
Abstract
Objective
The number of individuals presenting with a mental health crisis in Australia has been steadily increasing. This review aims to identify what crisis intervention services are available in Australia for consumers experiencing a mental health crisis without an underlying severe psychiatric illness, and to explore the experiences of consumers utilizing these services.
Method
Using PRISMA methodology, we conducted a review of four databases (Ovid Medline, PsycINFO, Web of Science, and Scopus) for articles relating to lived experience of consumers in Australian crisis intervention services. Inclusion and exclusion criteria were applied, and relevant articles assessed.
Results
Eleven articles met the inclusion criteria. Identified crisis services included emergency departments, emergency services, crisis helplines, and community centres. Persistent themes included negative attitudes from staff, discordance around what constitutes a mental health crisis warranting presentation, long wait times, and the role of these services in providing non-clinical emotional support rather than medical interventions.
Conclusion
This review identified clear discrepancies in consumer experiences between services, with specific aspects of care consistently linked to either positive or negative experiences. Improving staff communication and addressing judgemental attitudes may improve experiences. System reform would be better guided by further research into why consumers engage with specific crisis services.
Mental health related emergency department (ED) presentations have been steadily increasing in Australia over the past decade. 1 In 2022-23, there were almost 300,000 such presentations, accounting for approximately 3% of all Australian ED visits. 2 The most common reasons for a mental health presentation related to stress and substance use. 2 This increased service demand has resulted in extended wait times for consumers as hospital services struggle to manage the influx. 1
Despite the increasing demand, there is growing international evidence suggesting that EDs are not always the most appropriate setting for mental health presentations. Numerous studies have suggested that EDs are often poorly equipped to support individuals experiencing a mental health crisis, for a variety of reasons.3–6 While the concept of a mental health crisis is often complex and difficult to define, this review will define it as the presence of emotional distress beyond the coping mechanisms of the individual. 7 For consumers experiencing a mental health crisis characterised by a relapse of a severe psychiatric illness, EDs may be appropriate settings, as these individuals often require medical intervention and potentially psychiatric inpatient admission. However, a significant proportion of people experiencing a crisis do not have any underlying severe psychiatric illness.1,8 These crises often result from psychosocial stressors and suicidal ideation. For this population, the ED is less suitable, as they can often be effectively managed in a less clinical environment.1,9
The recent Royal Commission into Victoria’s mental health system highlighted the importance of providing a range of alternative services to the ED that are better suited to supporting consumers during a mental health crisis. 1 Currently, there are a variety of governmental and non-governmental services available for someone in crisis to access in Australia. 10 These include the ED, police and ambulances services, crisis assessment and treatment teams (CATT), helplines such as Lifeline or Beyond Blue, and a select number of community services and organisations.
Existing literature on mental health crisis pathways predominately focuses on individual service models in isolation, with limited comparative analysis across multiple pathways. As such, it is currently unclear whether inequalities exist between these services, or if consumers would benefit from engaging with one service over another. Additionally, the literature is largely quantitative, emphasising service efficacy through metrics such as reductions in ED presentations and clinical outcomes. There is limited qualitative research about consumers lived experiences utilising these services. The Royal Commission emphasised that insufficient consideration of the consumer experience acts as a barrier preventing service improvement and reform. 1 Therefore, the aim of this review is to identify what crisis interventions services are available in Australia for consumers without an underlying severe psychiatric illness during a mental health crisis and to explore the lived experiences of the consumers utilising these services.
Method
This review followed PRISMA guidelines and involved the systematic search of the four online databases, Ovid Medline, PsycINFO, Web of Science, and Scopus, for full text articles relating to the lived experience of individuals utilising mental health crisis intervention services. The databases were accessed between January–March 2025. Key words utilised in the search included mental health crisis, mental health service, psychiatric service, crisis intervention, crisis support, lived experience, and Australia.
To be included in this review, the articles had to contain the lived experience of consumers in Australia and pertain specifically to crisis intervention services. Articles were limited to those written in English. Articles about consumers’ lived experience within the mental health system in general were excluded, as were articles which represented the lived experience through quantitative data such as satisfaction scores. Articles which focussed on consumers with significant or severe psychiatric illness were also excluded (Figure 1). PRISMA flow diagram.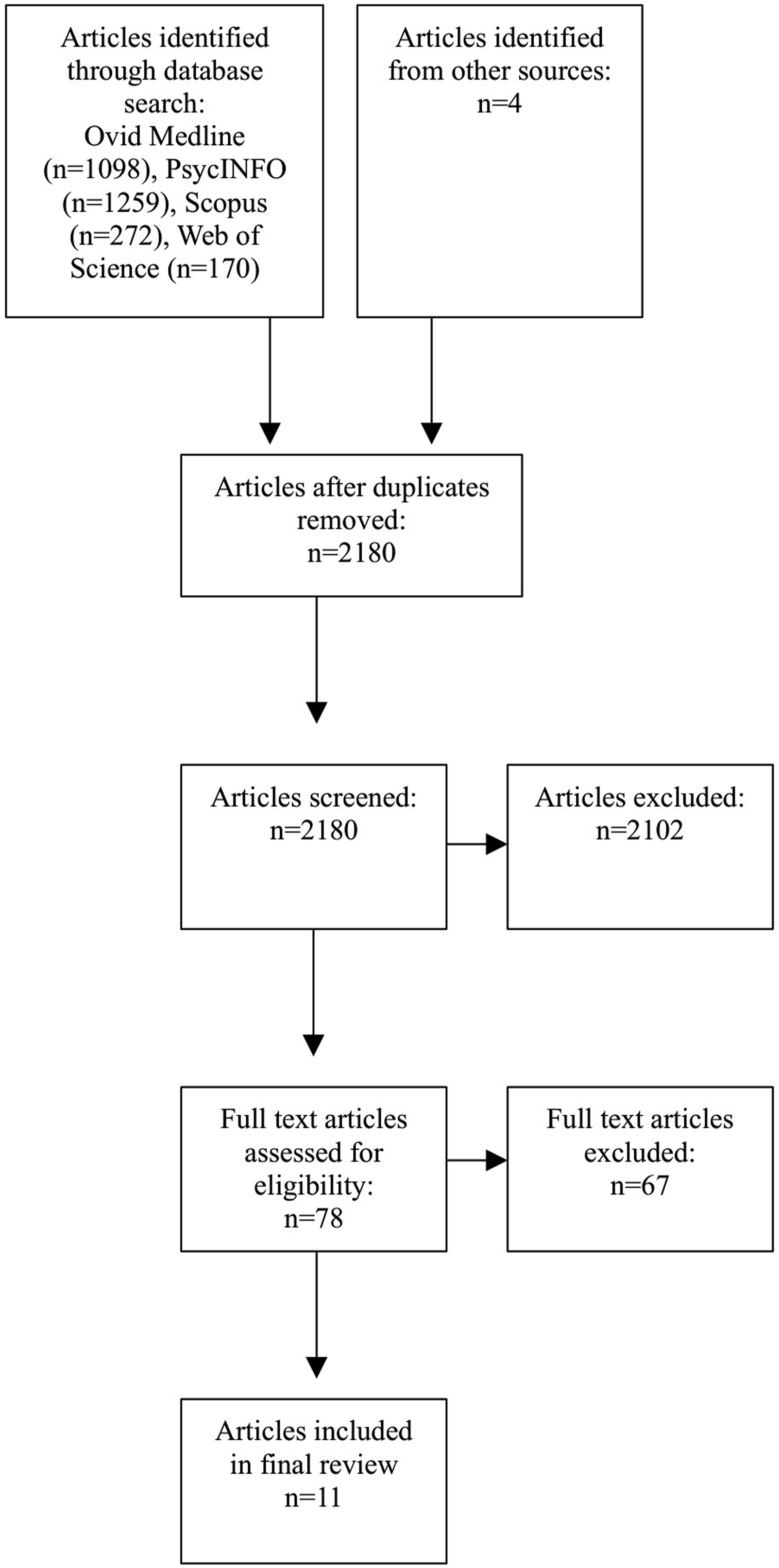
Results
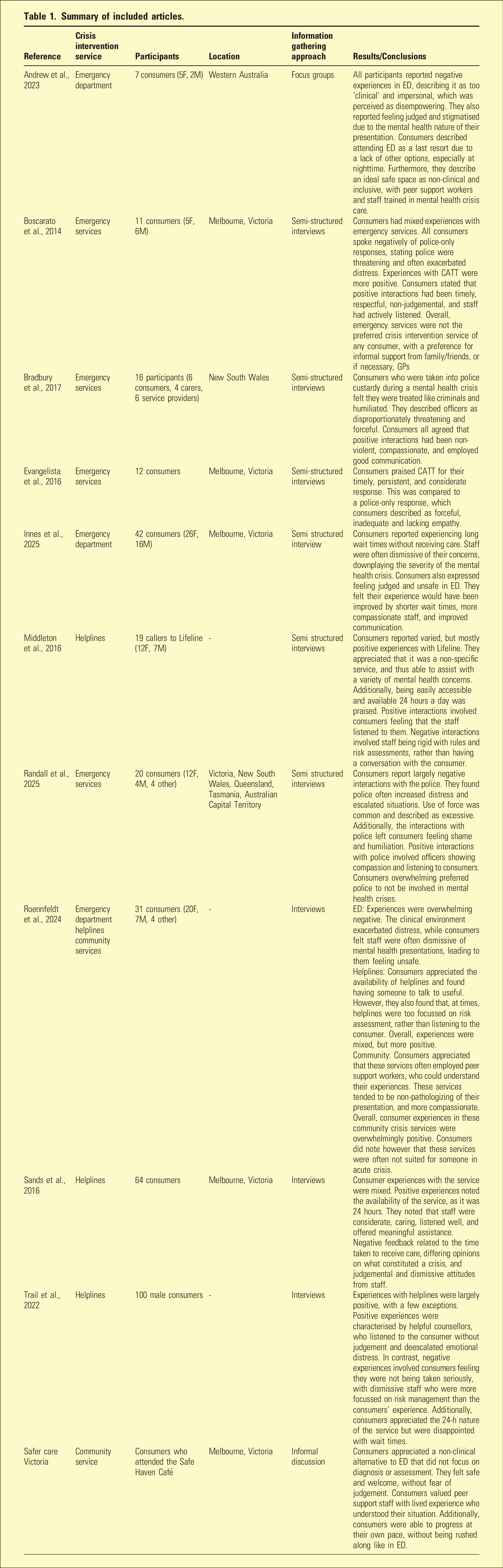
Summary of included articles.
Emergency department
Three articles7,11,12 discussed the experience of consumers who accessed ED during a mental health crisis in Australia. The responses of participants were overwhelmingly negative, with the majority of consumers describing ED as inadequate and poorly equipped for dealing with psychological distress, often worsening a crisis rather than resolving it.
The negative themes described by consumers were consistent across all three studies. Many described attending ED as a last resort, especially at nighttime. Consumers felt unsure of where else to access support during a crisis, especially when alternative support systems or services were unavailable. In the ED, consumers reported long wait times before receiving treatment, which contributed to feelings of being ignored. This exacerbated distress and resulted in consumers feeling unsafe. Additionally, the clinical and impersonal environment of ED further exacerbated feelings of isolation and fear. Staff were frequently described as judgemental, dismissive, and downplaying of the severity of crises. This left consumers feeling stigmatised and disempowered, believing that staff were not taking them seriously.
In addition to the experiences in ED, Andrews et al. 11 and Innes et al. 12 explored consumers’ opinions on how to improve the ED to better cater to those in crisis. Common suggestions included improved training for staff regarding mental health presentations, clear and effective communication, and non-judgemental attitudes. Consumers in both studies also strongly advocated for the inclusion of peer support staff in ED, believing these individuals with lived experience would be better able to advocate for them and their needs.
Emergency services
Four articles13–16 detailed consumer interaction with emergency services, including police, paramedics, and CATT. Police interactions were discussed in all four articles, with consumers describing their experiences as overwhelmingly negative. The police response was seen as distressing and often escalated the situation. Officers were characterised as threatening, coercive, and at times violent. Many consumers described being forcibly restrained by officers, which left them feeling humiliated and like criminals. Additionally, consumers felt the police response often lacked empathy and compassion, with officers displaying judgemental attitudes towards the consumers. Randall et al. 16 and Boscarato et al. 13 specifically reported that consumers overwhelmingly did not want police involved in a mental health crisis response. Positive experiences with the police, while very limited, involved officers showing compassion and listening to the consumer without resorting to violence and physical restraint.
Boscarato et al. 13 and Evangelista et al. 15 detailed consumer experiences with CATT. They reported mixed, but mostly positive, interactions. Consumers praised CATTs ability to deescalate the situation through a timely, compassionate, and respectful response. When compared to interactions with police, consumers described CATT as more likely to listen to their concerns in a respectful way. Members of the CATT were viewed as less judgemental and displayed more empathy for the consumer and their situation. Negative experiences with CATT were similar to those with police, in that consumers felt staff were dismissive, rude, and judgemental.
Helplines
Four articles7,17–19 explored consumer experience with Australian crisis helplines. Middleton et al. 17 looked specifically at consumer experience with Lifeline, while the other articles did not specify a service. Overall, they reported mixed, but largely positive, experiences. Common themes that emerged included consumers’ appreciation for the 24-h availability of helplines, as it allowed crisis support to be accessed at any time. Additionally, the convenience of being able to access help without having to leave the house was also appreciated. While the accessibility of the service was praised, a number of consumers noted extended wait times before being connected to support staff.
Consumer satisfaction with helpline services was largely influenced by how well they connected with the staff member they spoke to. Users who reported positive interactions described staff as caring and considerate. They listened to the consumer’s perspective without judgement, were able to deescalate emotional distress, and offer meaningful assistance. In contrast, negative interactions involved staff being described as judgemental or dismissive of the consumer’s crisis. A contributing factor to these feelings was staff’s perceived inflexibility with risk assessment and management. Many consumers felt that staff were overly focussed on completing a risk screening and prioritised it over addressing the consumer’s concerns. This resulted in consumers feeling that they were not being taken seriously by staff.
Community
Two articles7,20 discussed consumer experience with community crisis services. Safer Care Victoria 20 focussed specifically on St Vincent’s Safe Haven Café, while Roennfeldt et al. 7 did not specify a service. Consumers who attended community services appreciated having a non-clinical alternative to the ED and valued the non-pathologizing approach, which did not focus on diagnoses or assessments. Community services were more personal and provided meaningful human connection, which was lacking in the clinical environment of other crisis interventions. This cultivated a welcoming and inclusive space, which consumers could access without fear or judgement. The calmer environment also allowed consumers to navigate their crisis at their own pace, which was described as empowering.
The employment of peer support workers was also praised by consumers. The presence of individuals with lived experience gave consumers the opportunity to discuss their crisis with someone who could relate to their situation. Consumers in Roennfeldt et al. 7 however did note that these community services were not always best suited for assisting people experiencing a significant mental health crisis.
Discussion
This review of mental health crisis support services available in Australia demonstrates not just the variety of services available, but also the spectrum of experiences that consumers have had with these services. The studies included consumers from most states and territories in Australia, including both rural and metropolitan locations, thus providing insight from a geographically diverse Australian population. However, the studies were mostly limited to English speaking participants, and therefore results may not be representative of the experiences of non-English speaking consumers. Out of the four crisis support modalities discussed, emergency services, especially police, received the worst feedback from consumers. Officers were frequently characterised as threatening and intimidating, leaving consumers feeling humiliated and distressed.13–16 Consumers who attended an ED also reported largely negative experiences. The clinical and impersonal environment of the hospital left consumers feeling isolated and disempowered, while staff were often judgemental and dismissive.7,11,12 Australian crisis helpline receives similar criticism as the ED; however, overall consumers reported more positive and helpful experiences, and staff were described as more compassionate.7,17–19 Community crisis services, in contrast to the other three, received overwhelmingly positive feedback from consumers. These services were described as respectful, considerate, and understanding of the consumers’ situation.7,20
Analysis of the consumer experiences revealed four recurrent themes across all services. These include negative attitudes from staff, a discordance around what constitutes a mental health crisis warranting presentation to these services, long wait times when accessing help, and the role of these services as providers of non-clinical emotional support rather than medical interventions.
The majority of the negative experiences described by consumers related to how staff treated them. Interactions were frequently described as being judgemental and lacking empathy. Many consumers felt their crisis was not being taken seriously by the staff who they had turned to for help, resulting in many consumers reporting that they felt unsafe. This negative staff behaviour was reported most consistently by consumers who interacted with the ED and police; however, it was also reported to a lesser extent by those who accessed crisis helplines and community services. The experiences of consumers in this review are consistent with current literature1,4,21 relating to staff behaviour in mental health services in Australia. The recent Royal Commission in Victoria 1 found that judgemental and dismissive attitudes from staff were not just occurring in crisis care services but throughout all levels of mental health care. This suggests that there is still a significant stigma surrounding mental illness in Australia, which in turn creates barriers for consumers accessing care. It has been shown that negative experiences can lead to disengagement from the system, resulting in consumers delaying presentation for mental health support until they are experiencing an acute crisis. 22 This in turn places a greater burden on these mental health crisis services and likely results in poorer outcomes for consumers.
The second common theme that emerged from the articles is a discordance between what consumers and staff believe constituted a mental health crisis. Consumers felt staff minimised their experiences and attempted to downplay the severity of their crisis, leaving them feeling dismissed and ignored. Users of helplines and ED often reported that their perception of their crisis was not shared by service staff. Current literature emphasises the multifaceted and highly subjective nature of mental health crises and describes the broad spectrum of what an individual may experience during a crisis.23,24 This subjectivity can make it difficult to clearly articulate their experiences to care staff. 24 When combined with a lack of visible physical symptoms, consumers are often left feeling like they struggled to convince providers of the severity of their condition. 25 Staff not perceiving the consumer as being in a mental health crisis may have contributed to the judgemental and dismissive attitudes described by consumers above. This suggests that there is a disconnect between what mental health consumers in Australia view as a crisis, and what care providers deem an appropriate time to present to crisis support services. Further education of crisis support staff may therefore be needed to enhance understanding of why consumers may seek support, and the difficulties they may face when explaining their situation.
A third recurrent theme was the extended wait times experienced by consumers when accessing crisis support services. Users of helplines and ED frequently reported long delays before receiving care, which negatively impacted their overall experience. Research has shown that, on average, mental health presentations in ED wait significantly longer than non-mental health presentations.1,2 One contributing factor may be the dismissive attitudes of staff, and the differing interpretations of a mental health crisis discussed above. However, current literature1,2,26 has also shown that both ED and crisis lines have seen increased demand in recent years, and these extended wait times likely indicate that these services are struggling to meet the increased consumer demand. This suggests a growing need to expand these services to reduce wait times and improve the experience of those utilising the service.
The final theme identified is the role of these services as safe outlets for consumers to voice their distress, without requiring medical intervention. Across all four service pathways, consumers consistently described positive experiences when staff simply provided space to talk. Consumers felt most supported when staff took the time to listen to the consumer’s concerns without interruption, validated their perspectives, and made them feel seen and heard. This positive response was frequently achieved without providing any additional services to the consumer, beyond the opportunity to speak openly in a safe environment. This suggests that, for consumers in crisis without significant psychiatric illness, the primary value of these services lies in offering a supportive space to express emotions and discuss stressors, rather than delivering medical care or other tangible interventions. Community crisis services most frequently displayed this, with consumers who utilised these services reporting overwhelmingly positive experiences.7,20 One possible explanation for this is the presence of peer support workers with lived experience at these community locations. Consumers highlighted the importance of peer workers in providing a safe and understanding environment, and research27,28 has shown peer support workers to be effective in improving satisfaction of consumers utilising a service. This potentially demonstrates a need for peer workers to be present at all crisis support services, to improve the consumer experience, and encourage engagement with the services. 29
Strengths and limitations
This review’s strength is that it explores the experiences of consumers presenting in crisis to a wide variety of mental health services in Australia. This is a critically important topic, given the increasing demand on these services and the potential for this research to support reform to improve the consumer experience.1,2 Additionally, the inclusion of Australian specific studies in this review allows the findings to be directly applied to the Australian mental health system.
However, this review was limited by the number of available studies for each service, especially community crisis services. Although a wide range of services exists, 10 including multiple helplines and community services, this review was only able to explore the experiences of a limited number, due to a lack of available data. As such, experiences reported may not be entirely representative of each crisis intervention modality. Similarly, the small sample size in the majority of the reported studies is another limitation. Mental health crises are complex and heterogenous, with the needs and expectations of consumers varied.23,24 Thus, the small sample sizes reported in these studies may not be representative of the broader experiences of individuals utilising the service.
Recommendations and future directions
Overall, the findings of this review support several recommendations for improving consumer experiences with crisis services. The consistently negative experiences of consumers with police suggest that police should have an extremely limited, if any, role in responding to mental health crises. Similarly, the overwhelmingly poor experiences of consumers who accessed ED implies that, without any clear indication for medical interventions, ED also has a limited role during mental health crises for consumers without an underlying psychiatric illness. These findings also highlight a need for further mental health education and training of staff to combat the stigma and discrimination that continues to be experienced by those in a mental health crisis.
Helplines, in contrast, received largely positive feedback but were hindered by long wait times. Expansion of these services could provide consumers with easily accessible support, which consumers valued, while also alleviating the strain currently on the system and reducing wait times. One possible strategy that has shown promise internationally is the integration of AI chatbots and messaging services for crisis support, such as the Mindline project in Singapore, which has seen positive impacts in triage, counselling, and referral processes. 30
While this review has highlighted the value of non-clinical crisis services in the community and the inclusion of peer support workers, there is still a paucity of data relating to consumer experiences in community services. The Victorian Government has made attempts to expand such supports for less severe crises with the recent rollout of several Mental Health and Wellbeing Hubs and Locals. 31 However, these centres have not yet been evaluated for efficacy or for consumer satisfaction. As such, further research into the experience of consumers utilising community support services is necessary to produce a clearer guide on how best to further develop this service.
Finally, while several studies in this review included consumers from rural locations and First Nations consumers, the experiences of these groups were not specifically analysed. Both First Nations consumers and those in rural areas are significant users of mental health crisis services,2,26 yet there is little data on their specific experiences. Non-English-speaking consumers were also largely excluded from the studies included in this review, highlighting a similar gap. Therefore, further research into the experiences of these groups is needed to determine whether crisis intervention services are meeting the needs of Australia’s diverse consumer population.
Conclusion
The aim of this review was to assess the current services available in Australia for consumers to access during a mental health crisis, and to explore their experiences with these services. Despite small sample sizes and paucity of data for a number of services, it is clear that there is a discrepancy in consumer experience between services. The services which provide a safe place with respectful and compassionate staff were preferred by consumers, while the services which were dismissive, judgemental, and minimised the consumer’s experiences were heavily criticised. The mental health sector in Australia would benefit from further research into the experiences of diverse consumers accessing mental health crisis support.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This study did not require ethical approval as it is a systematic review of existing published data and does not involve human subjects or the collection of new data.
Data Availability Statement
No new data were created or analysed in this study. Data sharing is not applicable to this article