
Abstract
Background:
There is conflicting and equivocal evidence for the efficacy of compulsory community treatment within Australia and overseas, but no study from Queensland. In addition, although people from Indigenous or culturally and linguistically diverse backgrounds are over-represented in compulsory admissions to hospital, little is known about whether this also applies to compulsory community treatment.
Aims:
We initially investigated whether people from Indigenous or culturally and linguistically diverse backgrounds in terms of country of birth, or preferred language, were more likely to be on compulsory community treatment using statewide databases from Queensland. We then assessed the impact of compulsory community treatment on health service use over the following 12 months. Compulsory community treatment included both community treatment orders and forensic orders.
Methods:
Cases and controls from administrative health data were matched on age, sex, diagnosis and time of hospital discharge (the index date). Multivariate analyses were used to examine potential predictors of compulsory community treatment, as well as impact on bed-days, time to readmission or contacts with public mental health services in the subsequent year.
Results:
We identified 7432 cases and controls from January 2013 to February 2017 (total n = 14,864). Compulsory community treatment was more likely in Indigenous Queenslanders (adjusted odds ratio = 1.45; 95% confidence interval = [1.28, 1.65]) subjects coming from a culturally and linguistically diverse background (adjusted odds ratio = 1.54; 95% confidence interval = [1.37, 1.72]), or those who had a preferred language other than English (adjusted odds ratio = 1.66; 95% confidence interval = [1.30, 2.11]). While community contacts were significantly greater in patients on compulsory community treatment, there was no difference in bed-days while time to readmission was shorter. Restricting the analyses to just community treatment orders did not alter these results.
Conclusion:
In common with other coercive treatments, Indigenous Australians and people from culturally and linguistically diverse backgrounds are more likely to be placed on compulsory community treatment. The evidence for effectiveness remains inconclusive.
Keywords
Introduction
There has been a worldwide increase in the rates of compulsory intervention in mental health (Burns and Dawson, 2009; DeRidder et al., 2016). In Australia, community treatment orders (CTOs) require psychiatric patients to comply with conditions (e.g. compliance with their medication and/or attendance with outpatient services), which in turn allow them to live in the community. However, their use is controversial. A Cochrane review of international randomised controlled trials (RCTs) showed no evidence that CTOs reduced health service use and improved social functioning, mental state or quality of life (Kisely et al., 2017b).
By world standards, CTO use in Australia is high and rising, with considerable variations across states depending on the measure (Clugston et al., 2018; Light, 2019; Light et al., 2012a). For example, there are marked inter-jurisdictional differences in the percentage of community mental health contacts in the public sector that are involuntary. In 2016-17, these ranged from 3.1% in Western Australia to 16.2% in Victoria, and 22.3% among psychiatric patients in Queensland (Australian Institute of Health and Welfare, 2018). These high rates are potentially at odds with Australia’s ratification of the United Nations Convention on the Rights of Persons with Disabilities (CRPD), including those with ‘mental impairments’ (McSherry and Waddington, 2017; Newton-Howes and Ryan, 2017). In response, several Australian jurisdictions have changed their mental health legislation with a greater emphasis on human rights and patients’ capacity to consent to treatment. However, all have retained CTOs.
In addition to the possible effect on human rights, there is uncertainty concerning their effect on subsequent health service use. There have been only three RCTs of CTOs, two in the United States and one in the United Kingdom. None demonstrated significant benefit of CTOs in terms of hospital readmission rates, social functioning, quality of life, mental state or offending (Burns et al., 2013; Steadman et al., 2001; Swartz et al., 1999). However, randomised trials of CTOs face particular ethical and practical challenges (including relatively brief duration of follow-up), and these limit their utility. In critically appraising the two US trials, a Cochrane systematic review highlighted small sample sizes, the court-imposed nature of compulsory community treatment (CCT) and the exclusion of patients with a history of violence (Kisely et al., 2017b). In particular, court-ordered treatments in the United States have limited generalisability to clinician-ordered CTOs in Australia. The OCTET trial in England was more applicable to Australia but had limitations including the involuntary nature of the control condition, high rates of non-participation and cross-over between trial arms after randomisation (Burns et al., 2013).
Further RCTs of CTOs are unlikely, given ethical challenges inherent in randomising those who may lack insight, and who may be dangerous to themselves or others, to legal restriction versus truly voluntary care (Weich et al., 2018). As a result, there has been renewed interest in population-based observational studies such as before-and-after or matched cohort designs, several of which were undertaken in Western Australia, Victoria and New South Wales (Kisely et al., 2004, 2005, 2013, 2014; Preston et al., 2002; Segal and Burgess, 2006; Segal et al., 2017; Vaughan et al., 2000; Harris et al., 2019). These studies give conflicting or equivocal evidence for their efficacy, depending on the exact methodology. For instance, some authors report decreased admission rates and reduced bed use among those subject to CCT, while others do not.
Of further concern is the possible overuse of CCT in ethnic minorities. One of the few available studies showed that people who needed an interpreter had three times the risk of CTO placement on adjusted analyses (Moss et al., 2018). However, this was restricted to one Queensland health district that has one of the most culturally and linguistically diverse (CALD) populations in the state, with around 32% of the total population born overseas. The results may therefore not be generalisable to elsewhere. There is also limited information on CTO use in Indigenous Australians despite findings that this group are over-represented in terms of compulsory admission to hospital. Only one person was Indigenous out of 164 Victorians on CTOs (Brophy et al., 2006), while they were no more likely to be on an order than the general population in a population-based study from Western Australia (Kisely and Xiao, 2017).
Because of this uncertainty, we used anonymised administrative data to assess the effect of CTOs in Queensland, a jurisdiction where this has never been studied. The primary outcome of interest was subsequent inpatient bed-days, with secondary outcomes of community or outpatient contacts. The vast majority of studies report that CTOs increase community contacts and, in addition, this is a process rather than an outcome measure. If a CTO mandates outpatient attendance, it is unsurprising that contact increases. We also included forensic orders (FOs), an under-investigated form of court-ordered CCT. Finally, we investigated if patients from CALD backgrounds were more likely to be treated with CTOs and FOs than individuals from non-CALD backgrounds.
The Mental Health Act (2000) (QLD) was in force for the period of the study. This was implemented on 28 February 2002. As in other parts of Australia and New Zealand, it provided for involuntary treatment in the community through the introduction of CCT of two broad types: FOs issued by courts and CTOs (termed community involuntary treatment orders or ITOs) made by qualified mental health specialists. A psychiatrist has to confirm the order if the initial authorised doctor was not one, him or herself. Patients subject to an ITO must also be regularly reviewed by an independent mental health tribunal. An initial review must occur within 6 weeks of the order and thereafter at intervals of no longer than 6 months. Patients can also apply for review at any time.
Methods
We used linked administrative data from Queensland that cover all private and public hospital separations (patient discharges, transfers to another facility or deaths) and contacts with state mental health services (including public outpatient clinics) for the entire state. The Queensland Hospitals Admitted Patients Data Collection (QHAPDC) provided information on inpatient services while the Consumer Integrated Mental Health Application (CIMHA) gave details of the legal status of patients discharged into the community, as well as subsequent contacts with services. We followed guidelines for the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) (Vandenbroucke et al., 2007). These recommend giving characteristics of study participants including their demographic, clinical and social characteristics as well as information on other relevant variables. They also suggest reporting both unadjusted and covariate-adjusted estimates, along with their 95% confidence intervals, making clear which covariates were adjusted for and why they were included.
We identified all psychiatric inpatients who were discharged to CCT between 1 January 2013 and 28 February 2017. Only the first discharge within that time was included. For each case, we identified a control who was discharged into the community on a voluntary basis, matched on age group (5-year age group), sex, principal diagnosis and proximity to index discharge (±6 months). All subjects were followed up for 12 months.
Ethnic minority status was defined in line with the recommendations of the Australian Bureau of Statistics (1999) for cultural and linguistic diversity. The four core variables are Indigenous status, country of birth, main language other than English spoken at home and proficiency in spoken English. As the latter two were not recorded in our administrative data, we used preferred use of a language other than English as a proxy for both.
We initially used bivariate analyses to compare the effect of Indigenous status or country of birth on CCT placement. We compared people born in the following predominantly English-speaking locations (Australia, New Zealand, the United Kingdom, Ireland and North America) with those from elsewhere. This is because our previous study, restricted to just one of the 16 health districts in Queensland, suggested that people born in these locations had very similar rates of CCT placement. Next, we calculated adjusted odds ratios for the contribution of each variable to CCT placement while controlling for other possible factors by means of logistic regression. Variables were forced into the model based on being associated with the independent or other dependent variables, theoretically, or on univariate analysis. These included other relevant demographic factors such as marital status, education, metropolitan versus rural residence and socio-economic status as determined by statistical area of domicile, as well as primary diagnosis. We considered health service use as well including inpatient stays and outpatient contacts 1 year prior to the index date. Preferred use of a language other than English was also used as an indicator of CALD status in separate models.
We then compared changes in health service use between CCT cases and controls before and after the index dates. The primary outcome was a change in bed-days within 12 months of discharge as this is the most common follow-up period in studies that have reported both significant and non-significant results. This allowed comparison with previous work from elsewhere. The patient’s average length of stay before the CTO was subtracted from the patient’s average stay after the CTO to yield a change in episode duration.
We used bed-days rather than admissions as our primary outcome given the meaning of the latter can be unclear. For instance, does CCT reduce admission rates, thereby allowing individuals to remain in their communities during treatment, or are rates increased as a result of earlier identification of relapse (Kisely, 2009; Kisely and Campbell, 2007)?
We also compared mean changes in community and outpatients contacts between cases and controls over the same period. We adjusted for the same factors as in our analysis of CCT placement. We focused on outcomes at 1 year, as one has to be very cautious of ascribing an effect on health service use beyond a year after initial placement (Kisely et al., 2011).
Finally, we measured time to readmission within the same time frame (12 months post index date) using Kaplan–Meier survival curves and Cox regression to calculate adjusted hazard ratios. Skewed data were either divided about the median for categorical data or logarithmically transformed for continuous data. In the case of the latter, we added 0.1 to each value because of zeros.
We undertook sensitivity analyses of the effect of excluding cases on FOs (and their controls). We also adjusted survival using a propensity score derived from all possible confounders.
The study was approved by Metro South Ethics and Governance (HREC/17/QPAH/505-SSA/17/QPAH/506). Individual patient consent was not required as this was a study of anonymised administrative health data.
Results
The sample consisted of 7432 patients and the same number of controls (total n = 14,864). Of the cases, 7228 were on CTOs and 204 on FOs. Fifty-eight percent were male (n = 8624) with a median age of 35 years. Over half had schizophrenia or other non-affective psychoses (n = 7550), followed by 26% with affective disorders (n = 3980), and then a smaller number of organic, drug-induced, stress-related or personality disorders. Matching was successful, both groups sharing identical features for age or sex, and similar characteristics for diagnosis (Table 1).
Demographic and health service factors associated with CTO placement.
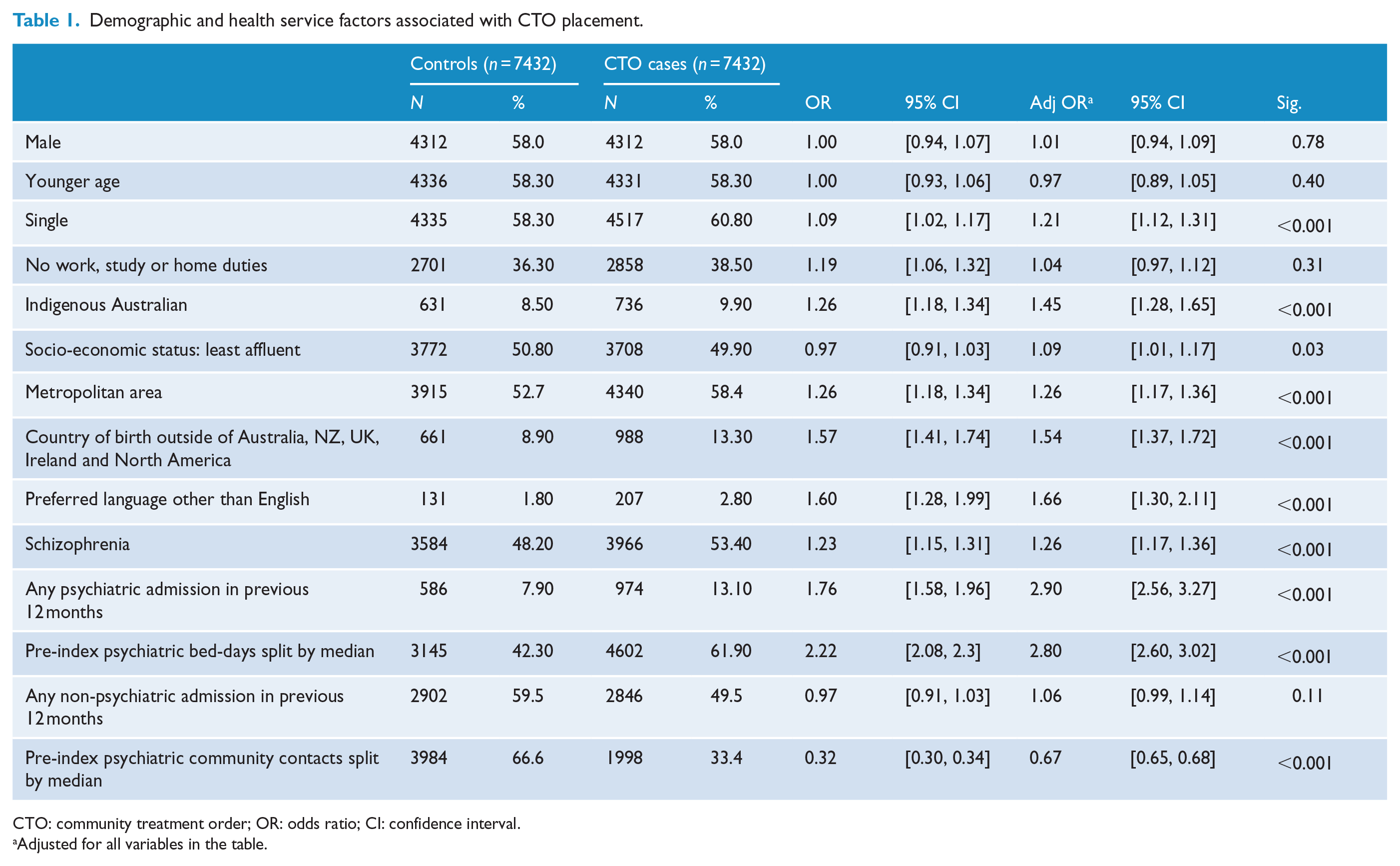
CTO: community treatment order; OR: odds ratio; CI: confidence interval.
Adjusted for all variables in the table.
New Zealand and the United Kingdom were the most common countries of birth after Australia (Figure 1). After that, the two most common places of birth were in maritime South East Asia (Indochina) and Southern or Eastern Africa. The most common languages other than English were Vietnamese, Farsi, Mandarin, Cantonese and Italian (Figure 2).
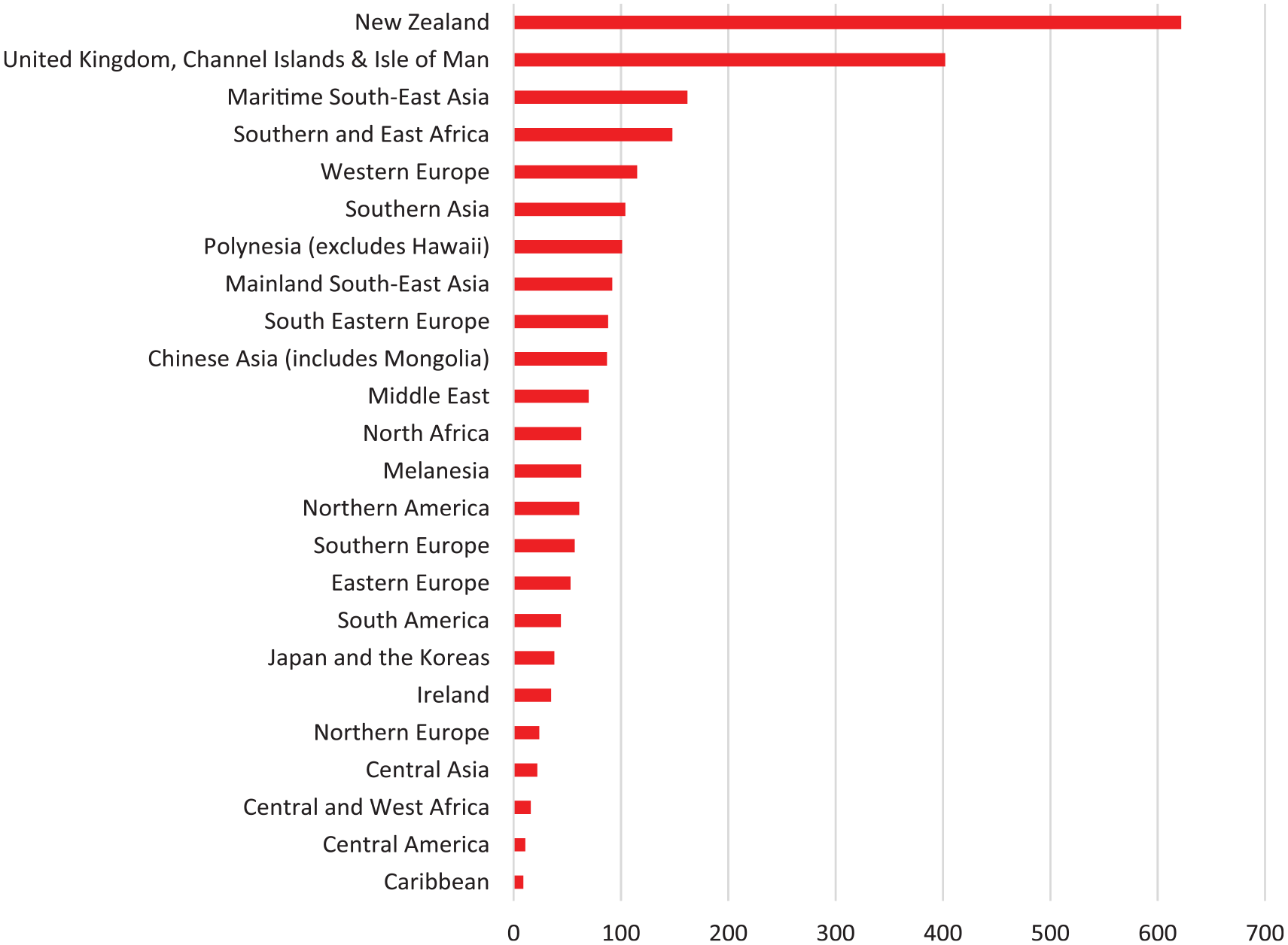
Countries of origin outside Australia.
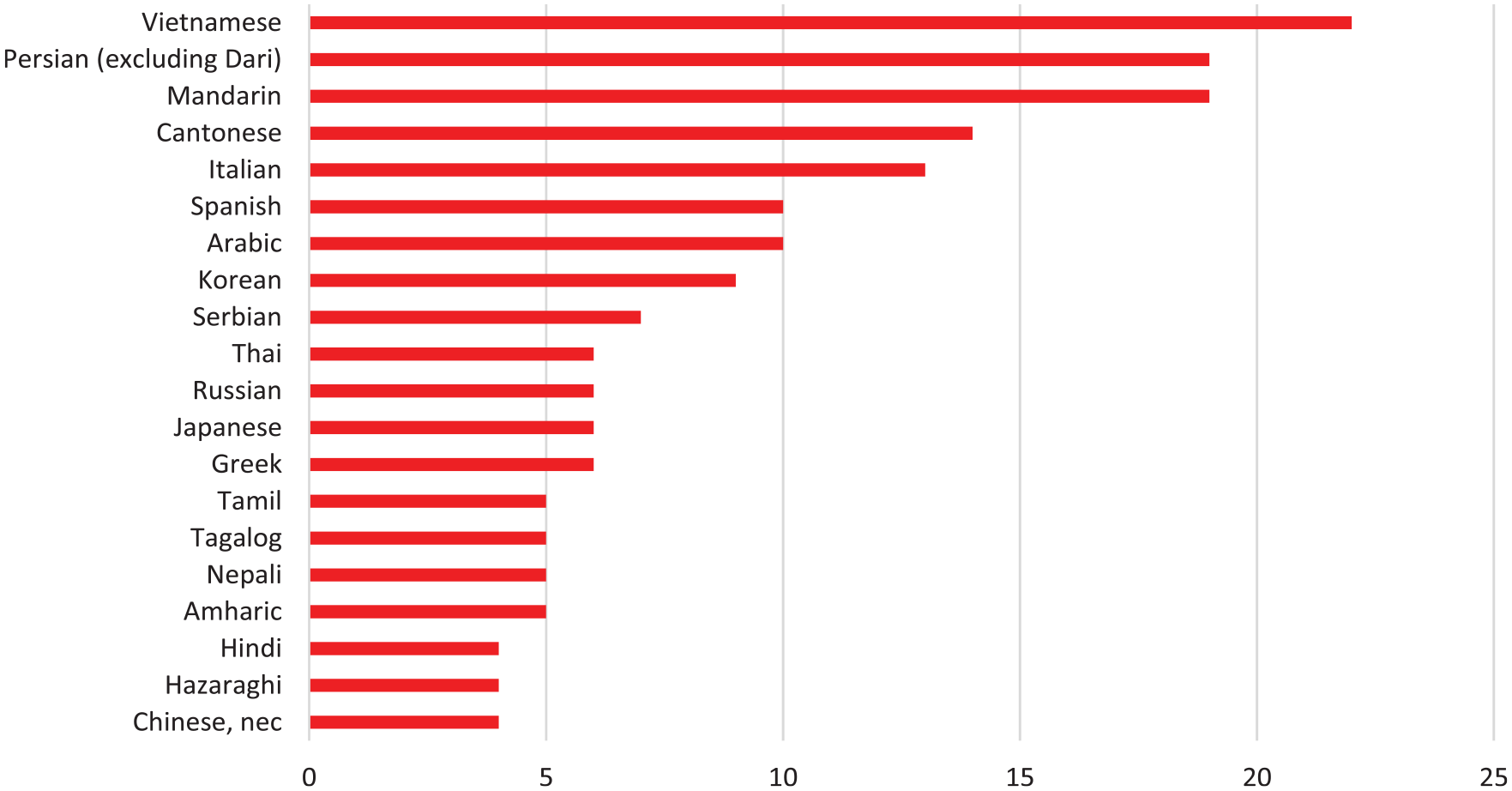
Preferred languages spoken other than English.
Table 1 compares the baseline characteristics of the CCT cases and controls. In bivariate comparisons, CCT cases were more likely to be single or live in a metropolitan area and less likely to be engaged in work, study or home duties. Indigenous Australians and people who were born in countries outside of Australia, New Zealand, the United Kingdom, Ireland and North America were at greater risk of CCT placement, as were those whose preferred language was other than English. A diagnosis of schizophrenia also showed a significant association. In terms of health service use, CCT cases had a greater number of both psychiatric admissions and bed-days. Both groups had a similar number of non-psychiatric admissions. However, CCT cases were less likely to have had outpatient contacts prior to CCT placement (Table 1).
We found similar results in the adjusted analyses. In particular, Indigenous Australians and those from a CALD background, as determined by county of birth or preferred language, were at greater risk of an involuntary order. CCT cases were also more likely to live in a socially deprived area.
Factors associated with changes in length of stay following CCT placement
CCT cases had eight fewer days in hospital in the year following the index date compared to the previous 12 months. Controls had seven fewer days. There were no significant differences between the two groups on analysis of the log-transformed data (Table 2). On unadjusted analyses, increased bed-days were associated with younger age, being single, unemployment, metropolitan residence, a diagnosis of schizophrenia and markers of health service use prior to the index date. By contrast, lower socio-economic status, or cultural and linguistic diversity, was associated with decreases in length of stay (Table 2).
Factors associated with change in log-transformed bed-days at 1-year follow-up.
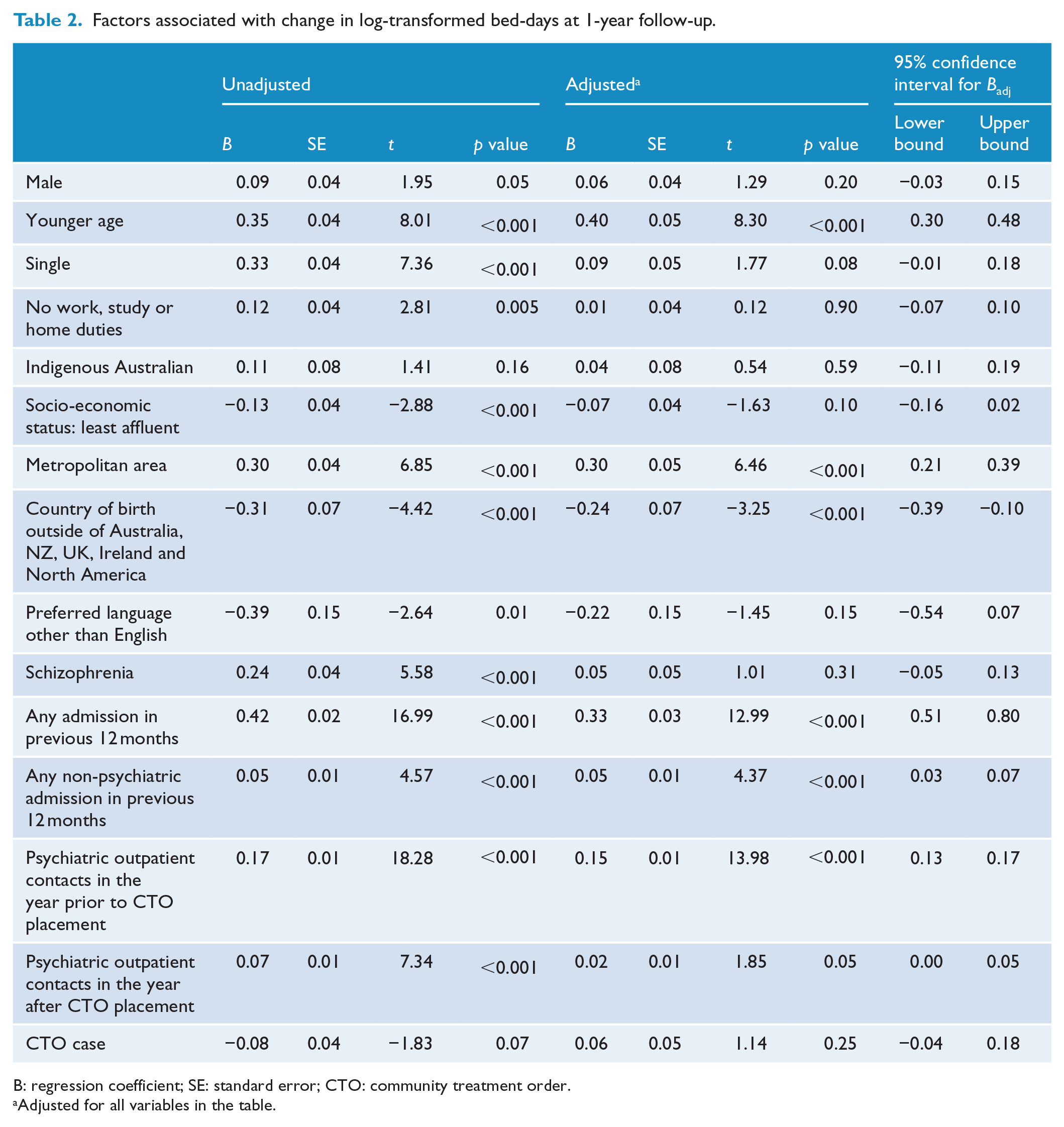
B: regression coefficient; SE: standard error; CTO: community treatment order.
Adjusted for all variables in the table.
After adjusting for all variables in the table, younger age, metropolitan residence and prior health service use, CCT was still associated with increases in length of stay. By contrast, country of birth other than Australia, New Zealand, the United Kingdom, Ireland or North America predicted reduced bed-days. There was no association between CCT placement and outcome.
Factors associated with changes in community contact following CCT placement
Unadjusted results are shown in Table 3. CCT cases had an average of 20 additional contacts compared to controls, this result being statistically significant on analysis of the log-transformed data. Table 3 also shows the results adjusted for all variables in the table. Lower socio-economic or Indigenous status was associated with fewer community contacts, while a diagnosis of schizophrenia and CCT placement were both associated with increased visits. Health service use as an inpatient prior to the index date had an inverse relationship with subsequent community contacts. There was no association between cultural or linguistic diversity and community contacts.
Factors associated with change in log-transformed psychiatric outpatient contacts at 1-year follow-up.
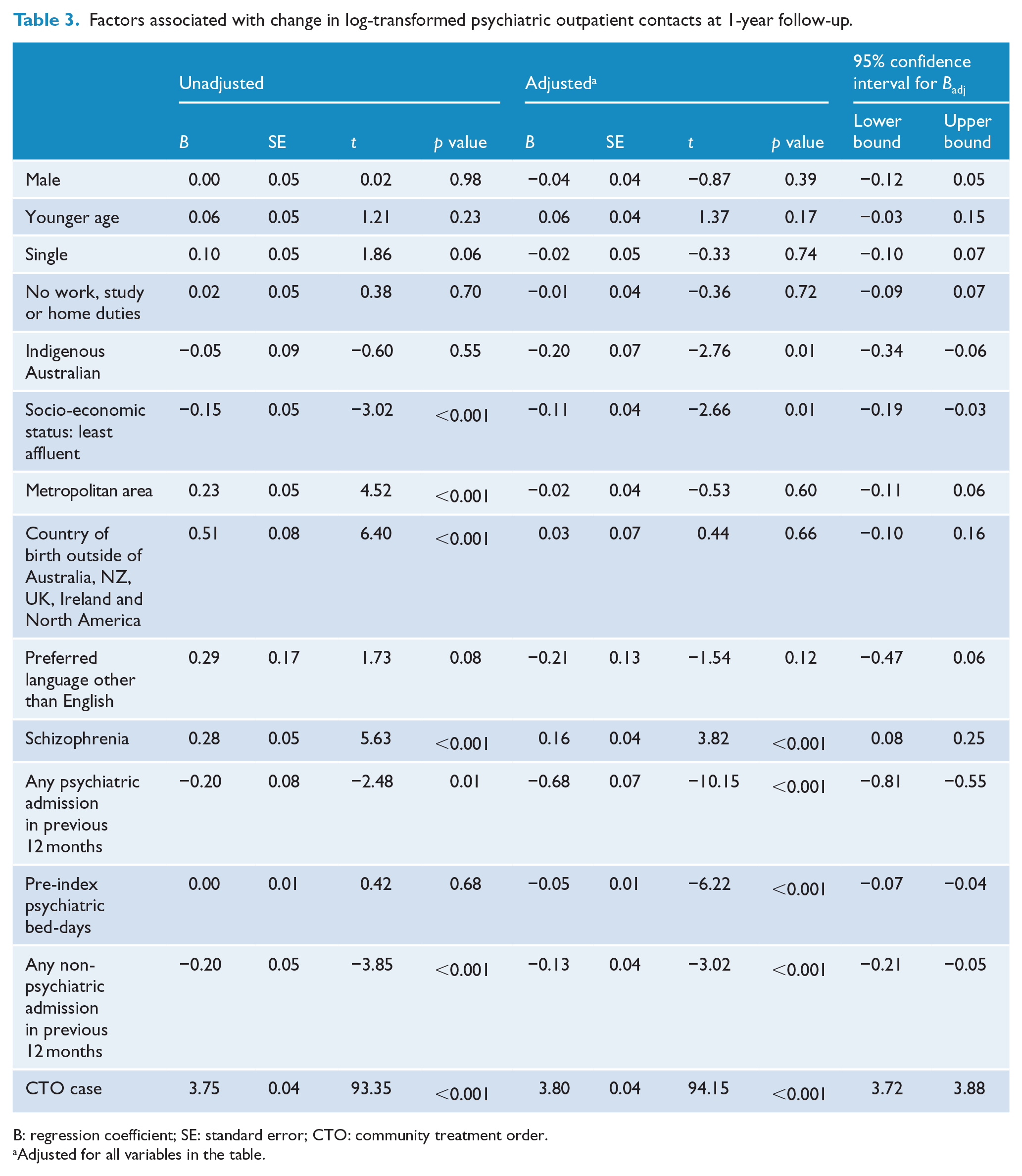
B: regression coefficient; SE: standard error; CTO: community treatment order.
Adjusted for all variables in the table.
Survival analyses
Over the 12 months of follow-up, 38.7% (n = 2874) of the CCT cases and 32.8% (n = 2434) of the controls were readmitted. Figure 3 shows that CCT cases also spent less time in the community prior to readmission on Kaplan–Meier survival analyses (log-rank χ2 = 5.14, p = 0.02).
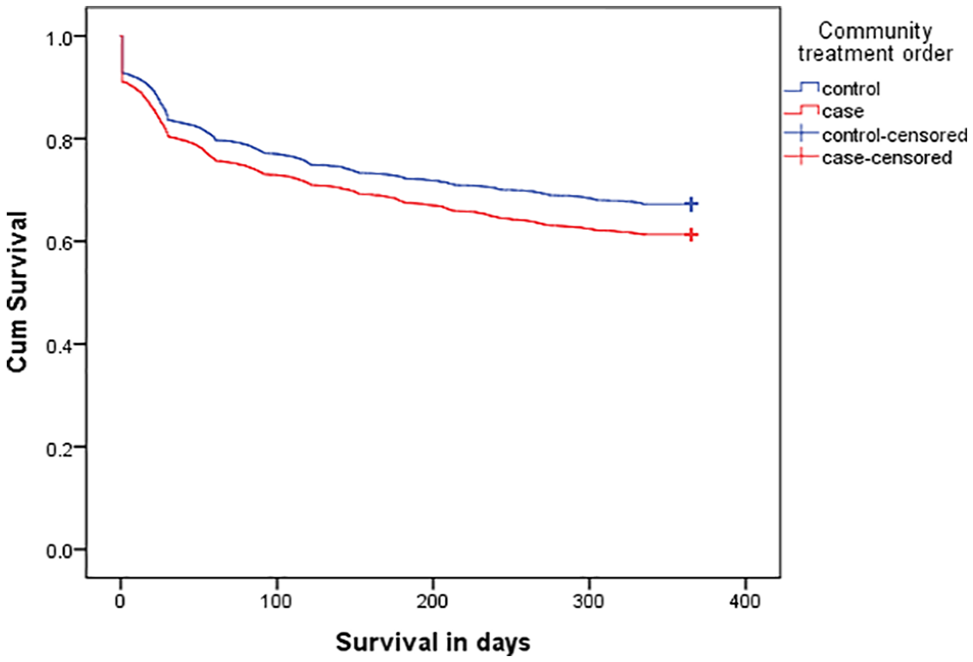
Time to readmission.
Table 4 shows variables that were associated with significant changes to the risk of earlier admission. We examined the relationship between the variables of interest and admission using both crude and adjusted ratios (Table 4). This shows that CCT cases were significantly more likely to be admitted in the subsequent year than those in the control group. Apart from being on an order, factors that were associated with a significantly greater risk of earlier admission on adjusted analyses were female sex, younger age, metropolitan residence, a diagnosis of schizophrenia and prior health service use. Cultural and linguistic diversity in terms of country of birth was also associated with decreased survival in the community.
Demographic and health service factors associated with early readmission.
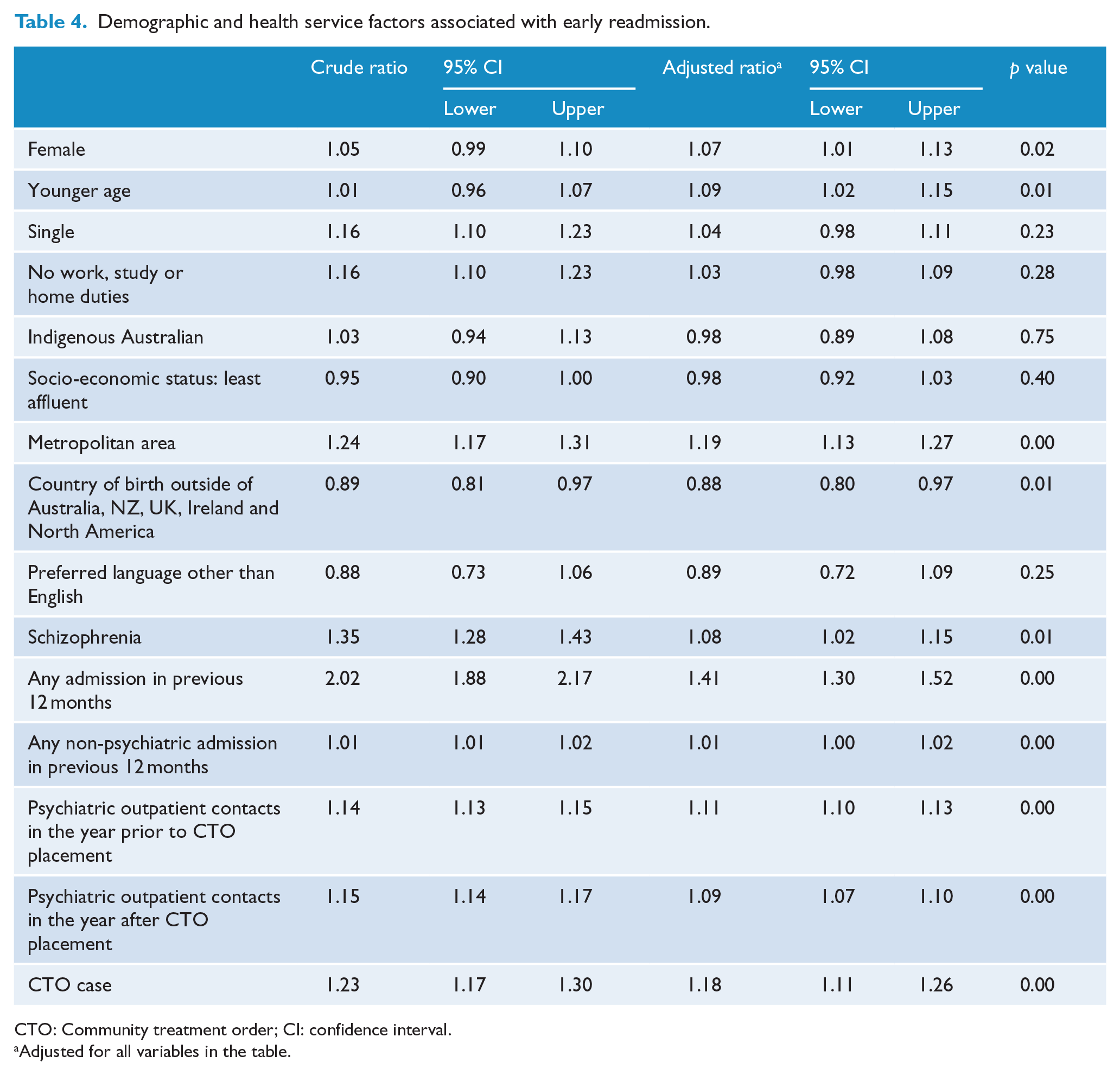
CTO: Community treatment order; CI: confidence interval.
Adjusted for all variables in the table.
Sensitivity analyses
We found similar results restricting the analyses to just those patients on CTOs (n = 7228), excluding FOs. CTO placement was more likely in indigenous patients (adjusted odds ratio [ORadj] = 1.44; 95% confidence interval [CI] = [1.27, 1.64]), people from a CALD background (ORadj = 1.52; 95% CI = [1.35, 1.71]), or those who had a preferred language other than English (ORadj = 1.66; 95% CI = [1.30, 2.13]). Being on a CTO shortened the time to readmission (adjusted hazard ratio [HRadj] = 1.18; 95% CI = [1.10, 1.26]) and did not reduce subsequent bed-days (B = 0.052, SE = 0.055, t = –0.95, p = 0.34). However, community contacts remained increased (B = 3.84, SE = 0.41, t = –9.47, p < 0.001). Finally, we found similar results for survival using propensity score analysis (HRadj = 1.13; 95% CI = [1.07, 1.19]).
Discussion
To our knowledge, this is the first study to report that Indigenous Australians are more likely to be subject to CCT. This is of concern and is in contrast to the only other similar study from Western Australia where Indigenous Australians were no more likely to be placed on such orders (Kisely and Xiao, 2017). The reasons for this are unclear as Indigenous Australians make up 3.5% of the population in both states. Explanations might include differences in the geographical distribution of Indigenous Australians, or the configuration and availability of services. For instance, data from the Australian Institute of Health and Welfare (2016) show that while the number of involuntary visits as a percentage of overall community contacts has remained stable at around 3% in Western Australia, it increased from 8.9% to 22.3% in Queensland over the same period (Figure 4).
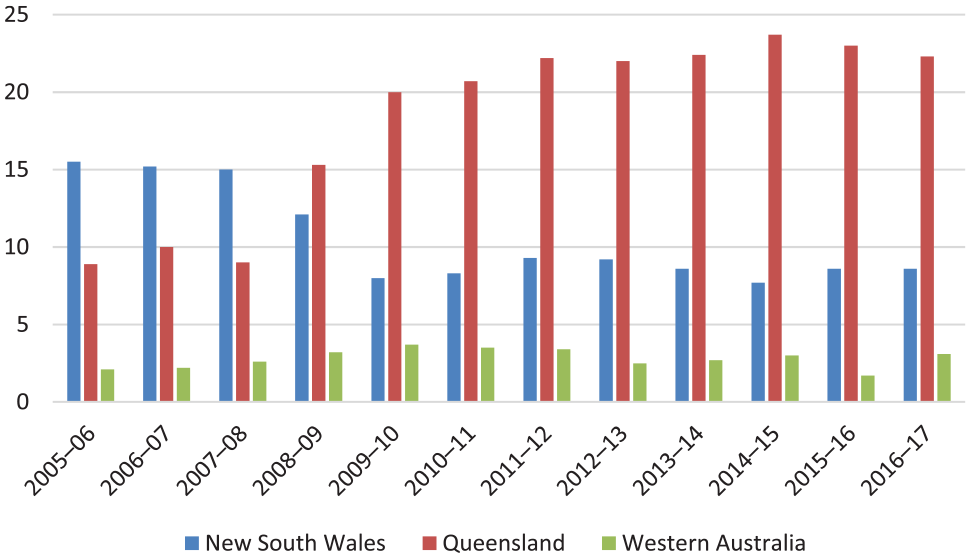
Number of involuntary visits as a percentage of overall community contacts.
Our results also add to the limited literature on the use of community orders in people from CALD populations. There have been only two jurisdiction-wide studies (Scotland and Western Australia) and, as in our data, these populations were significantly more likely to be subject to CCT (Bansal et al., 2014; Kisely and Xiao, 2017). The explanations may be similar to those for the higher rates of involuntary inpatient treatment in the same populations. These include the availability of culturally appropriate services, perceived discrimination and social isolation (Bansal et al., 2014; Karlsen et al., 2005). People from CALD backgrounds may therefore be reluctant to seek treatment and thus, when they do present, their symptoms are more severe (Straiton et al., 2014). This may be particularly relevant if English is spoken as a second language. Equity of access to mental health services is therefore essential so that mental health problems do not progress to the stage where compulsory treatment is required, whether this is as an inpatient or in the community.
In terms of effectiveness, and given the conflicting data on utility, it is important to study the use of compulsory community treatment in as many jurisdictions as possible. Although there has been work from Victoria, Western Australia and New South Wales, this is the first Queensland-wide study to investigate the effect on subsequent health service use. This is also the first study to include FOs, which are applied to patients charged with a serious offence. These are restrictive and include prescriptions that are not determined by the psychiatrist involved in directly in the provision of care (Suetani et al., 2019). Their nature fundamentally shifts the doctor–patient relationship, with the risk that the focus of care is custodial rather than recovery-oriented (Suetani et al., 2019).
We found no evidence that community orders reduced bed-days or delayed admission in the following 12 months, results that are consistent with most non-randomised studies using appropriately matched controls from around the world (Barnett et al., 2018). Within Australia, findings have been contradictory. Some work from Victoria has reported a beneficial effect but is limited by a reliance on some unusual outcomes that are different from those used elsewhere (Segal and Burgess, 2006; Segal et al., 2017). For instance, while most studies of CTO effectiveness specify that an outcome occur within a certain period of CTO placement, these papers reported on the mean number of bed-days per admission over 10 years without reference to the actual time of the order (Kisely et al., 2017a). Where results on total bed-days were presented, these were actually higher among the patients on CTOs than the controls. In other work, community treatment orders used on discharge from a first hospital admission were associated with a higher risk of readmission, rates only falling after subsequent hospital stays (Burgess et al., 2006). In addition, the generalisability of some of these findings is also limited by the fact that Victoria’s high rate of CTO use per head of population (Lawton-Smith, 2005) extends to cases of dementia (Segal and Burgess, 2006).
There have also been several papers from Western Australia. An initial study in the first year of operation of CTOs reported no difference in bed-days or admissions compared to controls matched on age, sex, discharge date and diagnosis (Preston et al., 2002). This approach was criticised for not taking into account an important reason for CTOs – to shorten future lengths of stay compared to pre-order levels. Over the subsequent decade, and in contrast to this study, CTO cases spent five fewer days in hospital from before the order compared to controls (Kisely et al., 2013).
However, when it was possible to adjust for forensic history by linking health and criminal justice data, the CTO group had increased readmission rates and lower community survival than matched controls (Kisely et al., 2004). This was confirmed in a further study that compared the CTO cases in Western Australia with matched controls from an international jurisdiction with a similar population and health service but no CTOs, the Canadian province of Nova Scotia (Kisely et al., 2005). This adjusted for the possibility that controls from the same jurisdiction may differ in ways for which it was not possible to match or adjust (Kisely et al., 2005). CTOs also had no effect on psychiatric symptomatology as measured by the Health of the Nation Outcome Scales (HoNOS) compared to matched controls at 6- and 12-month follow-up (Kisely et al., 2014).
Findings from New South Wales are similarly mixed. As in our results, an initial study found that community survival was reduced for people on CTOs compared to controls with no significant difference in the admission rate between the two groups (Vaughan et al., 2000). On the other hand, CTO cases on depot medication showed greater compliance and a significantly reduced readmission rate compared to those only receiving oral medication. However, limitations included a small sample from one health service and the suggestion that matching had not been entirely successful meaning that the controls were less ill and more insightful. A larger statewide study reported the reverse, with CTO cases having longer community survival and being at less risk of admission in the 6–12 months following placement (Harris et al., 2019).
It is unclear whether different rates of use in states could contribute to variations in outcome. Figure 4 shows the proportion of community contacts that are involuntary over 10 years for the three most populous states where data are available. On one hand, the proportion of involuntary contacts has fallen in NSW to 8.6% while it has risen to 22.3% in Queensland. This might suggest that the positive results for NSW reflect better targeting of the measure. On the other hand, Western Australia, where results are like those of this study (Kisely et al., 2004), had the lowest and most stable levels of the three states (Figure 4).
The one consistent finding across the literature is that CTOs increase community contacts compared to controls. However, as indicated previously, this is strictly speaking a process measure, not an outcome. If a CTO forces people to see a clinician, it is unsurprising that CTOs increase community contacts. Even so, our adjusted results suggest that community orders did not achieve this for either Indigenous Australians or those from CALD backgrounds.
In the absence of an effect over 12 months, some have argued that outcomes should be assessed for as long as a CTO is in place, however long that may be. For instance, the recent NSW study reported that CTOs had no effect on reducing subsequent days in hospital unless patients had been on them for over 2 years (Harris et al., 2019). Similarly, work from Victoria suggested that at least five orders were required to result in significantly reduced readmission rates (Burgess et al., 2006). Given that severe mental illnesses are long-term conditions, patients could potentially remain on them for the rest of their lives. In addition, any possible additional benefit from long-term placement would not explain the mixed findings when follow-up is limited to 12 months. For instance, the same NSW study reported benefit even within shorter periods of follow-up, while other Australian studies did not.
Limitations
This was a study of administrative health data, which may be subject to recording bias and lack information on social disability, risk, forensic history and dangerousness, as well as influences on service provision such as homelessness, family supports or substance use. We also relied on proxy indicators such as place of birth and preferred language to determine CALD status. In addition, we had to combine disparate countries because of limited numbers and this may have obscured important differences. Similarly, our data did not distinguish between Aboriginal Australians and Torres Strait Islanders.
In terms of outcomes, it is possible that cases and controls differed in ways for which it was not possible to match or adjust. In terms of the variables for which we had data, the fact that CCT cases were more likely to be single, unemployed, be diagnosed with schizophrenia, and have had more admissions but fewer community contacts prior to the order might suggest they were more unwell and more difficult to engage. This group may have had worse outcomes if they had not been on an order. Because of the low numbers of FOs, we were unable to undertake detailed comparisons with CTOs, other than a sensitivity analysis of their exclusion. In line with many other studies, outcome was restricted to 12-month follow-up and differences may have emerged over a longer period. However, this would not explain the variation in results when compared to studies of similar length.
Finally, our data relate to the Mental Health Act (2000) (QLD), which was replaced by the Mental Health Act (2016) (QLD) on 5 March 2017. The 2016 Act placed greater emphasis on capacity but retained both FOs and CTOs, the latter renamed treatment authorities. This may have implication for the applicability of our findings to current practice, as all the patients in our sample would have embarked on their orders under the provisions of the previous legislation. However, an evaluation of the impact of the new Act from the Office of the Chief Psychiatrist suggests little change in the number of orders, including those initiated in the community (Queensland Health, 2019). For instance, there was little difference in the number of community-based orders in the first full year of operation of the new Act (Queensland Health, 2018) compared to the previous year (Queensland Health, 2017). This mirrors findings in other Australian jurisdictions where a greater emphasis on capacity in updated legislation has not resulted in the anticipated decline of community orders, except possibly in Victoria (Light, 2019; Ryan, 2019). However, even in Victoria, it is unclear whether reductions in use are due to changes to the Act, or the effect of changes to funding in the state (Vine et al., 2019). For instance, there is evidence that Victorian Mental Health Tribunals are not correctly applying the assessment of capacity to their decisions (Ryan, 2019).
Given the uncertainty regarding their effectiveness, it is surprising that the use of CTOs in Australia remains high, raising questions about both the transparency and accountability of the mental health system (Light et al., 2012b). The markedly different rates of use do not seem to be explained by differences in legislation, suggesting the influence of factors in addition to just clinical need (Lawton-Smith, 2005; Light et al., 2012a). Reasons for these differences are unclear and merit further research. Clinician-based factors might include perceived liability for the conduct of patients in the community, the possible impact of coercion on the therapeutic alliance and expectations of third parties (Dawson, 2007). Past patterns of involuntary outpatient care, as well as the structure and quality of the mental health services, may also contribute (Dawson, 2007; Light et al., 2017).
In conclusion, and as in other coercive treatments, Indigenous Australians and people from CALD backgrounds are more likely to be placed on CCT. This is of particular concern given the fact that their effectiveness remains unclear.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.