
Abstract
Objectives:
Australia and New Zealand have some of the highest rates of compulsory community treatment order use worldwide. There are also concerns that people from culturally and linguistically diverse backgrounds may have higher rates of community treatment orders. We therefore assessed the health service, clinical and psychosocial outcomes of compulsory community treatment and explored if culturally and linguistically diverse, indigenous status or other factors predicted community treatment orders.
Methods:
We searched the following databases from inception to January 2020: PubMed/Medline, Embase, CINAHL and PsycINFO. We included any study conducted in Australia or New Zealand that compared people on community treatment orders for severe mental illness with controls receiving voluntary psychiatric treatment. Two reviewers independently extracted data, assessing study quality using Joanna Briggs Institute scales.
Results:
A total of 31 publications from 12 studies met inclusion criteria, of which 24 publications could be included in a meta-analysis. Only one was from New Zealand. People who were male, single and not engaged in work, study or home duties were significantly more likely to be subject to a community treatment order. In addition, those from a culturally and linguistically diverse or migrant background were nearly 40% more likely to be on an order. Indigenous status was not associated with community treatment order use in Australia and there were no New Zealand data. Community treatment orders did not reduce readmission rates or bed-days at 12-month follow-up. There was evidence of increased benefit in the longer-term but only after a minimum of 2 years of use. Finally, people on community treatment orders had a lower mortality rate, possibly related to increased community contacts.
Conclusion:
People from culturally and linguistically diverse or migrant backgrounds are more likely to be placed on a community treatment order. However, the evidence for effectiveness remains inconclusive and limited to orders of at least 2 years’ duration. The restrictive nature of community treatment orders may not be outweighed by the inconclusive evidence for beneficial outcomes.
Keywords
Introduction
Community treatment orders (CTOs) in Australia and New Zealand allow compulsory treatment in the community for people with mental illness. They were first introduced in Victoria in 1980s and their use has subsequently spread throughout Australia and New Zealand. In international comparisons, CTO use in both Australia and New Zealand is comparatively high, and rising, although rates vary considerably within both countries. For instance, rates in Australia range from 40.0 per 100,000 population in Western Australia to 112.5 per 100,000 in the adjacent state of South Australia (Light et al., 2017). Similarly, the national average in New Zealand of 84 per 100,000 encompasses a low of 33 per 100,000 in Canterbury and a high of 151 per 100,000 in the Waitemata (O’Brien, 2014).
There is conflicting and equivocal evidence for the efficacy of CTOs in Australasia and elsewhere (Kisely, 2016; Maughan et al., 2014; Rugkasa, 2016). In addition, although people from Indigenous or culturally and linguistically diverse (CALD) backgrounds are over-represented in terms of incarceration and compulsory admissions to hospital, little is known about whether this also applies to compulsory community treatment.
In terms of outcomes, there have been numerous narrative reviews, some systematic, that have included information on CTO use in Australia and New Zealand (Maughan et al., 2014; Rugkasa, 2016), but only two meta-analyses of the available data, one of which was a Cochrane systematic review (Barnett et al., 2018; Kisely et al., 2017). Both concluded that there was limited evidence that CTOs improved outcomes in terms of readmission rates, number of inpatient days or psychosocial functioning. The only consistent effect was an increase in community contacts.
However, both had limitations especially as regards applicability to Australia and New Zealand. The Cochrane systematic review was limited to just three randomised controlled trials in the United Kingdom and the United States (Kisely et al., 2017). The other did include a wider range of studies including some from Australia, although not New Zealand (Barnett et al., 2018). However, this study had several limitations (Barnett et al., 2018). First, it did not include several more recent studies and second, it only presented analyses of unadjusted data. In non-randomised studies such as cohort, case control and cross-sectional studies, it is important to adjust for potential confounders to adjust for the possibility that people on compulsory community treatment may differ in important ways from voluntary controls. In addition, the review only considered admissions, bed-days and community contacts and did not consider other outcomes such as clinical features. Finally, it did not consider predictors of compulsory community treatment placement.
We therefore undertook a systematic review and meta-analysis on both the predictors and outcomes of CTO placement in Australia and New Zealand. We specifically assessed whether people from Indigenous or CALD backgrounds were more likely to be on compulsory community treatment, as well as the subsequent effect of CTOs on a range of health service, clinical and psychosocial outcomes.
Method
Search strategy
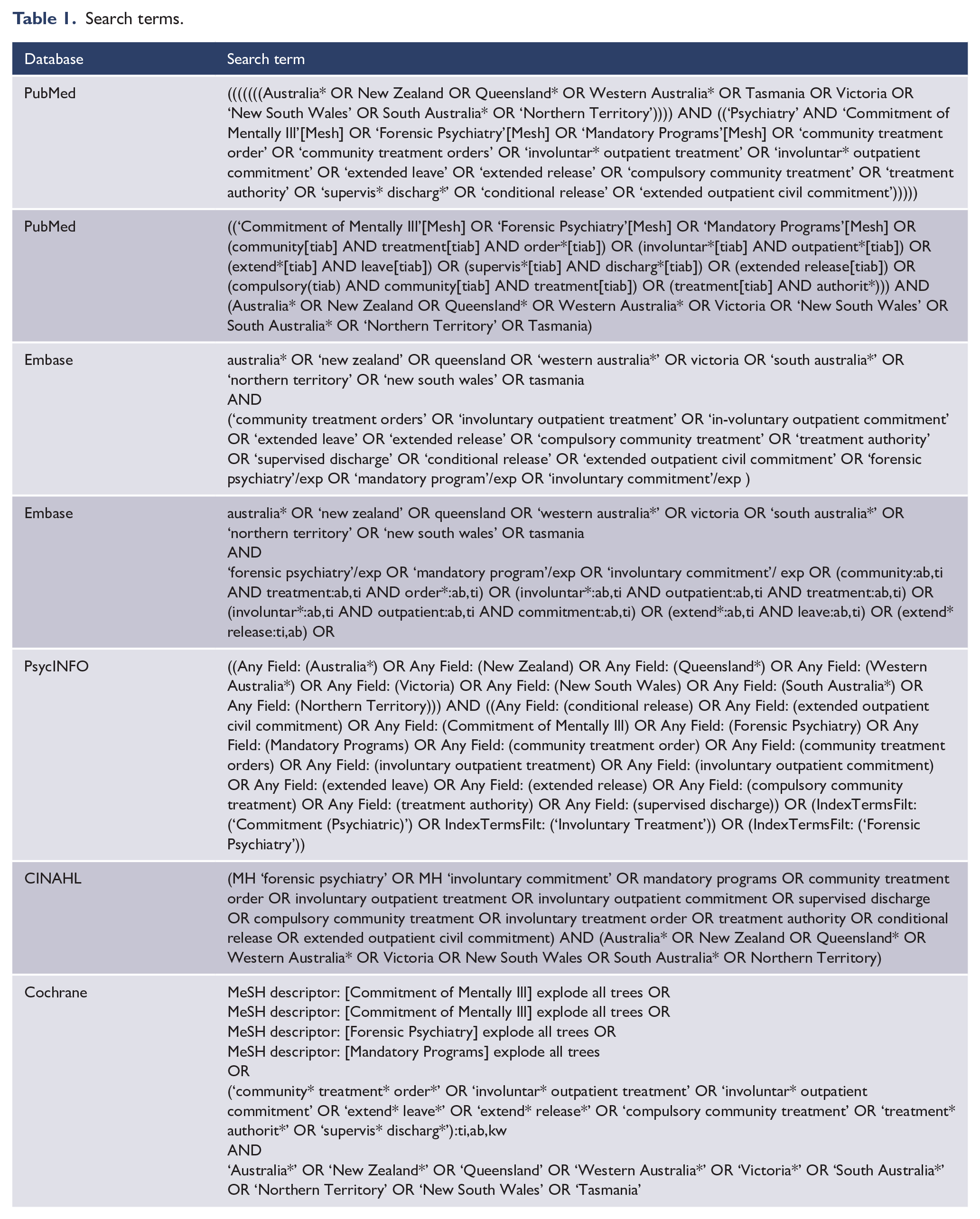
The protocol for this systematic review was registered with PROSPERO (CRD42020155996) and the Australian New Zealand Clinical Trials Registry (ACTRN12620000333910). We followed guidelines from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Moher et al., 2009). We sought advice from a research librarian prior to the commencement of this search. Articles were located by searching the following databases from inception to January 2020: PubMed/Medline, Embase, CINAHL and PsycINFO. There were no language restrictions. Table 1 shows our search terms. Ethical approval was not required for this systematic review, as all included primary data that had previously been published.
Search terms.
Two of the authors (S.M. and D.Y.) independently screened records and abstracts. Where there was a lack of consensus, a third reviewer was consulted (S.K.). The reference lists of selected retrieved papers were screened to identify additional studies that met inclusion criteria.
Inclusion criteria
We included any of the following study designs conducted in Australia or New Zealand that compared people on CTOs for severe mental illness with controls receiving voluntary psychiatric treatment: randomised controlled trials, cohort, case control and cross-sectional studies.
Exclusion criteria
We excluded studies of compulsory treatment in the community for drug or alcohol dependence and community treatments for mentally or behaviourally disordered offenders, as well as any designs that did not compare people on a CTO with controls from the same jurisdiction receiving voluntary psychiatric treatment.
Outcomes
Our primary outcomes were hospital admissions, bed-days and community contacts in the 12 months following CTO placement. We included bed-days as well as admissions given the meaning of the latter can be unclear. For instance, does compulsory community treatment reduce admission rates, thereby allowing individuals to remain in their communities during treatment, or are rates increased as a result of earlier identification of relapse? (Kisely, 2009; Kisely et al., 2017) We focused on outcomes at 1 year as this is the most common end-point in the literature and the impact of an intervention on health service use beyond 1 year is difficult to ascertain (Kisely et al., 2017).
However, we also assessed for the presence of these events up to 10 years from entry into the study. Secondary outcomes included the following over the same time frames: psychiatric symptoms as measured by a standardised psychiatric instrument, concordance with psychiatric treatment, employment as defined by full or part-time work or study and contacts with the criminal justice system as defined by any arrest, conviction or imprisonment.
Study quality
All studies identified for inclusion were cohort and cross-sectional studies. We assessed quality using the Joanna Briggs Institute tool for non-randomised studies. This covers the three following areas: selection of the study groups in terms of case definition, representativeness and source of controls; comparability of the groups such as the use of matching or multivariate techniques; and measurement of exposure and outcomes in a valid and reliable way. The version for cross-sectional studies has eight items and the one for longitudinal designs has 11 items, with a score of seven and above an indicator of study quality (Koh et al., 2011).
Analysis
Where data were available for two or more studies, they were combined in a meta-analysis using RevMan or Win-Pepi (Abramson, 2011). We gave preference to data from studies that had been adjusted for potential confounders, particularly for the analyses of outcomes. For dichotomous predictors of CTO placement such as gender, single status and not being engaged in work, study or home duties, we combined data using the odds ratio, while we used the log adjusted risk ratio for outcomes such as readmission or mortality. The latter enabled us to plot risk and hazard ratios on the same forest plots even though they were not combined in the same meta-analysis. We used the mean difference for continuous data such as the number of bed-days or community contacts, assessing for publication bias where there are at least 10 studies. We used an I2 statistic value of greater than 50% as an indicator of significant heterogeneity. We explored any heterogeneity further through sensitivity analyses of the effect of omitting each study in turn. The random effects model was used for all the analyses because we could not definitively exclude between-study variation even in the absence of statistical heterogeneity.
Results
We found 7487 citations of interest in the initial electronic searches of the Cochrane Central Register of Controlled Trials, PubMed/Medline, Embase and PsycINFO. Of these 50 full-text papers were potentially relevant and assessed for eligibility (Figure 1). In all, 30 publications from 12 studies met inclusion criteria, of which 24 publications could be included in a meta-analysis (Figure 1 and Table 2). Allowing for overlap between the studies, there were approximately 53,170 subjects and 164,864 controls. Table 3 gives details of those studies excluded at the full-text level.
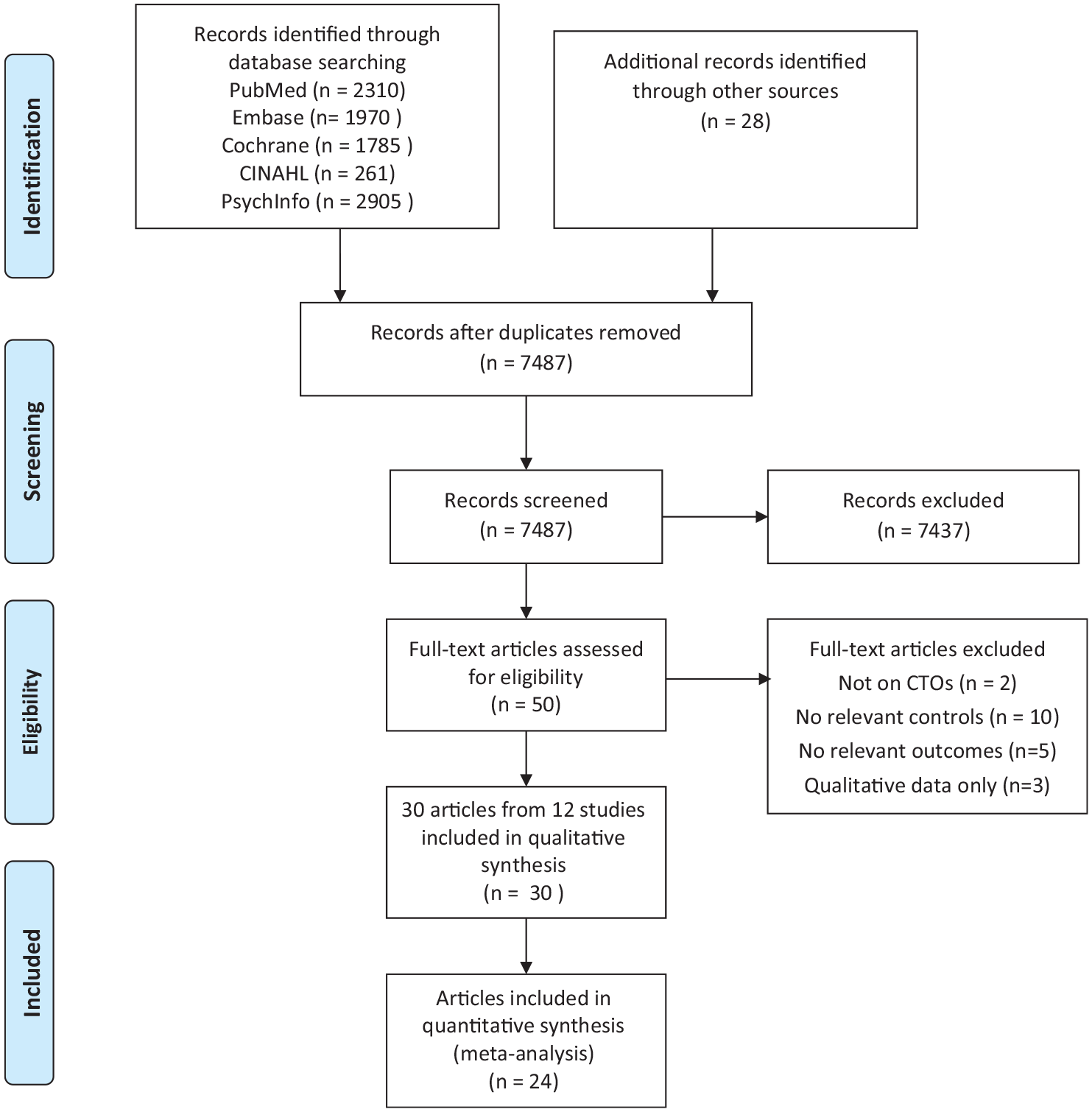
PRISMA 2009 flow diagram.
Included studies.
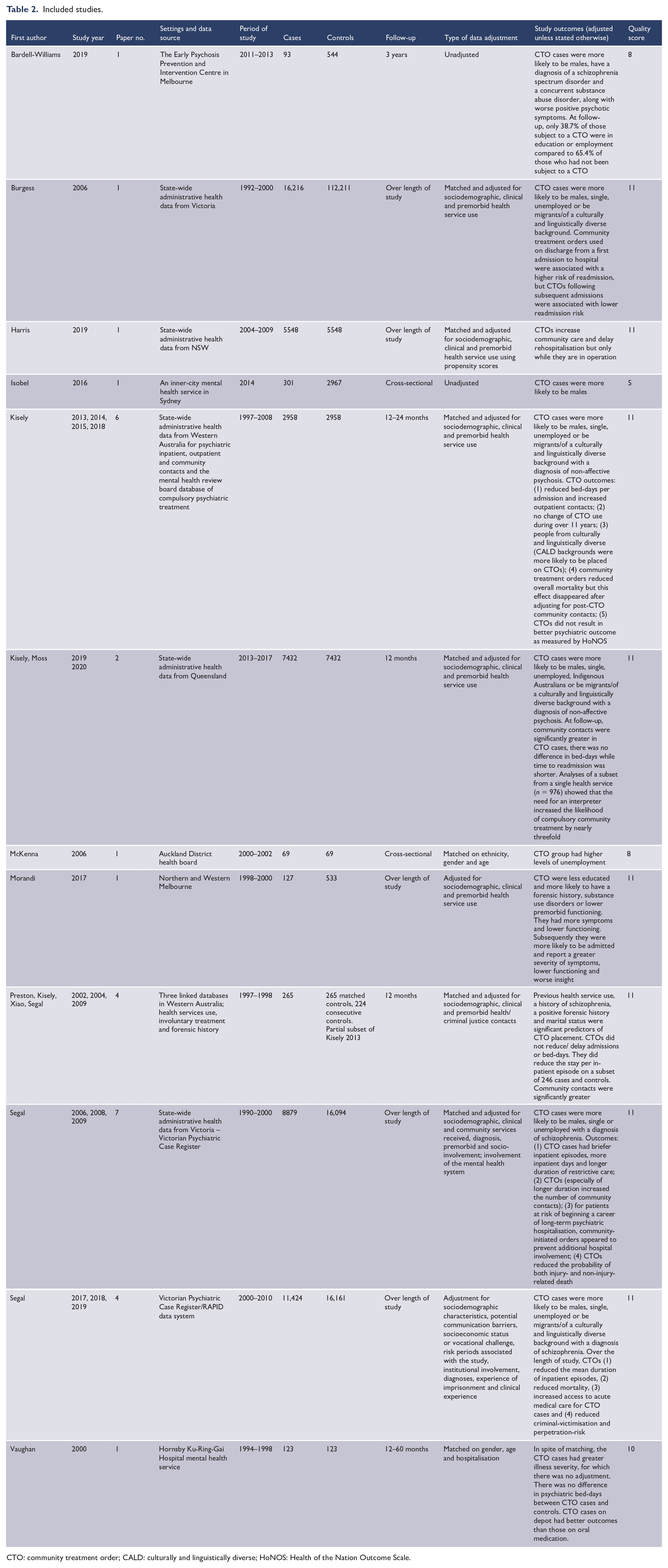
CTO: community treatment order; CALD: culturally and linguistically diverse; HoNOS: Health of the Nation Outcome Scale.
Excluded papers.
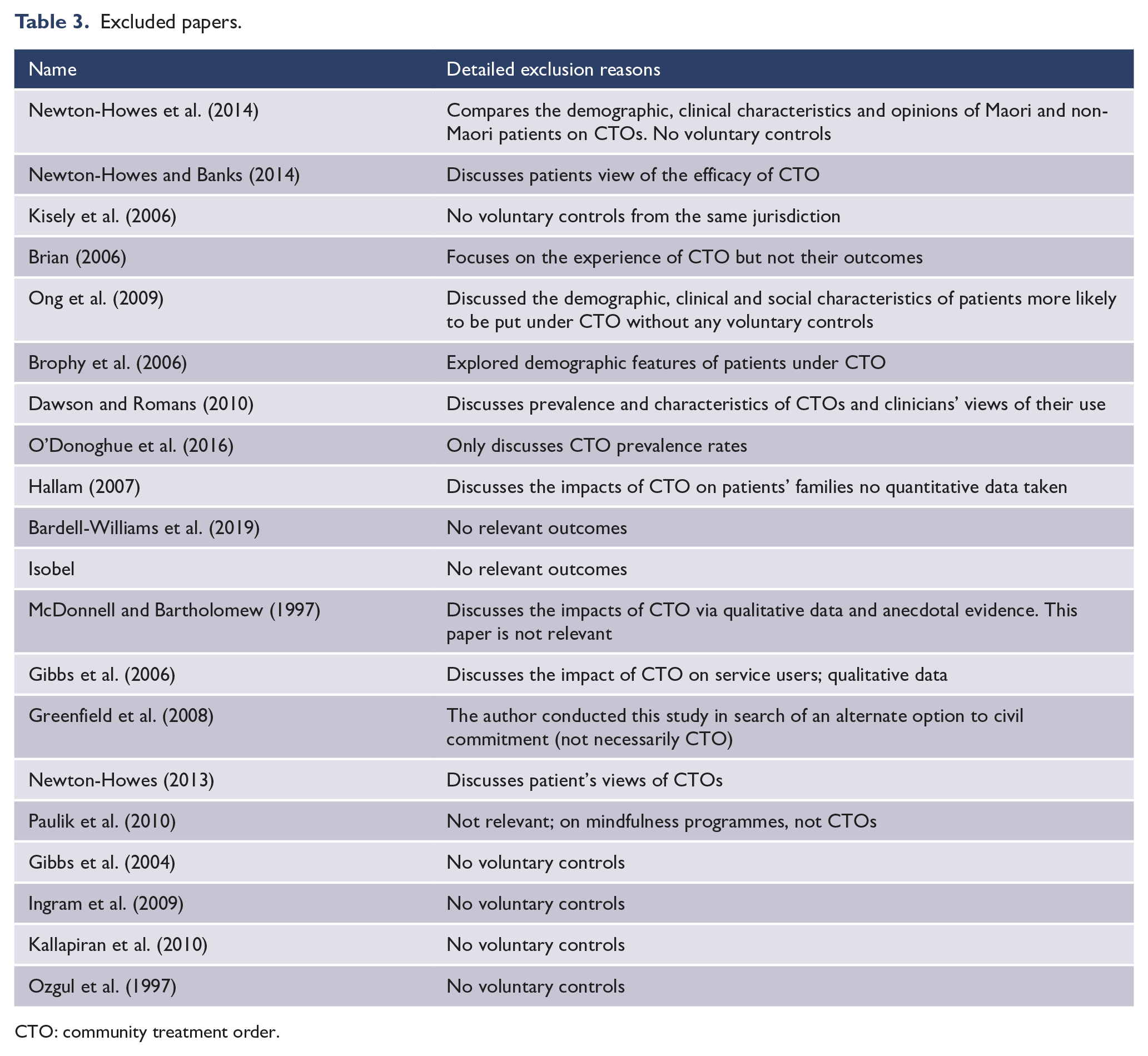
CTO: community treatment order.
Of the 12 included studies, 5 came from Victoria (Bardell-Williams et al., 2019; Burgess et al., 2006; Morandi et al., 2017; Segal and Burgess, 2006a; Segal et al., 2017a), 3 from New South Wales (NSW) (Harris et al., 2019; Isobel and Clenaghan, 2016; Vaughan et al., 2000), 2 from Western Australia (Kisely et al., 2013a; Preston et al., 2002) and 1 each from Queensland (Kisely et al., 2020) and New Zealand (McKenna et al., 2006). There were none from South Australia, Tasmania or the two territories. All but four used administrative data, with seven using linked state-wide data sets from Victoria, Western Australia and NSW and Queensland. In two studies, this included linkages to criminal justice data. Of the remainder, three were file audits and the fourth a survey
The bulk of individual articles came from three large administrative data sets. The first study was of Victorian administrative data from 1990 to 2000 (Segal and Burgess, 2006a, 2006b, 2006c, 2006d, 2006e, 2008, 2009). The second was of CTOs in Western Australia in the year prior and following their implementation from 1998 to 1999 (Kisely et al., 2004; Preston et al., 2002; Segal et al., 2009; Xiao et al., 2004). This was later extended till 2011 (Kisely et al., 2013a, 2013b, 2014a, 2014b, 2015; Kisely and Xiao, 2017). The third study was again of Victorian administrative data, this time from 2000 to 2010 (Segal et al., 2017a, 2017b, 2018, 2019). Study quality was good with all but one scoring seven or above (Table 2).
Factors associated with CTO placement
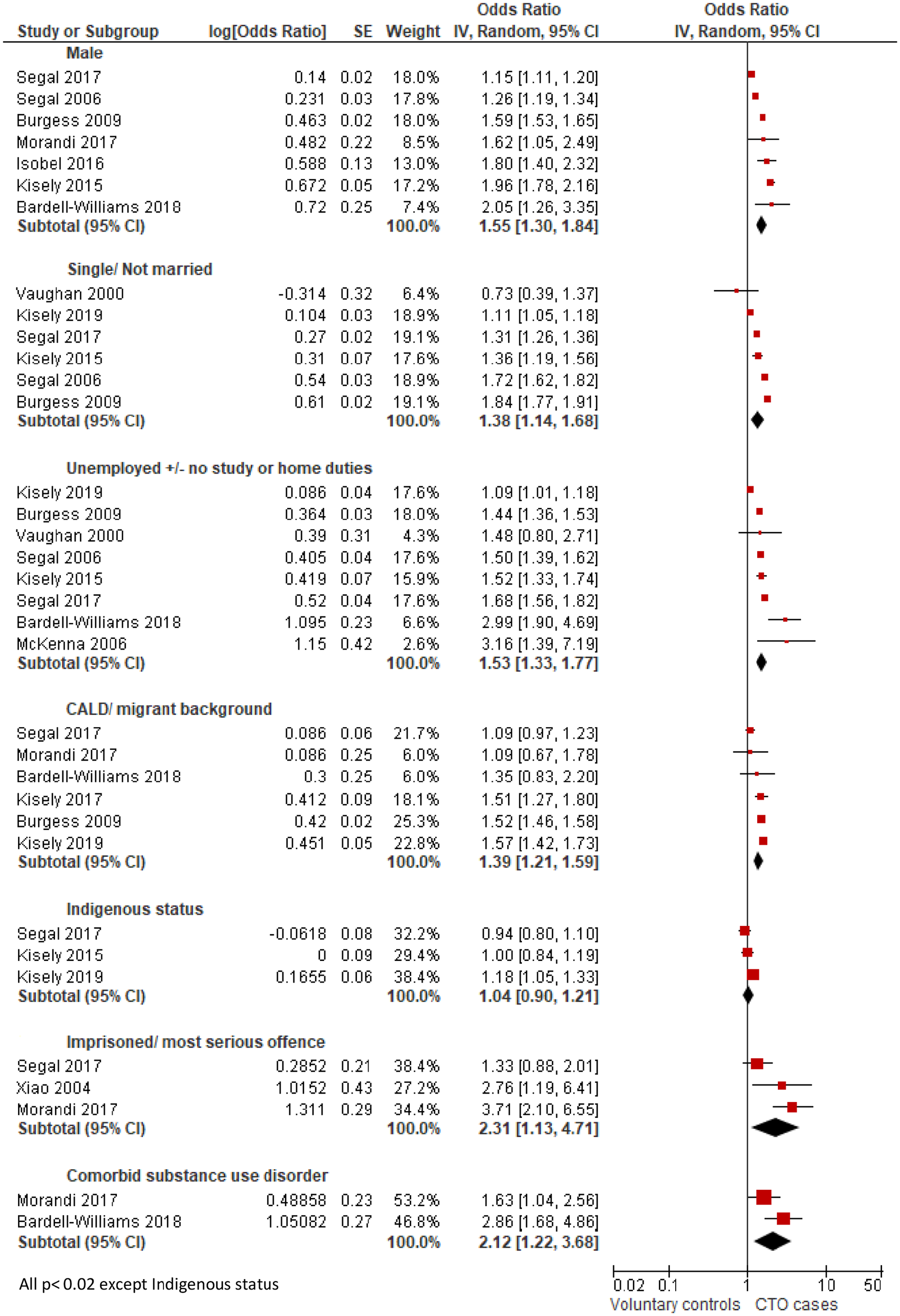
Nine papers from eight studies had data that could be meta-analysed (Figure 2). Seven studies were from Australia and the eighth from New Zealand. People who were male, single and not engaged in work, study or home duties were significantly more likely to be subject to a CTO. In addition, those from a CALD or migrant background were nearly 40% more likely to be on an order. This was reflected in the findings from two individual studies that were not included in the meta-analysis where those who had a preferred language other than English were 66% more likely to be on a CTO (Kisely et al., 2020), while those who required an interpreter had nearly a threefold greater risk of placement (Moss et al., 2018). By contrast, Indigenous status was not associated with being on a CTO. Other factors associated with being on a CTO were comorbid substance use disorders and prior contacts with the criminal justice system in terms of imprisonment or serious offences.
Factors associated with CTO placement.
In terms of diagnosis, patients with schizophrenia or non-affective psychosis were significantly more likely to be on a CTO (Bardell-Williams et al., 2019; Kisely et al., 2013a, 2015, 2020; Segal and Burgess, 2006a; Segal et al., 2017a). However, it was not possible to meta-analyse whether particular psychiatric disorders were associated with CTO placement because of the wide range of ways they were classified. Over 10% of the study sample from two Victorian studies that spanned 20 years had a diagnosis of dementia (Segal and Burgess, 2006a; Segal et al., 2017a).
Effect of CTOs on inpatient outcomes
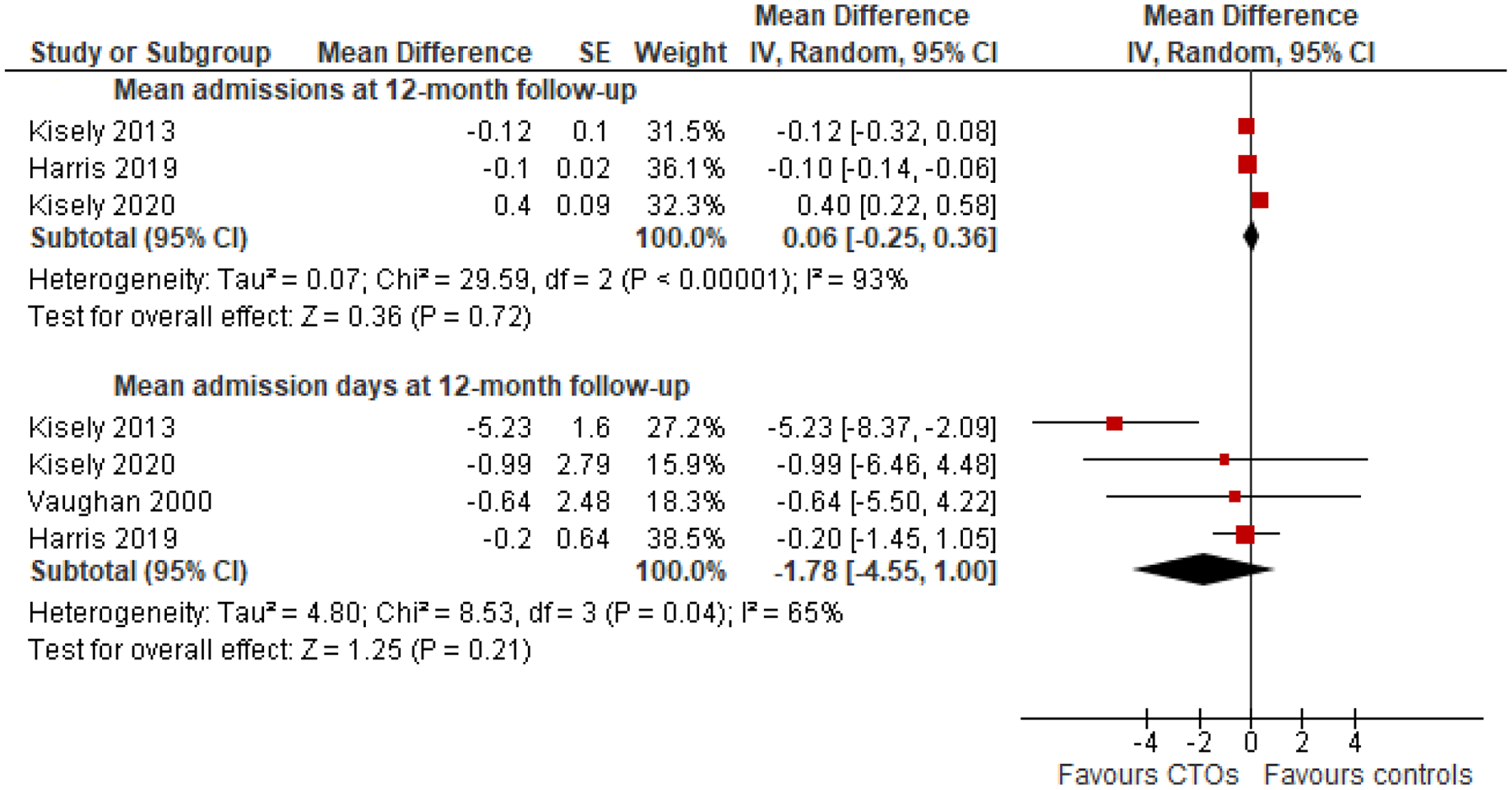
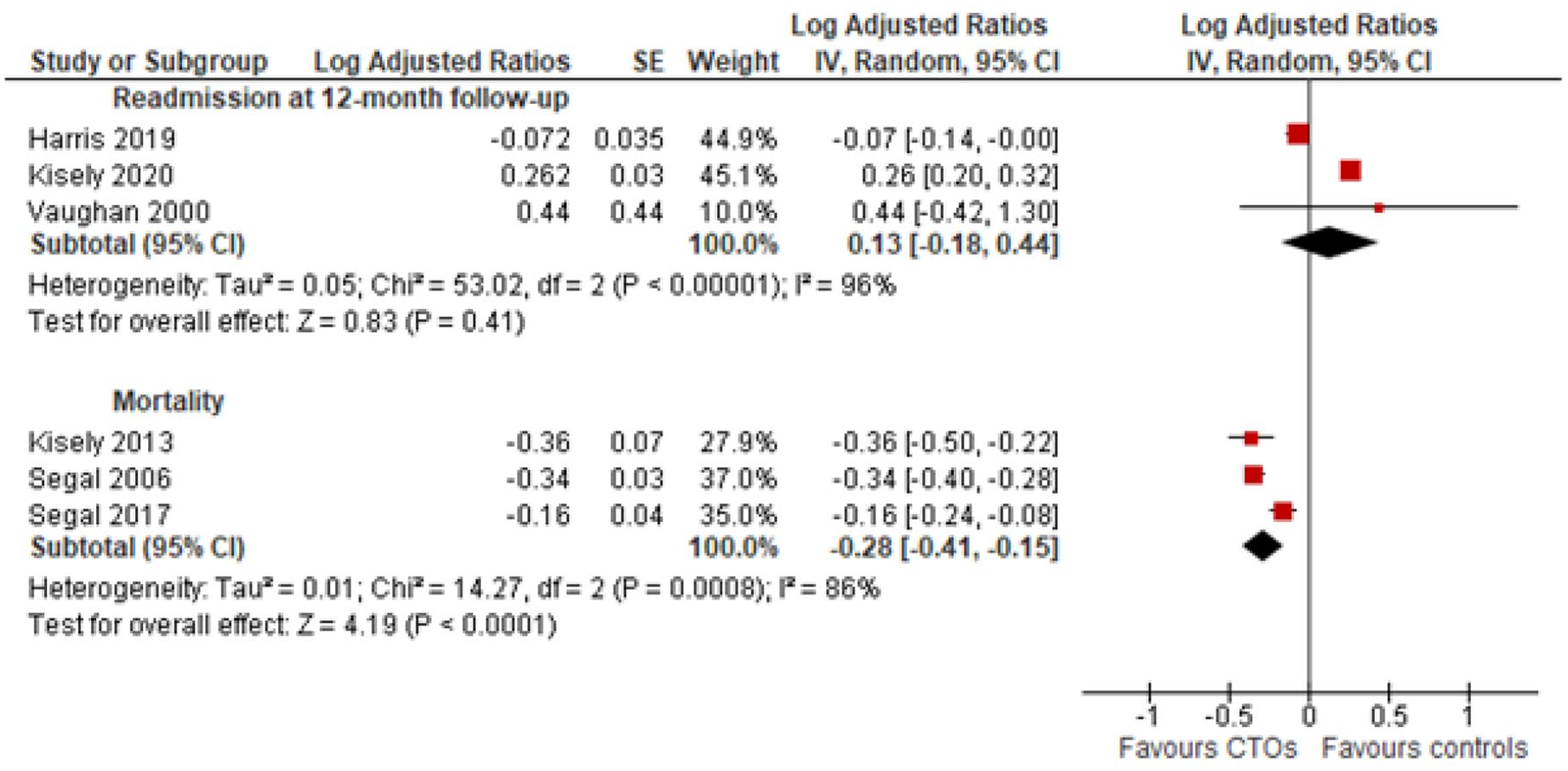
It was possible to combine data from five studies for inpatient outcomes at 12 months follow-up. All these studies considered the influence of potential confounders through the use of matching or multivariate analyses. This included demographic variables, previous health service use, diagnosis and, in some cases, forensic history. However, in the case of one, matching was not entirely successful with evidence that the CTO cases had more severe illness (Vaughan et al., 2000). There were no significant differences between CTO cases and controls in the mean number of admissions and bed-days (Figure 3), or the overall risk of admission (Figure 4). CTO cases also had a lower likelihood of community survival (hazard ratio = 0.13; 95% confidence interval [CI] = [0.05, 0.20]; three studies; I2 = 81%).
Mean number of readmissions and bed-days over 12 months.
Ever readmitted and mortality.
In two other studies, both from Victoria, the time of follow-up was unclear. This is because the effect of CTOs on inpatient use was compared to controls over the course of the study in terms of the mean number of bed-days per admission over 10 years without specific reference to the timing of CTO placement and how much occurred prior to the order. As a result, it was impossible to include the data in the meta-analysis. In both studies, the mean duration of inpatient stay per admission in the CTO group was less than for controls over the 10 years of the study. However, in the study where it was measured, total inpatient days were actually higher in the CTO group.
Two studies evaluated the longer-term effects of CTOs, one from Victoria and one from NSW (Burgess et al., 2006; Harris et al., 2019). Both used state-wide administrative data with statistical adjustment for potential confounders when comparing CTO cases with controls. In the Victorian study, while the risk of admission increased following CTO placement in the initial years of use, there was a lower readmission risk from the fifth order onwards. The risk also declined over the 8 years of the study period (Burgess et al., 2006). Similarly, the NSW study found that the greatest reduction in admissions and bed-days compared to controls was in those who had been on CTOs for more than 24 months (Harris et al., 2019).
Effect of CTOs on outpatient/community outcomes
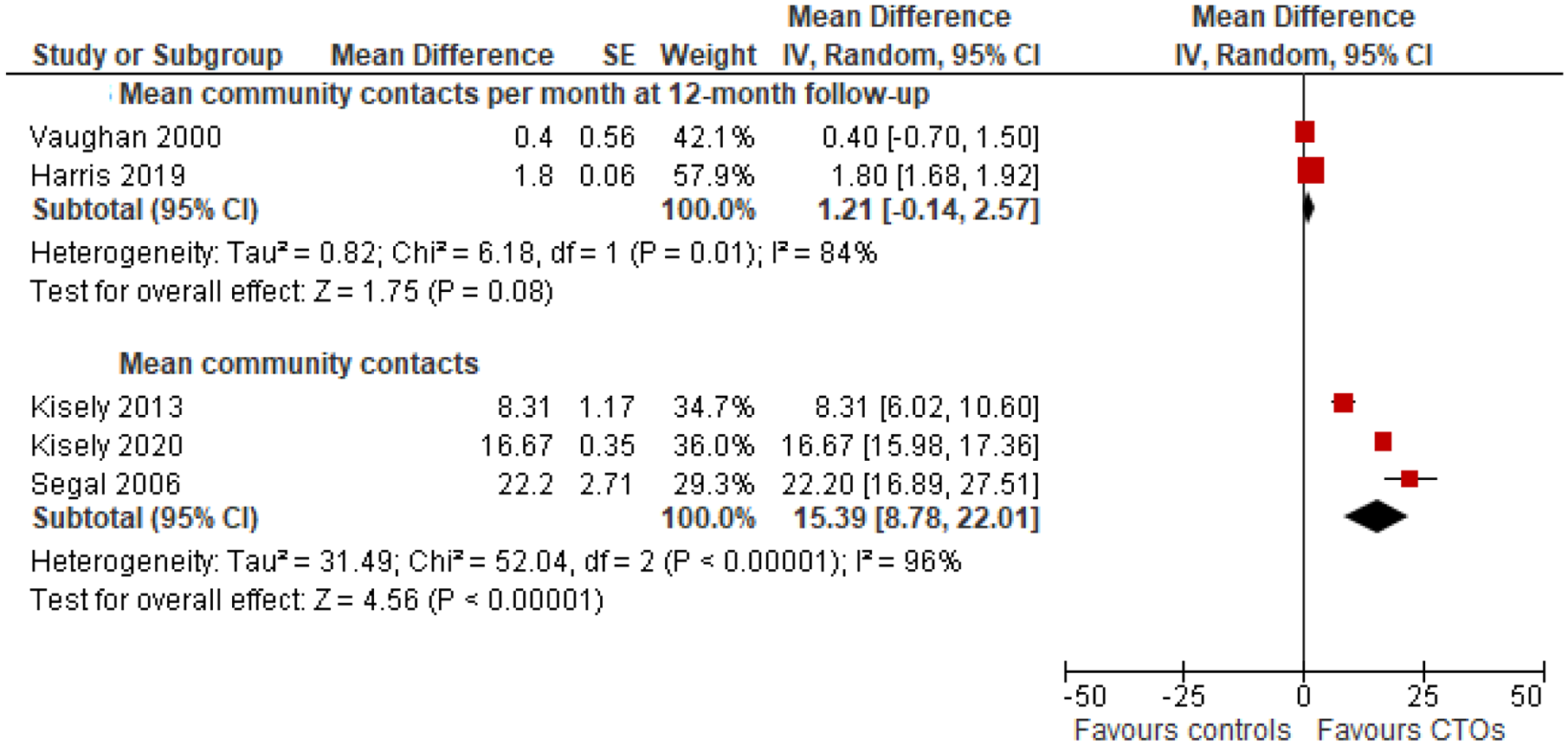
CTOs significantly increased outpatient and community contacts in four out of the five studies where this was measured with an average increase of 15.4 days compared to controls (Figure 5). This came down to 12.6 days when we restricted analyses to the first 12 months of follow-up.
Mean number of outpatient or community contacts.
Other outcomes
It was only possible to combine data on mortality (Figure 4). In one study, this was at both 1- and 2-year follow-up (Kisely et al., 2013b); in the other two, it was unspecified (Segal and Burgess, 2006b; Segal et al., 2017b). Mortality was significantly lower in the CTO group (Figure 4), although in one study this benefit was no longer apparent after adjusting for outpatient or community contacts following placement (Kisely et al., 2013b). In terms of other outcomes, one paper reported no difference in Health of the Nation Outcome Scale scores (HoNOS) between CTO cases and controls at both 6- and 12-month follow-up (Kisely et al., 2014a). One Victorian study reported that CTOs increased access to medical care for physical comorbidities over the duration of the study (Segal et al., 2018); another from Western Australia reported that orders did not improve access to specialist procedures at 1- and 2-year follow-up (Kisely et al., 2014b). Finally, the same Victorian study reported that over a decade those on CTOs were less likely to be the victims or perpetrators of crime although, again, there was no specific reference to the time of CTO placement (Segal et al., 2019).
Heterogeneity and publication bias
All the above results showed significant heterogeneity. We therefore explored this by excluding each study in turn in every analysis. This resulted in I2 values of 0% in six analyses but generally unchanged results (Table 4). We were unable to analyse for the effects of publication bias as none of the analyses had 10 or more studies.
Sensitivity analyses of heterogeneity.
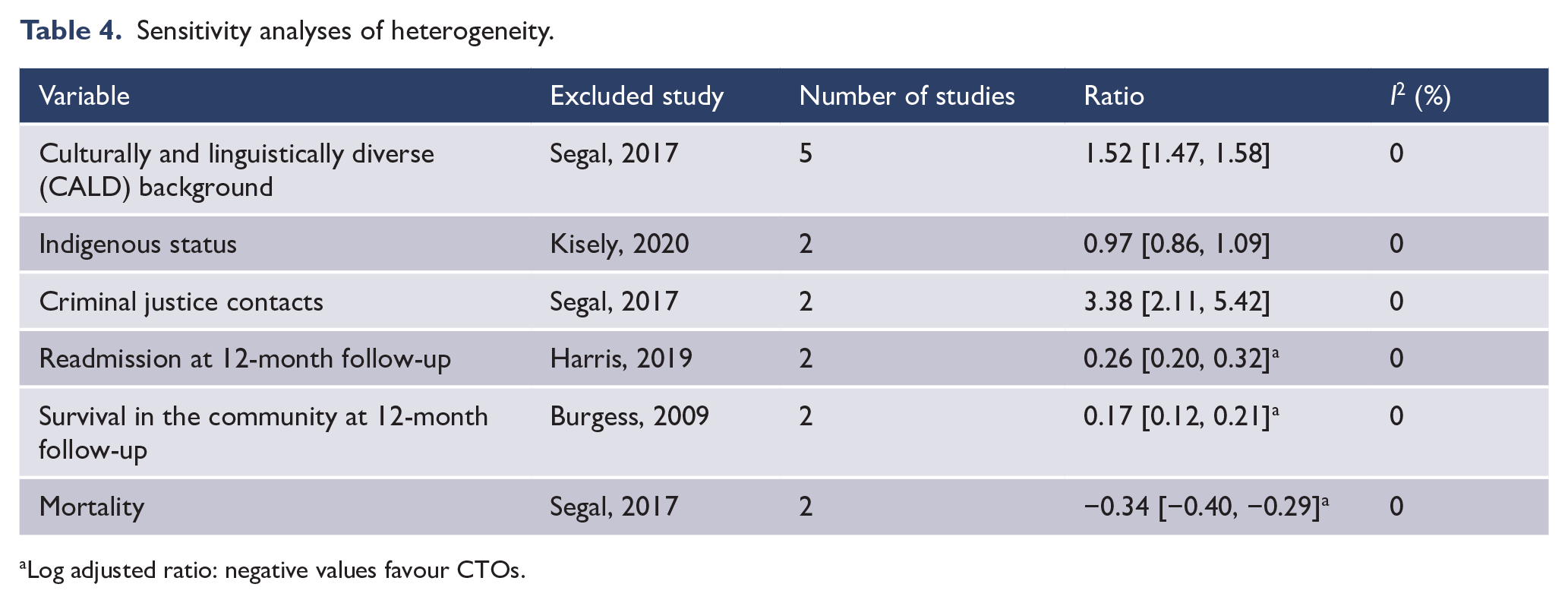
Log adjusted ratio: negative values favour CTOs.
Discussion
This is the first systematic review and meta-analysis of predictors and outcomes of compulsory community treatment in Australia and New Zealand. The findings may have relevance for other jurisdictions such as Scotland, England and Wales that have similar clinician-initiated orders, as opposed to court-ordered outpatient commitment in the United States. On meta-analysis, male gender, single status, a forensic history and substance use disorders were all associated with CTO placement. In addition, results from single studies suggested that people with non-affective psychoses or schizophrenia were also more likely to be placed on an order.
Of concern, we found that Australians from CALD backgrounds were significantly more likely to be subject to an order mirroring studies from both Scotland and London (Bansal et al., 2014; Patel et al., 2011). This finding is also consistent with results that could not be included in the meta-analysis where patients who required an interpreter were almost three times more likely to be treated on a CTO than those who did not require an interpreter (Moss et al., 2018). In general, experiences of the mental health system for people from a CALD background can be very different. Admissions are more likely to follow home visits, they are less likely to be referred to specialists by their general practitioner, they are more likely to be subject to involuntary admission and the police are more likely to be involved in the admission or readmission process (Mfoafo-M’Carthy, 2014; Stolk et al., 2008). Explanations include an inability to communicate with service providers, poor staff attitudes, not being able to have their families present, not being listened to, not being given clear explanations, unfamiliar forms of care and overall system inflexibility (Johnstone et al., 2008; Johnstone and Kanitsaki, 2007). The need for an interpreter may create further barriers to communication in terms of accuracy and time required to undertake an assessment, especially when the interpreter is from a different culture or sub-culture. Wider societal factors include perceived discrimination, social isolation, unemployment and lower socioeconomic status (Bhui et al., 2003). Racism is an additional contributor even after adjusting for sociodemographic variables (Bansal et al., 2014; Karlsen et al., 2005) and rates of psychotic disorders (Tortelli et al., 2015).
By contrast, Indigenous patients were not at greater risk of CTO placement even after controlling for sociodemographic variables and rural residence despite the higher rates of involuntary psychiatric admission in this population (Nagel, 2003). The reasons for this are unclear but one possibility is the limited availability of appropriate services to actually administer a CTO in non-urban areas (Kisely et al., 2015).
In terms of outcomes, community orders did not reduce bed-days or admissions in the 12 months following placement in keeping with most non-randomised studies using appropriately matched controls from other countries (Barnett et al., 2018). Of note was that all the studies of outcome came from Australia.
Although we were unable to include the data in a meta-analysis, CTOs may show greater benefit over the longer term. For instance, the NSW study reported that CTOs had no effect on reducing subsequent days in hospital unless patients had been on them for over 2 years (Harris et al., 2019). Two Victorian studies found that CTO cases had fewer bed-days per admission over a decade (Segal and Burgess, 2006a; Segal et al., 2017a), even though the overall number of days was not reduced (Segal and Burgess, 2006a). Other work from the same state suggested that at least five orders were required to significantly reduce readmission rates (Burgess et al., 2006). Given that the maximum period of an order is 12 months (Vine et al., 2019), this could result in several years of CTO placement given that severe mental illnesses are long-term conditions. This is a possibility confirmed by one of the Victorian studies where CTO cases were subject to longer durations of overall compulsory treatment despite reduced inpatient care.
There were two areas where CTOs showed statistically significant benefits over 12 months. One is that CTOs increased community contacts compared to controls, a consistent finding across the literature (Maughan et al., 2014). However, this is strictly speaking a process measure, not an outcome. If CTOs mandate clinic attendance, it is unsurprising that CTOs increase community contacts. The second benefit was a reduced mortality rate, which is in line with similar findings from Great Britain (Barkhuizen et al., 2020). These reductions may be due to closer follow-up in the community given that the benefits at 1- and 2-year follow-up disappeared after adjustment for community contacts following the order (Kisely et al., 2013b). This highlights the importance of close follow-up after discharge from hospital regardless of CTO status, but also raises the question of whether the same degree of supervision could be achieved using less coercive methods.
Limitations
All the included studies were observational designs, and many were of administrative health data, which may be subject to recording bias and lack information on social disability, risk as well as influences on service provision such as homelessness, family supports or substance use. Studies also used proxy indicators of CALD status such as place of birth and preferred language. Similarly, none of the studies distinguished between Aboriginal Australians and Torres Strait Islanders. In addition, we were only able to find one study from New Zealand and this did not compare the use of CTOs in those of Māori and Pākehā backgrounds. Several of the included studies were authored by the lead author of this systematic review. However, study selection and quality appraisal were undertaken by two of the other authors (S.M. and D.Y.).
In terms of outcomes, there were no randomised controlled trials, only cohort and cross-sectional studies. Although these studies matched or adjusted for a wide range of possible confounders, it is still possible that cases and controls differed in other ways which meant the former were more unwell and difficult to engage. This group may therefore have had worse outcomes than if they had not been on an order. However, if the CTO cases were truly more ill in ways for which it was impossible to control, it is puzzling that they also had a lower mortality. Finally, there was no study of outcomes from New Zealand.
The results of our meta-analyses showed a high degree of heterogeneity. We explored this further by excluding each study in turn. As a result, the I2 values were 0% while findings such as the over-representation of those from a CALD background were unchanged. We also tried to accommodate heterogeneity using the random effects model for all our analyses. Nevertheless, our results should be treated with caution. Finally, we were also unable to test for publication bias as none of the outcomes had 10 or more studies.
In conclusion, this study confirms findings from other countries that cast doubt on the effectiveness of CTOs, which is of concern given that their use in both Australia and New Zealand remains high by worldwide standards. In particular, people from CALD backgrounds are more likely to be placed on an order. However, the evidence for effectiveness remains inconclusive and restricted to orders of at least 2 years’ duration. This raises the question as to whether they are a least restrictive option.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Two authors (S.M. and D.Y.) were supported by the University of Queensland’s Summer Scholar Programme for work on this study.