
Abstract
Objective:
Depression has been identified as a priority disorder among children and adolescents. While numerous reviews have examined the individual and family factors that contribute to child and adolescent depressive symptoms, less is known about community-level risk and protective factors. The aim of this study was to complete a systematic review to identify community risk and protective factors for depression in school-aged children (4–18 years).
Method:
The review adopted the procedures recommended by the Cochrane Non-Randomised Studies Methods Working Group and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A comprehensive literature search was conducted to identify both observational and intervention study designs in both peer-reviewed and non-peer reviewed publications.
Results:
A total of 21 studies met the inclusion criteria. Seventeen of the 18 community association studies and 2 of the 3 intervention studies reported one or more significant effects. Results indicated that community safety and community minority ethnicity and discrimination act as risk factors for depressive symptoms in school-aged children. Community disadvantage failed to achieve significance in meta-analytic results but findings suggest that the role of disadvantage may be influenced by other factors. Community connectedness was also not directly associated with depressive symptoms.
Conclusion:
There is evidence that a number of potentially modifiable community-level risk and protective factors influence child and adolescent depressive symptoms suggesting the importance of continuing research and intervention efforts at the community-level.
Keywords
Introduction
Worldwide, approximately 5% of adolescents suffer from depression (Costello et al., 2006; World Health Organisation [WHO], 2012). Adolescence is considered a period of high risk for the onset of psychopathology (Spear, 2000). In the United States, approximately 75% of mental disorders present before the age of 24, and 50% begin before the age of 14 (Kessler et al., 2005). Adolescent depression has also been identified as a predictor for depression in adulthood (Lewinsohn and Essau, 2002). Retrospective studies of depressed adults and prospective studies of adolescents indicate that depression often emerges during the mid-adolescent (13–15 years) period of development (Hankin et al., 1998; Lewinsohn and Essau, 2002). Longitudinal evidence suggests more pronounced increases in the incidence of major depressive disorder after age 11 and again after age 15, with rates levelling in young adulthood (Kim-Cohen et al., 2003). Expanding knowledge relevant to the life-course development and aetiology of internalising problems in childhood and adolescence suggest these periods in development as opportune times for intervention (Letcher et al., 2009).
Depressive disorders are identified as the leading contributor to the burden of disease and injury for children and adolescents (Gore et al., 2011; WHO, 2012). Some studies suggest that medical expenditure on children with depression is significantly higher in comparison to children with other mental health conditions (Glied and Neufeld, 2001; Mandell et al., 2003). For this age group, depression is associated with a number of negative outcomes including academic difficulties, impaired social relationships, high-risk sexual behaviour and a 30-fold increased risk of completed suicide (Horowitz and Garber, 2006). Adolescents with depressive disorders are also at high risk for legal problems, exposure to negative life events (American Academy of Child and Adolescent Psychiatry [AACAP], 2007), as well as adolescent pregnancy and early parenthood (Jaycox et al., 2009). A high proportion of adolescents who experience depression will also experience another mental disorder (commonly a substance-use, anxiety or behavioural disorder), as well as an increased likelihood of developing other chronic illnesses (Bhatia and Bhatia, 2007). The effects of adolescent depression extend beyond the individual. Parents of depressed adolescents report lower parent mood and increased strain (Jaycox et al., 2009).
Due to its prevalence and association with impairment and long-term consequences, depression has been identified as an international priority (WHO, 2012). Historically, efforts to reduce the impact of mental illness have focussed on the treatment of intra-psychic elements of individuals (Herrman et al., 2005). However, even in a perfect health care system, modelling suggests that only 35% of the burden of affective disorders could be averted through optimal treatment (Andrews et al., 2004). The unchanging pattern of prevalence rate trends in recent years suggests the current approach of increasing treatment investment has had little success at reducing the significant burden of mental disorders (Jorm and Reavley, 2012; Reavley et al., 2011). In order to reduce the prevalence of depression, prevention approaches are needed.
Emerging evidence suggests that preventative approaches offer a cost-effective solution to reducing the economic burden of mental illness (Mihalopoulos and Chatterton, 2015; Mihalopoulos et al., 2012; Muñoz et al., 2010). Furthermore, evidence indicates that high quality, comprehensive programmes delivered in collaboration with schools and communities can not only improve child mental health but also lead to improved general health, social functioning and academic and work performance (Barry et al., 2009). Intervening at the community-level holds substantial promise as it affords an opportunity to affect whole populations (Rose, 1992, 2001).
Mental health promotion aims to modify determinants of mental health in order to improve the mental health and well-being of populations, communities or individuals (Commonwealth Department of Health and Aged Care [CDHAC], Mental Health and Special Programs Branch, 2000; Keleher and Armstrong, 2005). It is generally achieved through the implementation of multiple evidence-based interventions across a number of programmes, settings, sectors and policies (Keleher and Armstrong, 2005). These interventions aim to reduce risk factors and increase protective factors, in all areas of influence – individual, family, school and community (Beaglehole and Bonita, 2009).
The impact of individual-, peer- and family-level factors on child and adolescent depression is frequently reported in the literature (Cairns et al., 2014; McLeod et al., 2007; Twenge and Nolen-Hoeksema, 2002; Yap et al., 2014). Meta-analytic findings indicate sound evidence for a number of individual-/peer-level factors including relationship with positive peers, alcohol and other drug use, adaptive stress coping, sleep, weight and dieting (Cairns et al., 2014). Meta-analytic findings also suggest family conflict, parental over involvement, parental warmth, parental hostility and a number of other parenting factors are associated with adolescent depression (McLeod et al., 2007; Yap et al., 2014). Similarly, meta-analytic evidence suggests that the school environment also exerts a significant influence on depression in school-aged children. Adolescents’ perceptions of school connectedness (Kidger et al., 2012), teacher support (Kidger et al., 2012) and school attainment (Riglin et al., 2014) are associated with adolescent depression. School bullying has also been associated with later depression (Ttofi et al., 2011).
The research examining community-level risk and protective factors is less organised. There has only been one meta-analysis or review in this area. A meta-analysis that examined the impact of community violence exposure on mental health outcomes (Fowler et al., 2009) identified that community violence was associated with increased internalising symptoms.
Little is known about what other community-level factors may influence the development of adolescent depression. While socio-economic status is frequently implicated as a risk factor for child and adolescent depression (Herrman et al., 2005; McDermott et al., 2010), there appears to be limited evidence to support these claims. Indeed, a meta-analysis of individual-level variables did not support socio-economic status as a moderator of childhood depression (Twenge and Nolen-Hoeksema, 2002). To date, the existing literature relevant to community risk and protective factor impacts on child and adolescent depression is disorganised, providing an overall limited evidence base to advance researchers and policy makers. This study aims to identify what community risk and protective factors influence the development of depression in school-aged children (4–18 years).
Numerous reviews support the effectiveness of preventative interventions in adolescent samples (Calear and Christensen, 2010; Horowitz and Garber, 2006; Merry et al., 2011). Early findings suggested that selective and indicated interventions were more effective than universal programmes in the prevention of child and adolescent depression (Horowitz and Garber, 2006). Some researchers argued that due to the limited evidence supporting the effectiveness of universal interventions offered in school settings, it would be premature to disseminate these interventions more widely (Spence and Shortt, 2007). Policy makers suggested that further research is required to identify effective universal approaches (McDermott et al., 2010).
However, a Cochrane Review later suggested that universal approaches are effective in reducing depression (Merry et al., 2011). These findings were replicated in a review of school-based randomised controlled trials (RCTs) (Corrieri et al., 2013). Furthermore, a meta-analysis of 32 RCTs, including both adult and adolescent populations, indicated no difference in the effectiveness of interventions based on the type of approach (universal, selective or indicated) implemented (Van Zoonen et al., 2014). Overall evidence suggests that universal approaches offer cost-effective means of reducing the prevalence of depression.
Current preventative interventions have been criticised for being more focussed on treatment and early intervention than prevention, usually only targeting individual-level factors despite calls for the use of multimodal approaches (AACAP, 2007; Corrieri et al., 2014; Horowitz and Garber, 2006; Spence and Shortt, 2007). The majority of current preventative interventions are Cognitive Behavioural Therapy (CBT), Interpersonal Therapy (IPT) or psycho-education based and are offered in school settings (Calear and Christensen, 2010; Merry et al., 2011; Neil and Christensen, 2007; Van Zoonen et al., 2014). Brief interventions that only target individual-level factors such as improving problem solving skills will likely be insufficient to produce lasting effects in reducing the prevalence of depression (Spence and Shortt, 2007).
Furthermore, to achieve population-level reductions in depression, it is necessary to address the underlying determinants of mental health through coordinated responses across a range of services and settings (Jacka and Reavley, 2014; Jorm, 2014). Population-level approaches are needed to reduce community prevalence rates. Such approaches have proven to be effective in Australia in minimising the impact of other health outcomes such as suicide and smoking (Jorm, 2014). However, there is limited understanding of community-level predictors of adolescent depression that could be targeted through such approaches. Furthermore, there are no known reviews of community interventions targeting risk and protective factors for adolescent depression.
The purpose of this study was to complete a systematic review of community risk and protective factors for depressive symptoms in school-aged children (4–18 years). The study adopted a broad scope examining both observational and intervention study designs in both peer-reviewed and non-reviewed publications and used the procedures recommended by the Cochrane Non-Randomised Studies Methods Working Group (Reeves et al., 2011).
Methods
Search strategy and bias
Due to the nature of health promotion, terminology is often imprecise and studies may be found in a variety of electronic databases (Beahler et al., 2000). As such, a broad range of search terms (see Appendix A) were developed based on current meta-analyses and reviews in the topic area (e.g. Merry et al., 2011; Thomson et al., 2006). Using these search terms, an extensive search was conducted through the EbscoHost MegaFILE Premier Facility across the following databases: Education Research Complete, E-Journals, Humanities International Complete, PsycARTICLES, PsycEXTRA, Psychology and Behavioural Sciences Collection, PsycINFO, Social Work Abstracts and Urban Studies Abstracts. After reviewing articles identified in the initial search, a more specific list of search terms was generated and five further searches were carried out (see Appendix B-F). Database searches included unpublished theses.
Armstrong et al. (2011) and Beahler et al. (2000) suggest that additional search strategies, other than database searching, should be employed to locate non-peer reviewed studies (grey literature). A time-limited grey literature search was conducted, including a search of a number of government and community websites (see Appendix G). In addition, current meta-analyses and reviews in the areas of child and adolescent depression, health promotion and community interventions were located and reference lists reviewed (e.g. Barrera et al., 2007; Cuijpers et al., 2006; Horowitz and Garber, 2006; Keleher and Armstrong, 2005; Perry et al., 2010; Sellström and Bremberg, 2006; Stice et al., 2009; Suter and Bruns, 2009; Thomson et al., 2006; Twenge and Nolen-Hoeksema, 2002). Furthermore, the reference lists of included studies were reviewed to identify potential studies. The main search was carried out over a three-month period from July to October, 2012. The extensive search conducted minimised any potential problems of fugitive literature; the issue of failing to include hard-to-locate articles (Rosenthal, 1995).
Eligibility criteria
Studies in languages other than English, unless appropriately translated, were excluded from this analysis. Given that prevention research in this area is relatively new and prior reviews in this area have not identified studies before this time (Fowler et al., 2009; Centre for Allied Health Evidence, 2009), all searches were restricted to studies after 1992. In order to minimise potential bias in study inclusion, the following pre-determined inclusion and exclusion criteria were established.
School age participants
Participants had to be between the ages of 4–18 years at the time the outcome variable was assessed.
Depressive symptom variable
The study had to include a valid measure of childhood depressive symptoms (e.g. self-report of depressive symptoms) or participants had to be diagnosed through clinical interview with a depressive disorder (e.g. Major Depressive Episode). For the purpose of this study, depressive symptoms included: dysthymia, major depressive disorder, mood disorders, depressive symptoms, internalising symptoms or disorders and emotional symptoms or disorders. Studies that did not disaggregate internalising but only provided a combined score of internalising and externalising behaviours (e.g. Child Behaviour Checklist [CBCL] total internalising and externalising problem behaviours) were excluded from the study. Retrospective accounts of depressive symptoms (i.e. adults reporting on their depressive symptoms as a child) were also excluded.
Community-level factors
The study had to examine either community-level risk or protective factors, or an intervention targeting community risk and protective factors. The study had to include a community measure (e.g. Index of Relative Disadvantage) or individual report (e.g. Children’s Report of Exposure to Violence) of a community-level variable or compare depressive symptoms across two distinct communities (e.g. community affected by political violence and a community not affected by political violence). Alternatively, studies examining the effectiveness of a community-level intervention needed to assess an intervention aimed at addressing a community risk or protective factor (e.g. intervention increasing socio-economic status). In this review, the term community refers to the environment external to the individual, family and school settings.
Studies included in previous meta-analyses
The decision was made to exclude studies that exclusively examined school-level variables or the effectiveness of school-level interventions, given the extensive research conducted in this area (e.g. Kidger et al., 2012; Merry et al., 2011). At the time, the literature search was conducted, the only review/meta-analysis examining community-level factors associated with children’s internalising symptoms was Fowler et al.’s (2009) meta-analysis. Fowler et al. (2009) conducted a comprehensive meta-analysis on the effect of community violence on internalising symptoms. Fowler et al.’s (2009) study included studies up to 2007. As such, the decision was made to search for community violence studies 2007 and after, to identify research that may add to existing findings.
Relevant statistical comparison
The relationship between the predictor variable and the outcome variable had to be tested statistically. Studies that only reported unadjusted prevalence rates (e.g. 10% children from low-socio-economic communities had depression and 11% of children from high socio-economic communities had depression) were excluded from this analysis.
Study quality and bias
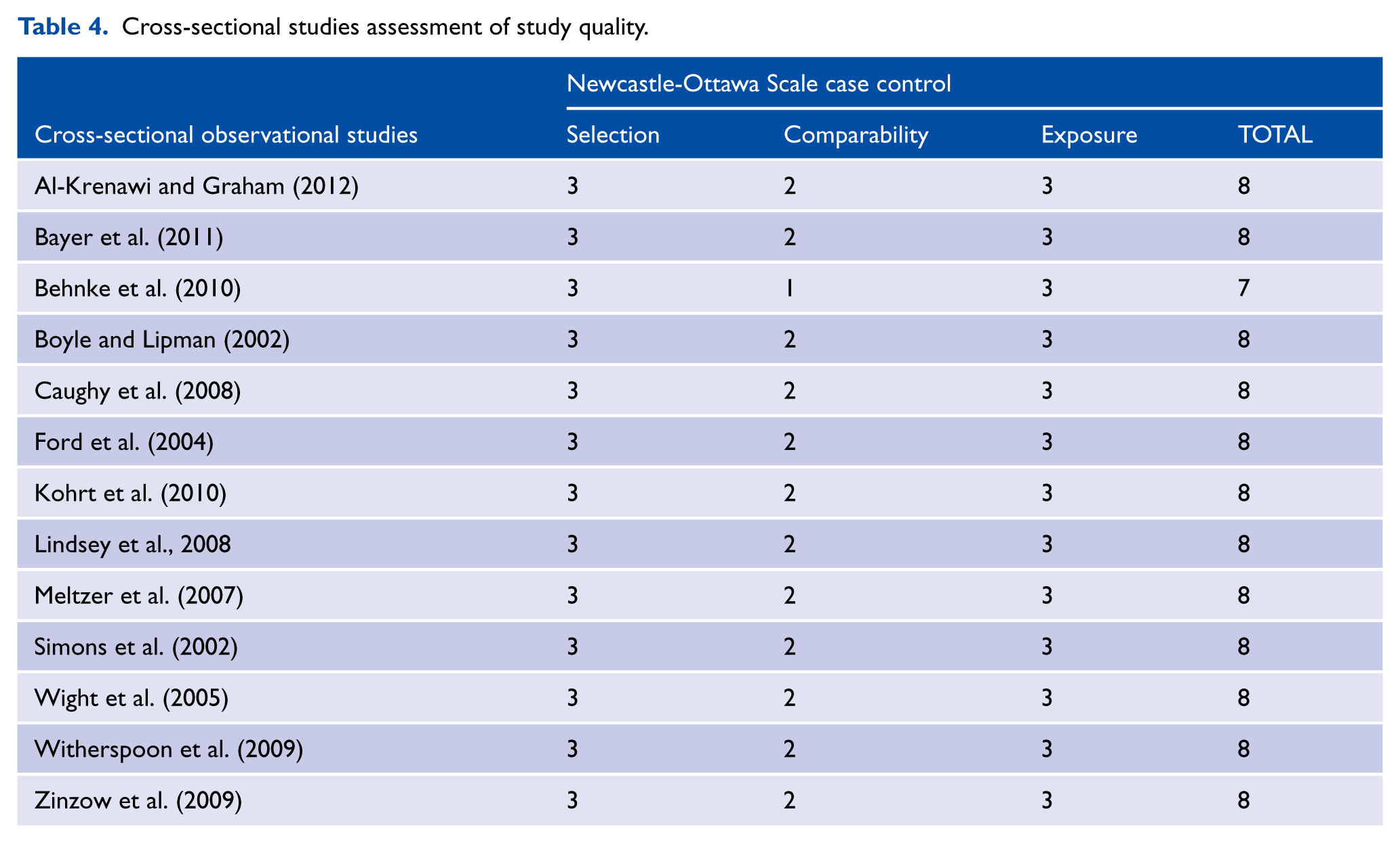
The quality of studies was assessed using the validated Newcastle-Ottawa Scale (NOS: Wells et al., 2008) in accordance with the Cochrane Non-Randomised Studies Methods Working Group (Reeves et al., 2011). The NOS evaluates the quality of non-randomised studies, including cohort and case-control studies using a ‘star’ rating system to judge the quality of a study and potential for within study bias. Ratings are applied over three areas: the selection of study groups, the comparability of the groups, and the ascertainment of either the exposure or outcome of interest for case-control or cohort studies respectively. The maximum numbers of stars a study may receive over these categories are four, two and three respectively to produce a combined maximum score of nine. The raters met prior to assessing studies to discuss any discrepancies in their interpretation of the assessment tool. Question 4 of the NOS scale states that controls with previous occurrences of the outcome of interest should be excluded. Given the participants are children and adolescents, the decision was made to not remove a star if studies did not assess and exclude previous occurrences of depression.
Data extraction, analysis and reporting bias
This study employed systematic strategies to identify and appraise relevant studies to ensure quality and limit potential bias, in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Liberati et al., 2009) and the Cochrane Non-Randomised Studies Methods Working Group (Reeves et al., 2011). Each individual study was independently reviewed by a minimum of two authors. There were some minor disagreements between raters, but these were clarified by consensus. After discussions, the inter-rater agreement was 100%.
Given the heterogeneity of study designs, measures and analyses in the included studies, it was not appropriate to pursue traditional methods of using effect sizes to calculate meta-analytic results. Following previous reviews of adolescent mental health that examined similar heterogeneous literature (Ryan et al., 2010; Yap et al., 2014), we adopted Stouffer’s method. Stouffer’s method was used to combine p-values and determine whether the synthesised results were significant (Becker, 1994). Stouffer’s z was calculated by dividing the sum of the z (Pi) values by the square root of k, where k is the number of included studies. Where possible, included studies were grouped into themes and a meta-analysis was completed reporting sample effect size and p-values. Where no exact p-value was provided, conservative estimates were adopted. For example, if a study stated an effect was p < 0.05, it was estimated at p = 0.049. Effect sizes were conservatively estimated based on the p-value and analytic sample size.
Results
Study selection and bias
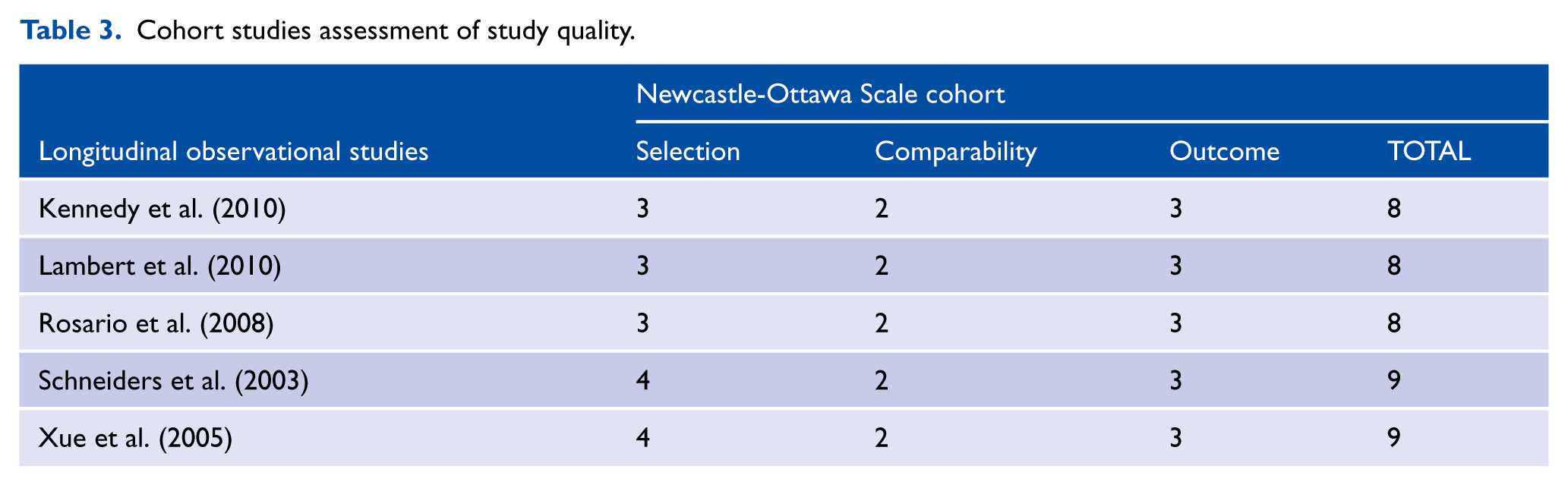
The literature search (see Figure 1) identified 21 studies that met the inclusion criteria (see Tables 1 and 2). For a full reference list of the studies that were considered for inclusion but ultimately excluded from this study, see Appendix H. Thirty-eight percent of the included studies were retrieved through the grey literature search, thus reducing the likelihood of publication bias in this study (Armstrong et al., 2011). The NOS scale was used to identify potential within study bias (see Tables 3 and 4). Overall, included studies were of high quality and received the following star ratings: 7 stars (k = 1), 8 stars (k = 15) and 9 stars (k = 2).
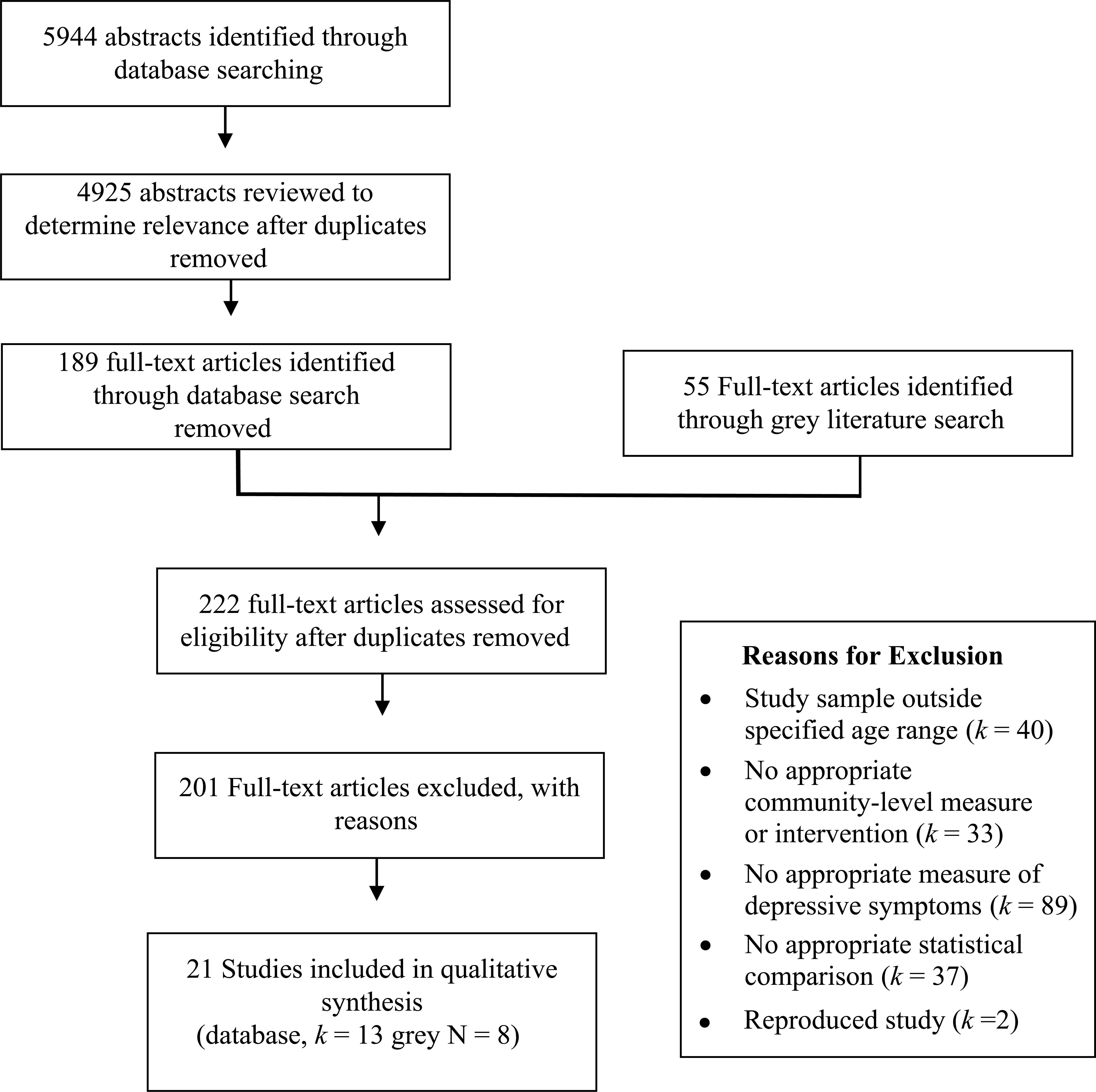
Flow diagram for article selection.
Findings from observational studies examining community-level risk and protective factors.
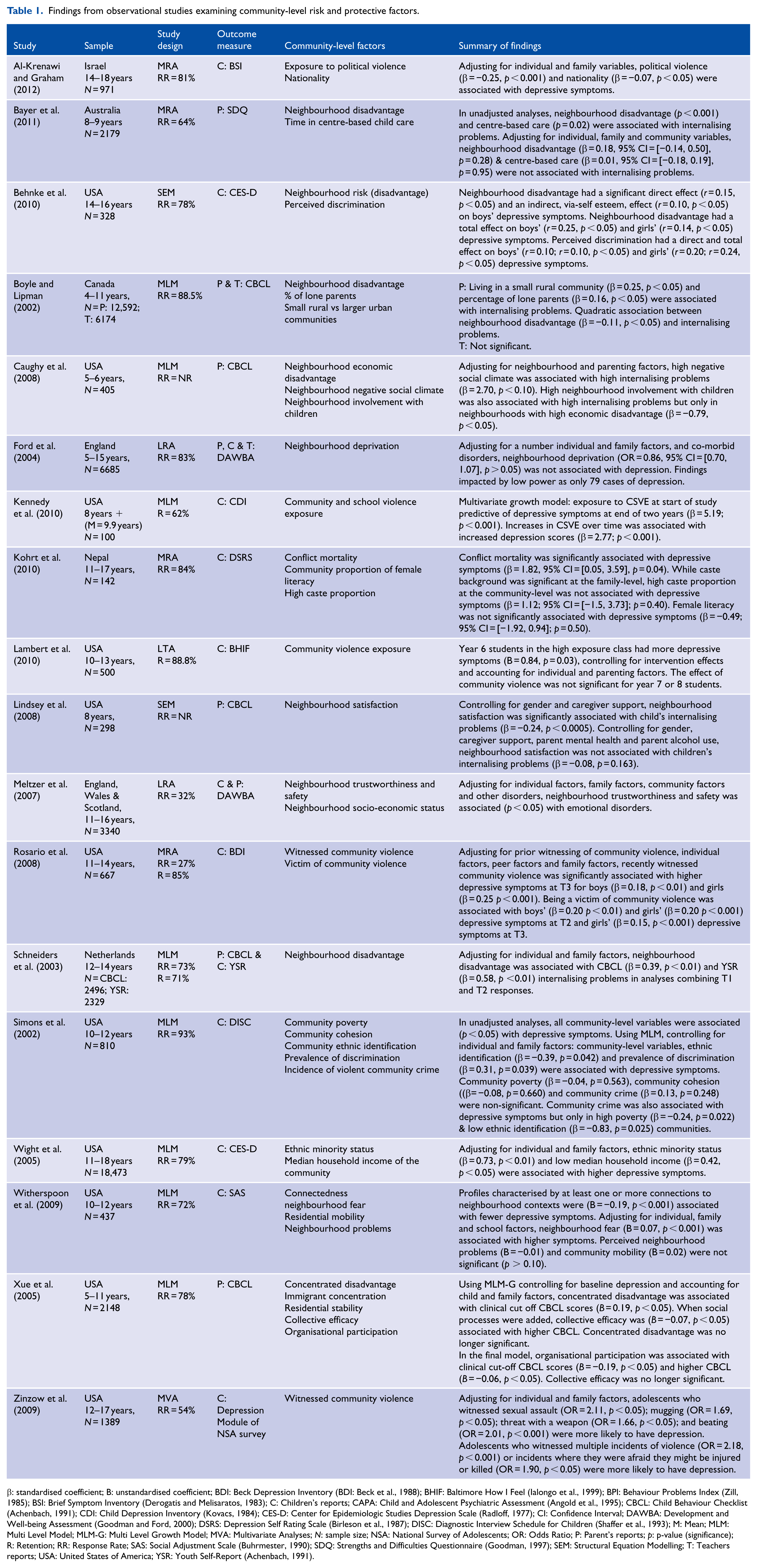
β: standardised coefficient; B: unstandardised coefficient; BDI: Beck Depression Inventory (BDI: Beck et al., 1988); BHIF: Baltimore How I Feel (Ialongo et al., 1999); BPI: Behaviour Problems Index (Zill, 1985); BSI: Brief Symptom Inventory (Derogatis and Melisaratos, 1983); C: Children’s reports; CAPA: Child and Adolescent Psychiatric Assessment (Angold et al., 1995); CBCL: Child Behaviour Checklist (Achenbach, 1991); CDI: Child Depression Inventory (Kovacs, 1984); CES-D: Center for Epidemiologic Studies Depression Scale (Radloff, 1977); CI: Confidence Interval; DAWBA: Development and Well-being Assessment (Goodman and Ford, 2000); DSRS: Depression Self Rating Scale (Birleson et al., 1987); DISC: Diagnostic Interview Schedule for Children (Shaffer et al., 1993); M: Mean; MLM: Multi Level Model; MLM-G: Multi Level Growth Model; MVA: Multivariate Analyses; N: sample size; NSA: National Survey of Adolescents; OR: Odds Ratio; P: Parent’s reports; p: p-value (significance); R: Retention; RR: Response Rate; SAS: Social Adjustment Scale (Buhrmester, 1990); SDQ: Strengths and Difficulties Questionnaire (Goodman, 1997); SEM: Structural Equation Modelling; T: Teachers reports; USA: United States of America; YSR: Youth Self-Report (Achenbach, 1991).
Findings from studies assessing the effectiveness of community interventions.
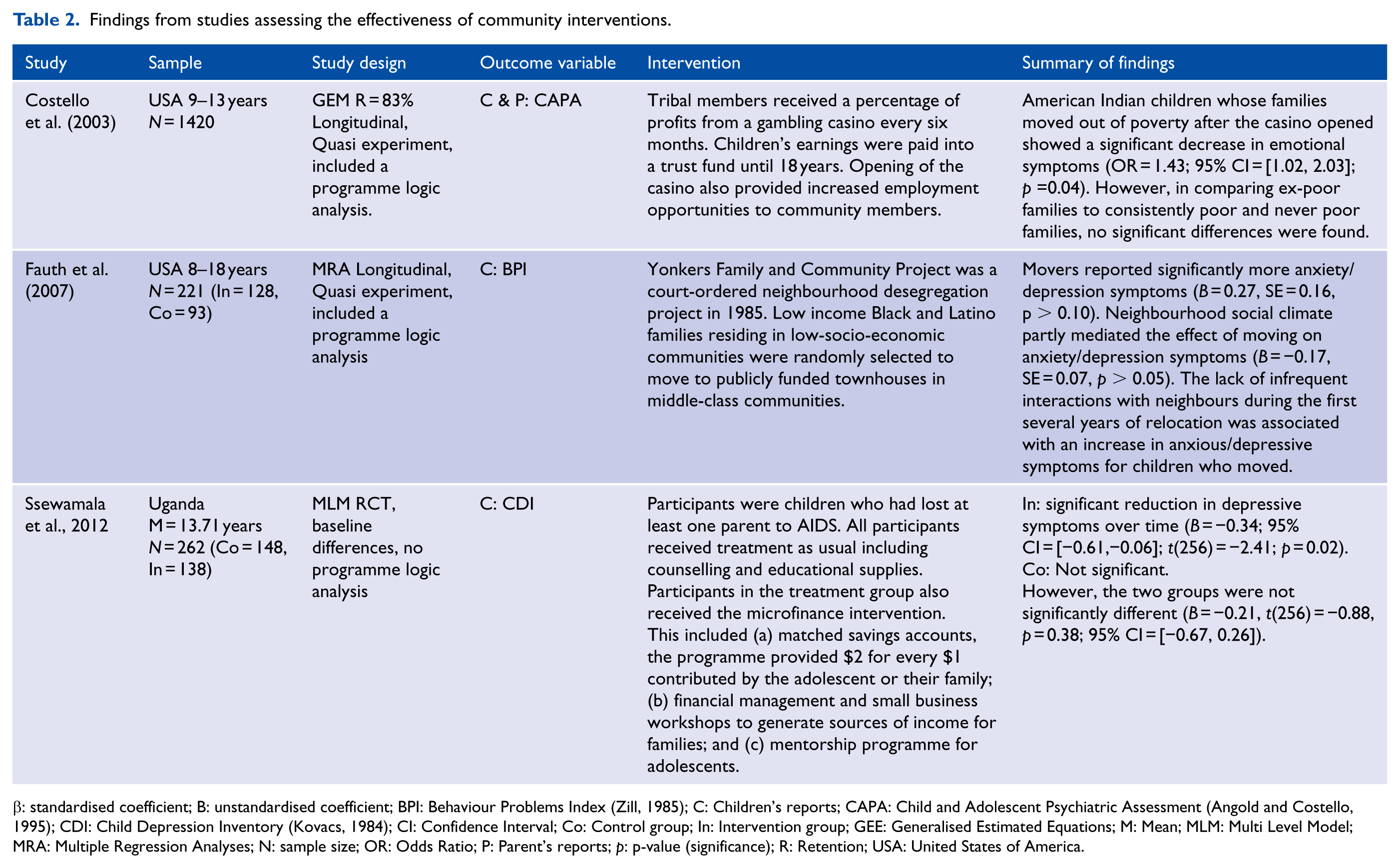
β: standardised coefficient; B: unstandardised coefficient; BPI: Behaviour Problems Index (Zill, 1985); C: Children’s reports; CAPA: Child and Adolescent Psychiatric Assessment (Angold and Costello, 1995); CDI: Child Depression Inventory (Kovacs, 1984); CI: Confidence Interval; Co: Control group; In: Intervention group; GEE: Generalised Estimated Equations; M: Mean; MLM: Multi Level Model; MRA: Multiple Regression Analyses; N: sample size; OR: Odds Ratio; P: Parent’s reports; p: p-value (significance); R: Retention; USA: United States of America.
Cohort studies assessment of study quality.
Cross-sectional studies assessment of study quality.
Participants
All studies included in the review used independent data sets. The total number of participants included in this review was 55,655 (range = 100 to 18, 473). Studies were conducted in the following countries: Australia (k = 1), Canada (k = 1), Israel (k = 1), Nepal (k = 1), Netherlands (k = 1), Uganda (k = 1), United Kingdom (k = 2) and the United States of America (k = 13). The majority of studies examining community risk and protective factors included samples of participants that were representative of the general population (k = 9).
Observational studies that examined sub-sets of the population (k = 9) included the following: children from politically violent areas in the Gaza Strip and West Bank (Al-Krenawi and Graham, 2012), children of Latin American background (Behnke et al., 2010), children of mothers exposed to partner violence (Kennedy et al., 2010), child soldiers of war (Kohrt et al., 2010); children of African American background (Lambert et al., 2010; Simons et al., 2002), children of African American background who are at risk of or have been abused (Lindsey et al., 2008), children from Hispanic and African American backgrounds (Rosario et al., 2008) and children from low-socio-economic backgrounds (Witherspoon et al., 2009). Details of participants in studies examining community interventions are provided in Table 4.
Depression outcome variables
The majority of studies used self-report measures. Only four studies used clinical interviews to assess child and adolescent depression. Depressive symptom measures were rated by or based on the reports of children (k = 12), parents (k = 4), both child and parent (k = 3), both parent and teachers (k = 1) and parent, child and teachers (k = 1).
Studies examined the following outcome variables: depressive symptoms (k = 10), depressive and anxiety symptoms (k = 1), internalising symptoms (k = 6), emotional disorder symptoms (k = 1) and depressive and emotional disorders (k = 3). Fourteen different measures were used to measure depression; the most common was the CBCL (Achenbach, 1991; [k = 5]).
Community risk and protective factors
Studies included in the review identified a number of community risk and protective factors that were grouped into four categories. The sections that follow consider the three risk factors (community disadvantage, community safety and community minority ethnicity and discrimination) and one protective factor (community connectedness). In this review, community disadvantage refers to communities of lower socio-economic status. The majority of studies assessing the impact of disadvantage used measures that assessed multiple domains (e.g. rate of unemployment, mean household income). Community safety refers to safety within the community. The majority of studies assessed an individual’s perception of community safety on domains such as witnessing violence, whether individuals felt safe in their neighbourhood and perceptions of crime. Community minority ethnicity and discrimination included studies that examined communities with high levels of individuals from culturally and linguistically diverse backgrounds and communities with high levels of perceived discrimination. Community connectedness refers to an individual’s perceived connection to their community and includes measures of social cohesion, community involvement and attachment to community.
Community disadvantage
Nine observational studies (Bayer et al., 2011; Behnke et al., 2010; Boyle and Lipman, 2002; Caughy et al., 2008; Ford et al., 2004; Schneiders et al., 2003; Simons et al., 2002; Wight et al., 2005; Xue et al., 2005) included a community measure of disadvantage. Using the Stouffer method, the combined effect on child depressive symptoms across all studies was not significant (N = 46,171, p = 0.073, Effect Size [ES] = 0.025). The differences and distinctions of the individual studies are discussed in more detail below.
Four studies reported direct significant effects. Three studies, using representative samples, identified a significant association between community disadvantage and increased levels of depressive symptoms (4–11 years: Boyle and Lipman, 2002; 12–14 years: Schneiders et al., 2003; 11–18 years: Wight et al., 2005). Similarly, a study of Latin American adolescents (14–16 years) identified that neighbourhood disadvantage had a significant total effect on boys and girls (Behnke et al., 2010).
The findings of a number of studies suggested that the effects of community disadvantage may be mediated through other factors. Bayer et al. (2011) identified a significant association between internalising problems and neighbourhood disadvantage in unadjusted analyses; however, in accounting for a large number of risk factors using multivariate regression, no significant relationship was maintained. Some studies suggested that the impact of community disadvantage may be influenced by other community-level variables. Simons et al.’s (2002) study of African American children (10–12years) suggested that community safety was only significantly associated with increased depressive symptoms in poor communities. Caughy et al. (2008) identified that neighbourhood involvement with children was significantly associated with children’s (5–6 years) internalising problems, but only in disadvantaged communities. Another study, that used multi-level modelling in a representative sample, identified that community disadvantage was significant until community social processes were added, and then community disadvantage was no longer significant (Xue et al., 2005).
Community safety
A total of nine observational studies (Al-Krenawi and Graham, 2012; Caughy et al., 2008; Kennedy et al., 2010; Kohrt et al., 2010; Lambert et al., 2010; Meltzer et al., 2007; Rosario et al., 2008; Witherspoon et al., 2009; Zinzow et al., 2009) included individual reports of community safety. Using the Stouffer method, the combined effect on child depressive symptoms was significant (N = 7951, p = 0.027, ES = 0.069). The differences and distinctions of the individual studies are discussed in more detail below.
Eight studies identified that low community safety was directly associated with increased depressive symptoms. Some studies suggested that the impact of community safety on child depressive symptoms may also vary by other community-level variables such as community disadvantage and ethnic identification. In a study of African American children (10–13 years), the majority of whom resided in urban settings with violent crime rates that exceeded national averages, high exposure to community violence was associated with significantly more depressive symptoms (Lambert et al., 2010).
Community minority ethnicity and discrimination
Six observational studies (Al-Krenawi and Graham, 2012; Behnke et al., 2010; Kohrt et al., 2010; Simons et al., 2002; Wight et al., 2005; Xue et al., 2005) utilised both self-report and community measures of minority ethnicity or discrimination. Using the Stouffer method, the combined effect on child depressive symptoms was significant (N = 22,872, p = 0.028, ES = 0.041). The differences and distinctions of the individual studies are discussed in more detail below.
Four identified that high community minority ethnicity and discrimination were directly associated with increased depressive symptoms. The findings of two multivariate analyses suggest that the effects of community minority ethnicity may be mediated through other factors. A representative sample that used multi-level modelling to control for a large number of individual and family variables did not identify a significant association between immigrant concentration and younger children’s (5–11 years) internalising problems (Xue et al., 2005). Similarly, applying multivariate regression models to control for village clusters and accounting for a range of individual and family variables, no significant association was identified between high caste proportion and depressive symptoms in adolescent (11–17 years) soldiers of war (Kohrt et al., 2010).
Community connectedness
Four observational studies (Caughy et al., 2008; Simons et al., 2002; Witherspoon et al., 2009; Xue et al., 2005) used individual reports of community connectedness. Using the Stouffer method, the combined effect on child depressive symptoms was not significant (N = 3800, p = 0.241, ES = 0.051). The differences and distinctions of the individual studies are discussed in more detail below.
One study, of children (10–12 years) from disadvantaged communities reported that high neighbourhood connectedness was directly associated with significantly fewer depressive symptoms (Witherspoon et al., 2009). The findings of this study and the other three studies suggest that the effects of community connectedness may be mediated through other factors, such as other community-level variables. In a representative sample of children (5–11 years), informal social control and social cohesion were significantly associated with higher internalising symptoms, but after adding organisational participation to the model, social control and cohesion were no longer significant (Xue et al., 2005). A study of African American middle-aged children (10–12 years: Simons et al., 2002) identified significant associations between community connectedness and depressive symptoms in an unadjusted analysis, but relationships were not significant in the adjusted analysis. Caughy et al. (2008) identified that high neighbourhood potential for community involvement with children was significantly associated with children’s (5–6 years) internalising problems, but only in disadvantaged communities.
Other community factors
There is some evidence that children may fare less well in remote and poorly organised communities. A study of Canadian children utilising a representative sample, indicated that children (4–11 years) from small remote communities had higher levels of internalising symptoms than children from large urban communities (Boyle and Lipman, 2002). In a representative sample of children (5–11 years), residents’ involvement in local organisations was significantly associated with lower CBCL scores (Xue et al., 2005). Six separate studies examining time in centre-based care, residential stability, residential mobility, neighbourhood problems, neighbourhood satisfaction and female literacy did not identify any significant associations with depressive symptoms.
Community intervention studies addressing disadvantage
Three intervention studies examined effects of poverty alleviation on child emotional disorder symptoms or depression. One reported significant effects; however, using the Stouffer method, the combined effect on child depressive symptoms was not significant (N = 1903, p = 0.055, ES = 0.127).
However, the interventions were not homogenous in content. One intervention relocated families from disadvantaged communities into middle-class communities, another was a microfinance intervention for children who had lost a parent from AIDS. The third intervention provided financial gains and employment opportunities to parents after a casino opened in a native Indian reserve.
Discussion
Summary of evidence
This report presents the first systematic review and meta-analyses of studies that have investigated associations between community factors and depressive symptoms in school-aged children (4–18 years). The meta-analyses revealed significant effects in the observational studies for community safety and community minority ethnicity and discrimination. Effects failed to reach significance for the observational studies of community connectedness, community disadvantage and for the three intervention studies examining effects of alleviating disadvantage. Seventeen of the 18 observation studies and two of the three intervention studies reported one or more significant effects.
Similar to the findings of a meta-analysis assessing the association between exposure to violence outside the home and mental health outcomes (0–25 years: Fowler et al., 2009), this study confirmed a significant association between community safety and depressive symptoms in school-aged children (4–18 years). Fowler et al. (2009) identified that community violence exposure had a moderate significant overall effect on young people’s internalising symptoms (d = 0.45, 95% CI = [0.44, 0.47], k = 82, N = 25,960). The effect size was substantially higher than that of this study (ES = 0.069, p = 0.027, k = 9, N = 7951). There are a number of potential reasons for this. First, Fowler et al. (2009) utilised unadjusted correlations from studies to calculate an overall effect size, whereas this study reported adjusted effect sizes that accounted for a large number of covariates. Second, the Stouffer method adopted in this study likely produced a more conservative estimate of the overall effect size.
Third, Fowler and colleagues’ inclusion criteria differed to that of this review in: including studies with an older age group (participants up to 25 years of age), and also adopting a broader definition of community violence including any violence that occurred outside the home including school violence and shootings.
While minority ethnicity has been identified as an individual-level risk factor in policy documents (McDermott et al., 2010), to date, there has been no systematic review on the impact of minority ethnicity and discrimination at the community-level. This study identified a significant association between community minority ethnicity and discrimination and depressive symptoms in school-aged children.
A growing body of research supports the association between community disadvantage and a range of developmental, physical and mental health outcomes for children and adolescents (Brooks-Gunn and Duncan, 1997). While meta-analytic results did not achieve significance, given the conservative estimates adopted using Stouffer’s method, these results should be interpreted with caution. Effect sizes were estimated at 0.025 for the observational studies and at 0.127 for the intervention studies suggesting that findings would likely be significant in larger samples. Findings from a number of the included studies suggested that community disadvantage may influence the role of other community-level factors (e.g. community connectedness and community minority ethnicity and discrimination).
There has also been limited prior research systematically reviewing the association between community connectedness and depressive symptoms in school-aged children. Meta-analytic findings in this study did not reach significance. However, as there were only four studies included in the analysis, caution is advised in interpreting these results. The effect size was estimated at 0.049, suggesting effects would be significant with a larger sample size. Furthermore, some of the included studies indicated that the impact of community connectedness on depressive symptoms may be mediated by other factors such as community disadvantage. Indeed, one community intervention indicated that children relocated from disadvantaged communities into middle-class communities who had little social interaction with their neighbours experienced greater levels of depressive symptoms (Fauth et al., 2007). Such findings highlight that while it is evident that community-level variables act as risk and protective factors for depression in school-aged children, greater understanding of the process of how community-level factors impact depressive symptoms is required.
Limitations
A potential limitation of this review was that only one of the included studies was an RCT (Ssewamala et al., 2012). A second limitation of the current evidence base was the heterogeneous range of community-level outcomes and measures, depressive symptom outcomes and measures and analysis used across studies. This heterogeneity led to difficulties comparing findings and limits the conclusions that can be drawn, particularly in terms of generalisability. The exclusion of non-validated measures of community-level and depression outcomes also limited this review, as 61% of studies were excluded for these reasons. This particularly restricted the number of intervention studies included in the current analysis. A third limitation of this review was the limited range of potential community influences that have been investigated in the included studies. A fourth limitation is that relatively few studies have been well integrated with literature and theories relevant to the development of child and adolescent depression. A fifth limitation of this study was the use of Stouffer’s method to determine effect sizes. In this study, conservative estimates were adopted for studies that did not provide exact significance values, thus producing the lower bounds of effects sizes because of this. It is likely that some non-significant findings would be significant in larger samples. A final limitation of this study was time and resource constraints. Given that 38% of the included studies were retrieved through the grey literature search, the availability of further search time may have revealed additional studies.
Future research
While stakeholders identify the areas of prevention, children and adolescents and affective disorders as priority areas for research, there is little funding supporting preventative research for children and adolescents (Christensen et al., 2013). Considering the increasing prevalence, high costs and poor outcomes associated with childhood depression, further observational studies are recommended to address the limitations of the current evidence base. Given the difficulties and ethical constraints associated with randomising individuals to communities and communities to interventions, population and longitudinal studies offer the next highest level of evidence to evaluate the effect of community-level variables on childhood depressive symptoms. Future research should give careful consideration to study design to minimise the heterogeneous nature of research in this area, and support the development of a robust evidence base.
The use of psychometrically validated mental health and community-level measures is advised. The use of sub-clinical outcomes in epidemiology research is recommended due to difficulties with power when using clinical diagnoses (Ford et al., 2004). Furthermore, the significant negative outcomes associated with sub-clinical symptoms (González-Tejera et al., 2005; Lewinsohn et al., 2004) and the importance of early intervention calls for further research examining sub-clinical presentations. Depressive symptoms in children and adolescents are frequently co-morbid with anxiety symptoms (AACAP, 2007; Angold et al., 1999) and indeed in school-aged children, anxiety is frequently a precursor to depression (McDermott et al., 2010). Given the similarities in presentation and treatment of internalising symptoms in school-aged children, the use of measures that assess overall internalising symptoms (e.g. CBCL and Strengths and Difficulties Questionnaire [SDQ]) is suggested for future research. Future research should also utilise widely used psychometrically valid measures to assess community-level variables.
Studies included in this review also used a wide variety of analytic methods. Not all studies controlled for individual, family and other community-level variables. It is important that analyses account for variation between communities and adjust for multiple risk and protective factors in the one analysis to identify true effects. It is suggested that future research utilise appropriate statistical analyses relevant to examining variables at the community-level such as multi-level modelling.
This study considered a limited number of community factors that may influence child and adolescent depression. For example, there were no studies examining effects of community opportunities for physical activity or for improved nutrition. Community variables to consider in future research identified through the literature search include: availability of local services; community-levels of child abuse and neglect, community attitudes to child discipline, built environment characteristics, the impact of natural disasters, and availability of open space and opportunities for physical activity. Again, based on excluded studies, community interventions that could be evaluated in future research include: neighbourhood investment and regeneration programmes, coordination between child welfare and mental health services, policy changes such as the 4-year-old kindergarten universal access programme and early developmental interventions that may subsequently impact depression in school-aged children such as facilitated playgroups, early attachment initiatives and infant mental health programmes in at-risk populations such as disadvantaged communities.
Relatively few studies in this review were well integrated with literature and theories relevant to the development of child and adolescent depression. As one example, efforts to reduce the impact of economic disadvantage on child depressive symptoms may benefit by being better integrated with developmental theories. Developmental theory and some evidence in the present review would imply that community disadvantage and safety may act indirectly, for example, by disrupting mother–child bonding. Thus, relevant child mental health promotion efforts may be better directed at protecting mother–child bonding in disadvantaged families (Letcher et al., 2009).
Indeed, the findings of the current meta-analysis indicate that community variables act as risk and protective factors for depression in school-aged children. Future research would benefit from understanding the process by which this occurs. For example, one of the studies in this review suggested that small remote communities may act as a risk factor for depression in school-aged children. Given the geographic spread of communities in countries such as Australia, Canada, the United States and China, further research in this area is relevant. It may be useful to compare small remote indigenous and non-indigenous communities as well as examine how access to services may impact depressive symptoms in rural areas. While not as relevant to developed nations, international research could assess the impact female literacy, an important indicator of community gender equality, has on depressive symptoms. In examining the impact of community-levels of female literacy, it may be important to assess how this impacts self-esteem and in turn depressive symptoms.
Clinical and policy implications
Given the high prevalence and significant long-term impacts and costs associated with child and adolescent depression, there has been a significant shift in recent years towards prevention and early intervention by researchers, governments, mental health services and policy makers. The lack of systematic research on community-level factors influencing child and adolescent depression has been noted in policy documents (McDermott et al., 2010). This study provides a significant contribution to the field of child and adolescent depression by identifying and quantifying a number of potentially modifiable community risk and protective factors.
Identified community-level risk and protective factors for depressive symptoms in school-aged children can be targeted in health promotion through: (a) universal programmes preventing depression by targeting community-level variables associated with depression across the whole population, (b) early intervention by identifying at-risk individuals and sub-populations for targeted interventions and (c) treatment by considering identified risk and protective factors in individual assessment and treatment planning.
A determinants approach argues that addressing the underlying community influences for mental health (e.g. community safety, discrimination) is likely to have a greater and more sustainable impact across large populations. Addressing many of the community-level risk and protective factors for depression will likely impact positively on other child and adolescent outcomes and indeed on a range of outcomes for other community members. For example, as risk factors such as community safety and community minority ethnicity and discrimination act on large population aggregates, they not only impact child depression, but also other costly outcomes such as injury and poor physical health.
Findings from this study echo support for the demands for a national mental health prevention strategy (Jorm, 2014). To achieve population-level reductions in depression, it is necessary to address the underlying determinants of mental health (e.g. community safety, community minority ethnicity and discrimination) through coordinated responses across a range of services and settings (Jacka and Reavley, 2014; Jorm, 2014). The findings of this study indicate that risk factors for child and adolescent depression operate outside the mental health sector (Jacka and Reavley, 2014). Comprehensive government policies are required to support action across sectors and disciplines in order to address these determinants and reduce the prevalence of depression (Jorm, 2014).
Conclusion
In conclusion, the current systematic review reveals significant associations between community-level risk and protective factors and child and adolescent mental health. It is argued that with the increasing rise in prevalence and associated cost of mental health problems, community health promotion and early intervention are necessary to minimise the impact of depressive symptoms. As such, further observational studies are required to investigate how community-level risk and protective factors influence depressive symptoms and how effective community interventions can be designed.
Footnotes
Declaration of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.