent with other work where people who were discharged to a treatment order immediately following their initial psychiatric admission had better outcomes than later placement (Segal, 2020).
A series of consecutive studies from Victoria (Australia) suggested there was a reduction in the mean length of bed-days per episode over the decade of each study, but this was without reference to the actual timing of the CTO (Segal and Burgess, 2006a; Segal et al., 2017a). Importantly, any effect had almost halved to 2.75 days in the most recent work possibly reflecting long-term reductions in length of stay in general (Segal et al., 2022). Any benefits may also require the presence of assertive community treatment, which is not always available.
Although the finding was only suggestive, a final reported benefit was a reduction in mortality in three out of five studies identified by SRs. This is in line with findings from an epidemiological study from Great Britain (Barkhuizen et al., 2020). These reductions may be due to closer follow-up in the community as the benefits at 1- and 2-year follow-up disappeared after adjustment for community contacts meaning there could be less coercive alternatives of ensuring the same level of community support (Kisely et al., 2013). Importantly, there were no significant differences in mortality rates in the most recent study that was confined to people with a diagnosis of schizophrenia (Segal et al., 2023).
There was limited quantitative research on harms. Only two SRs measured perceived coercion on a standardised scale where people on CTOs reported increased scores (Kisely et al., 2017; Pridham et al., 2016), although this was non-significant in one case (Kisely et al., 2017).
The mixed findings were echoed by those from the qualitative SRs of the views of people on CTOs, their families, supporters and clinicians where there was more evidence of possible harms (Table 4). While a majority supported the use of CTOs, they also had concerns, especially regarding stigmatisation, the focus on medication and restrictions on freedom and autonomy. Family members and clinicians were generally positive about the effect of CTOs particularly on ensuring community follow-up, but those subject to them were more ambivalent – perhaps because they shouldered more of the negative impacts of CTOs.
Limitations
Most of the SRs were of observational studies, often using administrative health data. These may be subject to recording bias and lack information on social functioning. Cases and controls may also have differed in ways for which it was not possible to adjust. There were limited data on the possible harms of CTOs, particularly using quantitative methods. Even where there was qualitative research on possible harms, respondents were not presented with less coercive and more effective alternatives such as advance directives.
Although the SRs were rated as mid to high quality by NIH criteria, many of the constituent meta-analyses results had high heterogeneity, and low numbers of contributing studies limited the assessment of publication bias. All of these factors contributed to weak or suggestive levels of evidence for the limited number of comparisons where there were significant differences apart from community contacts. In addition, study heterogeneity prevented the meta-analysis of results from different SRs and there were also overlapping findings of the same outcomes. We therefore did not synthesise results across the studies beyond describing the overall direction of findings. Finally, several of the included SRs were authored by one this umbrella review’s authors (S.K.). However, study selection and quality appraisal were always undertaken independently by two authors (T.Z. and S.K.) with a third reviewer available in the case of any disagreements (L.B.).
Implications for future research
Findings of improved outcomes with better targeting of CTOs suggest the need for further research into the reasons behind the marked differences in their use even within the same country, as is the case in Australia. This includes mixed methods, legal and policy research to better understand the driving factors underpinning this variance and the subsequent effects on outcomes. Given the difficulty of undertaking RCTs in this area, alternative approaches to assessing outcomes could be quasi-experimental designs such as CBA studies and interrupted time series of administrative health data. More research is also needed to establish the relative merits of the different interventions available, such as advance directives, assertive community treatment or the various forms of compulsory community treatment, rather than comparisons of individual approaches against treatment as usual. There should also be more research into the effect on outcomes that are more relevant to people on CTOs and their families including symptomatology, social functioning and satisfaction, rather than reliance on measures of health service use alone. This should also include further exploration of the potential harms, as well as benefits.
Conclusion
This umbrella review highlights continued uncertainty over the benefits of CTOs, as well as the relative lack of research (especially quantitative) on associated harms. Evidence for effectiveness is largely restricted to orders of at least 2 years’ duration or the fifth CTO, raising the question as to whether long periods under CTOs are less restrictive than short inpatient admissions. Differences in outcomes between high- and low-use jurisdictions suggest that, at the very least, CTOs should be better targeted to people most likely to benefit.
Supplemental Material
sj-docx-1-anp-10.1177_00048674241246436 – Supplemental material for The benefits and harms of community treatment orders for people diagnosed with psychiatric illnesses: A rapid umbrella review of systematic reviews and meta-analyses
Supplemental material, sj-docx-1-anp-10.1177_00048674241246436 for The benefits and harms of community treatment orders for people diagnosed with psychiatric illnesses: A rapid umbrella review of systematic reviews and meta-analyses by Steve Kisely, Tessa Zirnsak, Amy Corderoy, Christopher James Ryan and Lisa Brophy in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: S.K. authored several of the systematic reviews that were included in this umbrella review. However, to reduce risk of bias, study selection and quality appraisal were always undertaken independently by two authors (T.Z. and S.K.), with a third reviewer available in the case of any disagreements (L.B.). There are no other conflicting interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funding for this project came from the Victorian Government’s Independent Review Panel of Compulsory Treatment Criteria & Alignment with Decision-making Laws in Mental Health Legislation and an Australian Research Council Discovery Project (DP230100967).
Availability of Data and Materials
Data supporting the findings are available from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.