
Abstract
Background:
Growing evidence suggests that community-based interventions may be effective for anxiety and depression. This study aimed to describe studies of community interventions delivered to adults and/or young people, either in person or online, evaluated in randomised controlled trials and provide an indication as to their effectiveness, acceptability, quality of data and where possible, mechanisms of action. We included interventions delivered at and/or by museums, art galleries, libraries, gardens, music groups/choirs and sports clubs.
Method:
We developed and followed a preregistered protocol: PROSPERO CRD42020204471. Randomised controlled trials in adults and young people were identified in an extensive search with no date/time, language, document type and publication status limitations. Studies were selected according to predetermined eligibility criteria and data independently extracted and then assessed using Risk of Bias 1. The studies were deemed too heterogeneous for meta-analysis and were therefore reported using a narrative synthesis.
Results:
Our analysis included 31 studies, with 2898 participants. Community interventions most studied in randomised controlled trials were community music (12 studies, 1432 participants), community exercise (14 studies, 955 participants) and community gardens/gardening (6 studies, 335 participants). The majority of studies were from high-income countries – many were in specific populations (such as those with physical health problems) and were generally of low quality. Dropout rates across the included studies were low (1 participant on average per 100 participants). The inadequate description of interventions limited identification of potential mechanisms of action.
Discussion:
The uncertainty of the evidence allows only a weak recommendation in support of community interventions for anxiety and depression. The results suggest community engagement is a promising area for wide-reaching interventions to be implemented and evaluated, but more high-quality trials are needed, especially in young people and under-represented communities.
Introduction
Mental disorders are prevalent, preventable and potentially reversible. Mental illness is thought to impact over one in four of the world’s population (Kessler et al., 2009), although this figure is arguably underestimated (Vigo et al., 2016). Interventions available from the healthcare sector do not meet the need arising from common mental disorders, such as anxiety and depression (Alonso et al., 2018; Jorm et al., 2017; Thornicroft et al., 2017).
Healthcare systems do not currently have the capacity to deliver interventions to treat or prevent mental illness to all who would potentially benefit (Campion et al., 2022). An alternative to medical and psychological interventions is engagement with community assets, such as sports, music and singing, museums, arts and gardening. Community-based activities are thought to improve health and well-being by acting as a ‘social cure’ (Sani et al., 2015; Wakefield et al., 2022) and may be cost effective by reducing the use of health care services (Kellezi et al., 2019).
Social prescribing is increasingly used as a means of linking individuals to community-based assets, to support mental health (Daly et al., 2022; Kwong et al., 2021). The evidence base for the effectiveness and cost-effectiveness of social prescribing link workers in primary care for improving physical and mental health outcomes has been challenged in a recent systematic review (Kiely et al., 2022). Although providing a comprehensive overview, scoping reviews on the effect of leisure on health (Fancourt et al., 2021; Fancourt and Finn, 2019) have limitations due to a lack of critical evaluation of study quality or quantitative data synthesis. A more systematic and evidence-based approach is needed, particularly regarding efficacy (Clift, 2020).
Addressing inequalities in healthcare is a global priority (Whitehead, 1992). Young people and under-represented people, such as ethnic minorities, have high and increasing mental health needs (Fink et al., 2015; Knies and Kumari, 2022; Marmot et al., 2012). These groups have been adversely affected by the COVID-19 pandemic, are less likely to access healthcare (Shanahan et al., 2022) and even prior to the pandemic young people were feeling increasingly disconnected from local communities (Rees, 2020). Community-based interventions may reach a broader cross-section of society than clinical interventions (Baskin et al., 2021) and may operate through mechanisms different from or complementary to medical or psychological interventions (Fancourt et al., 2021). Thus, there is a drive to discover the evidence for the effectiveness of strategies not delivered by mental health professionals for anxiety and depression in young people (Wolpert et al., 2019). Although three quarters of mental disorders emerge before the age of 25 years, people aged 16–24 years are least likely to seek help (Andrews et al., 2001; Olfson and Klerman, 1992), many not engaging with conventional interventions, such as medication or talking therapies. In light of this, this review will separately assess the evidence for community intervention in participants of the 16–24 years age range. Investing in community-based initiatives could address the rising need for the intervention and prevention of anxiety and depression for those most in need.
Finally, exploration of community-based resources available digitally is a priority. By developing interventions using digital media, community resources could be utilised more effectively (Bennett et al., 2019). Evidence suggests online delivery is preferable for some groups (Kaihlanen et al., 2022; Rauschenberg et al., 2021) and may overcome barriers to accessing healthcare, and adhering to treatment, measurable by lower dropout rates. Online community-based interventions may be more acceptable for groups previously associated with low help seeking, but this has yet to be evaluated. In addition, digital interventions will continue to be deliverable in future pandemics (Philippe et al., 2022).
This study aimed to describe studies of community interventions delivered to adults and/or young people, either in person or online, evaluated in randomised controlled trials (RCTs) and provide an indication as to their effectiveness, acceptability and quality of the data and where possible, mechanisms of action. We included interventions delivered at and/or by museums, art galleries, libraries, gardens, music groups/choirs and sports clubs.
Questions
Which populations, interventions, comparators and outcomes are evaluated in RCTs of community-based interventions in community-dwelling adults and young people (aged 16 years and over)?
What is the evidence from RCTs for the effectiveness and acceptability of in-person and online community interventions for anxiety and/or depression in adults and young people?
What is the quality of the data?
What mechanisms of action of community interventions are responsible for their effectiveness, as identified in RCTs?
Methods
The protocol for this systematic review was prospectively registered with PROSPERO (CRD42020204471) and written following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline. The authors met after the search and filtering but before full data extraction to discuss the direction of the review, given the large number of studies. Due to the volume of studies, it was decided to include RCTs only, and to exclude studies set in residential care homes or hospital in-patient units. In addition, the review focused on primary mental health outcomes (of anxiety and depression) and dropouts as a measure of acceptability. Outcomes were not assessed using GRADE, since after evaluation of the population, intervention, control and outcomes (PICO) data for the included studies, a quantitative synthesis was deemed not appropriate due to heterogeneity (Schünemann et al., 2013).
Types of study
All relevant RCTs reporting useable data were included. Trials in which randomisation was implied were considered. All quasi-randomised studies were excluded.
Types of intervention
Types of intervention include community-based interventions, online or actual, with or without a key worker (or link worker), on a group or individual basis and including single or multiple sessions. These included interventions delivered at, or by museums, art galleries, libraries, gardens, music/singing groups, youth groups and sports clubs. Interventions based in the workplace or schools and social prescribing, if the intervention involved engagement at or with a community-based resource (in person or online), were included. Comparison interventions could include medication, psychological therapies, treatment as usual (TAU), non-specific or no intervention, waitlist interventions or other community interventions.
Exclusions
Interventions based solely within health services or supported living environments (nursing homes, retirement homes, care homes) or social interventions, such as parenting, employment and financial support were excluded. Interventions which combine medication/psychological therapy with the community intervention were not included unless the additional intervention was also present equally in the control group. The interventions that involved solitary activities (such as watching a movie, reading a book, exercising alone or web-based activities, such as gaming) that were not community delivered or hosted actually or virtually by a community-based entity/organisation were not included.
Types of participants
Types of participants include people aged 16 years or over with anxiety (such as generalised anxiety disorder or social anxiety) or unipolar depression of any severity or in whom the treatment of depression or anxiety, the reduction of symptoms of anxiety or depression or the prevention (primary or secondary) of anxiety or depression was the aim of the study. Participants with levels of psychological distress on a scale deemed to equate with depression and/or anxiety were also included. Anxiety and/or depression could be comorbid with physical health conditions. Studies with a specific focus on treating other mental health conditions, physical health conditions, obsessive-compulsive disorder (OCD) or phobias were excluded. In studies on children, most participants (>50%) must have been 16 years or older.
Types of outcomes
The primary outcome was a clinically important change in symptoms/remission/prevention of depression and/or anxiety as defined by the study. If an outcome was reported for multiple timepoints, all of these were collected. Secondary outcomes were summarised but not evaluated. Dropouts were used as the measure of acceptability, as studies in this area rarely reported adverse events or other measures of acceptability.
Study selection
The eligibility assessment was performed independently in a blind standardised manner by the reviewers (R.S.S., S.M.T., H.B., E.G.O.). Disagreements were resolved by consensus or in consultation with a third reviewer. Reviewers checked for duplicates.
Information sources and search strategy
Search (electronic)
The information specialist (F.S.) searched the Cumulated Index to Nursing and Allied Health Literature (CINAHL), the Cochrane Library (including Cochrane Database of Systematic Reviews [CDSR] and Cochrane Central Register of Controlled Trials [CENTRAL]), Embase, Epistemonikos, MEDLINE and PsycINFO on 21 June 2020 and updated this search on 25 September 2021 with no date/time, language, document type and publication status limitations. A more detailed search method and search strategies per database were reported in Supplemental Appendix Table S6. The search results were de-duplicated in EndNote X6.
Searching other resources
Reference lists of relevant papers were searched and experts in the field were contacted to determine if other studies were available.
Data management
Rayyan was used to sort studies for inclusion and exclusion. Excel was used to manage extracted data.
Review process
Duplicate citations were removed by the information specialist (F.S.) prior to screening for inclusion/exclusion. The senior author (R.S.S.) completed an initial screen to remove clearly ineligible studies due to the high number and clear inappropriateness of many of the studies returned by the search. For example, studies in mice and in vitro lab experiments were ineligible by title alone. This is accepted as pragmatic methodology as in Kiely et al. (2022).
Titles and abstracts of citations identified by the search were independently screened for inclusion according to the predefined PICO criteria. Full-text reports were obtained where necessary. Full texts were screened by two reviewers and disagreements resolved by discussion. Where disagreements remained, a third senior author (E.G.O. or R.S.S.) made the final decision.
Data were extracted into predesigned forms and included citation, language, country, setting, name and a brief description of strategy/intervention, name and a brief description of comparison strategy/intervention, participants (age range, gender, definition of disorder), outcomes (comparative data, however reported, short-, medium- and long-term) and information describing the intervention according to the Template for Intervention Description and Replication (TIDieR; Hoffmann et al., 2016). Any missing information was recorded as incomplete.
Risk of bias and quality assessment
The Cochrane Risk of Bias 1 tool was used to assess bias across the following domains: adequate random sequence generation, concealment of allocation, adequacy of blinding/indirectness of assessment dealing with incomplete data.
Data synthesis strategy
A qualitative synthesis using aggregate data, summary statistics and overall measures of effect was performed. Studies were not sufficiently homogeneous to carry out a quantitative synthesis.
Results
Search and selection of studies
The search identified 24,465 records. After removing 8931 duplicate records, the reviewers (R.S.S., E.G.O., S.M.T., H.B.) screened 15,534 records independently. The process of selection of studies has been recorded in Figure 1.
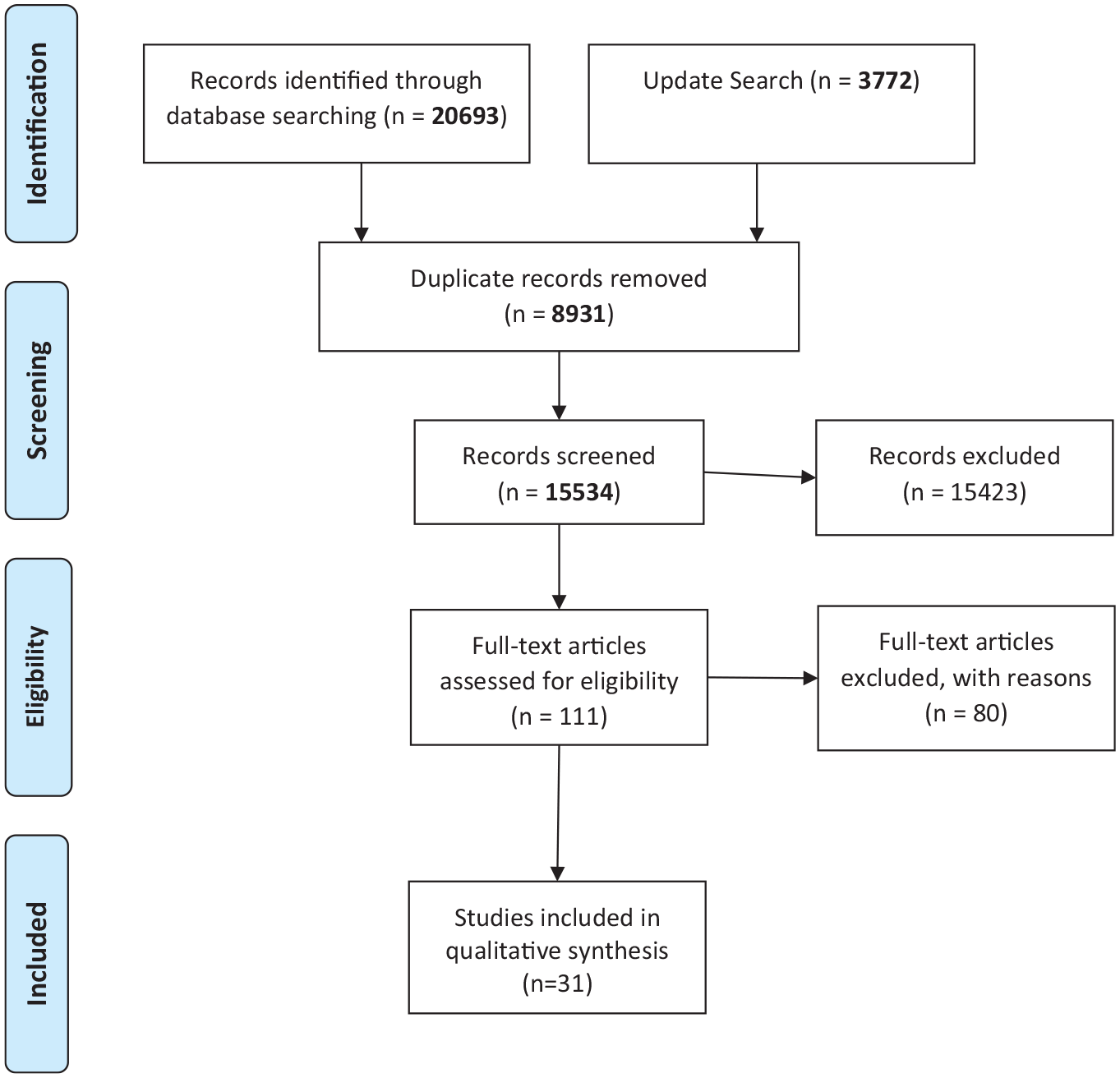
Process of selection of studies for systematic review based on PRISMA flow diagram.
Overall description of studies
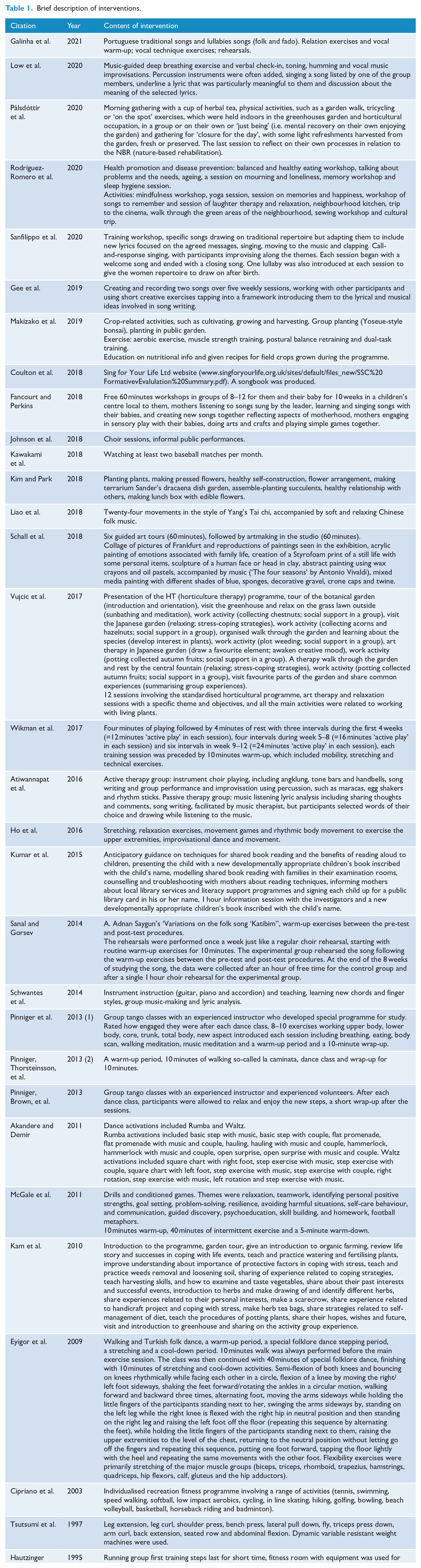
There were 31 studies included (see Table 1 for a brief description of each intervention). The results of studies have been categorised by intervention type for ease of comparison in Table 2. Eighty studies were excluded on the basis of full texts (see Supplemental Appendix 1, Table S1 for the rationale for exclusion). The included studies were not sufficiently homogeneous to conduct a meta-analysis.
Brief description of interventions.
Results of the studies.

SD: standard deviation; CI: confidence interval; TAU: treatment as usual; n/a: not applicable.
Risk of Bias domains: allocation concealment, blinding participants and therapist, blinding assessors, random sequence generation, incomplete outcome reporting, selective reporting and other bias.
Scales: Self-Reporting Questionnaire (SRQ-20), Edinburgh Post-natal Depression Scale (EPDS), Hospital Anxiety and Depression Scale (HADS), The PROMIS emotional distress short forms (SF), The Depression, Anxiety and Stress Scale–21 Items (DASS-21), Geriatric Depression Scale (GDS-15), Beck Depression Inventory (BDI-II), Patient Health Questionnaire (PHQ-8), Center for Epidemiologic Studies Depression Scale (CES-D), The State-Trait Anxiety Inventory (STAI), The Depression Anxiety Stress Scale (DASS20), The Montgomery–Åsberg Depression Rating Scale (MADRS), The Beck Depression Inventory (BDI-IA), The Inventory for Depressive Symptomatology (IDS), Beck Anxiety Inventory (BAI), and Self-Rating Depression Scale (SDS).
No entry indicates study did not adjust.
Type of intervention
Community exercise and community music interventions were the most studied when counting individual studies and total size (by number of participants) (see Figure 2(a) for an overview). The interventions targeted a variety of demographics, and neither of these intervention categories were only applied to one illness or age group across included studies. Outcomes alongside anxiety and depression included cognition, physical health and self-esteem. Music interventions had the greatest number of participants (n = 1432). Sample sizes for music studies were larger than exercise studies, with a mean size of 119. Community exercise studies had a mean size of 68 and a total size of 955. There were six eligible studies which focussed on gardening, with a mean sample size of 56. One RCT included a museum-based intervention, one was set in a library and one in a sports stadium (watching baseball). Some studies assessed interventions combining multiple modalities (Liao et al., 2018; Makizako et al., 2019; Pinniger et al., 2013b; Rodríguez-Romero et al., 2020) or compared two or more types of interventions with each other (Wikman et al., 2017). The content of the interventions has been summarised in Table 1.
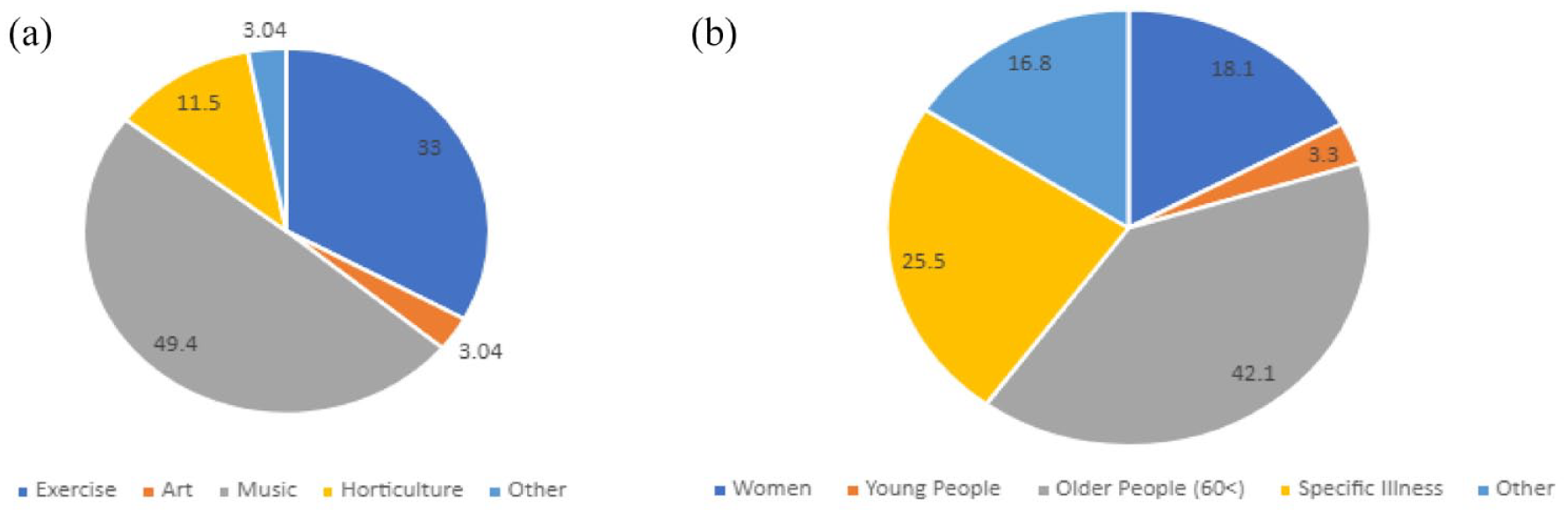
(a) Percentage of participants per study based on the type of intervention assessed. (b) Percentage of participants per demographic studied.
Demographics
Older people were the most studied, with 1222 participants, in over 10 studies. Other highly studied groups were women, with some studies focussing on specific life stages. One study (Sanfilippo et al., 2020) focused on the antenatal period, two on the post-natal period, one on perimenopause and one on older age. Eleven out of the 32 RCTs focused on intervention in an existing illness, with the aim of reducing anxiety or depression. These illnesses were usually chronic/severe mental illnesses, such as major depressive disorder (see Supplemental Appendix Table S3). Other studies focused on chronic pain, dementia or cancer. Young people (aged 16–24 years) were studied least, with only two eligible RCTs, comprising 98 participants in total.
Study location
Most studies have been conducted in western countries and high-income economies. Seven studies were conducted in middle-income countries and one study in a low-income country (Sanfilippo et al., 2020, in The Gambia). Figure 3 shows the distribution of studies by country, with green denoting three or more studies published in that country and grey denoting no eligible RCTs included in this systematic review.
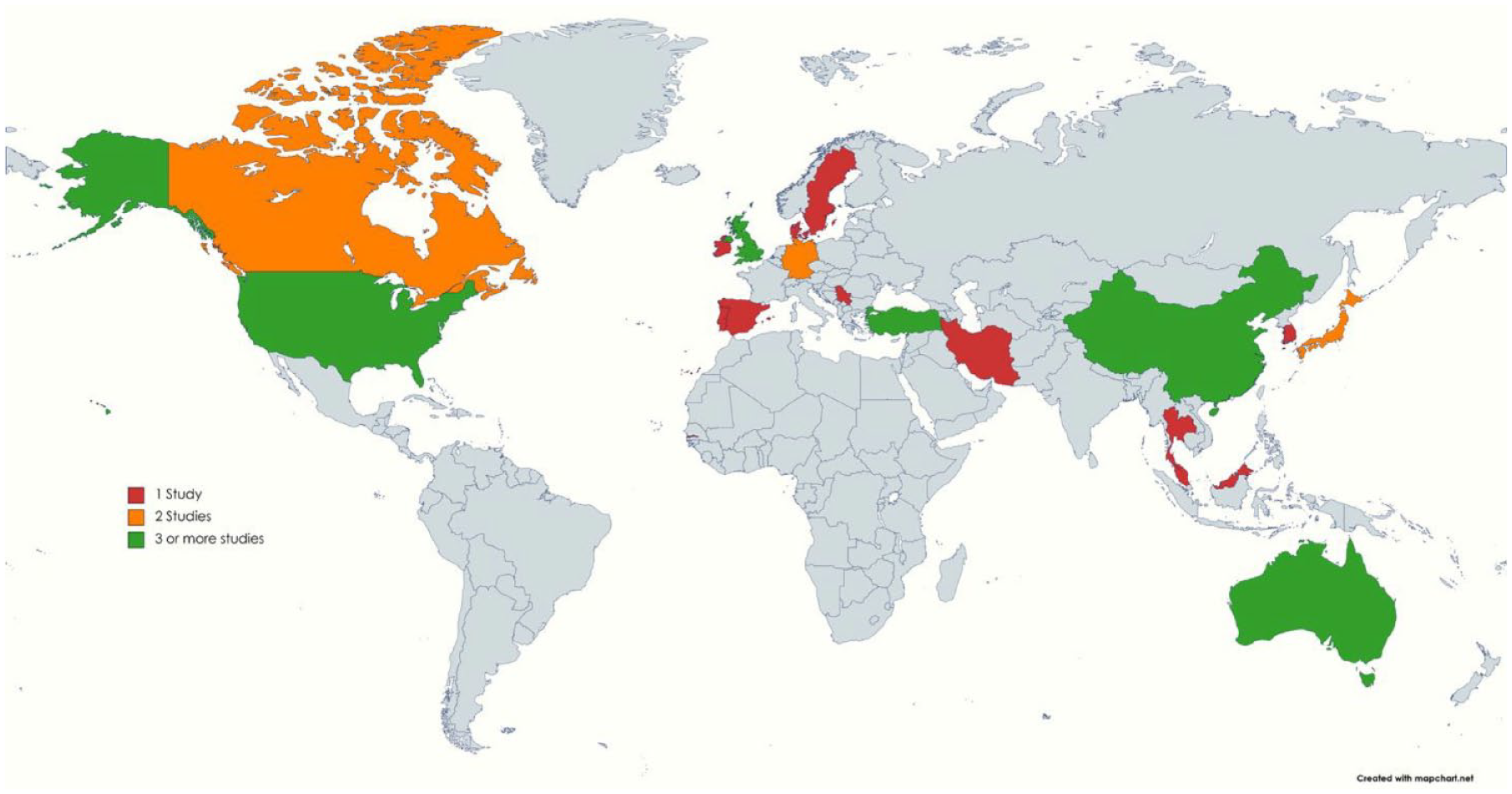
Locations where studies took place. Red denotes one eligible study, orange denotes two eligible studies and green denotes three or more studies.
We have grouped interventions by type (community music, community exercise, community gardening, art, libraries, others, online) in order to describe the studies in more depth (participants, interventions, comparators and outcomes) as well as to describe the evaluation of effectiveness and acceptability of the interventions and quality of the studies.
Community music
Participants, interventions, comparisons and outcomes
There were 12 eligible RCTs. The total number of participants studied was 1432. The average number of participants was 119 (range = 14–390). One study (Gee et al., 2019) was specifically aimed at young people. Two studies did not report raw data. Four RCTs were conducted in middle-income countries. Four studies compared the intervention on depression or anxiety with an ‘active’ control, e.g. group counselling. The studies were not suitable for a meta-analysis or synthesis without meta-analysis (Campbell et al., 2022). The populations studied were heterogeneous, and included rural farming communities, people with chronic pain, healthy older people, women in the antenatal period or women with post-natal depression and young people.
Music interventions included taking part in a choir, therapeutic song writing, interpreting lyrics or playing instruments (see Table 1 for an overview). The interventions were dissimilar, e.g. song writing and choir activity on instrument playing. Comparators included waitlist controls, passive music therapy, usual care, creative play or unstructured choir singing time. Other outcomes assessed included quality of life, neurological and behavioural function, cost-effectiveness, social identification, loneliness and friendship.
Effectiveness, acceptability and quality
Where it was possible to calculate adjusted mean differences, only one study (Schwantes et al., 2014) reported a mean difference in outcome score large enough to be arguably clinically significant as well as statistically significant: Beck Anxiety Inventory (BAI) Average Mean Difference (AMD) −5.37 [−10.6963, −0.0437] and Center for Epidemiological Studies Depression Scale (CES-D) AMD −3.73 [−7.2733, −0.1867]. All studies reported a decrease in anxiety or depression outcome, apart from Galinha et al. (2021) where a non-statistically significant increase in anxiety was reported. The total number of dropouts across the studies was 149, which was 9.61% of the total number of participants. The quality of the individual studies ranged from very low to moderate.
Community exercise
Participants, interventions, comparisons and outcomes (these should come from Table 1)
The total number of participants studied was 955; the mean study size was 68 (range = 17–147). Four studies did not report sufficient raw data (sample sizes, mean values and standard deviation). Three RCTs were conducted in low- or middle-income countries. The RCTs published covered a range of demographics, including older people, women and those with existing mental or physical illnesses. Due to the variety of study designs, and the heterogeneity of the targeted populations and of the tested interventions, we were not able to perform a meta-analysis or synthesis without meta-analysis.
There were 14 eligible RCTs which studied the effect of community exercise on anxiety and depression. These interventions included team sports, yoga classes, group strength training, dance and Tai chi. Comparators included waitlist, TAU, individual exercise activities and progressive muscle relaxation. Other outcomes assessed included physical performance, balance, social connection, pain and sleep quality.
Effectiveness, acceptability and quality
Of the studies that presented enough data to calculate AMD with 95% confidence interval (CI), two studies reported clinically significant decreases in Beck Depression Inventory (BDI) scores for the intervention arm: McGale et al. (2011) AMD −6.62 [−8.0288, −5.2122] and Akandere and Demir (2011), AMD −3.58 [−6.4255, −0.7345]. Most studies reported decreased depression outcomes, apart from Hautzinger and Kleine (1995) where the control group had markedly low scores both pre- and post-test. Studies rarely reported significant decreases in anxiety for exercise interventions. The total number of dropouts across the studies was 80 which was 1.13% of the total size. In some cases, dropouts were not reported. Many studies did not describe the methodology in sufficient detail to draw conclusions about quality (see Supplemental Appendix Figures S2 and S3 for the Risk of Bias assessment).
Community gardens/gardening
Participants, interventions, comparisons and outcomes
There were six eligible studies on gardening in a community setting. The total number of participants overall was 335, with a mean size of 68 (range = 24–101). Two studies did not report sufficient raw data. One RCT was performed in a middle-income country. The studies were not suitable for a meta-analysis or synthesis without meta-analysis (Campbell et al., 2022). The populations studied were heterogeneous, and included psychiatric inpatients, stroke patients, healthy older people and perimenopausal women.
Interventions included visiting botanical gardens, growing plants and learning about psychological theories while engaging in horticultural practices. Two studies combined horticulture with other therapies (Makizako et al., 2019; Rodríguez-Romero et al. 2020). The interventions were dissimilar (see Table 1 for a description of each intervention). The comparators were also varied; controls included alternative workshops, art therapy, TAU or waitlist control. The outcome raw data were in some cases not reported (Vujcic et al., 2017) or used scales only relevant to a specific group, e.g. the Geriatric Depression Scale. Other than anxiety and depression, other outcomes assessed by the studies included personal well-being, work behaviour, menopausal symptoms, Dignan’s ego identity, disability and mental fatigue.
Effectiveness, acceptability and quality
One study reported clinically and statistically significant change in outcome for the intervention group (Kim and Park, 2018): the State-Trait Anxiety Inventory (STAI) AMD −12.7 [−17.7352, −7.6648] and the Self-Rating Depression Scale (SDS) AMD −4.4 [−6.4502, −2.3498]. All studies reported a decrease in depression score for the horticultural therapy group, as did the studies that reported anxiety scores. The total number of dropouts across the studies was 13 which is less than 0.5% of the total number of participants studied (see Table 1 for a description of the studies and Supplemental Appendix Figures S2 and S3 for the Risk of Bias assessment).
Art
There was a single eligible RCT on the role of art and culture (Schall et al., 2018). This study compared participants with dementia and their caregivers visiting an art gallery, with a waitlist control. The focus of the study was the effect of the museum visits on cognition, mood and quality of life. The study found no significant change in depressive symptoms in the museum intervention group compared with the control. Raw data were not reported. The dropout rate was 96, with 88 participants included in the final analysis. Reasons given for the dropouts included serious illness, death and residential placement. The quality of the evidence was low, due to attrition and performance bias (see Supplemental Appendix Figures S2 and S3 for the Risk of Bias Assessment).
Libraries
Kumar et al. (2015) studied the effect of an intervention involving reading in libraries with adolescent mothers compared to routine clinical care on depressive symptoms (in the mother) and infant reading behaviour and subjective reading enjoyment. The total number of participants analysed was 28 dyads, with one dropout per group. The results demonstrated a clinically significant reduction in the number of participants fulfilling the criteria for depression (Beck Depression Inventory [BDI-IA] >10). The strength of recommendation for the evidence for depression reduction was moderate, since the effect size was large, despite a small sample size and a high risk of bias.
Others
Kawakami et al. (2019) studied the effects of watching baseball on depressive symptoms in older people. Other outcomes assessed were executive and cognitive functioning, health-related quality of life, subjective happiness and physical activity. The total number of participants was 58, with no dropouts. The control was a waitlist control. The results demonstrated a reduction in CES-D score in the intervention group compared to the control (intervention group; median change = −2, interquartile range [IQR] −4 to −0, control group; median change = 0, IQR = −4 to −2). The study did not report sufficient raw data (no standard deviations). The quality of the study was moderate/low due to inadequate blinding.
Online studies
A few online studies of community interventions have been published. Since the COVID-19 pandemic, online delivery of interventions has become more frequent. Despite this, no published studies or ongoing studies of community online interventions were eligible for this SR.
Ongoing studies
There were nine eligible RCTs which were ongoing (see Supplemental Table S2 for ongoing studies in Appendix). We contacted the authors for data on 15 March 2022, but either there was no response or the data were not yet available.
Targeted interventions
Some studies assessed interventions that were culturally or age-specific to the participants included. There were six culturally specific interventions, six age-specific interventions and one study which was age and culture specific. Cultural interventions included traditional music, Tai chi and other cultural dances, such as Turkish folklore dance. Age-specific interventions included life review techniques, reflection on menopause or music from the participants’ youth. Only two studies were targeted at young people (see Supplemental Appendix Figure S1 for proportions of studies).
Mechanisms of action
We used the TIDieR checklist (Hoffman et al., 2016) to assess the reporting of the content of interventions (see Supplemental Appendix Table S4). Most studies did not report sufficient information about the components or duration or frequency of interventions, and characteristics of who was delivering the intervention, the facilities or the location of the intervention were generally not clearly described. Only one study reported whether or not the intervention had been modified during the study. Sixteen out of 31 studies described some assessments of treatment adherence. A few studies identified a rationale or potential mechanisms of action or embedded analysis of dosing into their study design for the assessment of efficacy. No studies elicited whether mechanisms of action for an effective intervention differ depending on the target group’s socio-economic or other demographic characteristics.
Discussion
Trials of community-based interventions on anxiety and depression appear to be feasible but currently focus narrowly on specific populations and intervention types. Those most studied include the elderly (>60), women (during different life stages and in general) and those with pre-existing physical or mental health conditions. The vast majority took place in high-income countries. Types of intervention most researched were community music and community sports, with relatively fewer studies on museums/arts, libraries or gardening. While it is encouraging that such studies appear to be feasible, trials are rare in populations with high unmet mental health need, such as young people or in low- and middle-income countries (LMIC) settings. Experimental research of potentially promising interventions such as culture and the arts or gardening has been relatively neglected. While some interventions demonstrated promising efficacy, most were not described in sufficient detail to replicate or draw inferences regarding dose or mechanism of effect. Importantly, it is unclear if the experience itself or the community aspect potentially improving human connection was efficacious. In addition, studies were small (median n = 59, mean n = 92, IQR = 69) and had a high risk of bias, mainly due to performance bias (systematic differences between the groups other than only the intervention), incomplete outcome reporting and inadequate controls. Nine studies did not report sufficient raw data. In some cases, there was insufficient information about the conduct of the study to allow for reliable risk of bias assessment across multiple domains. In general, the interventions appeared to be acceptable, with the mean dropout size of 11.66 across the 29 studies that reported dropouts, which comes to a 10% mean dropout rate across all studies included in this review. However, other measures of acceptability were rarely used.
Community music interventions were well studied, with the largest combined size of the modalities included. A few studies reported clinically significant changes in anxiety or depression. The majority of the studies were of low quality. Therefore, we were unable to draw firm conclusions about the effectiveness of community music interventions for anxiety or depression. A previous Cochrane systematic review has found that music therapy and TAU is superior to TAU only in depressive disorder, but with little effect on anxiety (Aalbers et al., 2017). This Cochrane review was not specific to community-based interventions, although some group music therapy interventions were included. All interventions were delivered by trained therapists or health professionals; in contrast, in this current review, the profession of the intervention deliverer was not an exclusion criterion.
Trials of interventions utilising community exercise were relatively more common than other community intervention categories, accounting for 47% (15/32) of included RCTs. Many studies had small numbers of participants, low rates of blinding and incomplete outcome reporting; therefore, the overall the quality of evidence for community exercise interventions was low. Notably higher quality studies demonstrated a dose–response effect of the intervention on the outcomes measured, such as McGale et al. (2011). Individual exercise therapy has been suggested to have a moderate effect on depression (Cooney et al., 2013). One form of community exercise, group dance movement therapy, has been systematically reviewed but not studied well enough for reliable estimates of efficacy (Meekums et al., 2015). The evidence base for exercise therapies in young people with depression or anxiety is scarce and inconclusive (Larun et al., 2006; Wolpert et al., 2019). Other studies have demonstrated that community exercise may overcome barriers to help seeking particularly in young males (Swann et al., 2018). Our review suggests that community exercise could be a promising means of reducing depression and anxiety across a variety of demographics but requires higher quality intervention research.
There were a few RCTs in many potentially efficacious community-based interventions, such as gardening, arts, libraries or other cultural modalities. We were unable to draw any conclusions on the effectiveness of these interventions. At the time of writing there have been no systematic reviews of gardens/gardening for anxiety or depression, apart from in the elderly (Gramaglia et al., 2021). Importantly, this review was specific to long-term care residents, and not the community setting. There is some evidence that horticultural therapy mediates its effect through social connectedness (Ng et al., 2021). Therefore, horticulture may be well-suited to community settings.
Highlighted in this review is the potential for community-based interventions to target under-represented groups, as well as young people. Marginalised young people often do not seek help from health services (Cauce et al., 2002; Rickwood et al., 2007; Stunden et al., 2020). Therefore, given that social prescribing takes place in primary care, they would miss out on being referred to a link worker who could potentially signpost them to appropriate support.
We found that 13/32 RCTs included interventions which were culturally specific or age specific to the population targeted. Elements of the interventions were sometime co-produced, e.g. Low et al. (2019) demonstrated high engagement with minority groups (79% self-identified as Black). Co-production and cultural or generational relevance may be key to engagement in community-based intervention in minorities and those at either end of the life cycle. A scoping review of community-based interventions to improve mental health in minority communities concluded that there is insufficient evaluation and argued that we must understand better how the interventions work (Baskin et al., 2021). Finally, it is unclear if the interventions work best when they are ‘matched’ to their target population, as argued by Stuart et al. (2022) or if an effective intervention will work regardless of the age/ethnicity/gender previous interests of the people taking part, as suggested by Fancourt et al. (2021).
Strengths
This systematic review is the first to assess community-based interventions for anxiety and depression. It includes articles published from any timepoint, in any language. We performed a second search and screened grey literature databases. As such our results provide a comprehensive overview of trialled interventions to treat and prevent anxiety and depression.
Limitations
The review process may have missed articles and did not include quasi-randomised trials, reports, cohort studies or case–control trials. We were unable to perform a meta-analysis due to the heterogeneity of the included studies. Some studies did not provide sufficient data to include outcome data in the quantitative summary, which may have limited the accuracy of our results. The nature of the studies included affects our conclusions. There is a systematic bias due to the understandable impossibility of blinding participants to the intervention, it is not possible to conclude from our studies the size of this bias. Most interventions were not adequately described which severely restricts any conclusions regarding dose or mechanism of action. Other aspects increased risk of bias, such as incomplete outcome reporting and some studies with high attrition rates. We did not formally assess for publication bias.
The lack of information regarding the mechanism by which these interventions work means that we cannot yet suggest what is needed for an effective community intervention or whether this could be equally effective when delivered online. In addition, there was little assessment of cultural aspects of mental health and well-being, especially in relation to community and identity. It is possible that effective community interventions rely on being culturally coherent to the participants involved.
Implications
It is clear from our review that young people and minority groups are under-represented in the studies. In the context of increasingly recognised mental health problems, and the potential benefits of early intervention, these groups should be studied more (Moran et al., 2022). Online interventions have the potential to reach under-served or vulnerable people. Despite this, online interventions utilising community-based resources have not been well studied. The co-produced online museum–based intervention (Syed Sheriff et al., 2021) demonstrates proof-of concept for future work in this area.
There is ample evidence that studies focussing on ‘WEIRD’ (Western, educated, industrialised, rich and democratic) populations do not generalise well (Henrich et al., 2010). The RCTs in this review were mostly centred on high-income countries. Nevertheless, it is possible to deliver a community-based intervention in LMICs, as demonstrated by Sanfilippo et al. (2020). Future work should prioritise studies in non-WEIRD populations.
Furthermore, due to insufficient description of the interventions used, the ‘dose’ and mechanisms of action were difficult to evaluate. Further studies are needed to assess the mechanisms by which interventions are effective, and how best to deliver interventions. It is unclear if interventions work regardless of the target population, or if they need to be age and culture specific, or ‘matched’ to the interests of the individual. No studies have asked the following questions: Do community interventions work regardless of severity of an individual’s mental illness? Are they most effective as an early intervention, primary prevention or rehabilitation? Do we need to match the intervention to the population for it to be effective? Which are suited to social prescribing?
Future studies in this area should be randomised control trials and should clearly define, as per the TIDieR checklist, the components of the community intervention. Studies should discuss what training the investigators delivering the intervention require and provide links to the resources used. Ideally, they should be culturally or life stage specific or aim to determine whether this is important. More direct measures of treatment effect might also be considered. Populations with high unmet mental health needs such as young people and minority groups should be studied, and online delivery should be considered. Moreover, there is a need for theoretical frameworks to inform what works best in which populations and contexts.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221150362 – Supplemental material for Community interventions for anxiety and depression in adults and young people: A systematic review
Supplemental material, sj-docx-1-anp-10.1177_00048674221150362 for Community interventions for anxiety and depression in adults and young people: A systematic review by Hadassah Buechner, Sureyya M Toparlak, Edoardo G Ostinelli, Farhad Shokraneh, Jessica Nicholls-Mindlin, Andrea Cipriani, John R Geddes and Rebecca Syed Sheriff in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors acknowledge Ms Verity Abbots, Ms Thandiwe Hoggarth and Ms Taneesha Jones-Seale from the Oxford Health NHS Foundation Trust, Warneford Hospital, Oxford, OX3 7JX, UK. The authors also acknowledge Andrew Przybylski from the Oxford Internet Institute, University of Oxford, 1 St Giles, Oxford, OX1 3JS, UK. The authors acknowledge and thank the following medical students, who extracted some of the articles, Joseph Milton, Leenah Abuelgasim and Neginsadat Mirtorabi.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: E.G.O. has received research and consultancy fees from Angelini Pharma. A.C. has received research and consultancy fees from INCiPiT (Italian Network for Paediatric Trials), CARIPLO Foundation and Angelini Pharma. H.B., R.S.S., F.S. and S.M.T. do not have any conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research study was supported by COVID-19 Research Response Fund. R.S.S. was supported by the National Institute for Health Research (NIHR) Oxford Health Biomedical Research Centre (grant BRC-1215-20005) and by the NIHR Research Professorship awarded to Professor Andrea Cipriani (grant RP-2017-08-ST2-006). E.G.O. was funded by the NIHR Research Professorship to Professor Andrea Cipriani (grant RP-2017-08-ST2-006), by the NIHR Applied Research Collaboration Oxford and Thames Valley (ARC OxTV) at Oxford Health NHS Foundation Trust, by the NIHR Oxford cognitive health Clinical Research Facility and by the NIHR Oxford Health Biomedical Research Centre (grant BRC-1215-20005). The views expressed are those of the authors and not necessarily those of the UK National Health Service, the NIHR or the UK Department of Health and Social Care.
Registration and Protocol
This study was prospectively registered with PROSPERO 2020: CRD42020204471.
Availability of Data
On request from the corresponding authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.