
Abstract
Objective:
Mental health–related calls to emergency services made via 111 (New Zealand) or 000 (Australia) often represent critical junctures for the person in crisis. Traditionally, police, ambulance and mental health services work separately to manage such emergencies. Sequential agency responses may be protracted and cause escalation. This study tests multi-agency co-response aiming for more integrated, faster, safer and less coercive management of mental health crises.
Methods:
Immediate and 1-month outcomes of mental health emergency calls made to police and ambulance were compared according to whether they occurred on days with co-response availability. Outcomes measured included emergency department admission and waiting times, psychiatric admissions, compulsory treatment, use of force, detention in police cells and the time to resolution of the event. Relative risk estimates were constructed.
Results:
A total 1273 eligible mental health emergency callouts occurred between March 2020 and March 2021 (38% coded ‘mental health’ emergencies, 48% suicide risk and 14% as ‘other’), 881 on days with co-response availability and 392 on days without. Co-response interventions were resolved faster and were more likely to be community-based. Fewer than one-third (32%) led to emergency department admissions, compared with close to half (45%) on days without co-response (risk ratio: 0.7 [0.6, 0.8]). In the following month, the number of emergency department and mental health admissions reduced (p < 0.01 and 0.05, respectively). There were no statistically significant differences in use of force and few people were detained in police custody.
Conclusion:
Co-response intervention increased the likelihood of mental health crises being resolved in the community and reduced hospitalisations. Benefits were sustained at 1 month.
Keywords
Introduction
Worldwide and in Australasia, the number of people requesting services for mental health and addiction issues has risen steadily (Associated Society of Medical Specialists, 2021; Jones and Olsen, 2011). In New Zealand, the number of individuals seen for mental health care grew by approximately 40% in the years between 2010/2011 and 2019/2020, putting the health system under considerable pressure (Elliott, 2017; Office of the Health and Disability Commissioner, 2018; Patterson et al., 2018). He Ara Oranga, the 2018 Mental Health and Addiction Inquiry Report commissioned by the New Zealand Government described a consistent theme heard from service users as having to fight for access to mental health care due to high thresholds of acuity, limited and non-existent services, or complex care requirements beyond current service provision. We heard that some people presenting with a high risk of suicide were deemed ineligible for help and were unable to find timely, responsive service …. (Patterson et al., 2018: 54)
Perhaps as a result of this pressure on health services, mental health–related calls to emergency services have also seen steep increases, in line with international trends (Frankham, 2019). This is when police or ambulance services are contacted through an emergency number such as 911 or 000 (111 in New Zealand) to respond urgently to a mental health crisis. Such calls comprise a large – and increasing – proportion of the first responder workload (Godfredson et al., 2011; Hollander et al., 2012). In 2014, New Zealand Police responded to 21,545 emergency calls coded as ‘mental health’ and ‘threatened or attempted suicide’ incidents (Williams, 2019), and in 2020, this had increased to 70,225 events (New Zealand Police, 2021), with an estimated 21% of all police callouts relating to mental health issues (Porter, 2021). Since 2016, mental health emergency calls to Police have increased by 60% with a further 44% increase projected by 2025 (New Zealand Police, 2021).
Having police operate as a de facto mental health crisis service reportedly has negative consequences for service users, staff and providers. Risks include police, ambulance and emergency department (ED) capability being overwhelmed (Australasian College for Emergency Medicine, 2018; Scotcher, 2021); the person experiencing increased distress or (re-)traumatisation, with resulting agitation leading to the overuse of compulsory treatment orders (Meehan et al., 2019), inappropriate detention in police cells (Independent Police Conduct Authority, 2015) and an increase in use of force by police (Morabito et al., 2017; O’Brien et al., 2011). For example, during a 5-month period in 2016, one New Zealand study found police used force, most commonly handcuffs, in 78% of people they attended, who were experiencing a mental health crisis (Holman et al., 2018). First responders often feel ill-equipped to deal with mental health crises and the level of stress reported by police is much higher when attending mental health emergencies than other callouts (Seo et al., 2021).
Typically, police and ambulance services transport people they think require mental health interventions to EDs to await further assessment, sometimes against their will. In recent years, EDs have been experiencing significant problems in accommodating and caring for such presentations. The Australasian College for Emergency Medicine (2018) studied 65 EDs in Australia and 7 in New Zealand, and found that patients attending ED for a mental health crisis routinely experienced unacceptably long waits and this was often detrimental to their mental state. In some cases, patients waited up to 24 hours to access a bed or treatment (Australasian College for Emergency Medicine, 2018, 2019).
A mental health crisis marks a critical juncture, and people’s experiences during this time can colour future engagement with mental services. The status quo response is often disjointed and (re-) traumatising (Sweeney et al., 2018). The New Zealand mental health inquiry, He Ara Oranga, considered that a broader range of mental health and addiction services were required to support people in crisis, suggesting ‘alternative crisis response models such as a co-response model where police, District Health Board mental health services and paramedics jointly attend mental health callouts’ as one such example (Patterson et al., 2018: 115). Prior to this study, this type of ‘tri-service’ crisis response model had not been tested in New Zealand. Internationally, there has been a slowly growing body of evidence indicating that ED presentations and hospital admissions can be averted by co-response models that combine police, paramedic and mental health expertise (Lee et al., 2015; McKenna et al., 2015a; Meehan et al., 2019), although there has been high heterogeneity in the models tested, and a lack of controlled testing.
The Australian ‘PACER’ model (Police, Ambulance, Clinician Early Response) teams a mental health clinician, police officer and paramedic together in a first responder vehicle to attend mental health crises. Such models are operational in several Australian states, including parts of Victoria, Western Australia and New South Wales. PACER outcomes have been evaluated by several studies (Allen Consulting Group, 2012; Furness et al., 2017; Huppert and Griffiths, 2015; Lee et al., 2015; Shapiro et al., 2015; Henry & Rajakaruna, 2018) with generally favourable results. Evaluation findings indicate that the co-response approach may represent a more efficient use of police resources when managing mental health crises than usual practice (Allen Consulting Group, 2012; Lee et al., 2015; Shapiro et al., 2015).
PACER programmes have been positively received by stakeholders (Evangelista et al., 2016; Lee et al., 2015; McKenna et al., 2015b). Furness et al. (2017) found that participants who received the co-response intervention (n = 18) believed their interaction to be more procedurally just than participants who interacted with police only (n = 25), although the number of participants and the difference in raw mean were small (Furness et al., 2017). Similarly, McKenna et al. (2015b) showed that the PACER model brought about a strong partnership between mental health nurses and the police through refining roles, developing knowledge and skills, improving communication and sharing information, with participating staff rating the PACER approach as a significant improvement when compared to business as usual.
Despite favourable qualitative evidence and some quantitative data, the implementation and investigation of co-response teams (CRTs) has also been criticised, with a systematic review finding a lack of robust evidence to evaluate the effectiveness of the co-response model (Puntis et al., 2018).
This study relates to the first CRT test in New Zealand commencing in March 2020. The objective of the study was to see whether a CRT would improve outcomes for service users and reduce demand on EDs and first responders.
Methods
Aim and outcome variables
This study aimed to assess the impact of the CRT on the immediate and 1-month outcomes following mental health–related emergencies. The primary outcome was ED service utilisation. Other outcomes included the time to resolve mental health crises, rates of admissions to hospital, rates of coercive treatment under the Mental Health Act and aversive outcomes for consumers (such as use of force).
The protocol of this study (and an associated qualitative investigation) was determined a priori and is published at http://hdl.handle.net/10523/12704
Study design
A quasi-natural experiment design using linked de-identified data from police and health data sets was chosen as the best method of answering the study question while minimising bias and promoting best ethical practices. A randomised control design was not possible. Namely, it was not thought appropriate to randomise 111 calls, nor were people who were the subject of such emergency calls likely to be able to provide informed consent to participation. Instead we collected de-identified data from all mental health–related emergency calls to Police or Ambulance in the study period between 17 March 2020 and 16 March 2021 (inclusive). Eligibility criteria were mental health 111 calls for service entered in the Police National Intelligence Application (NIA) database (New Zealand Police, 2010) in the Wellington District. The exposure variable was whether the call for assistance was received during a 24-hour period when CRT was available (for some time during that period) or during a 24-hour period when the CRT was not available. These 24-hour periods were termed ‘Day with CRT’ and ‘Day without CRT’. In the protocol, the intent to use an adjacent policing area (without CRT) in the same District as an additional control was signalled, however, shortly after the study commenced, an operational decision was made by Police to extend CRT availability to this area.
The chosen study design was used to reduce the risk of bias from confounding factors. Whether the emergency call centre assigned a call to the CRT was not random but depended on CRT availability (the team was in operation less than one-third of the week) and the features of the call. Even when the CRT was rostered, there was selection bias in which calls they attended, as they were more likely to be involved in complex cases considered likely to require mental health expertise and less likely to be involved in critical Priority 1 calls, which needed an urgent containment. Furthermore, the CRT did not work overnight. Mental health 111 calls made late at night may differ substantively from those made during the day (for example, there may be a higher risk of substance use being involved). If data were analysed according to the intervention received, bias would be introduced because of the uneven distribution of clinical variables acting as confounding features (i.e. if the CRT was selectively deployed to calls considered likely to require compulsory treatment, then CRT intervention would be associated with compulsory treatment). Hence, we analysed data from all callouts received over 24-hour periods when there was some CRT availability (‘Days with CRT’) compared with data from all callouts received over 24-hour periods when there was no CRT availability (‘Days without CRT’).
Data were extracted separately by New Zealand Police analysts and health analysts from Police and Health databases, respectively, and then supplied to SEP, SK and AK linked only by a secure keycode with identifying information (e.g. name, address, date of birth, unique health identifier) removed. Police data sources provided information on calls for service, response and duration times, priority coding and outcome. From the health data sources, mental health and ED outcome data were extracted including demographic data (age, gender and ethnicity), legal status and type, outcome of assessment and follow-up action. These data were extracted from electronic health records using a data extraction tool constructed a priori. As only nine cases (0.3%) could not be linked across the Police and Health databases, these cases were excluded from the analysis.
Ethics approval
The Health and Disability Ethics Committee (Northern region) granted ethics approval, reference 20/NTB/98. Locality approval was obtained from the relevant Police and health services. Māori consultation was undertaken with the Ngāi Tahu Research Committee.
Description of the intervention and comparator models of care
The co-response model of care
When a Police or Ambulance Communications Centre received a 111 call about a mental health emergency, the operator would decide if it was related to general mental health or suicide risk and, if appropriate, would assign the callout to the CRT.
The CRT consisted of a multidisciplinary team with staff members working approximately four 10-hour shifts a week (generally 0830 till 1830 hours) in an urban centre. When the team was operational, three staff (one uniformed police officer, one uniformed paramedic and one plain clothes mental health clinician) would form an ‘away’ unit, available to attend mental health crisis calls in the field. Two other staff (a mental health clinician and police officer) acted as a ‘home’ liaison team, remaining at base to search records, collate information, provide advice and make referrals. Each CRT member had access to their respective service’s records, e.g. the mental health clinician accessed past health documentation. Mental health emergency calls were triaged by police and paramedic 111 communications centre. When dispatched, the CRT used the respective skills of the three professions to contain the scene and manage any acute risks, assess physical health needs and undertake mental health assessment. They would then formulate a management plan, involving the person and their family in decision-making wherever possible. Sometimes the emergency could be resolved on site and sometimes the person required transport to another location such as a community mental health base for further intervention. The CRT were unable to admit directly to the acute inpatient ward, so if they thought the person needed further assessment by a mental health crisis team and/or admission to hospital, they would transport them to ED. If the person remained at home, management plans might include follow-up by their General Practice (GP), a community mental health team, a counsellor or the crisis team.
The ‘business as usual’ model of care
In the conventional response when there was no CRT, the Police Communications Center would assign mental health–related emergency to a police dispatcher. The dispatcher would determine the urgency of the response and select an available police unit in the area. The assigned police officers would be given the name, address and details of the incident. On arrival at the scene, the attending officers might re-contact the Communications Centre to request further support, such as the provision of an ambulance. In this response, the police responders had access to past police records but not to mental health records, and were unlikely to know whether the person was a client of mental health services. If the distressed person needed further mental health assessment, they would usually be transported to the ED. This could occur voluntarily or involuntarily using police powers enabled by mental health legislation. If the person was aggressive, they might be taken to the police cells to await further assessment there – sometimes involving the use of force such as handcuffs or restraint.
Data analysis
The events were first described using summary statistics. This included mean (M) and standard deviation (SD) for numeric variables and the number (n) and percentage (%) of events per category for categorical variables. The between-group difference in mean was assessed using Welch’s unequal variances t test for numeric variables. Non-parametric Kruskal–Wallis signed rank sum tests were also performed to check the results in the case of non-symmetrical distributions. For categorical variables, chi-square tests were conducted to test whether the distributions were the same for the two groups. The results were checked using Fisher’s exact test.
Relative risk estimates for key outcome variables were used to analyse the impact of the intervention. The risk estimates summarise the difference in outcomes for days without CRT to days with CRT. For numeric variables, risk difference in mean was analysed using a normal distribution approximation. Rate ratios for count variables were first analysed using the negative binomial distribution, then replicated using a Poisson distribution. Risk ratios (RRs) for categorical variables were computed using the binomial distribution with a natural log link function. To ensure the validity of distributional assumptions, bootstrap samples from empirical distributions were used to corroborate all results. All bootstrap analyses were based on 100,000 simulation runs.
Finally, sensitivity analyses were performed to ensure that differences between weekday and weekend presentations and the differential coding of events were not acting as confounding variable results.
Results
Allocation to comparison groups
Between 17 March 2020 and 16 March 2021, there were 207 days with CRT availability and 158 days with no CRT availability. In total, 1273 mental health–related callouts met the criteria in the catchment area over the study period. These presentations are summarised in Table 1. Overall, 38% of calls were coded by the operators as mental health emergencies (1M), 48% were coded as suicide risk (1X) and 14% were coded as ‘other’ mental health. The dispatching agency was New Zealand Police for 87.5% of cases and ambulance for 12.5%.
Clinical and demographic information of service users and intervention received.
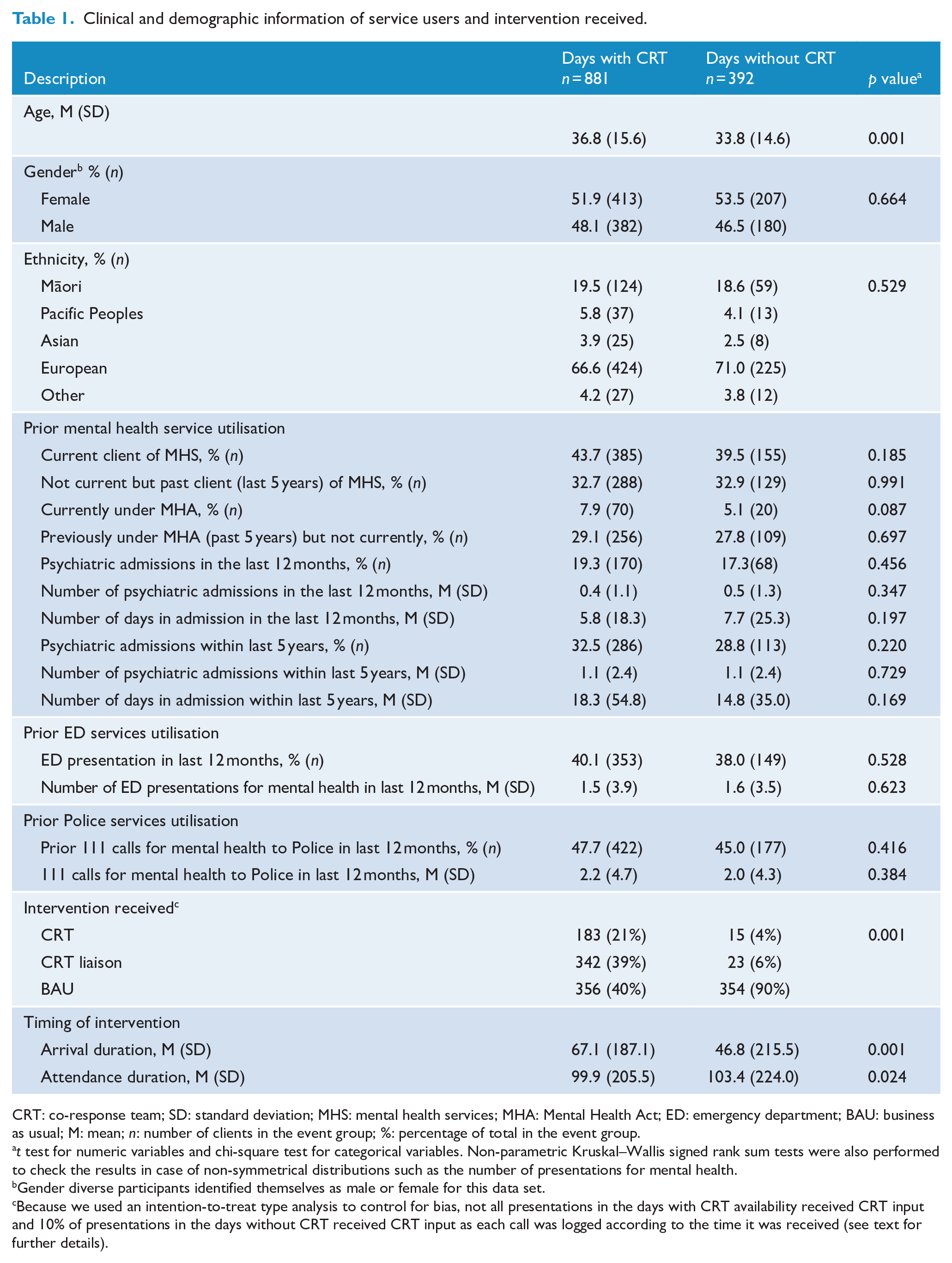
CRT: co-response team; SD: standard deviation; MHS: mental health services; MHA: Mental Health Act; ED: emergency department; BAU: business as usual; M: mean; n: number of clients in the event group; %: percentage of total in the event group.
t test for numeric variables and chi-square test for categorical variables. Non-parametric Kruskal–Wallis signed rank sum tests were also performed to check the results in case of non-symmetrical distributions such as the number of presentations for mental health.
Gender diverse participants identified themselves as male or female for this data set.
Because we used an intention-to-treat type analysis to control for bias, not all presentations in the days with CRT availability received CRT input and 10% of presentations in the days without CRT received CRT input as each call was logged according to the time it was received (see text for further details).
Presentations received one of three responses. If someone was assessed face to face by the CRT team, this was coded as a ‘CRT’ response. If the CRT did not attend in person but provided guidance to the deployed police officers or paramedics, this was coded as a ‘CRT liaison’ response. If a mental health crisis call did not receive any input from the CRT, this was coded as a ‘BAU’ response (business as usual).
During the days with CRT, 881 mental health–related callouts were recorded. Of these calls, 356 received a BAU response, while CRT and CRT-liaison attended 183 and 342 calls, respectively. In total, the CRT were involved in 60% of these callouts.
During days without CRT, 392 mental health–related callouts were recorded. Of these calls, 354 received a BAU response, while a further 15 and 23 calls were provided with CRT and CRT-liaison services. On first glance, this may not make sense – how could someone be seen by the CRT when the CRT was not available? The reason for this is that each call was coded according to the time it was logged. If a call came in overnight during a 24-hour period when the CRT was not available, it was coded to a day without CRT. However, the call may not have been allocated until the start of the next working day, at which time a CRT shift started and the CRT became involved.
Baseline demographics
The patterning of gender and ethnicity was similar across groups but people presenting on the days with CRT were older, with a mean age of 36.8 years compared to 33.8 years, a difference that was statistically significant.
In terms of prior service utilisation, there were no significant differences between people who presented on CRT available days compared to other days. This suggests that clinical risk factors were distributed fairly evenly across groups.
The majority (62.9%) of people assessed by the CRT were seen at their own homes. The CRT liaised with and referred to a variety of agencies, most commonly mental health services. They also arranged GP follow-up or services through other agencies such as Work and Income New Zealand (WINZ), the government agency for social welfare. Most CRT callouts resulted in the person remaining in the community. Referrals to the crisis resolution service, community mental health teams, GPs, WINZ, NGOs and student health services were made for approximately 75% of callouts. Clinical outcomes within 24 hours for each group are summarised in Table 2.
Clinical outcomes within 24 hours following the mental health crisis call.
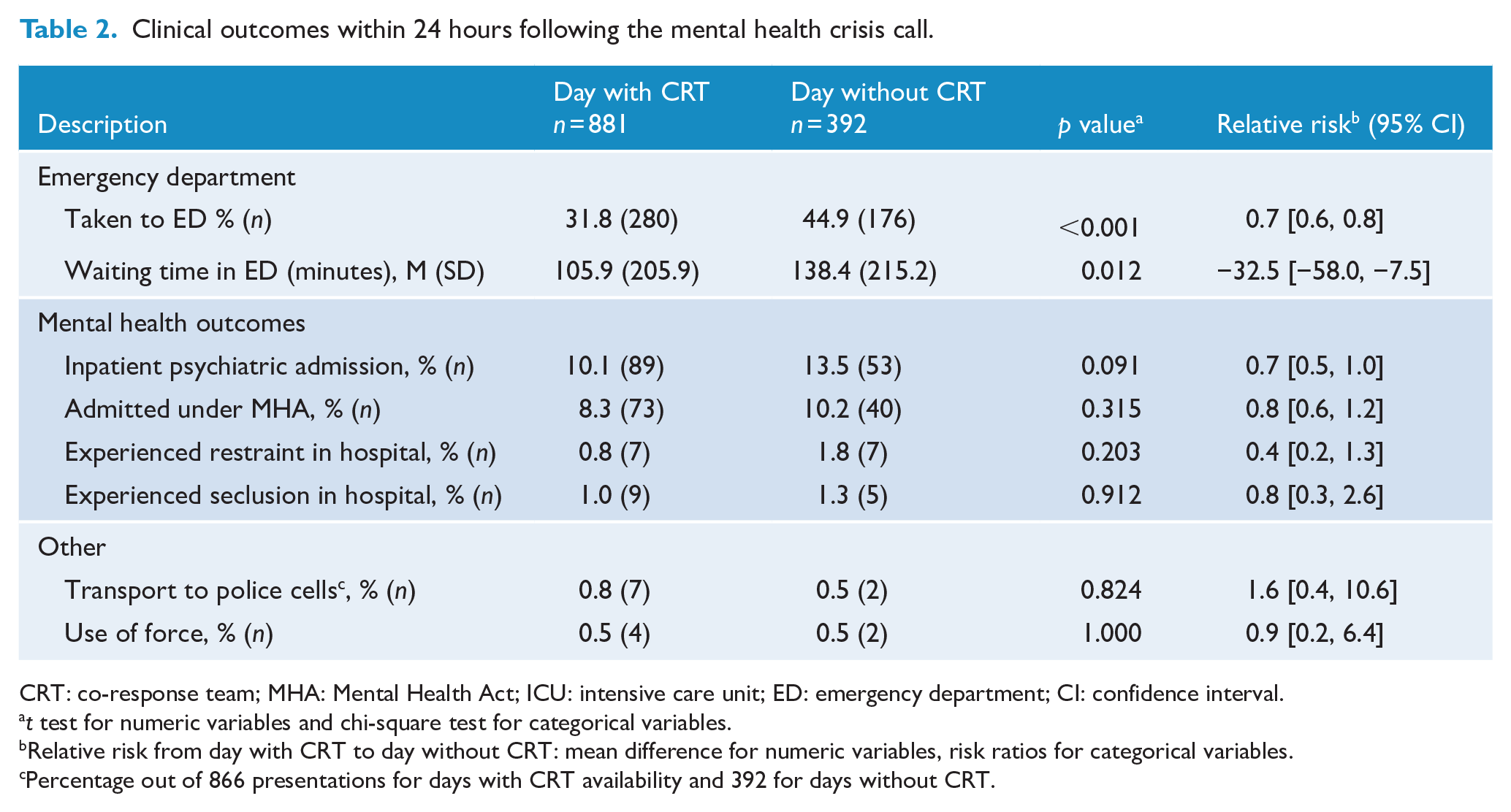
CRT: co-response team; MHA: Mental Health Act; ICU: intensive care unit; ED: emergency department; CI: confidence interval.
t test for numeric variables and chi-square test for categorical variables.
Relative risk from day with CRT to day without CRT: mean difference for numeric variables, risk ratios for categorical variables.
Percentage out of 866 presentations for days with CRT availability and 392 for days without CRT.
Callout duration
The overall average callout duration on days with CRT – shown as attendance duration in Table 1 – was 4 minutes less than on the days when there was no CRT, suggesting mental health–related emergency calls could be resolved faster.
ED utilisation
CRT availability was associated with a significant reduction in the ED utilisation (Figure 1). During days with CRT availability, fewer than one-third of service users (32%) were taken to the ED, compared with almost half of service users on days without CRT (45%). The relative risk for an ED presentation on Days with CRT was 0.7 (95% confidence interval [CI] = [0.6, 0.8]), meaning a 30% reduction in the probability of attending ED. On average, service users waited in the ED for 32.5 fewer minutes on days with CRT. This may have contributed to the shorter attendance duration during days with CRT – police officers may have spent less time waiting with service users on days with CRT.
Emergency department service utilisation.
Psychiatric admissions
On days the CRT was available, 10.1% of calls resulted in the service user being admitted to a psychiatric unit. This was similar to the 13.5% of people admitted on the days that CRT was not available. Compulsory admission under the Mental Health Act occurred for 8.3% of people seen on days with CRT compared with 10.2% of people on days without CRT. The service user experiences during the psychiatric admissions are illustrated in Figure 2. Overall, there was a non-significant trend towards lower admission rates and less coercive treatment in the 24 hours following the mental health–related emergency call.
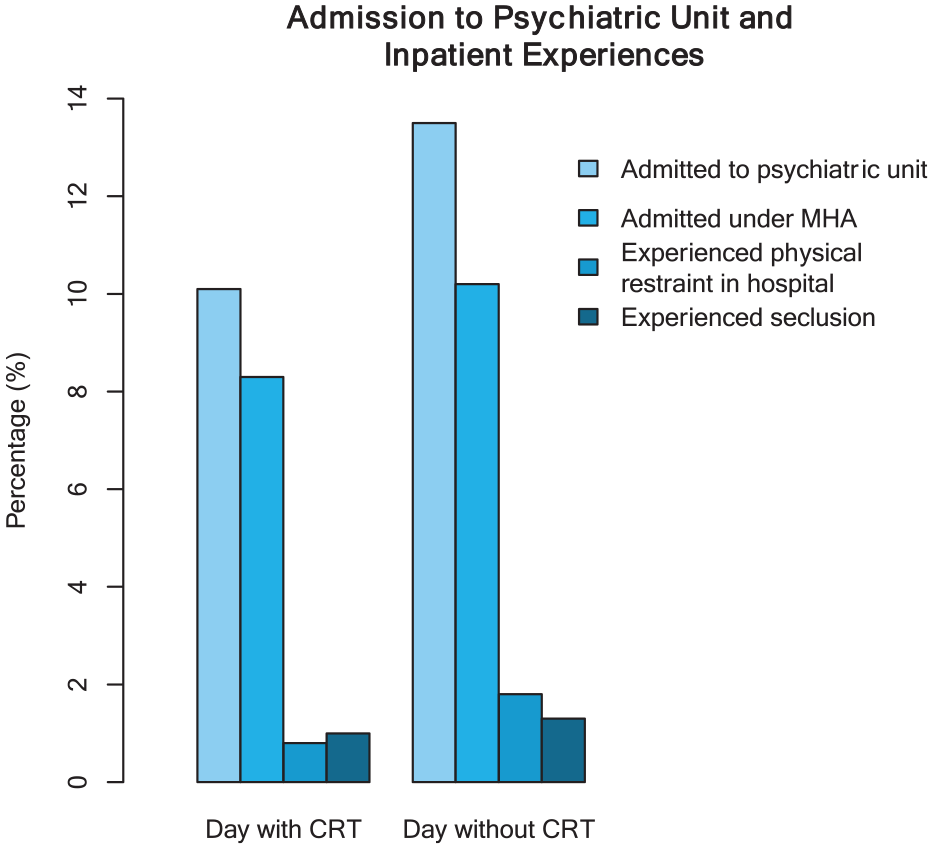
Experiences related to psychiatric admission on days with CRT versus days without CRT.
Other outcomes
The differences in other service utilisations were also checked between groups. There were no significant differences in rates of mental health respite care (2.6% across groups), medical admission (10.1% across groups) or intensive care unit (ICU) admission (0.5%). There was one death as a result of a suicide on a day with CRT. This occurred before the arrival of dispatch team at the scene.
Use of force and time in police cells
Physical or mechanical restraint or other tactical options were used by police when they considered the service user was presenting a serious and immediate risk to self, others or to staff. These instances were recorded by each police officer attending the callout. In New Zealand, mental health legislation provides that police can transport a ‘person appearing to be mentally disordered’ to an ‘appropriate place’ including a police station, where they can be held for up to 6 hours while psychiatric assessment is arranged. A health facility is generally considered to be the appropriate destination, but occasionally when a person is perceived to be behaving in a particularly challenging way, the police may elect to transfer them to police cells to wait assessment. In total, 19 service users were transported to police cells during the study period. All but one of these transports (18/19) occurred following the BAU responses. Only one of these service users was charged with an offence, the others being civilly detained for the purpose of psychiatric assessment. The estimated risk of being transported to police cells for BAU to CRT responses was 10 to 1 indicating that CRT input reduced the time that mentally disordered people spent in police custody.
Similarly, there were only 13 use of force events recorded for mental health–related calls across the district. These recorded events do not include incidents where only handcuffs were used, as handcuffs without the use of pain compliance or without use of an additional tactical option are not a reportable use of force. In six cases, the reason documented was violence towards first responders, in five it was to prevent immediate self-harm risk and in the other two it was threatened violence. The BAU dispatch team attended 53.8% of these cases indicating a similar RR between BAU and CRT responses.
Clinical outcomes 4 weeks after the event
The long-term effects of CRT involvement were analysed in terms of presentations to the ED along with other service utilisation outcomes. All events were followed up 1 month (30 days) after the initial attendance and the results are summarised in Table 3.
Clinical outcomes in the 4 weeks following the mental health crisis call.
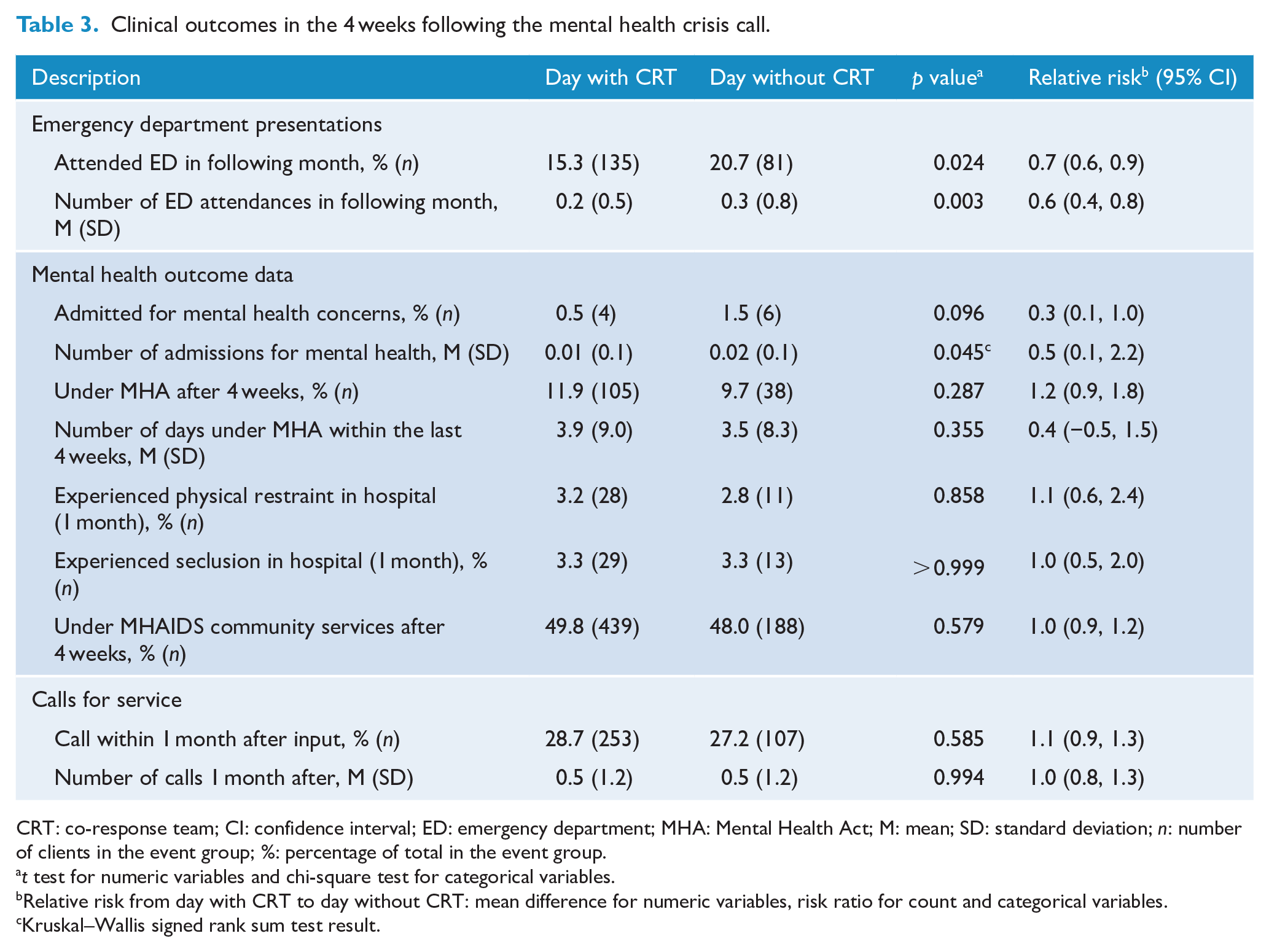
CRT: co-response team; CI: confidence interval; ED: emergency department; MHA: Mental Health Act; M: mean; SD: standard deviation; n: number of clients in the event group; %: percentage of total in the event group.
t test for numeric variables and chi-square test for categorical variables.
Relative risk from day with CRT to day without CRT: mean difference for numeric variables, risk ratio for count and categorical variables.
Kruskal–Wallis signed rank sum test result.
People who presented on days with CRT were less likely to attend ED within the 1-month follow-up period, with an RR estimate of 0.74 (95% CI = [0.58, 0.94]). Correspondingly, the average number of ED presentations in that 1-month period was also lower for days with CRT with an RR estimate of 0.59 (95% CI = [0.44, 0.80]) obtained using a negative binomial distribution. The risk of being admitted to a psychiatric unit was also lower for people who had presented on days with CRT, but these numbers were small.
There were no significant differences in coercive practices such as the rates of people experiencing seclusion or restraint in hospital, or in utilisation of compulsory treatment. Just over 25% of service users were the subject of repeated mental health–related 111 callouts in the following month – a proportion similar in both groups. There had been no deaths in either of the groups at 1-month follow-up.
Sensitivity analyses
Due to rostering issues, a higher proportion of days with CRT occurred during the week than over the weekend. To check that this was not confounding results, subgroup analysis was repeated comparing only data collected from Monday to Friday. As expected, this reduced the number of observations (to n = 842 for days with CRT and n = 204 for days without CRT) hence reducing the power of tests performed. However, the outcomes were consistent with the findings of the main analysis including the reduction in the number of ED presentations 1 month following the callout (RR: 0.67, 95% CI = [0.46, 0.98]).
On the days with CRT, more types of events were coded ‘Other’ compared to the days without CRT. In the consultation with the agencies involved, it was identified that this was due to different event selection criteria applied by the CRT (i.e. the CRT were probably more nuanced in their coding), whereas other teams tended to code everything as 1M (mental health) or 1X (threatened/attempted suicide). Subgroup analysis was repeated excluding the ‘Other’ events. The results from this analysis (n = 705 for days with CRT and n = 381 for days without CRT) again found all effects were consistent with the main analysis including the ED outcomes, for example, giving an RR of 0.78 (0.68, 0.91) for ED presentations within 24 hours and RR of 0.76 (0.59, 0.98) for the 1-month follow-up.
Discussion
Summary of findings
This study suggests benefits of the CRT including reduced ED utilisation, with a substantial effect size. During days with CRT, fewer than one-third of service users (32%) went to the ED, compared with close to half of service users on days the CRT was not available (45%). On average, service users waited in the ED for 32.5 fewer minutes on CRT available days. People who presented on the days with CRT were also less likely to attend ED within the 1-month follow-up period, with an RR estimate of 0.74. The risk of being admitted to a psychiatric unit may also have been lower for people who presented on days with CRT, but these numbers were small, and the trends did not reach significance.
The average attendance duration on a day with CRT was shorter by 4 minutes compared to a day without CRT. This may be because the CRT was able to manage time-consuming Mental Health Act processes more efficiently, or perhaps CRT liaison enabled the re-direction of distressed service users back to their mental health care team.
These findings align with previous observational studies and evaluations, particularly of the PACER model in Australia, which suggest that co-response may represent a more efficient use of resources than previous practice in the management of mental health crises (Allen Consulting Group, 2012; Lee et al., 2015; Shapiro et al., 2015) and provide better processes and outcomes for stakeholders (Furness et al., 2017; McKenna et al., 2015a).
Limitations
The intention-to-treat data analysis, with participants being compared according to whether they presented on a day with some CRT availability as opposed to whether they actually received CRT input was a conservative approach, which may underestimate the effects of the CRT. The CRT never worked more than 10 hours in a 24-hour period and during days with CRT, fewer than two-thirds of service users had CRT contact. However, this approach increases the confidence that any differences seen between the two groups are true treatment effects rather than arising from a third variable.
There may be some discrepant measurement bias across the CRT and BAU data sets that may also contribute to an underestimation of effects. While the CRT data were fully captured through a combination of the Communications and Resource Deployment System (CARD) and manual CRT log data, there were some challenges in identifying relevant events in the BAU data set. BAU events were limited to those events for which there was a corresponding NIA occurrence. The presence of an NIA occurrence provided identifying information about the subject of the event, required for linking New Zealand Police and Health data, and identifying multiple calls for service by the same individuals within the New Zealand Police data set. This may have led to under-reporting of some of the negative outcomes for the BAU data set, resulting in under-estimation of the true benefit of the CRT. Furthermore, some variables that we intended to compare, such as the use of manual restraints, were not well captured within the New Zealand Police data sets. There were also a small number of cases that could not be linked across the New Zealand Police and health data sets.
We were unable to analyse by ethnicity as intended as there was too much missing data and measurement bias. There was no ethnicity data recorded for 23% of the calls, and the accuracy of the ethnicity data that were recorded is unclear.
The COVID-19 pandemic affected the number of participants in the study because 111 calls reduced during level 4 and level 3 lockdowns (March–May 2020). The overall reduction in calls for service resulted in the study being not as well-powered as anticipated. This meant that we did not identify significant differences in the lower frequency events, such as arrests, the use of force and seclusion or restraint, as the counts were few.
It is difficult to directly compare our results with other co-response models due to heterogeneity in the models of care and study design.
Recommendations for future research
The results of this comparative study suggest that the CRT services can provide short- and medium-term benefits for service users requiring emergency services for mental distress. These findings were strengthened by the assignment of service users into groups based on the CRT shift hours, which resulted in a balanced distribution across various demographic backgrounds and clinical histories. The 24-hour shift units were necessary to help achieve this balance. Moreover, the study period included nationwide lockdown periods introduced in response to the COVID-19 pandemic. All types of ED presentations were lower during these lockdown periods. The results presented are, therefore, likely to be conservative estimates of CRT benefits. The results of sensitivity analyses were consistent with the findings from the main analysis, which provides added assurance that the improved outcomes are likely to be the result of study intervention rather than due to chance.
Despite the comprehensive volume and range of results reported here, a long-term analysis would be important, as well as the results of implementation in other regions across New Zealand. This would help to ascertain whether the benefits are sustained over a longer period and would provide a larger study size to examine the low-base-rate outcomes, which this study was not sufficiently powered to investigate, such as suicide and the use of force and seclusion.
This study presents the de-identified quantitative outcomes demonstrating effectiveness. However, it is important that the experiences of stakeholders are canvassed, particularly service users and their family. In a companion study, we have conducted qualitative interviews with over 50 key stakeholders including CRT service users, their family, partner agencies, CRT staff and managers. Participants expressed high levels of satisfaction with the CRT, viewing it as safe, able to provide timely expert advice and providing person-centred care that reduced the risk of violence and coercive interventions. The overwhelming majority of participants interviewed (89.4%, n = 42) expressed a high degree of satisfaction with the CRT, rating themselves as ‘extremely satisfied’ or ‘very satisfied’.
Conclusion
Traditionally, police, mental health and ambulance services have worked separately managing mental health crises. This study tested a co-response with staff from each of these services cooperating to manage mental health–related 111 callouts. The research targeted a hard-to-reach population and investigated a culturally responsive and client-centred intervention using a quasi-natural experimental design. The multi-agency joint response had clear benefits in increasing the likelihood of mental health crises being resolved in the community and reducing hospitalisations, ED response time and repeat presentations. The CRT intervention involved joint decision-making and multi-agency collaboration, which can help first responders provide more integrated and nuanced responses to emergency callouts involving mental health crises.
Although it is difficult to generalise these findings without replicating the study in other populations and geographic locations, the effectiveness of CRT intervention in our study population and the results from other similar models cautiously suggest that co-response be considered a better service model for those experiencing mental health emergencies.
Footnotes
Acknowledgements
We thank Director Simon Williams and Inspector Simon Welsh of the Evidence-Based Police Centre and the staff from the Police National Headquarters, particularly Inspector Brett Callander, Dr Melissa Smith, Ms Meredith Cole and Ms Nicole Martin-Lupp, for supporting the study. We also thank the three agencies who sponsored the CRT intervention: Wellington Mental Health Services (MHAIDS 3DHB), Wellington Free Ambulance (WFA), the Wellington District Police, and the CRT team lead by Senior Sergeant Matthew Morris. The study could not have occurred without the input of policy analyst, Steve McGinnity, who extracted the de-identified health data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The intervention was funded by New Zealand Police, Wellington Free Ambulance and The Mental Health, Addictions and Intellectual Disability Services 3DHB. This independent research was funded by the New Zealand Police.