
Abstract
Objective:
Indigenous suicide prevention is an important focus for national health policies. Indigenous suicide rates in formerly colonial English-speaking countries such as the United States, Australia and New Zealand are considerably higher than the general population, particularly in young males. Given the similarities in their sociocultural history, a time series analysis was conducted to assess recent sex and age trends of suicide in the Indigenous and general populations in the United States, Australia and New Zealand.
Methods:
Using the number of deaths by intentional self-harm and estimated resident population, suicide incidence rates were calculated for the years 2006–2019 and stratified by Indigenous status, year, time period, sex and age group (above 15 years). Incidence rates were plotted. Using the Poisson regression model, calculated suicide incidence rate ratios were used to make comparisons for sex and age.
Results:
Across all countries studied, Indigenous suicide rates have increased over time, with Indigenous males having higher suicide rates than Indigenous females. However, the increase in Indigenous female suicides was greater than that for Indigenous males in Australia and New Zealand. Indigenous males aged 15–44 years have the highest suicide rates across all countries.
Conclusion:
Indigenous suicide rates have remained consistently high in the United States, Australia and New Zealand, with Indigenous males aged 15–44 years showing the highest rate. However, suicide rates for Indigenous females in Australia and New Zealand are increasing more rapidly than males. Given this, it is critical that further research is dedicated to understanding and addressing the issues driving this problem, particularly in youth.
Introduction
Suicide is a major contributor to premature mortality with more than 800,000 deaths globally each year (Bilsen, 2018). While Indigenous suicide rates vary around the world (from 0 to 188 deaths per 100,000 population), formerly colonial English-speaking countries such as the United States, Australia and New Zealand (NZ) have high rates of Indigenous suicide, with younger males being at particularly high risk (Pollock et al., 2018). Indigenous organisations have advocated for national policies specifically addressing youth suicide, and NZ has acted in this area (Cousins, 2017; Hatcher, 2016; Pollock et al., 2018; Ridani et al., 2014; Wexler and Gone, 2012). There is an ongoing need to monitor the outcomes of Indigenous suicide prevention programmes.
The initial effects of colonisation on Indigenous suicidality are extremely challenging to assess as death records lacked Indigenous identification in earlier periods (Hirini and Collings, 2005; Hunter and Harvey, 2002; United States Census Bureau, 2021). Accordingly, the differences in when the suicide rate rises started may be partly attributable to differences in when the death records in each country began Indigenous identification. However, previous studies have demonstrated that US Indigenous suicide rates have been rising since the 1950s, with youth suicide rates almost quadrupling from 1950 to 1980 (Strickland, 1997). This may be partly accounted for by the establishment of the Indian Adoption Project in 1958 (Substance Abuse and Mental Health Services Administration (SAMHSA), 2018). In Australia, the suicide rate for Indigenous Australians was 17.0 per 100,000 compared to 13.3 per 100,000 for their non-Indigenous counterparts from 1988 to 1998 (Hunter and Milroy, 2006), with more significant disparity in suicide rates since this time period (i.e. 23.7 per 100,000 for Indigenous Australians compared to 12.3 per 100,00 for their non-Indigenous counterparts between 2014 and 2018) (Australian Bureau of Statistics [ABS], 2019). Similarly, in NZ from 1985, suicide rates for Māori males aged 15–24 years began to exceed than those of non-Māori non-Pacific males (Drummond, 1997; Hirini and Collings, 2005). The combined effects of continuing colonisation and rapid social change are thought to have conferred further risks to young Māori males who were already susceptible to suicide (Hirini and Collings, 2005). In contrast, Māori female suicide rates remained relatively stable from 1970 to 1990, with increases noted towards the end of this observation period. The progressive escalation of suicide rates among Indigenous people in recent years is probably attributable to a complex interplay of factors and precipitants, and there is good reason for continued investigation of how best to take preventive action.
The current study investigates national suicide rates from the early 2000s, analysing and contrasting Indigenous and total populations in the United States, Australia and NZ. We compare the suicide trends over time and assess and compare changes in sex and age patterns of Indigenous suicide in the different populations across the three countries.
Methods
We analysed suicide rates for the United States, Australia and NZ between the years 2006 and 2019 for residents aged above 15 years, using all data being available for this period. Confirmed number of deaths by intentional self-harm and estimated resident population (ERP) were collected for each country. Data for the United States were obtained from the Centres for Disease Control and Prevention (CDC) WONDER 1999–2019: Underlying Cause of Death by Bridged-Race Categories database. Data were collected for the general and Indigenous (i.e. American Indian or Alaskan Native with no Hispanic or Latino origin) US populations, stratified by sex and age groups. Deaths by intentional self-harm were identified using the International Classification of Diseases, 10th Revision (ICD-10) codes X60-X84 and Y87.0.
Australian data were obtained via a custom request to the ABS. Deaths were identified using the ICD-10 codes X60-X84 and Y87.0, and are reported for New South Wales, Queensland, South Australia, Western Australia and the Northern Territory only. This is because, as per the ABS, only these five states and territories have evidence of sufficient levels of Indigenous identification and numbers of deaths to support mortality analysis. The ERPs for the relevant groups were based on the results of the 2016 Census of Population and Housing, with figures for the Indigenous population adjusted for net undercount as measured by the Post-Enumeration Survey (ABS, 2018).
Statistics New Zealand was used to attain the ERPs. A number of suicide deaths in NZ stratified by Indigenous status, sex and age groups were obtained from the Ministry of Health. NZ uses the ICD-10 codes X60-72 and X74-X84, omitting X73 and Y87.0 (Ministry of Health, 2019). This is because X73 is considered invalid for mortality coding in NZ. Furthermore, as only a small number of deaths fall under the Y87.0 code, it is not expected to significantly impact the overall figure (C Lewis, 15 September 2021, personal communication).
Based on Indigenous status, sex and age group, the suicide incidence rates (IRs) were calculated by taking the number of deaths by intentional self-harm divided by the ERP for each group. ERPs aged above 15 years were considered as the denominator to calculate the suicide rates. The rates were then plotted over time according to the year, time period, Indigenous status, sex and age group. A Poisson regression model was applied to examine the suicide rates between groups. The suicides were treated as count data – the rate of suicides for respective denominator. To reduce the confounding bias, models were adjusted by age and era. The estimates were calculated using the likelihood ratio method and were expressed as incidence rate ratios (IRRs) from the Poisson model. The two-sided test was performed for all analyses, and 95% confidence intervals (CIs) and p values were reported. All statistical analyses were conducted using R version 4.1.0 and Stata version 16.1.
Results
Between 2006 and 2019, total population suicide rates (including Indigenous population) for both sexes have increased significantly in Australia and the United States but remained relatively stable in NZ (Figure 1). In all countries, all-race male suicide rates remain significantly higher than all-race female rates (Figure 1).
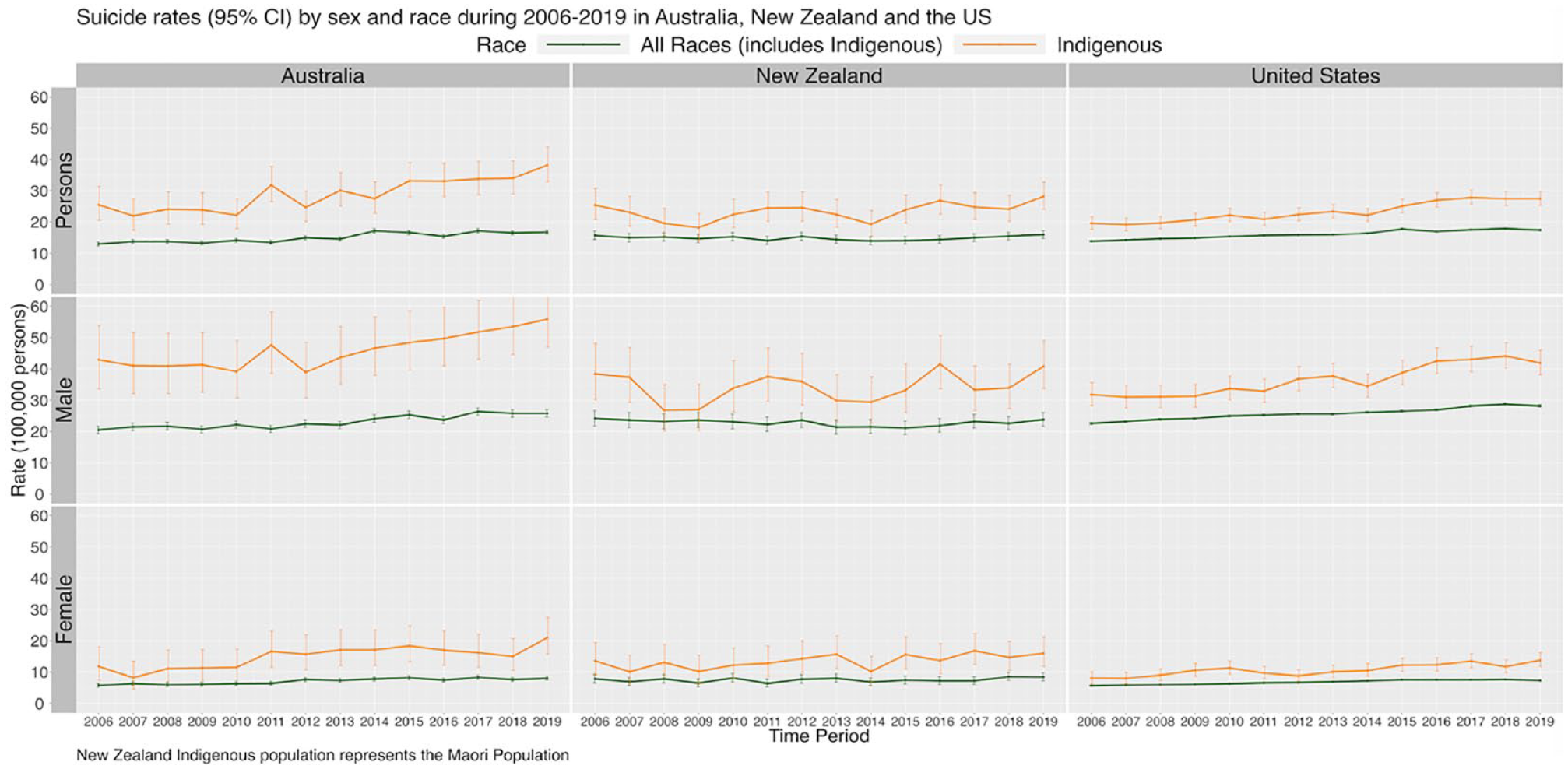
Suicide rates by sex and race during 2006–2019 in Australia, New Zealand and the United States.
Of the Indigenous populations, Australia has the highest suicide rates (Figure 1) compared to the US and NZ. Despite some fluctuation, Indigenous suicide rates for all countries and sexes showed significant increases between 2006 and 2019 (Figure 1 and Table 1). The largest increases occurred in the US (IRR = 1.15, 95% CI = [1.09, 1.22], p < 0.001) in 2011–2015 and (IRR = 1.42, 95% CI = [1.33, 1.50], p < 0.001) in 2016–2019, while NZ showed the least change (IRR = 1.09, 95% CI = [0.96, 1.23], p = 0.19) in 2011–2015 and (IRR = 1.26, 95% CI = [1.11, 1.42], p < 0.001) in 2016–2019 (Table 1). Indigenous males have higher suicide rates than Indigenous females (Table 2), but the increase in female suicide rates relative to Indigenous males was greater in Australia and NZ (Table 1). In the United States, increases in Indigenous suicide rates were largely proportionate between Indigenous males and females (Table 1).
Suicide rate ratios in the Indigenous population by sex and era in Australia, New Zealand and United States during 2006–2019 adjusted by age.
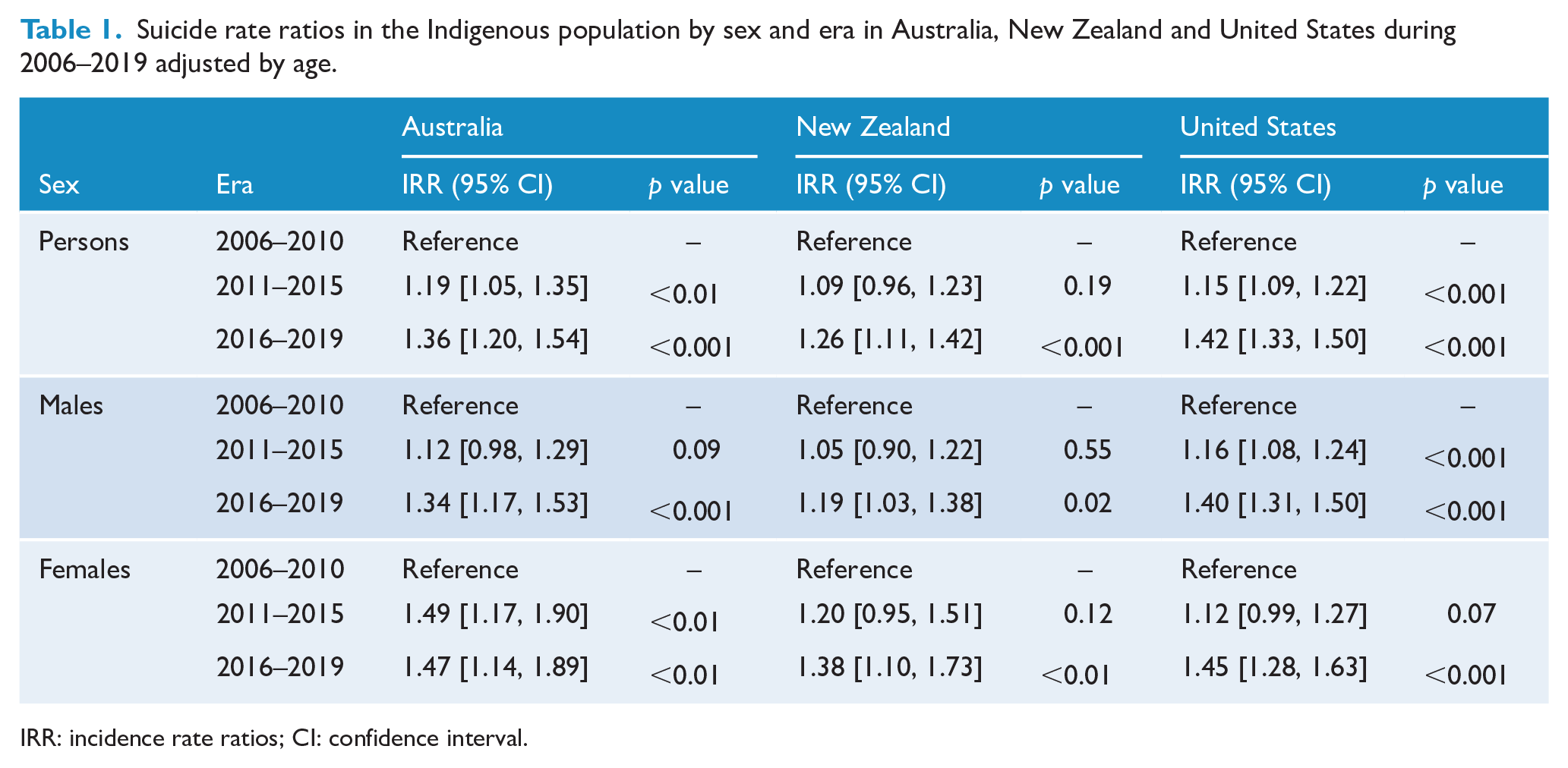
IRR: incidence rate ratios; CI: confidence interval.
Age-specific suicide rates and rate ratios in the Indigenous population by sex in Australia, New Zealand and United States during 2006–2019 adjusted by era.
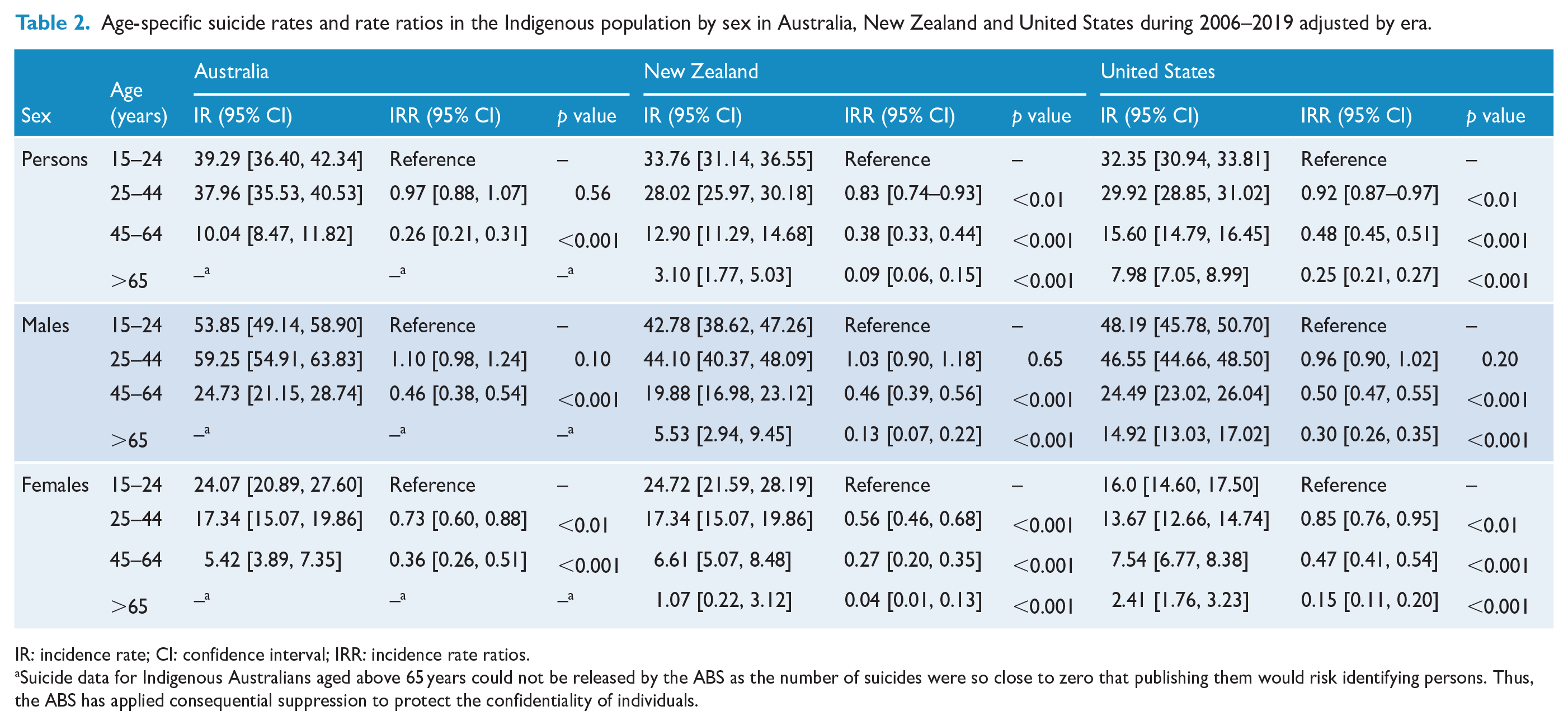
IR: incidence rate; CI: confidence interval; IRR: incidence rate ratios.
Suicide data for Indigenous Australians aged above 65 years could not be released by the ABS as the number of suicides were so close to zero that publishing them would risk identifying persons. Thus, the ABS has applied consequential suppression to protect the confidentiality of individuals.
Australia has the highest Indigenous suicide rates for people aged 15–44 years (IR = 39.29 in those aged 15–24 years; IR = 37.96 in those aged 25–44 years) (Table 2). In all countries, total Indigenous suicide rates are highest in those aged 15–24 years (IR = 39.29 in Australia; IR = 33.76 in NZ; IR = 32.35 in the US); this suicide rate decreases significantly with increasing age (Table 2). This trend is also observed for all Indigenous females and Indigenous US males (Table 2). Indigenous males aged 25–44 years have the greatest suicide rates in Australia and NZ (Table 2). In all countries, the suicide rate for those aged 15–44 years is more than double of those aged 45 years and above (Table 2).
Discussion
Total population and Indigenous suicide rates have significantly increased over time in the US and Australia. In NZ, Indigenous suicide rates have risen while total population suicide rates have remained largely stable.
Male suicide rates, regardless of Indigenous status, have consistently been higher than female rates in all countries during the reporting period. Indigenous males aged 15–44 years are most at risk for suicide in all countries studied. Young Indigenous males are susceptible to multiple risk factors that heighten their suicide risk, including high incarceration rates, risk-taking behaviour and alcohol and substance misuse (Armstrong et al., 2017). These, when combined with existing suicidal thoughts, are likely to increase suicide risk, especially considering that youth suicides are often impulsive and linked to supposedly minor situational triggers (Armstrong et al., 2017).
Policy and programme implications
In NZ, formal processes exist to include Māori at the government and community level. These include incorporation of the principles of the Treaty of Waitangi through the Waitangi Tribunal; evidence of consultation with Māori on grant applications; requirements for health professionals to understand the relevance of the Treaty of Waitangi; having Māori representation on interview panels and use of Māori in conversation (Hatcher, 2016). Māori also constitute a larger proportion (17%) of the NZ total population, than Indigenous people in Australia (3%) and the United States (2%) (Australian Institute of Health and Welfare [AIHW], 2021; IWGIA, 2022; Statistics New Zealand, 2021). Lack of political representation and thus action to implement and maintain social infrastructure in the United States and Australia may partially account for increasing Indigenous suicide rates (Dudgeon and Holland, 2018; US Department of Health and Human Services, 2010). In the context of having a larger Indigenous proportion of population, NZ Indigenous groups may have more powerful advocacy and opportunities for consultation, which could result in less discrimination and more adequate resources to improve socioeconomic conditions. Of particular concern is the Australian Indigenous population, whose suicide rates are higher than the United States and NZ.
Suicide interventions which assist Indigenous people are often adaptations of those created for non-Indigenous populations (Harlow et al., 2014; Pollock et al., 2018). However, Indigenous risk factors are often different to those of the general population, and their concepts of suicide frequently differ from Western concepts (Nasir et al., 2016). Furthermore, these adapted interventions have been reported to have adverse and limited effects on suicide-related outcomes for Indigenous populations (Pollock et al., 2018). Therefore, Indigenous-led suicide interventions that focus on community-specific priorities to account for cultural differences have been recommended (Gibson et al., 2021). There is evidence of reduced suicidality and increased protective factors with such interventions. However, due to weak study designs and lack of rigorous evaluation methods to assess the outcomes, little is known about their implementation, effectiveness and sustainability (Harlow et al., 2014; Pollock et al., 2018).
Gibson et al. (2021) studied the influence of community-level cultural connectedness on Queensland’s Indigenous suicide rates and found higher Indigenous suicide rates in areas with low levels of cultural social capital (participation of community members in cultural events, ceremonies, organisations and community activities) and high levels of reported discrimination. This study importantly identified that strategies to increase cultural connectedness and reducing institutional and personal racism could reduce suicide rates at an area-specific level. It would be important to see if these study findings are replicated across the rest of Australia to inform community and region-specific suicide prevention approaches.
Canada has very high Indigenous suicide rates, but only limited aggregated whole of country data are publicly accessible for the Canadian Indigenous groups, and because the number of deaths by intentional self-harm and ERP stratified by age and sex could not be attained for the Inuit, First Nations and Métis peoples, Canada was excluded from this analysis. However, Canada displays many parallels to the countries studied. Analogously, Indigenous suicide was a rare occurrence in the pre-colonial society, with rates only rising with arrival of settlers (Truth and Reconciliation Commission of Canada, 2015). Between 2011 and 2016, suicide rates for the Inuit people were nine times higher than that of non-Indigenous people (72.3 vs 8.0 deaths per 100,000), the First Nations people three times higher (24.3 deaths per 100,000) and the Métis people almost two times higher (14.7 deaths per 100,000) (Centers for Disease Control and Prevention, 2020; Herne et al., 2014; Kumar and Tjepkema, 2019). Today, their most vulnerable group remains those aged 15–24 years with rates having increased more than sixfold since the early 1980s (Hicks et al., 2007). Furthermore, in all three Indigenous groups, suicide rates for males were higher than their female counterparts (Kumar and Tjepkema, 2019). As such, there is evidence to indicate a vulnerability in young Canadian Indigenous males aged 15–24 years, a finding that would be consistent with the results of this study, and thus, emphasising the concern for Indigenous male youth suicide in anglosphere countries globally.
Limitations
Data were extracted from the CDC, ABS and Statistics New Zealand. These data may be subject to underreporting of Indigenous suicide rates when an individuals’ Indigenous status is not reported. In this study, suicide rates were only presented for the Indigenous and general populations (including Indigenous populations) as the CDC does not collect data with a specific non-Indigenous identification in the United States. As rates for the general population in our study are inclusive of Indigenous rates, the data may be biased and skewed towards minimising differences, particularly for NZ, given that Māoris make up 17% of the total population. However, Indigenous people make up small percentages of the population in Australia (3%) and the United States (2%) (AIHW, 2021; IWGIA 2022). Indigenous vs non-Indigenous suicide rates may also be confounded by age as Indigenous populations typically have a younger age structure than non-Indigenous populations (ABS, 2022; Ministry of Health, 2018; US Bureau of Labor Statistics, 2019). While we examined population suicide rates combined at a national level, research has shown that suicide rates vary significantly between regions and within Indigenous groups (Pollock et al., 2018). Therefore, further detailed research analysing these differences could provide greater insight into how suicide prevention interventions can be better tailored to individual communities. It is important to note that the suicide data for 2019 are still preliminary and subject to revision.
Conclusion
In the United States, Australia and NZ, Indigenous suicide rates have continued to increase between 2006 and 2019. Suicide rates for Indigenous females are increasing more rapidly than males in Australia and NZ. Indigenous males aged 15–44 years have the highest suicide rates across all the countries studied.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the College of Medicine and Public Health, Flinders University, Adelaide, SA, Australia
Ethical Approval and Informed Consent
No ethical approval or consent was required as this paper does not involve research with humans or animals and relates to de-identified data.