
Abstract
Objectives:
This study investigated trends in hospital-treated self-harm and hospital presenting suicidal ideation in the period before and after COVID-19 public health responses by key socio-demographic groups among those presenting to hospitals in the Western Sydney (Australia) population catchment.
Methods:
Emergency department presentations for the period January 2016 to June 2021 were used to specify a series of interrupted time-series models to compare the observed and expected event rates of (1) hospital-treated self-harm and (2) hospital presenting suicidal ideation in the period following the onset of COVID-19 public health measures in March 2020. Rate differences between observed and expected rates in the post-implementation period were also estimated in models stratified by sex, age group, country of birth and socio-economic status.
Results:
There was no significant increase in hospital-treated self-harm in the period post-implementation of public health orders (March 2020) compared to the previous period, although there were lower than expected rates of emergency department presentations among non-Australian-born males, males aged 0–14 years and 25–44 years, and females aged 45–64 years. In contrast, there was a significant increase in hospital presenting suicidal ideation, particularly among women (rate difference per 100,000 = 3.91, 95% confidence interval = [1.35, 6.48]) and those aged 15–24 years (both males and females, rate differences ranging from 8.91 to 19.04), and among those residing in lower socio-economic status areas (both males and females, rate differences ranging from 0.90 to 2.33).
Conclusion:
There was no increase in hospital-treated self-harm rates in the 15 months post-implementation of COVID-19 public health orders in Western Sydney; however, there was a significant increase in hospital presenting suicidal ideation. The limited change in suicidal behaviour may reflect the success of social and economic supports during this period, the benefits of which may have been different for young people, and those of lower socio-economic status.
Introduction
Concerns have been raised that restrictions implemented in response to the COVID-19 pandemic (such as physical distancing, restrictions on gatherings and neighbourhood lockdowns) may have negative effects on suicidal behaviour and that these impacts may differentially affect younger and more marginalised cohorts in populations (Gunnell et al., 2020; Niederkrotenthaler et al., 2020). This is largely due to a potential increase in exposure to a combination of risk factors including financial stress, domestic violence, alcohol misuse, mood disorders, and loneliness and social isolation (Gunnell et al., 2020).
Emerging international evidence, predominantly from high-income countries, suggests that in the early months after the COVID-19 pandemic there have been limited impacts on suicide and self-harm, and evidence of a decline in suicide rates in New South Wales (Pirkis et al., 2021). Mitigation strategies such as income and employment support, increases in digital and telehealth mental health support, and novel approaches to keeping people connected to employment may have contributed to stability. Previous studies have also shown the relative impacts of unemployment on suicide during periods of high (or low) general unemployment (Milner et al., 2013; Morrell et al., 1993, 2007).
Despite this, recent reports from Australia have suggested that the ongoing social and economic disruption of the COVID-19 pandemic has been associated with intermediary factors that may be associated with suicidal behaviour, e.g., increased contacts to digital crisis and mental health support services (Batchelor et al., 2021; Lifeline, 2021; Titov et al., 2020), higher levels of self-reported psychological distress and suicidal ideation (Fisher et al., 2020; Newby et al., 2020), and a poorer sense of well-being, especially among young people (Munasinghe et al., 2020). A review of health service use reported a decrease in mental health presentations to community teams, emergency departments and public hospitals in the early months of the pandemic, although there have also been signs of a trend towards pre-pandemic levels (Sutherland et al., 2020). Thus, the direct and indirect effects of COVID-19 and associated measures on suicidal behaviour require close monitoring and surveillance.
There have been few studies to date in the Australian context examining trends in hospital-treated self-harm and mental health service use in the period following the onset of the COVID-19 pandemic (Jacob et al., 2020; Page et al., 2021). Most evidence has related to changes in self-reported indicators of mental health in the early months of the pandemic (Fisher et al., 2020; Newby et al., 2020). Few studies have provided an assessment of the ongoing impacts of the COVID-19 pandemic in the period after the initial implementation of physical distancing policies in March 2020 in Australia. Accordingly, the current study investigates trends in hospital-treated self-harm and hospital presenting suicidal ideation in the period before and after the onset of the COVID-19 pandemic by key socio-demographic factors among those presenting to hospital emergency departments in the Western Sydney (Australia) population catchment.
Methods
Data
Data were obtained for the period January 2016 to June 2021 from the NSW Emergency Department Data Collection (EDDC) for the geographic catchment of the Western Sydney Local Health District. The Western Sydney Local Health District represents a population of approximately 946,000 (Western Sydney Local Health District, 2021) and comprises the Local Government Areas of Parramatta, Blacktown, Cumberland and The Hills Shire. This population is characterised by substantial demographic and socio-economic heterogeneity, with 50% of the population speaking a language other than English at home (Western Sydney Local Health District, 2021). EDDC data were obtained following approval by the Sydney Children’s Hospitals Network (SCHN) Human Research Ethics Committee (SCHN HREC 2021/ETH00461).
Exposure period
The exposure period was defined as the period after the implementation in March 2020 of Public Health Orders that limited movement and gatherings of people, and mandated closure of specified business premises (Levin and Kashyap, 2020), and which have remained in varying forms since then (NSW Government, 2021a).
Outcomes
The main outcomes of interest for this study were (1) hospital-treated self-harm and (2) hospital presenting suicidal ideation. Cases of self-harm presenting to the emergency department were identified using a combination of three diagnosis fields available in the EDDC database: ‘main diagnosis’, ‘presenting problem’ and ‘reason for admission’. Emergency department presentations include those who were subsequently admitted to hospital, as well as those not admitted to hospital. Approximately 87% of emergency department presentations following intentional self-harm are subsequently admitted to hospital (Sperandei et al., 2021). The main diagnosis field is coded using the SNOMED-CT system for the ‘problem to be treated’, with all patients allocated a pre-determined code for this field. The description of the codes used for hospital-treated self-harm can be found in Supplementary Table 1. The ‘reason for admission’ field is coded using International Classification of Diseases, 10th Revision (ICD-10). For this field, ICD-10 codes relating to intentional self-harm (X60-X84) were selected. The ‘presenting problem’ field consists of a drop-down menu with approximately 280 pre-selected case descriptions selected based on the problem as described by the patient or accompanying person. Hospital-treated self-harm cases were included where the emergency department presentation was coded as ‘MH – Self-Harm’. Although not always included in this type of analysis, the use of this ‘presenting problem’ field has been shown to almost double case enumeration of hospital-treated self-harm (Sperandei et al., 2021).
Hospital presenting suicidal ideation cases were selected using the same procedure described above. That is, using the corresponding SNOMED-CT codes (Supplementary Table 1), the ICD-10 code R45.81 (suicidal ideation) in the ‘reason for admission’ field, and the description ‘MH – Suicidal Ideation’ for the ‘presenting problem’ field.
There were a total of 1,048,955 emergency department presentations to the four emergency departments of Western Sydney Local Health District for the period January 2016 to June 2021 From these, 72,109 (6.9%) were excluded for being presentations to care (e.g. removing stitches, wound care, patient review) or marked as ‘registered in error’. Of the 976,846 remaining emergency department presentations, 7045 were identified as hospital-treated self-harm presentations, relating to 5168 unique individuals, and 13,122 emergency department presentations were identified as hospital presenting suicidal ideation only, relating to 9089 unique individuals.
Socio-demographic factors
Data from both sexes were analysed. Age at presentation was categorised as: 0–14 years, 15–24 years, 25–44 years, 45–64 years and 65 years or older. Country of birth of cases was also enumerated and classified as ‘Australian-born’ and ‘not Australian-born’. The area-based socio-economic status (SES) of cases was determined using quintiles of the Index of Relative Socio-economic Advantage and Disadvantage (IRSAD) associated with the reported residential postal code, based on the 2016 census (ABS catalogue number 2033.0.55.001).
Analysis
An interrupted time-series analysis (Harper and Bruckner, 2017) was used to assess the association between the onset of public health measures implemented in response to the COVID-19 pandemic and (1) hospital-treated self-harm and (2) hospital presenting suicidal ideation. The number of emergency department presentations was transformed to event rates per 100,000 population using the observed and estimated population for the Western Sydney region (Centre for Epidemiology and Evidence, 2021). Monthly rates for the period January 2016 to February 2020 were then used to fit a linear model based on the trend and seasonality of the time series, with indicator variables for each month (Hyndman and Athanasopoulos, 2018). This model was then used to predict the expected monthly rates for the period from March 2020 to June 2021. The predicted values were compared to the observed values and the mean difference (and 95% confidence interval [CI]) between monthly observed and expected rates was estimated. Analyses were conducted in R Studio version 4.1.1 (R Core Team, 2021) using the forecast package.
Results
Hospital-treated self-harm
There was no statistical evidence of an increase in total hospital-treated self-harm in the period post-implementation of COVID-19 public health orders, compared to the period prior to implementation, among males or females (Figures 1 and 3(A)). There were also few differences between observed and expected rates by age group, SES or country of birth, with the exception of lower hospital-treated self-harm event rates among non-Australian-born males (rate difference [RD] per 100,000 = −0.64, 95% CI = [−1.00, −0.28]), males aged 0–14 years (RD = −0.63, 95% CI = [−0.89, −0.38]) and 25–44 years (RD = −1.99, 95% CI = [−3.83, −0.14]); and females aged 45–64 years (RD = −2.77, 95% CI = [−3.74, −1.80]) (Figure 3(A)). Lower hospital-treated self-harm rates were also evident for some SES quintiles (quintiles 2 and 3 for males, and quintile 2 for females).
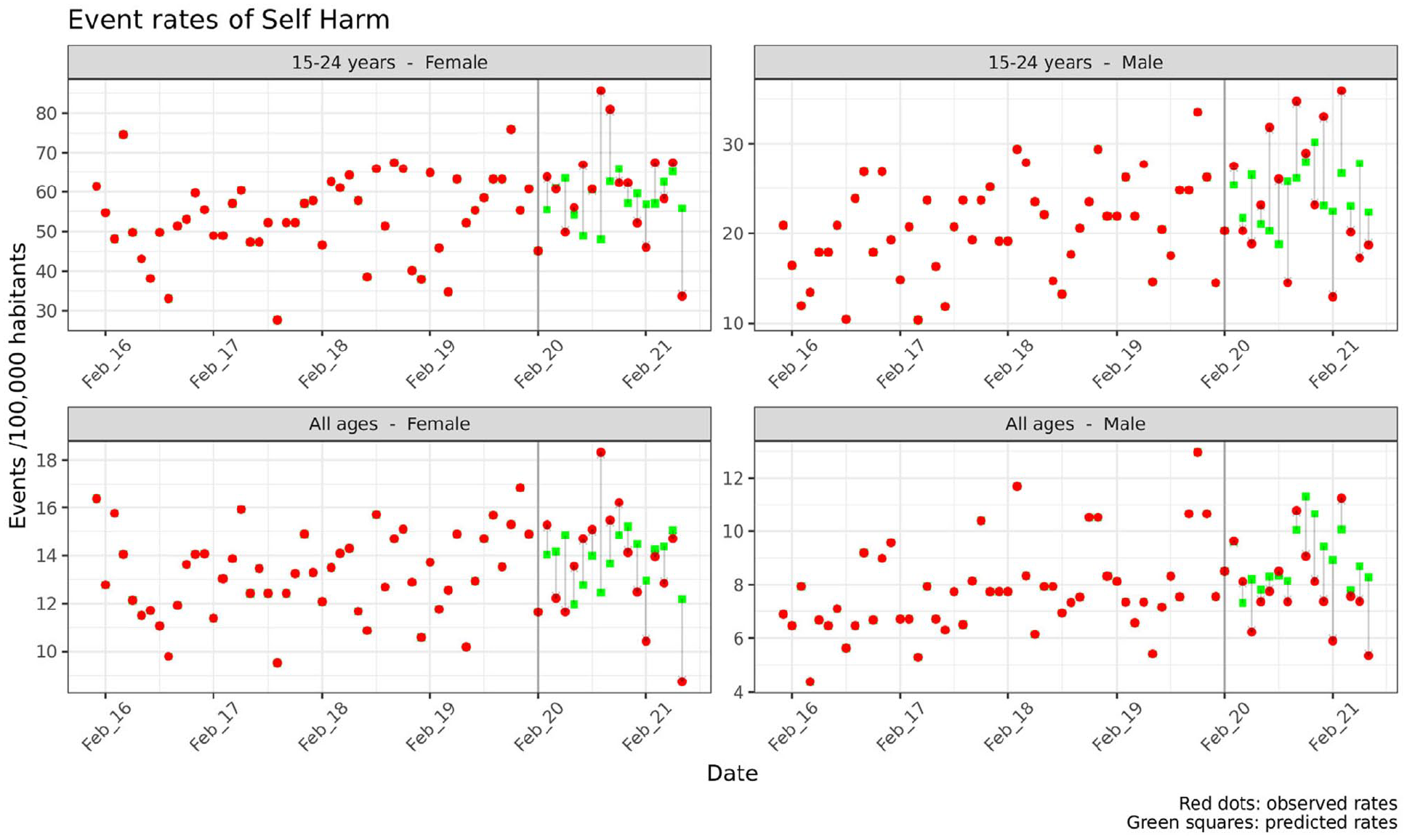
Monthly event rates for hospital-treated self-harm, pre- and post-implementation of COVID-19 public health orders (Western Sydney Local Health District emergency department presentations, January 2016 to June 2021).
Hospital presenting suicidal ideation
There was also no increase in total hospital presenting suicidal ideation in the period post-implementation of COVID-19 public health orders compared to the period prior to implementation among males (Figures 2 and 3(B)), but a significant increase among females (RD = 3.91, 95% CI = [1.35, 6.48]) (Figure 3(B)). There were significant differences between observed and expected rates among males aged 15–24 years (RD = 8.91, 95% CI = [3.00, 14.82]), and females aged 0–14 years (RD = 1.41, 95% CI = [0.60, 2.23]), 15–24 years (RD = 19.04, 95% CI = [6.18, 31.90]), and 45–64 years (RD = 2.85, 95% CI = [0.19, 5.53]) (Figure 3(B)). Hospital presenting suicidal ideation was also higher among lower SES groups for both males and females (RDs ranging from 0.90 to 2.33 among quintiles 4 and 5), the Australian-born for males (RD = 1.87, 95% CI [0.39, 3.36]), and for both the Australian-born (RD = 2.42, 95% CI = [0.24, 4.60]) and non-Australian born (RD = 1.50, 95% CI = [0.67, 2.33]) for females (Figure 3).
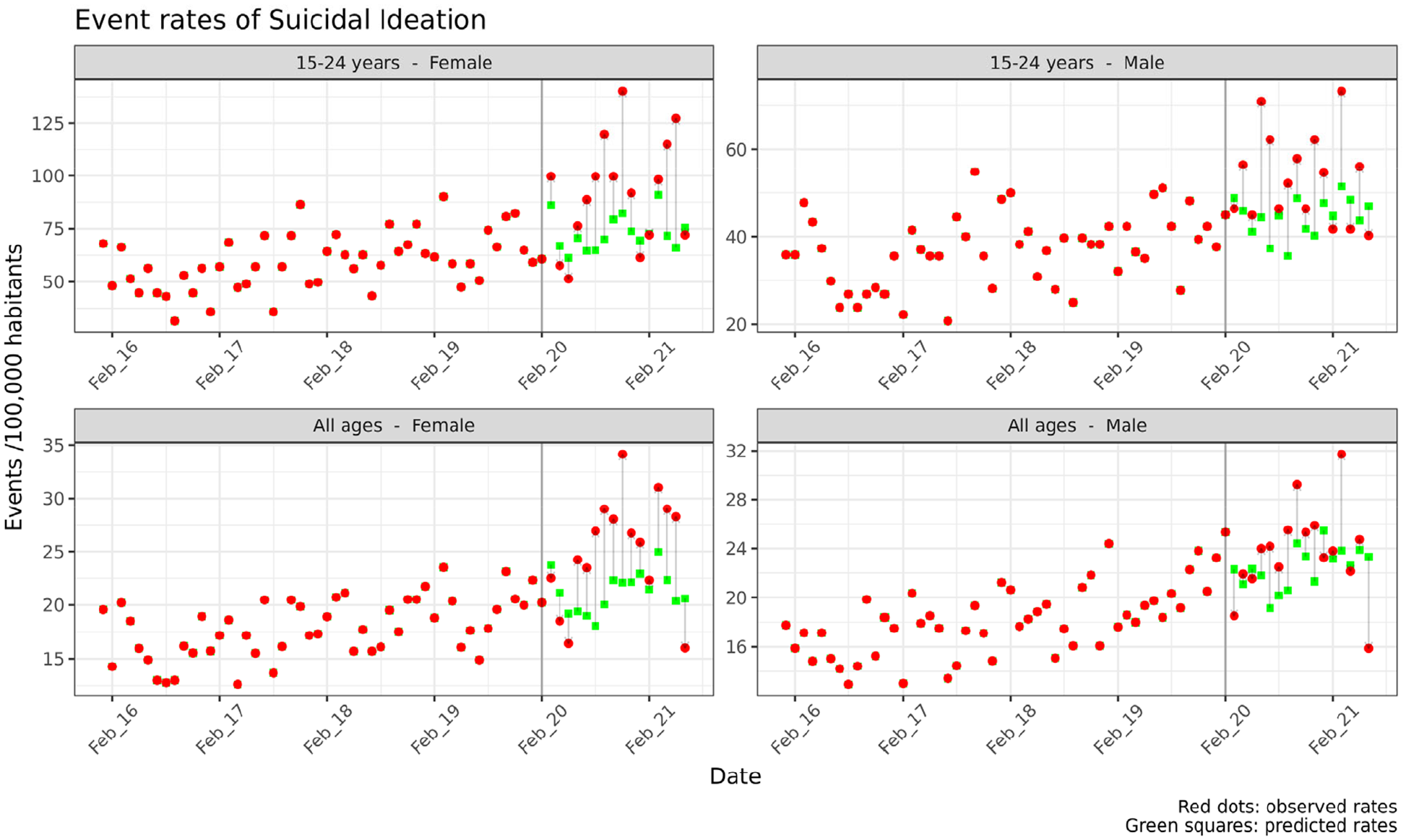
Monthly event rates for hospital presenting suicidal ideation, pre- and post-implementation of COVID-19 public health orders (Western Sydney Local Health District emergency department presentations, January 2016 to June 2021).
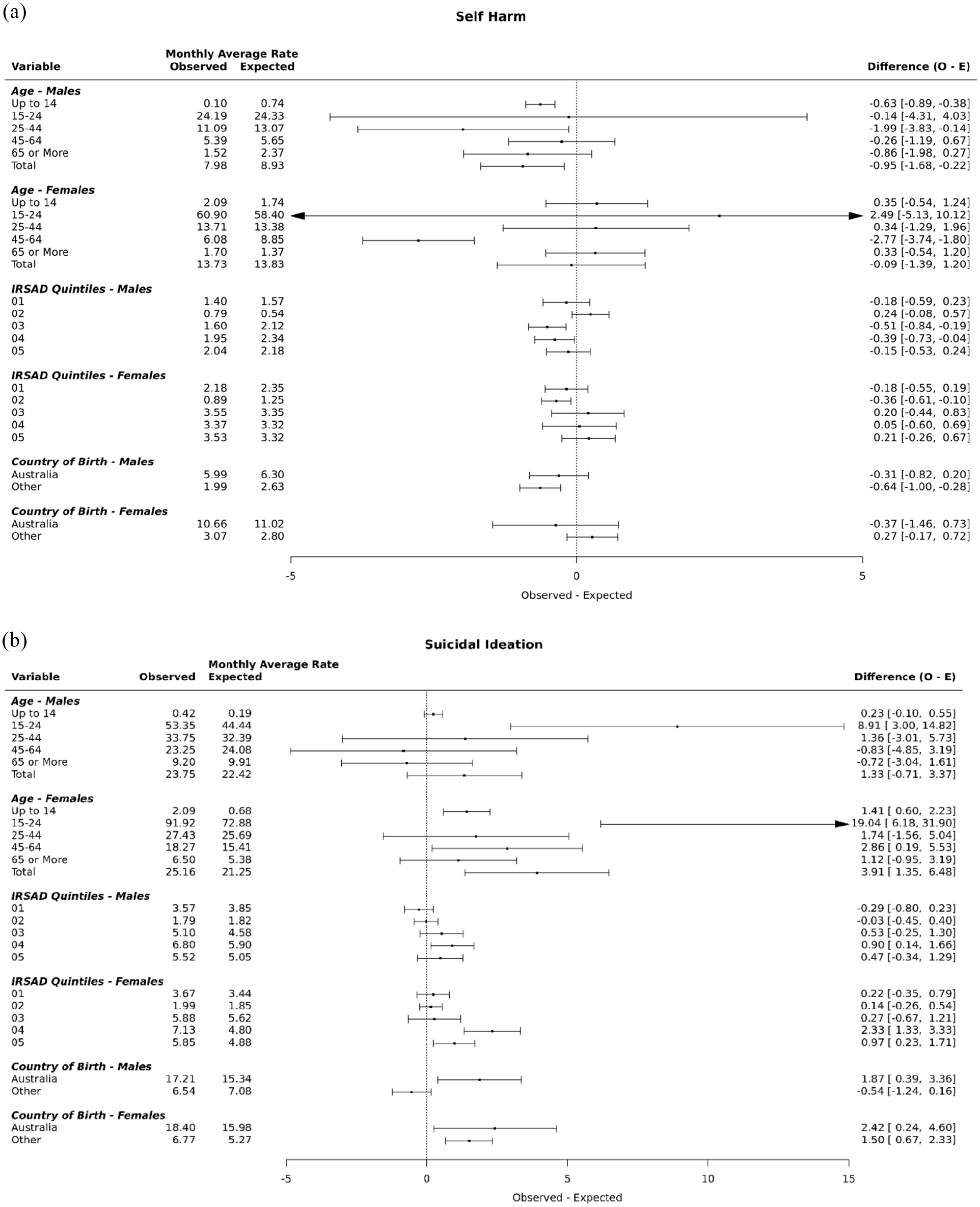
Differences in monthly event rates for hospital-treated self-harm and hospital presenting suicidal ideation, pre- and post-implementation of COVID-19 public health orders (Western Sydney Local Health District emergency department presentations, January 2016 to June 2021).
Discussion
This study investigated trends in hospital-treated self-harm and hospital presenting suicidal ideation in the period before and after the onset of the COVID-19 pandemic public health orders in the Western Sydney (Australia) population catchment. There was a significant increase in hospital presenting suicidal ideation in the period post-implementation of the public health orders (March 2020) compared to the previous period, particularly among women, and those aged 15–24 years (both males and females), and among those residing in lower SES areas (both males and females). In contrast, there was no significant increase in hospital-treated self-harm, although there were lower rates of emergency department presentations among non-Australian-born males, males aged 0–14 and 25–44 years, and among females aged 45–64 years.
The findings suggest that the COVID-19 pandemic may have had an impact on intermediate factors associated with suicidal behaviour, such as suicidal ideation, but not hospital presenting self-harm per se. This is consistent with recent studies that have also reported increased psychological distress (Fisher et al., 2020; Newby et al., 2020) and decreases in self-reported well-being (Munasinghe et al., 2020; O’Connor et al., 2021). However, there have been few changes in suicide (Pirkis et al., 2021) and increasing evidence of a reduction in hospital presenting self-harm in the early months of the pandemic (John et al., 2021; Jollant et al., 2021; Kapur et al., 2021).
The findings from this study also suggest women, young people and people from socioeconomically disadvantaged backgrounds are especially vulnerable. This is consistent with longitudinal studies in the United Kingdom that have reported increases in suicidal ideation and lower levels of mental well-being among women, younger adults (18–29 years) and people from lower socio-economic backgrounds (O’Connor et al., 2021; Pierce et al., 2020). The lockdowns and social and economic disruptions accompanying the COVID-19 pandemic have been associated with a rise in a combination of risk factors that may disproportionately affect these sub-populations. These shared risk factors include financial stress and domestic violence (Morgan and Boxall, 2020; Pfitzner et al., 2020; Roesch et al., 2020), alcohol misuse (Newby et al., 2020) and loneliness (O’Connor et al., 2021). Previous studies have suggested contemporaneous impacts of social and economic disruption on suicide (Chang et al., 2009, 2013; Värnik et al., 1998) which, as yet, appear not to have emerged. The current findings relating to suicidal ideation may reflect an indication of emerging risk, and continuous monitoring over the longer term is needed given the likely social and economic challenges associated with the COVID-19 pandemic.
The limited change in suicidal behaviour in the Australian context may reflect the success of economic supports from government (e.g. Jobkeeper and Jobseeker), in keeping people connected to their employment. However, the level of effectiveness may have been different for different demographic groups (e.g. young people, and those of lower SES), particularly for those in casual and insecure employment who were less likely to be eligible for this economic support. This may also reflect the importance of relative levels of economic distress (Milner et al., 2013; Morrell et al., 1993, 2007) and a collective understanding of the transience of this period of social and economic disruption. For example, previous studies have shown a strong association between the relative unemployment rate and the relative suicide rate, suggesting that being unemployed in periods with high general unemployment is less stressful than being unemployed during periods of general low unemployment. This is possibly linked to a ‘pulling together’ phenomenon, where community cohesion and mutual support may increase during intense periods of social disruption and/or public health emergencies (Gordon et al., 2011; Zortea et al., 2020). Increased use of help lines and online resources were also noted during period of public health restrictions (Berger and Reupert, 2020; Titov et al., 2020), perhaps reflecting an increased societal awareness of potential mental health impacts and evidence of help-seeking behaviour that may have contributed to lower likelihood of a presentation to an emergency department setting.
There are a number of methodological limitations when interpreting the findings from the current study. First, the main outcomes of the study (self-harm and suicidal ideation) relate to cases presenting to an emergency department setting and therefore are likely to be an under-enumeration of suicidal behaviour in the general community of Western Sydney. It is not possible to ascertain with the current data whether there was differential access and availability of services pre- and post-implementation of public health orders. However, it might be possible that those who self-harmed may have been less likely to present to hospital given the restrictions on movement during the early period of public health responses, and also a fear of COVID-19 infection in a hospital setting. For example, a study on healthcare activity in NSW showed a reduction in healthcare-seeking behaviour (including emergency department visits) during the early post-implementation period (March to June 2020), compared to the previous year (Sutherland et al., 2020).
It is also possible that there is ascertainment bias in the cases of hospital-treated self-harm, due to the limitations and potential miscoding, or misclassification, of using EDDC fields containing ICD-10 and SNOMED-CT codes. Being able to determine suicidal intent among those presenting to emergency department settings is not always straightforward, and there are likely cases of self-harm that were not coded, or coded as non-intentional outcomes (e.g. where poisoning or overdose was evident). This source of ascertainment bias was partially addressed by using the additional information in the ‘presenting problem’ field, which has previously been shown to improve the ascertainment of hospital-treated self-harm by almost 50% (Bandara et al., 2021).
While self-harm rates appear not to have increased in the short term, it is an important health outcome for continued monitoring given the likely prolonged social and economic effects of the pandemic. The rise in suicidal ideation, particularly among young people, women and people from socioeconomically disadvantaged regions is an area of public health concern. Ongoing monitoring and evaluation of interventions that aim to prevent suicidal behaviour and provide appropriate access to mental health care are needed. This includes the range of current mental health programmes and partnerships that have been funded, such as Towards Zero Suicide initiatives (NSW Health, 2021), the Safeguards programme (NSW Government, 2021b), the NSW School-Link programme (NSW Government, 2021c), and other early intervention and assertive outreach models of care that are being implemented in response to the COVID-19 pandemic (NSW Government, 2021b). The likely impacts of broader social and financial supports implemented during the initial period of the COVID-19 pandemic also highlights the ongoing importance of the social determinants of suicidal behaviour and the need for equitable access to mental health services and suicide prevention initiatives to ensure that the right mental health care is provided to the right people at the right time.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211068393 – Supplemental material for The impact of the COVID-19 pandemic on hospital-treated self-harm in Sydney (Australia)
Supplemental material, sj-docx-1-anp-10.1177_00048674211068393 for The impact of the COVID-19 pandemic on hospital-treated self-harm in Sydney (Australia) by Sandro Sperandei, Andrew Page, Piumee Bandara, Arianne Reis, Rowena Saheb, Pankaj Gaur, Sithum Munasinghe, Kathryn Worne, Carolyn Fozzard and Vlasios Brakoulias in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.