
Abstract
Emergency Psychiatry is evolving. In an environment that lacks a clear evidence base, and where a constellation of factors is driving up Emergency Department presentation rates and lengths of stay, several stakeholders are working towards and clamouring for change. With the goal of collaborating with such parties, we believe Emergency Psychiatrists should position themselves to establish and advocate for best-practice change in culture, research, clinical care and training, and funding in the provision of mental health crisis care. To this end, we have formed the NSW Emergency Psychiatry Network, a group of Emergency Psychiatrists with a broad experience in a range of settings, from tertiary metropolitan emergency facilities with access to subspecialty psychiatric services, to rural and remote emergency settings with sporadic in-reach from local mental health services and telehealth. We unanimously recognise the need to upskill both Emergency Department and Mental Health clinicians in crisis care, and the need for committed, evidence-based Mental Health resourcing within Emergency Departments.
Introduction
Psychiatric presentations to Emergency Departments (EDs) are escalating (Australian Institute of Health and Welfare, 2022). While this phenomenon has attracted attention and a push for change from Emergency physicians, as reflected in multiple documents produced by the Australasian College of Emergency Medicine (ACEM) (Duggan et al., 2020), psychiatric opinion leaders and administrators have been slow to recognise and act on these trends in a systematic way.
We argue that it is time for psychiatrists delivering services in the ED to drive closer collaboration between the psychiatric community, Emergency Medicine and ACEM, government and other stakeholders. We must encourage a joint effort to build a culture that puts patients first and urge investment in frameworks for research and evidence-based clinical care for patients with psychiatric symptoms in EDs across Australia. We have therefore established the NSW Emergency Psychiatry Network and believe the Network should be extended across Australia and New Zealand.
The current state of play
Over time, the assessment and management of urgent psychiatric presentations has gravitated towards the general hospital ED setting (Australian Institute of Health and Welfare, 2022). This brings Emergency Psychiatry to the intersection of systems with oft-opposing expectations of outcomes and responsibilities. These interfacing systems include police, ambulance, consumer advocates, legal frameworks, non-government organisations, the general community, and carers and family members, as well as in-hospital groups, including the ED, hospital inpatient teams, hospital management and the Emergency Psychiatry team’s own Mental Health (MH) service. Empathy can be difficult under such chaotic conditions, making it perhaps unsurprising that EDs are places where our patients have met stigma and discrimination from various stakeholders (Knaak et al., 2017). In an attempt to challenge that stigma (and manage other challenges), some larger EDs now have co-located MH teams consisting of psychiatrists, registrars, nurses, allied professionals and increasingly, peer workers, while others have instituted a consciously collaborative approach between MH, ED, Alcohol and Drug, and Toxicology teams. There has also been innovation in many rural and remote EDs that now use Mental Health Emergency Care tele-psychiatry services.
Significant challenges
Despite these innovations, multiple challenges are evolving. Our members report that increasing demands on MH services and erosion of resourcing mean some community teams can no longer provide services that demonstrate fidelity to the Crisis Team model, which puts escalating inflow pressure on EDs. Effective crisis interventions within the ED remain inadequately researched (Johnston et al., 2019), leaving considerable room to improve the knowledge base regarding the efficacy of EDs as treatment environments. Finally, over the last two decades, waiting times for inpatient beds have escalated (Duggan et al., 2020).
Psychiatric Emergency Care Centres (PECCs) were established in NSW and Queensland, and other short stay units were established nation-wide, in an effort to facilitate exit from EDs. However, in the case of PECCs, there is ‘no convincing evidence to support a . . . best-practice model of care’ (New South Wales Ministry of Health, 2015), leading to confusion regarding the purpose of the model and impacting ED outflow.
The final challenge pertains to funding. There has been a recent $87 million NSW Government Towards Zero Suicides commitment to support those at risk of suicide, and a $2.3 billion Australian Government National Mental Health and Suicide Prevention Plan. However, the perennial challenges of short funding cycles, brief lead-time, lack of requirement to show an evidence-based approach and the absence of commitment to inpatient and emergency MH services continue to mar the provision of excellent Emergency Psychiatry care.
NSW Emergency Psychiatry Network: a commitment to change
While there have been multiple calls to action (Duggan et al., 2020), there has not yet been a systematic, well-organised approach representing the stance of the Australasian Psychiatric community. In this time of increasing chaos in EDs, we need a clear collective voice.
We have thus formed the NSW Emergency Psychiatry Network, a group of psychiatrists invested in the provision of excellent emergency MH care.
The NSW Emergency Psychiatry Network members bring experience in Emergency Psychiatry from a mix of remote and urban settings, in both Adult and Child and Adolescent services, across facilities with varied models of care and levels of staffing. Across the board, our members report a need to upskill both ED and MH clinicians in the area of crisis care and to secure a commitment to improve relationships between ED and MH clinicians. This includes a focus on collaborative system improvement, rather than the current approach that at times holds ED MH clinicians accountable when patients are stranded in ED, adding further strain to relationships. A more systematic focus on upskilling within the Royal Australian and New Zealand College of Psychiatrists (RANZCP) and ACEM training programmes may offer the opportunity to bring this to consciousness for both groups.
We intend to collaborate actively with the RANZCP, health departments, ED clinicians, and interested hospital and community multidisciplinary clinicians, including peer workers, to create a healthcare environment that is favourable to the recovery of those in the throes of a crisis. We believe that a national network would increase visibility and response coordination, improve empathy and respect across services, and emphasise the value of an Emergency Psychiatry sub-speciality lens.
What we call for
We believe Emergency Psychiatry has ‘come of age’. Rather than a by-product of a series of policy decisions over the years, Emergency Psychiatry must be seen as a valuable and intentional sub-speciality that requires a systematic approach. We call for the changes outlined in Box 1.
Policy, Practice and Resourcing Priorities for Emergency Psychiatry in NSW.
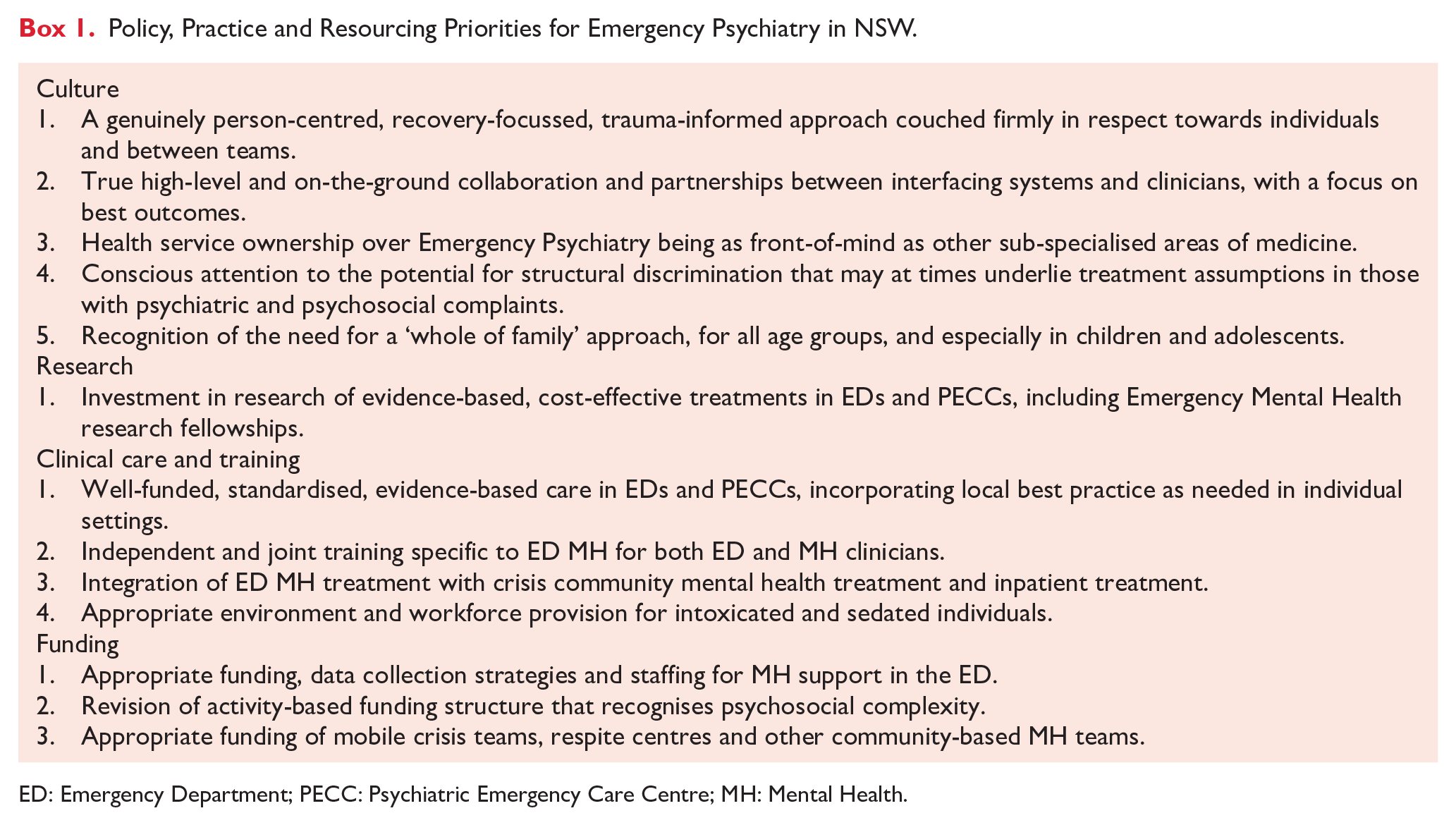
ED: Emergency Department; PECC: Psychiatric Emergency Care Centre; MH: Mental Health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.