
Abstract
Purpose:
To examine the rates and profiles of intentional self-harm hospital admissions among people from culturally and linguistically diverse and non-culturally and linguistically diverse backgrounds.
Methods:
A retrospective analysis of 29,213 hospital admissions for self-harm among people aged 15 years or older in Victoria, Australia, was conducted using data from the Victorian Admitted Episodes Dataset between 2014/2015 and 2018/2019. The Victorian Admitted Episodes Dataset records all hospital admissions in public and private hospitals in Victoria (population 6.5 million). Population-based incidence of self-harm, logistic regression and percentages (95% confidence intervals) were calculated to compare between culturally and linguistically diverse groups by birthplaces and the non-culturally and linguistically diverse groups of self-harm admissions.
Results:
When grouped together culturally and linguistically diverse individuals had lower rates of (hospital-treated) self-harm compared with the non-culturally and linguistically diverse individuals. However, some culturally and linguistically diverse groups such as those originating from Sudan and Iran had higher rates than non-culturally and linguistically diverse groups. Among self-harm hospitalised patients, those in the culturally and linguistically diverse group (vs non-culturally and linguistically diverse group) were more likely to be older, Metropolitan Victorian residents, from the lowest socioeconomic status, and being ever or currently married. Self-harm admissions by persons born in Southern and Eastern Europe were the oldest of all groups; in all other groups number of admissions tended to decrease as age increased whereas in this group the number of admissions increased as age increased.
Conclusion:
There was considerable heterogeneity in rates of hospital-treated self-harm in culturally and linguistically diverse communities, with some countries of origin (e.g. Sudan, Iran) having significantly higher rates. Some of this variation may be due to factors relating to the mode of entry into Australia (refugee vs planned migration), and future research needs to examine this possibility and others, to better plan for support needs in the culturally and linguistically diverse communities most affected by self-harm. Combining all culturally and linguistically diverse people into one group may obscure important differences in self-harm. Different self-harm prevention strategies are likely to be needed for different culturally and linguistically diverse populations.
Keywords
Background
Intentional self-harm (herewith referred to as self-harm) is a serious public health concern in Australia. Self-harm encompasses a broad range of behaviours, but is typically defined as deliberately self-initiated harm and includes behaviours such as hanging, poisoning, and cutting with and without suicide intent (Nixon et al., 2008; Nock, 2010). Large-scale representative cohort studies in young Australians have found that over 8% of 14–19 years old report self-harm (Moran et al., 2012). Based on hospital data, there were an estimated 33,100 self-harm admissions in Australia in the financial year 2016–2017 (Australian Institute of Health and Welfare, 2019). In Victoria, there were 18,103 admissions involving those aged 10 years or older between July 2014 and June 2017 (Clapperton, 2019). Self-harm is one of the strongest predictors of suicide (Hawton and James, 2005): people treated in hospital for self-harm are at 30–200 times higher risk of suicide in the following 12 months (Cooper et al., 2005). Given that previous self-harm is a strong risk factor for suicide, the monitoring of self-harm and gaining a better understanding of the risk factors, particularly in communities that may be disproportionally represented in the incidence of self-harm, is key to suicide prevention efforts prioritised by the Australian Government. However, there is currently little research on the extent of self-harm in populations who have migrated to Australia.
More than 6.9 million Australian citizens were born overseas. Of these, nearly 1.9 million overseas-born citizens live in Victoria, equating to the state having the second highest prevalence of non-Australia-born residents (Australian Bureau of Statistics (ABS), 2016). For research purposes, culturally and linguistically diverse (CALD) communities include people who were born in non-English-speaking countries and/or those who do not speak English as the main language at home (Pham et al., 2021). Epidemiological research has suggested that there are considerable health disparities and unique conditions that arise in people from culturally diverse backgrounds (Abouzeid et al., 2013). Specifically, an inquiry from the Australian government in 2013 showed that new migrants with lower levels of English proficiency were statistically more likely to be overrepresented in social-economically disadvantaged groups (The Senate Standing Committees on Community Affairs, 2014) due to relatively high rates of unemployment and limited access to available services (Taylor, 2004). Such disadvantages together with mental distress, social exclusions, prejudice, discrimination or racism experienced in host countries have possibly placed people from multicultural backgrounds at increased risk for self-harm (Chan and Thambu, 2016; Skegg, 2005). Although international research has confirmed that cultural backgrounds and race or ethnicity is highly relevant to self-harm (Bhui et al., 2007; Cooper et al., 2010; Kuentzel et al., 2012), research on the relationship between culture and self-harm in Australia is relatively scarce. Taking cultural differences into account when developing interventions can help enable resources to be accessible, inclusive and responsive to the needs of people who require assistance. Therefore, research regarding the cultural impacts of self-harm will inform prevention opportunities and reduce self-harm.
As Australia is experiencing rapid immigration from diverse countries, the health care system needs to respond to CALD people’s needs. However, most research in Australia has focused on self-harm in general populations, with little research examining self-harm in culturally diverse communities. Therefore, this study is designed to examine the self-harm profile of CALD communities in Victoria Australia. We aim (1) to explore the ranking of hospital-treated self-harm incidence rates by CALD populations based on country of birth (COB) and (2) to compare the patterns and profiles of hospital-treated self-harm among people from CALD and non-CALD groups. The information will contribute to informing more targeted and effective self-harm prevention measures and provide direction for future research.
Methods
Study design
This study involved an analysis of Victorian hospital admission data and population data, which were used to calculate population-based rates of self-harm.
Data sources: Hospital admissions cases were extracted from the Victorian Admitted Episodes Dataset (VAED) which records all hospital admissions in public and private hospitals in the state of Victoria. The VAED is coded to the International Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modifications (ICD-AM). The ABS (2016) sourced population data that were stratified by year, age, sex and COB.
Participants
Inclusion criteria:
1. Self-harm: hospital admission records with ICD-10-AM (X60-X84) self-harm cause codes anywhere in the diagnosis codes and limited to those who also had an injury (S00-T98) or a mental health condition in the principal diagnosis (F00-F99);
2. Self-harm hospital admissions occurred in the financial years 2014/2015 to 2018/2019.
In total, 31,227 hospital admission records of patients who were admitted due to self-harm between 1 July 2014 and 30 June 2019 were reviewed for eligibility.
Exclusion criteria:
3. Intersex cases were excluded to maintain confidentiality as these numbers were less than 5 in the stratified data (n = 22);
4. Non-Victorian residents regardless of their visa status were excluded to match with population data (n = 863);
5. Younger than 15 years old (n = 855);
6. Missing COB information (n = 281).
Based on the criteria, we selected 29,213 self-harm hospital admission records for data analysis (one record can have more than one exclusion criteria).
Definitions
Self-harm admissions captured in this study include people who engaged in self-harm with or without the intention to die.
CALD group consisted of those who were born in non-English-speaking countries (Pham et al., 2021). We omitted the two CALD components ‘main language spoken at home’ and ‘Indigenous status’ in the CALD selection because population data by language spoken at home were not available (from the ABS website or elsewhere), and Indigenous population size in Victoria is very small compared with CALD and non-CALD populations, which affects the statistical power of research. Therefore, non-CALD populations included those who were born in English-speaking countries: Australia, the United Kingdom (England, Scotland, Wales, Northern Ireland), Republic of Ireland, New Zealand, Canada, United States of America and South Africa. Conversely, the CALD group included those who were born in other countries.
CALD admissions were also divided into nine subgroups of CALD by regions of birth (ROB) based on the ABS’s region classifications, specifically:
Oceania and Antarctica region, excluding Australia and New Zealand*;
North-West Europe, excluding the United Kingdom (England, Wales, Scotland, Northern Ireland) and Republic of Ireland*;
Southern and Eastern Europe;
North Africa and the Middle East;
South-East Asia;
North-East Asia;
Southern and Central Asia;
Americas, excluding Canada and the United States of America*;
Sub-Saharan Africa, excluding South Africa*.
* Persons who were born in English-speaking countries were excluded from the relevant CALD groups by ROB, and they were included in the non-CALD group.
Ethical consideration
Ethical approval was provided by the Monash University Human Research Ethics Committee (Project ID 23719).
Variables and data measurements
Demographic variables included sex, age group, remoteness, socioeconomic status, marital status, alcohol-related admission and CALD status. The Accessibility and Remoteness Index of Australia (ARIA+) (Hugo Centre, 2018) was used to define five remoteness categories. Socioeconomic status was classified as per the Socio-Economic Indexes for Areas (SEIFA). The specific SEIFA used in this study was the Index of Relative Socio-Economic Advantage and Disadvantage, with state deciles based on Statistical Local Areas. Lower decile ratings represented a greater disadvantage. COB data from the VAED was used to classify cases as CALD and non-CALD, and identify specific CALD regions. Hospital admissions were classified as alcohol-related if they included an ICD-10-AM diagnosis or external cause code referring to alcohol (McKenzie et al., 2010).
Injury-related variables including causes of injury, mechanisms of injury and poisoning, and place of injury occurrence were coded based on ICD-10-AM. Only the two most common places of self-harm injury were presented; these were ‘home’ and ‘health service area’. The latter included day procedure centre, health centre, home for the sick, hospice, hospital and outpatient clinic.
Outcomes of injury included length of hospital stay and injury severity. Injury severity was calculated using the ICD-based Injury Severity Score (ICISS) (Osler et al., 1996), a serious injury was considered to be one with an ICISS less than 0.941 (survival probability of 94.1% or less) (Cryer et al., 2008). Computation of the ICISS was based on injury diagnosis, a survival risk ratio (SRR) (proportion of survivors among all patients with that particular ICD-10-AM diagnosis) using the worst injury method (Henley and Harrison, 2009).
These variables are considered as relevant to the context as previous work has shown that there are links between these factors and self-harm or cultural backgrounds (Bhui et al., 2007; Chan and Thambu, 2016; Skegg, 2005).
Statistical methods
Rates of self-harm in CALD and non-CALD populations by COB, by age and sex per 100,000 population were calculated for the 5 years from 2014/2015 to 2018/2019. The denominators to calculate the rates are the estimated populations at December points of years, which were interpolated (for 2014/2015 to 2016/2017) and extrapolated (for 2017/2018 and 2018/2019) based on Victorian population data from two census years 2011 and 2016 (ABS, 2016); data were stratified by COB, age and sex. Age standardisation of rates was carried out using 5-year age groups and the direct method (Armitage et al., 2008). The standard population used was the Victorian resident population on 30 June 2011 (Australian Institute of Health and Welfare, n.d.).
Age of CALD and non-CALD groups were presented as means and confidence intervals (95% CIs) (Table 3). Percentages and 95% CIs were used to compare CALD and non-CALD groups of self-harm admissions by socio-demographic characteristics, injury types and injury outcomes. The four specific CALD groups by regions with the highest number of cases were compared with non-CALD groups (Table 3).
To compare the profile of self-harm between people from the CALD and non-CALD groups, univariate logistic regression modelling was carried out with the outcome variable of CALD status (CALD and non-CALD); independent variables included sex, age groups, remoteness, SEIFA, marital status, alcohol-related admission, mechanisms of injury or poisoning, places of self-harm occurrence, length of stay in hospital and injury severity (Table 3). Sample sizes were large in this study; therefore, effect sizes were more meaningful than p values to establish associations between outcome variables and demographic and other relevant factors (Lin et al., 2013). The effect size was calculated as the difference between the odds ratio (OR) of the group under consideration and the OR of the reference group (which equals 1) (Lin et al., 2013), with an effect size of ±30% considered as notable (Fernando et al., 2019). These variables were then included in a multivariable model to consider the effect of each variable while controlling for all other variables, with effect sizes assessed similarly.
Results
Sample
After reviewing eligibility, we selected 29,213 hospital admission records; these were allocated into two groups of CALD status based on COB, with 26,093 cases in the non-CALD group and 3120 cases in the CALD group. In the study sample, females comprised two-thirds of cases (n = 19,585, 67.0%) and there were more admissions among people in younger age groups than in the older groups. Most self-harm admissions are among persons living in metropolitan areas of Victoria (n = 19,095, 65.4%) and were from advantaged relatively socioeconomic groups.
Population-based self-harm rates by ROB and COB
In general, the CALD population had a much lower rate of self-harm than the non-CALD population (43.8 and 141.2 admissions/100,000 population-years respectively, p < 0.001). In the nine ROB of CALD communities, North-West Europe had the highest rate (86.3/100,000 population-years); in contrast, Asian areas had the lowest rates with 23.6/100,000 population-years for those born in North-East Asia, 35.0 for those born in South-East Asia (SEA) and 38.3 for those originating from Southern and Central Asia (SCA).
There were vast differences in rates of self-harm in CALD communities by specific COB. Sudan (179.2/100,000 population-years) had the highest rate, followed by Iran (134.6) and Kenya (121.0). All the 10 birth countries with the lowest rates of self-harm were in the CALD group. China, the largest CALD community in Victoria based on COB, had the lowest hospital-admitted self-harm rate with 17.9/100,000 China-born people (Table 1).
Countries of birth of Victorian residents with the highest and lowest rate of self-harm hospital admissions from July 2014 to June 2019.
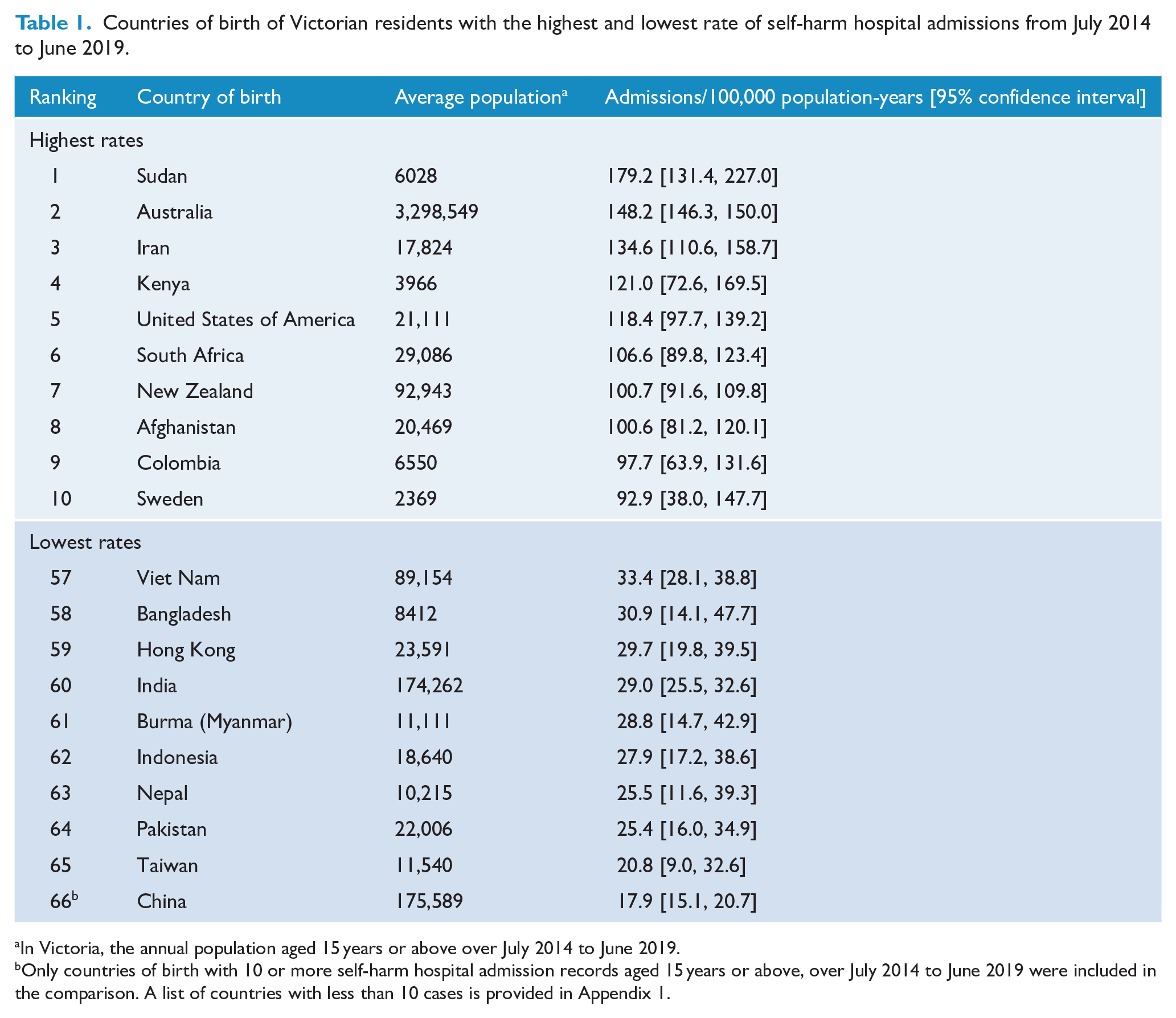
In Victoria, the annual population aged 15 years or above over July 2014 to June 2019.
Only countries of birth with 10 or more self-harm hospital admission records aged 15 years or above, over July 2014 to June 2019 were included in the comparison. A list of countries with less than 10 cases is provided in Appendix 1.
Age-standardised rates of self-harm
In both CALD and non-CALD groups, females presented a higher rate of self-harm than males. Specifically, the rates of self-harm hospital admissions among females from CALD and non-CALD groups are 54.0 and 187.5/100.000 people-years, respectively; they are 32.9 and 93.4 in males. Self-harm rate decreased with age in both groups, but it decreased more steeply with age in the non-CALD group than in the CALD group (chi-square test for trend, χ2 = 34.375, p < 0.001). The rates in the oldest age group (75+) were similar in CALD vs non-CALD.
Profiles of self-harm hospital-admitted people from CALD and non-CALD populations
Univariate analysis
Among those admitted to hospital for self-harm, the associations between various characteristics and CALD status are shown in Table 2. Older people, those living in metropolitan areas, being (ever) married and those who engaged in self-harm at home were more likely to belong to CALD than the non-CALD group. Being older increased the likelihood of being from the CALD group compared to the youngest group. Living in regional areas (compared to metropolitan areas) was negatively associated with CALD status. However, sex, SEIFA deciles, alcohol-related admission status and length of stay in hospital were not notably different in self-harm hospital-admitted people from CALD and non-CALD backgrounds.
Characteristics of CALD and non-CALD people who were admitted to hospitals due to self-harm.
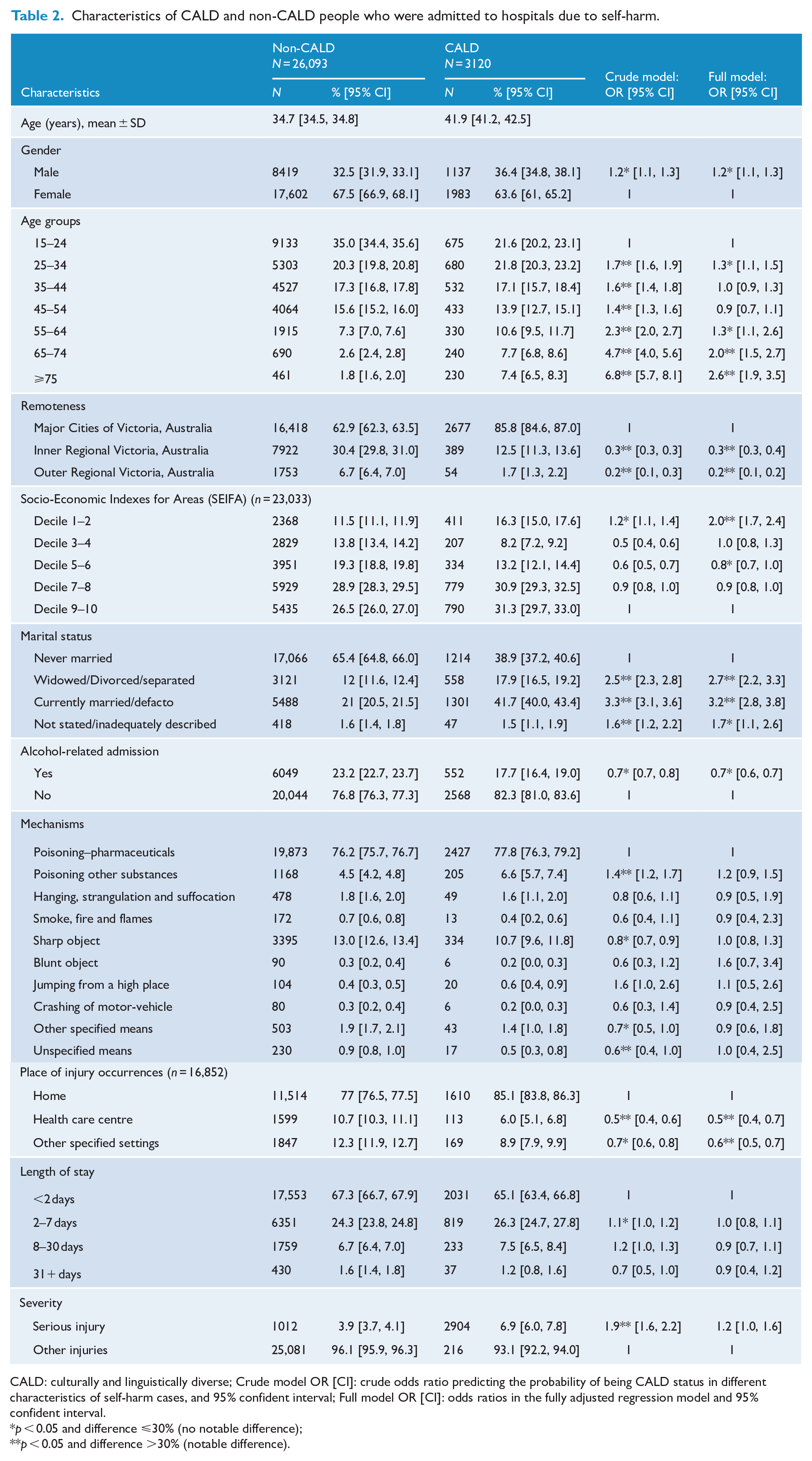
CALD: culturally and linguistically diverse; Crude model OR [CI]: crude odds ratio predicting the probability of being CALD status in different characteristics of self-harm cases, and 95% confident interval; Full model OR [CI]: odds ratios in the fully adjusted regression model and 95% confident interval.
p < 0.05 and difference ⩽30% (no notable difference);
p < 0.05 and difference >30% (notable difference).
Multivariable logistic regression model
Results of the fully adjusted modelling are presented in Table 2: Mechanism of injury and severity of injuries, which were associated with CALD status in the univariate analysis, were no longer statistically significant in the fully adjusted model. This means that the association between mechanism and severity of self-injuries and CALD status is explained by socio-demographic differences between CALD and non-CALD groups. SEIFA decile (not a statistically significant factor in the univariate model) became significantly associated with CALD status in the fully adjusted model.
Therefore, among those admitted to hospital due to self-harm, the profiles of the CALD and non-CALD groups were different in terms of age, remoteness, SEIFA, marital status and places where injuries occurred. There were no notable associations between sex, alcohol-related admission or length of stay (effect size ⩽ 30%) and CALD status.
Interactions between age groups and sex and between marital status and sex were explored in the models; these were not statistically significant.
Comparisons between specific CALD groups by ROB and the non-CALD population
Among the nine specific CALD groups based on ROB (excluding English-speaking COB), Southern and Eastern Europe (SEE; 669 cases), SCA (573 cases), SEA (487 cases), and North Africa and the Middle East (454 cases) were the four regions with the highest number of self-harm cases. These were selected as the four subgroups of CALD communities to compare with the non-CALD group (Table 3).
Characteristics of four CALD regions with the highest prevalence of self-harm and compared to the non-CALD group.
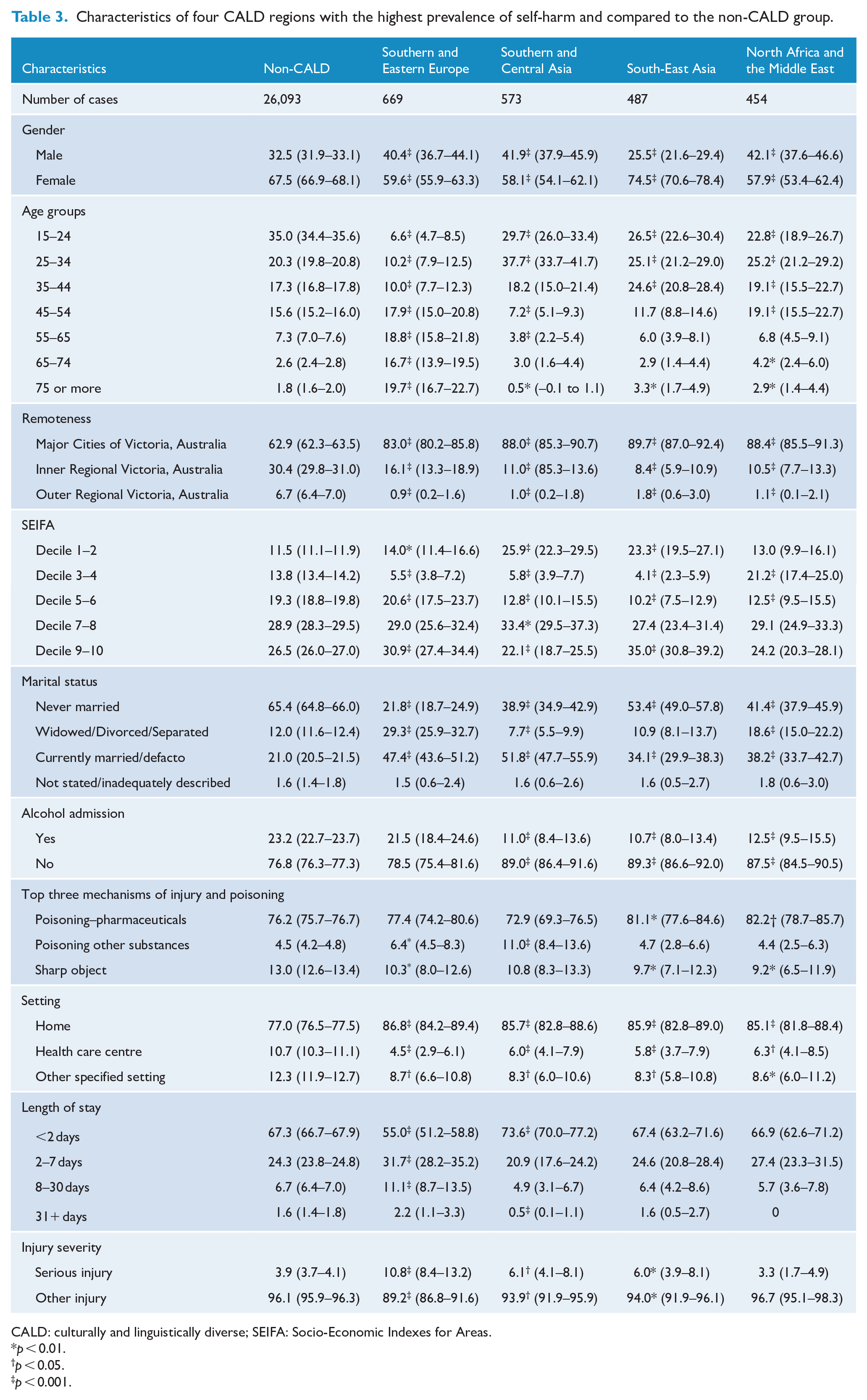
CALD: culturally and linguistically diverse; SEIFA: Socio-Economic Indexes for Areas.
p < 0.01.
p < 0.05.
p < 0.001.
Generally, Table 3 shows that there are differences in characteristics of the four subgroups of self-harm admissions by ROB (hereafter referred to as CALD subgroups) and they are also different to the non-CALD comparison group. Specifically, persons born in SEE were characterised by being the oldest of all groups; in all other groups number of admissions tended to decrease as age increased whereas in this group the number of admissions increased as age increased. The SCA group had the highest proportion of self-harm hospital admissions among those aged 25–34 years and the highest proportion of self-harm due to poisoning by ‘other substances’. Although females were overrepresented in all groups, they accounted for a higher proportion of admission in the SEA group than in the other groups. More than half of the group from SEA had never married (53.4%): the highest proportion among the four subgroups; in contrast, the SEE group was much less likely to be never married and much more likely to be widowed/separated/divorced compared with the other groups.
Discussion
The study examined whether rates of self-harm hospital admissions were different for CALD vs non-CALD communities, and potential correlates of self-harm. Results showed that as a group, CALD communities had lower rates of self-harm hospital admissions when compared with non-CALD communities. However, there was considerable heterogeneity in rates of self-harm in CALD communities, with some CALD communities (e.g. Sudanese, Iranian, Kenyan) having higher rates than some non-CALD populations, while large CALD communities originating from China, India and Vietnam had the lowest rates of self-harm.
It is possible that the differences in self-harm rates across CALD populations by COB may be due to differences in the way in which people from different COB arrived to live in Australia. For example, CALD populations from countries such as Sudan and Kenya may be disproportionately more likely to have entered Australia as refugees rather than through planned migration (e.g. China, India). Moreover, those arriving in Australia as refugees could be suffering from higher rates of mental distress (e.g. depression and anxiety) common in countries at war, or with civil conflict (i.e. Sudan). Sudan is known to have high levels of existing mental illness due to civil conflict, and people from Sudan are known to be more likely to have entered Australia as refugees (Milner and Khawaja, 2010; Schweitzer et al., 2006). In contrast, the lower rate of self-harm in the Chinese population is consistent with patterns of self-harm in Chinese people in countries such as England (Chang et al., 2015). Unfortunately, we were unable to directly compare the rates of self-harm by CALD populations with the corresponding rates in their countries of origin, due to limited available evidence about hospital-admitted self-harm in the relevant birth countries.
The study raises important questions around the need for self-harm platforms and databases to collect more detailed data on how people entered Australia and under what circumstances (e.g. as refugees fleeing conflict, or as planned migrants). Such data would help inform policy decisions and resource allocation to those populations most likely to be in need of support for reducing self-harm and suicide. Prevention activities are already under-resourced and sometimes ill-directed, so knowledge of who is most likely at risk and where they are situated would allow more strategic deployment of prevention efforts and resources.
Despite the country-specific differences in rates of self-harm, the overall rates of self-harm were more than threefold lower in CALD populations compared with non-CALD populations. This finding is somewhat contrary to expectations and common public discourse around migrant difficulties in Australia as these groups of people have been reported to experience unique conditions that are also risk factors for self-harm such as social isolation, language barriers, prejudice, discrimination and racism (Bhui et al., 2007; Chan and Thambu, 2016; Skegg, 2005). However, previous research in Australia and Canada which found a twofold lower rate of self-harm in immigrants compared to long-term Australian/Canadian residents (Saunders et al., 2019; Stapelberg et al., 2020) provides support for the present results. Patterns of self-harm similar to those observed here in Australia and Canada have also been observed in the United States (Kuentzel et al., 2012). Additionally, although not focused on self-harm per se, work in Switzerland (Vazsonyi et al., 2017) suggests there are also lower rates of suicide in migrant vs permanent citizens. Taken together with the results of the present study along with those in other countries, it is worth tentatively suggesting that either CALD status may confer some sort of a protective effect from self-harm requiring hospital admission or that there may be potential bias in help-seeking from CALD/migrant groups. However, given that the present study and previous work have been unable to test either possibility, and there is extensive literature on difficulties that migrants experienced in Australia, we suggest that some caution should be made when identifying being CALD as a protective factor for self-harm. The following explanations for the lower rate found in CALD communities should be considered.
First, the smaller rate might be due to the impact of healthy migrant effects (Kennedy et al., 2015) as migration in many ways acts as a selection process that filters out the vulnerable and keeps them healthier resulting in migrants more likely to have a reduced risk of poor mental health and self-harm (Geros et al., 2020; Kwan and Ip, 2007; Lee, 2019). Furthermore, limitations in access to means of self-harm in CALD communities might also contribute to the lower rate. Although self-poisoning by pesticides is relatively common in Asia (Chowdhary et al., 2007), pesticides might not be commonly and readily available in Australia, especially in urban areas. Similarly, pharmaceutical prescribing might be less readily available in CALD groups such as African Americans, Hispanic Americans and Asians (Kelly et al., 2008; Pletcher et al., 2008; Singhal et al., 2016). Additionally, the role of valuing an individual’s body (i.e. one should not damage the body because it belongs to one’s parents in Asians; Liu, 2013) may also discourage self-harm events. Most importantly, there is a possibility that the lower rate might not truly reflect a lower frequency of self-harm in CALD individuals due to underreporting of self-harm data. Specifically, CALD people may not present to hospital following a self-harm episode (perhaps except for more severe cases with urgent need of hospital treatment) or they may be more inclined to report self-harm as unintentionally caused, possibly due to stigma around mental illness and self-harm (De Anstiss and Ziaian, 2010). There might also be other barriers such as discrimination practices, waiting time or scepticism about the effectiveness of treatments. Moreover, although religious activity (relatively common in CALD communities) has been found to be a protective factor against suicidal behaviour, Gearing and Lizardi (2009) revealed that people are less likely to label an incidence as self-harm/suicide if the main religion considers it a sin. Also, there might be bias in data quality on COB reported (Tran et al., 2012). These may all contribute to the lower rate of self-harm hospital admissions in CALD communities identified; however, future research is recommended to test these possibilities.
An additional contribution of the study relates to the differences in the profile of self-harm among the CALD groups and the non-CALD group. Specifically, CALD people who were hospitalised for self-harm were (relatively) more likely to be older, living in Metropolitan Victoria, from the lowest socioeconomic group (by area of residence), and ever or currently married, compared to non-CALD people. A similar pattern of self-harm age distribution in the CALD group has been observed in relation to mental health that some mental illnesses among migrants and refugees were more common in older people (Minas et al., 2008, Nickerson et al., 2019). The finding might be influenced by the effect of the length of stay in Australia of migrants and acculturation: as higher levels of acculturation (longer duration of stay in host countries, and migration at younger age) increase the risks of lifetime self-harm (Perez-Rodriguez et al., 2014).
However, further analysis of CALD subgroups (by ROB) and the non-CALD population also show differences in characteristics of the four CALD self-harm hospital admission subgroups. Particularly, the proportion of total self-harm cases increased with age in the SEE subgroup – the group that had the highest total number of self-harm hospital admissions compared to other CALD subgroups; the 25–34 age group represented the greatest number of self-harm cases in the SCA group, and females were particularly overrepresented in the SEA group. These differences in characteristics among CALD subgroups might be associated with race or ethnicity: for example, self-harm incidence in Asian or Black people has been reported to be different to White people (Bhui et al., 2007; Jablonska et al., 2009). Also, as non-English-speaking European countries are likely to have quite different socio-cultural and political backgrounds, they might have different psychosocial risk factors for self-harm, when compared to other CALD populations such as those from SEA and North-East Asia. Additionally, acculturation and different Australian migration history timelines might also explain the differences by region of birth: European people were one of the first migrants in Australia while Asian people came later after Australian migration policies changed in 1973 to welcome all migrants (Chinese immigration in the Gold Rush [1850s and 1860s] does not affect the CALD population today captured by this study). This study shows that among people admitted to hospital for self-harm, the CALD population is a highly heterogeneous group; therefore, we suggest that collapsing all people from CALD backgrounds into one group is not greatly helpful for understanding self-harm in Victoria, Australia. More importantly, potential opportunities for self-harm prevention would be missed if intervention strategies are only based on what we know about the general CALD group rather than separate CALD subgroups.
In summary, we believe that the relationship between CALD and self-harm is complex and multifactorial requiring further research to explore it; however, it is reasonable to conclude that hospitalisations for self-harm in Victoria occur less commonly among most CALD populations than the compared populations, and different self-harm prevention strategies are likely to be needed for different CALD subpopulations.
Strengths and limitations
This is the first detailed analysis of self-harm hospital admissions among CALD and non-CALD populations in Australia. The study was conducted in Victoria, the state which ranked second highest in terms of the number of non-Australian-born residents.
There are several limitations to the study. First, the total number of admissions by those in the CALD group was relatively small, which precluded more detailed analyses by subgroups of CALD communities. Second, one possible bias is that in the case of self-harm, the number of repeated admissions can be very high (Carroll et al., 2014) leading to the problem of over-recording the number of cases. This study is limited to reporting population-based incidence; it does not take a cohort approach to track repeat occurrences. Third, we only collected data on those who engaged in self-harm and presented at hospitals. Not all self-harm events that occur in the community results in hospital presentation; therefore, the rates presented in this study may be an underestimate of the incidence of self-harm. Fourth, defining CALD status by COB is another limitation because the two important components of CALD definitions including language spoken at home and Indigenous stats were omitted (Pham et al., 2021). Also, due to the small sample size of the Aboriginal and Torres Strait Islander people in Victoria, we included this group in the non-CALD population (based on the definition of CALD by COB), which may relatively increase the incidence of self-harm in the non-CALD group because the rates of self-harm in Aboriginal and Torres Strait Islander people have been reported to be relatively high (Stapelberg et al., 2020).
Finally, in order to compare the risk of self-harm among those from CALD and non-CALD populations, we divided study participants into two groups based on COB. We acknowledge that this categorising method makes the CALD group become a very mixed group (Sawrikar and Katz, 2009) of COB ranging from very low risk to very high risk of self-harm, which might mask some statistical effect on the result. To provide further information about specific CALD groups, we broke down the CALD communities into specific CALD groups based on ROB and compared them to the non-CALD communities (Table 3).
Future research
Future research using linked data to determine the number of people who engaged in self-harm and the risk factors for repeated self-harm is warranted. The complex relationship between health services accessibility of CALD people and self-harm, and whether self-harm was underreported due to cultural factors relating to stigma or barriers to accessing health services should be examined. A community-based survey for self-harm to be done in a culturally responsive way is recommended to have a better understanding of cultural factors related to self-harm (and treatment seeking). Together with this study, such recommended further works will contribute to providing a broader view of self-harm in CALD communities in Australia to inform self-harm prevention strategies.
Conclusion
Although future research is needed to build on the results of this study, the lower rate of self-harm in most CALD populations show that CALD status may confer some kind of protective factor for hospital-admitted self-harm in Victoria, Australia, except for specific CALD communities with higher rates of self-harm hospital admissions such as Sudan, Iran and Kenya. The results also indicate the differences in profiles between CALD and non-CALD self-harm hospital-admitted populations suggesting that self-harm prevention efforts may be more effective if targeted specifically to CALD and non-CALD populations. Also, to maximise its effectiveness in the CALD population, prevention initiatives should be targeted to each separate group by ROB.
Footnotes
Appendix
List of countries with a total number of self-harm cases in 5 years less than 10.

| Country of birth |
|---|
| 1. Papua New Guinea |
| 2. Spain |
| 3. Somalia |
| 4. Switzerland |
| 5. North Korea |
| 6. Finland |
| 7. Albania |
| 8. Korea, Democratic People’s Republic |
| 9. Kuwait |
| 10. Papua New Guinea |
| 11. Somalia |
| 12. Uruguay |
| 13. Belgium |
| 14. Switzerland |
| 15. Austria |
| 16. Czech Republic |
| 17. Montenegro |
| 18. Slovenia |
| 19. Spain |
| 20. Syria |
| 21. Zambia |
| 22. Denmark |
| 23. Eritrea |
| 24. United Arab Emirates |
| 25. Vanuatu |
| 26. Venezuela |
| 27. Bulgaria |
| 28. Cook Islands |
| 29. East Timor |
| 30. Laos |
| 31. Libya |
| 32. Oman |
| 33. Samoa, American |
| 34. Tajikistan |
| 35. Uganda |
| 36. Brunei Darussalam |
| 37. Cote d Ivoire |
| 38. Djibouti |
| 39. Estonia |
| 40. Mexico |
| 41. Peru |
| 42. Seychelles |
| 43. Sierra Leone |
| 44. South America |
| 45. South Sudan |
| 46. Southern Europe |
| 47. Tunisia |
| 48. Uzbekistan |
| 49. Belarus |
| 50. Burundi |
| 51. Central and West Africa |
| 52. Chad |
| 53. Ghana |
| 54. Greenland |
| 55. Guatemala |
| 56. Jamaica |
| 57. Kazakhstan |
| 58. Kosovo |
| 59. Latvia |
| 60. Liberia |
| 61. Macau (SAR of China) |
| 62. Melanesia |
| 63. Middle East |
| 64. Mongolia |
| 65. Namibia |
| 66. Nauru |
| 67. Nicaragua |
| 68. Nigeria |
| 69. Norfolk Island |
| 70. North Africa |
| 71. Slovakia |
| 72. Solomon Islands |
| 73. Spanish North Africa |
| 74. St Vincent and the Grenadines |
| 75. Sub-Saharan Africa |
| 76. Tanzania |
| 77. Tonga |
| 78. Yemen |
Acknowledgements
The authors would like to acknowledge the Victorian Agency for Health Information (VAHI) for providing the self-harm hospital admission data. We would like to thank Dr Dasamal Tharanga Fernando, Monash University Accident Research Centre, Monash University, for her statistical support and Prof. James Harrison at the National Injury Surveillance Unit for providing the SRRs.
Author Contributions
T.T.L.P. and J.B.-G. led the study. T.T.L.P. and J.B.-G. conceived the presented idea, developed the theory, analysed and interpreted the data. T.T.L.P. led the drafting of the manuscript with contributions from all authors on the manuscript. All the authors contributed to the interpretation of the results. All the authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This paper is part of a PhD thesis which is supported by the Injury Prevention Graduate Research Industry Partnership Program under the collaboration between Monash University Accident Research Centre and the Victorian Department of Health.