
Abstract
Objective:
No synthesis of the Australian evidence regarding targeted prevention and early intervention for mental health concerns among young children exists. This review aimed to (1) describe the types of targeted community-based mental health programmes evaluated in Australia to support children aged 1–9 years exhibiting internalising and/or externalising symptoms and (2) examine their impact on children’s internalising and externalising symptoms and disorder diagnosis.
Method:
A systematic review and meta-analysis was conducted (PROSPERO: CRD42021255257). Four databases (PsycINFO, PsycArticles, MEDLINE and CINAHL) were searched for Australian studies published in the past 10 years that quantitatively evaluated the impact of a targeted programme on children’s mental health. The National Institute of Health Quality Assessment Tools were used to evaluate the study quality.
Results:
Forty-two studies were included; the majority (67%) were medium quality. The mean sample size was 142 (SD = 170), children’s average age was 5.78 years (SD = 2.44) and 58% were male. Aboriginal and Torres Strait Islander children were underrepresented. Studies evaluated 16 programmes that targeted (1) externalising symptoms (n = 20 studies, n = 6 programmes), (2) internalising symptoms (n = 14 studies, n = 7 programmes) or (3) both, termed transdiagnostic programmes (n = 8 studies, n = 3 programmes). Externalising programmes achieved a significant moderate mean reduction in externalising behaviours (standardised mean differences = −0.56), internalising programmes yielded a small mean improvement in anxiety symptoms (standardised mean differences = −0.25) and 57% reduced odds of anxiety disorder diagnosis. Evidence supporting transdiagnostic programmes was inconclusive.
Conclusion:
Parenting-focused programmes targeting young children’s internalising or externalising behaviours have the largest local evidence base supporting their effectiveness. Limitations include a lack of engagement with fathers, triangulation of outcomes, homogeneity and implementation reporting. Greater implementation and evaluation of community-driven integrated and systemic approaches that identify, engage and support Australia’s most disadvantaged cohorts of young children and their families are needed.
Keywords
Emotional and behavioural concerns during early childhood (i.e. aged 1–9 years) are highly prevalent worldwide, and mental health disorders are the leading cause of childhood burden of disease globally (Baranne and Falissard, 2018; Barican et al., 2021). In Australia, approximately 1 in 7 children (14%) aged 4–11 years old experience mental health concerns in any given year (Lawrence et al., 2015). The international prevalence is similar, with 1 in 8 children (13%) in England and 1 in 6 children aged 2–8 years in the United States experiencing emotional and/or behavioural concerns (Cree et al., 2016; National Health Service [NHS], 2018). Anxiety is one of the most commonly experienced mental health concerns among young children (Carpenter et al., 2016), while behavioural concerns are more prevalent among children aged 6–11 years than any other age group (Ghandour et al., 2019). Within the context of the COVID-19 pandemic, public health measures such as city-wide lockdowns, social distancing, and closures of early childhood education centres and schools have negatively impacted the mental health of children, resulting in an unprecedented high need for mental health support (Sicouri et al., 2022).
Emotional and behavioural concerns are common presentations of mental ill health during early childhood. Behavioural concerns in childhood are characterised by hyperactivity, aggression, disobedience, tantrums or disruptiveness (Ogundele, 2018). They are also referred to as ‘externalising’ behaviours as they manifest in children’s outward behaviours and reactions to their external environment. Children who exhibit such behaviours may be at risk of developing attention-deficit/hyperactivity disorder (ADHD) or oppositional defiant disorder, experiencing juvenile delinquency during adolescence, or crime and violence in adulthood (Sallis et al., 2019). In contrast, emotional concerns predominantly encompass anxiety, fear, inhibition, sadness or withdrawal. These are considered ‘internalising’ behaviours as they are inhibited/internally focused symptoms that predominantly affect the child’s internal psychological environment, and may not be as overt or obvious to others (Ogundele, 2018). Children with internalising symptoms are at risk of developing anxiety disorders (i.e. generalised, social, obsessive-compulsive) or major depressive disorder (Ogundele, 2018). Despite their clear distinction in presentation, there is a significant reciprocal relationship and high rates of co-morbidity between internalising and externalising mental health concerns, with at least 25% of young children experiencing both (Sallis et al., 2019; Wertz et al., 2014). Given that the onset of 50% of adult mental health disorders occur by age 14 (Mulraney et al., 2021), the need for targeted prevention and early intervention for young children exhibiting such symptoms is well-established. Targeted prevention and intervention (or ‘indicated prevention’) refers to intervention efforts aimed at those at high-risk, such as young children displaying signs or symptoms of internalising or externalising behaviours (Colizzi et al., 2020). Targeted programmes are more effective at preventing long-term mental health concerns among children than universal interventions (Horowitz and Garber, 2006; Werner-Seidler et al., 2021) which are delivered to general populations that have not been identified on the basis of any particular risk factors. This is likely due to differences in the level of symptoms among children at baseline, with those receiving targeted interventions already showing signs and symptoms upon which to improve (Horowitz and Garber, 2006).
The development of emotional and/or behavioural concerns during childhood is predominantly influenced by the complex interactions between a child’s environment and their biological predispositions (Assary et al., 2018; Paclikova et al., 2019). Key risk factors encompass various adverse childhood experiences, such as poverty/low socioeconomic status (Hodgkinson et al., 2017), child maltreatment (i.e. neglect, abuse, Vasileva and Petermann, 2016), parental mental illness (Ayano et al., 2021), maladaptive parenting behaviours (Yap and Jorm, 2015) and family dysfunction (Sahle et al., 2021a, 2021b). Interventions to prevent or ameliorate the impact of these adverse childhood experiences could potentially prevent approximately 38% of childhood-onset mental health disorders (Sahle et al., 2021a, 2021b). Parenting programmes are one evidence-based form of prevention and early intervention for childhood mental health concerns as they seek to address such risk factors, including parenting styles, parent–child relationships and attachment (Barlow and Coren, 2017; Yap et al., 2016). Furthermore, specific cohorts of children, including children from refugee backgrounds, children living in rural or remote areas, children involved with the child protection system and Aboriginal and Torres Strait Islander children, are at greater risk of experiencing mental health concerns (National Mental Health Commission [NMHC], 2020). Therefore, Australia’s National Children’s Mental Health and Wellbeing Strategy proposes the need for community-driven early intervention approaches that seek to address the impacts of trauma and social determinants for young children exhibiting emotional and behavioural concerns (NMHC, 2020).
Children aged under 12 years of age are significantly less likely to access and receive support for emotional and/or behavioural concerns than young people aged over 12 years (Australian Institute of Health Welfare [AIHW], 2020). Specifically, in Australia, 46% of children under 12 years compared with 61% of adolescents aged 12–17 years exhibiting mental health concerns received support (Lawrence et al., 2015; Sawyer et al., 2019). Key barriers to accessing support for younger children include low caregiver/family awareness of appropriate services, limited availability of or access to suitable supports (e.g. long waiting lists), negative family attitudes towards mental illness and help-seeking, stigma, limited caregiver mental health literacy (e.g. lack of awareness of risk factors or early signs, limited capacity to identify such symptoms), strict eligibility criteria (e.g. younger children do not often meet criteria for a mental disorder) and large out-of-pocket costs (Hansen et al., 2021; NHMC, 2020; Shing et al., 2021). As internalising and externalising concerns during early childhood are strongly associated with the development of mental health disorders in adolescence and adulthood, targeted early intervention efforts need to be delivered to children experiencing early signs and symptoms rather than waiting until they become entrenched or develop into a diagnosable disorder later on (Mulraney et al., 2021). Early childhood therefore presents a critical time for targeted intervention.
Targeted prevention and early intervention for children already exhibiting emotional and/or behavioural concerns is predominantly delivered via community-based services. Community-based programmes are delivered within the child’s and family’s existing natural environment in their local community, such as in homes, local community centres, community service organisations, community mental health clinics or via local community outreach (i.e. parks, recreational centres). They are often designed to target the child’s symptom-specific factors (i.e. anxiety, disruptive behaviour), or risk factors (i.e. parenting styles) that may be linked to the child’s difficulties (Mejia et al., 2012). Targeted community-based mental health support for young children exhibiting externalising behaviours predominantly comprise parenting-focused interventions, such as the Triple-P Positive Parenting Program (Sanders et al., 2014), and Parent–Child Interaction Therapy (PCIT; Funderburk and Eyberg, 2011). Such programmes are underpinned by social learning and attachment theories, as parents are equipped with the skills to increase positive reinforcement of desirable child behaviour and reduce undesirable behaviour, while enhancing the parent–child relationship (Funderburk and Eyberg, 2011; Sanders et al., 2014). In contrast, targeted programmes for children experiencing internalising symptoms (i.e. anxiety and depression) are predominantly underpinned by Cognitive Behavioural Therapy (CBT)-based strategies (e.g. relaxation techniques, exposure, cognitive restructuring) with a focus on practical skills to help children effectively manage their symptoms (e.g. Crowe and McKay, 2017). There is over 30 years of local and international literature supporting evidence-based parenting programmes in improving children’s internalising and externalising behaviours among a diverse range of families (Barlow and Coren, 2017; Mejia et al., 2012; Yap et al., 2016). There is also extensive international evidence for targeted community-based therapy programmes that are directly delivered to the child (i.e. child-focused programmes), such as play therapy (Aja, 2018; Parker et al., 2021), and family support programmes (i.e. home visitation, Azzi-Lessing, 2013; Ordway et al., 2014).
To the authors’ knowledge, there has been no synthesis of the Australian evidence base regarding the impact of targeted community-based mental health programmes for young children on internalising and externalising outcomes. Comparable international reviews and meta-analyses have observed small to medium effect sizes for short-term reductions in internalising disorders and symptoms (Stockings et al., 2015) and decreased externalising behaviours (Uretsky and Hoffman, 2017) among children. However, there is limited synthesis of research conducted in the Australian context. While a recent Australian review found that community-based mental health programmes for adolescents and young people aged 10–25 years experiencing mental illness can alleviate internalising symptomatology (Savaglio et al., 2022), the overall impact of targeted programmes for younger Australian children specifically, remains unclear. Furthermore, the majority of the existing local and international literature focuses on universal mental health programmes, particularly in the school setting (e.g. Dray et al., 2017; O’Reilly et al., 2018), rather than targeted/indicated programmes. Specifically, Werner-Seidler et al. (2021) found that targeted school-based mental health programmes for children were associated with greater effect sizes for anxiety and depression than universal programmes. In contrast, synthesis of the Australian literature for targeted community-based programmes beyond the school setting is lacking.
While such programmes exist and are implemented across Australia, no systematic review or meta-analysis encompassing the various types of community-based mental health programmes for young Australian children (aged 1–9 years) exhibiting emotional and/or behavioural mental health concerns has been conducted. Such synthesis is needed to guide local practice, policy and to potentially inform the adaptation, implementation or scale-up of targeted community-based programmes for young children exhibiting signs and symptoms of mental ill health. The findings could also contribute to a more comprehensive and holistic international evidence base, while identifying gaps in the literature. Therefore, this review and meta-analysis aimed to (1) describe the types of targeted community-based mental health programmes evaluated in Australia to support children aged 1–9 years exhibiting internalising and/or externalising symptoms and (2) examine their impact on Australian children’s internalising and externalising symptomatology and disorder diagnosis. It is hypothesised that such programmes will yield a significant reduction in children’s internalising outcomes (i.e. anxiety disorders, major depressive disorder, and symptoms of anxiety and depression) and externalising outcomes (i.e. externalising disorders, such as ADHD and oppositional defiant disorder, and externalising symptoms), in comparison to the control condition.
Method
Design and protocol registration
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines (Page et al., 2021) were followed to conduct this systematic review and meta-analysis. The review protocol was registered with PROSPERO, an international database of prospectively registered systematic reviews in health and social care (Registration ID: CRD42021255257).
Search strategy
A systematic search of four electronic databases (PsycINFO, PsycArticles, MEDLINE, and CINAHL plus) were searched in November 2021. Combinations of the keywords child, mental health and program were used, along with customised medical subject heading search terms (see Supplemental Table 1 for the search strategy). Search terms were developed with a librarian, and also drawn from similar international systematic reviews (Charach et al., 2020). The reference lists and citations of eligible studies were examined.
Inclusion and exclusion criteria
Studies that met the following criteria were eligible for inclusion: (1) the study participants were children aged between 1 and 9 years 1 exhibiting emotional/internalising symptoms and/or externalising behaviour concerns, as assessed by various validated measures (e.g. Eyberg Child Behaviour Inventory, Child Behaviour Checklist, Spence Children’s Anxiety Scale); (2) the study was conducted in Australia; (3) the study quantitatively evaluated the impact of a targeted mental health programme that was delivered within the community (e.g. delivered in homes, community centres, etc.); (4) study outcomes included externalising behaviour (e.g. disruptive, antisocial behaviour), externalising disorders (e.g. ADHD, oppositional defiant disorder), internalising/emotional symptoms (e.g. anxiety and depressive symptoms), or internalising disorders (e.g. anxiety disorders, major depressive disorder); (5) the study used a quantitative evaluation study design (i.e. controlled study or pre–post study); and (6) the study was published in English from January 2011 to November 2021 inclusive. Studies were restricted to the past 10 years to provide a snapshot of the most current empirical evidence regarding the impact of interventions to inform current practice. Participants were aged between 1 and 9 years to address the lack of synthesis focused on young children (i.e. prior to adolescence), as a recent Australian review has previously examined mental health programmes for young people aged 10 years and over (Savaglio et al., 2022). This age range encompasses national and international definitions of early childhood (Department of Health and Human Services, 2020), and includes the years prior to the onset of adolescence (UNICEF, 2022).
Studies were excluded if (1) they did not examine the impact of the intervention on the child’s symptomatology (e.g. caregiver outcomes, cost-effectiveness, implementation); (2) the intervention was a smartphone or technology-assisted intervention only (e.g. mobile phone applications or online programme); (3) the intervention was a universal prevention programme delivered to all children (i.e. no risk or presence of symptoms) and (4) the intervention was delivered in an education setting. Studies examining technology-assisted and school-based programmes were excluded as they have been recently reviewed (Blewitt et al., 2019; Hollis et al., 2016; Werner-Seidler et al., 2021) and were not considered under the community-based scope of this review.
Study selection
The titles and abstracts of studies were independently screened by two researchers. The full-text versions of remaining studies were assessed for inclusion by the same two researchers. The interrater agreement (i.e. the proportion of studies given the same rating by the two researchers) was 0.92 during the title and abstract stage and 0.96 during the full-text stage. The two raters engaged in a cooperative discussion to resolve disagreements, during which they both articulated their reasoning for the rating and reached a final consensus.
Data extraction
A summary table was created to extract data from the included studies (see Supplemental Table 2). One researcher extracted data from the included studies, with a random 20% (n = 9) cross-checked for consistency. Studies were categorised according to intervention type. Data extracted included state where the study was conducted, study design, sample size, child characteristics (e.g. age, gender, type of symptoms), caregiver characteristics (e.g. age, gender, socioeconomic status) and intervention characteristics (e.g. duration, frequency, type of content delivered). This information was necessary to extract to identify any patterns or differences in programme impact based on child, caregiver or intervention characteristics.
Meta-analytic method
Separate meta-analyses were conducted for the included controlled and uncontrolled studies using Review Manager (RevMan5) software, as outlined in the Cochrane Handbook for Systematic Reviews of Interventions (2019). With the p-value set at p < 0.05, 95% confidence interval, estimated random effect size of 0.3 as identified in comparable meta-analyses (Uretsky and Hoffman, 2017), moderate to high levels of heterogeneity, and an average sample size of 70 per group across eligible studies, at least six studies were needed for each meta-analysis to achieve adequate statistical power of 0.80. For the controlled studies, a series of generic inverse variance random effects models were used to pool the standardised mean differences (SMD) in parent-reported outcomes between children from the intervention and control groups at the last available follow-up. For the uncontrolled studies, a random effects model was used to pool the SMD between pre-intervention and post-intervention. Random effects models were used to account for the large amount of heterogeneity both within and across the included studies as assessed with τ2 and I2 tests. The presence of publication bias was assessed by visual inspection of the funnel plot and by using Egger’s test. Studies’ effect estimates were pooled for the following outcome categories: externalising outcomes (externalising symptoms and frequency of engagement in externalising behaviours), internalising symptoms, anxiety (symptoms or diagnoses for the primary anxiety disorder at post-intervention) and depression (symptoms or diagnoses). The SMD was used as the effect estimate for the continuous outcomes as we expected variation in the scales used within each outcome category. Odds ratio was used as the effect estimate for disorder diagnoses as it was a dichotomous outcome. The number needed to treat (NNT) was computed for the dichotomous outcomes by calculating the inverse of the pooled absolute risk difference.
Quality assessment
The methodological quality assessment of included studies was conducted using two measures, depending on study design; the National Institute of Health (NIH) Quality Assessment Tool of Controlled Intervention Studies and the NIH Quality Assessment Tool for Before–After Studies (NIH, 2021). Key components of methodological quality (i.e. blinding, attrition rate, sample size and power, outcome measures, intervention adherence) were rated as ‘yes’, ‘no’, or ‘not reported’. Studies that were rated ‘yes’ for at least 70% of their assessment criteria were considered ‘high’ quality due to low risk of bias, studies that scored ‘yes’ for 50% to 69% of the criteria were categorised as ‘medium’ quality, and studies that fulfilled less than 50% of the criteria were classified as ‘low’ quality due to high risk of bias. A random 30% of studies were double-coded. Consensus was achieved through a cooperative discussion between the two researchers, where the interrater agreement was 0.98.
Results
Search yield
Figure 1 presents the PRISMA flowchart, outlining the stages of study selection. The database search yielded a total of 11,981 studies. Following the removal of 2456 duplicates, 9525 studies were screened for eligibility at the title and abstract stage, followed by 196 full-text studies. There were 154 studies excluded at the full-text stage, mainly as the study was not conducted in Australia. A total of 42 studies were deemed eligible for inclusion, of which 21 studies were included in the meta-analyses.
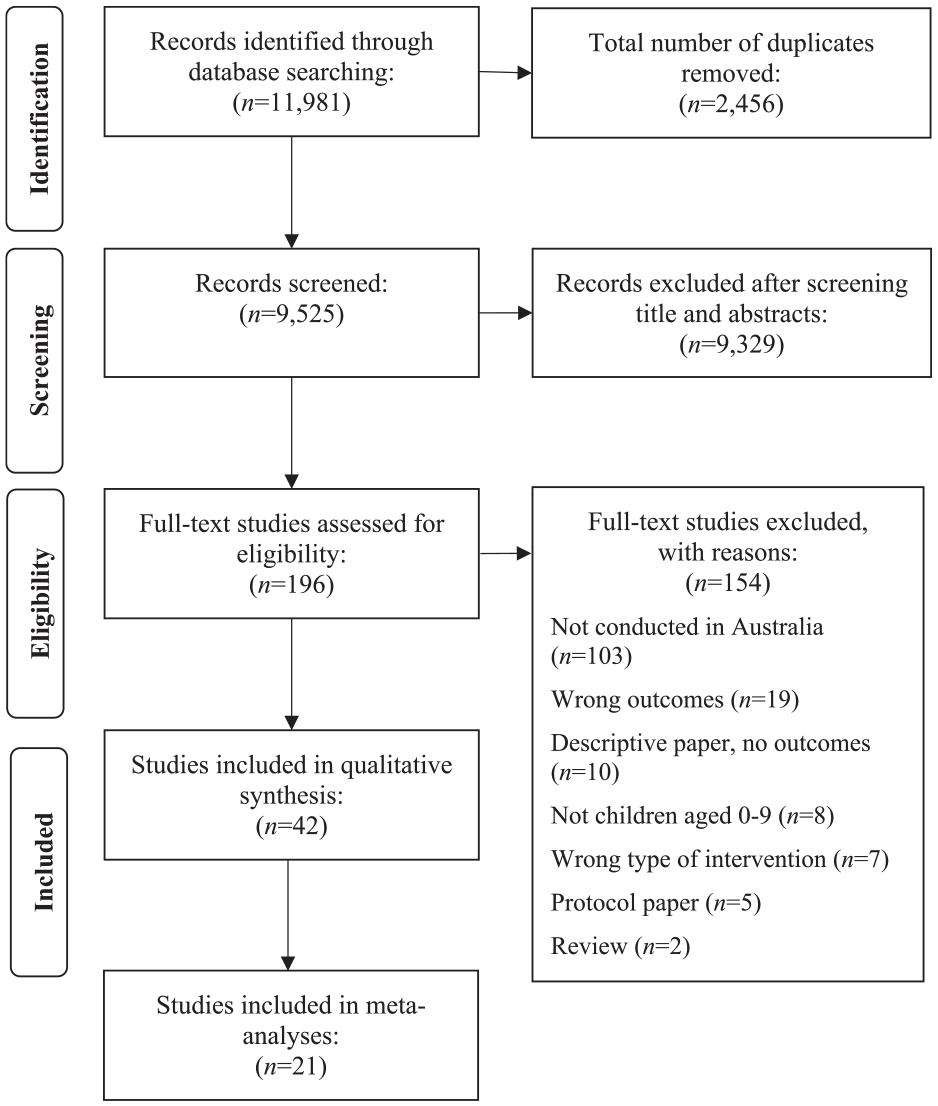
PRISMA flowchart illustrating the study selection process.
Study quality
The quality assessment ratings for the 42 studies are presented in Supplemental Table 3. There were 15 pre–post studies and 27 controlled studies (24 randomised controlled trials (RCTs) and 3 non-randomised controlled studies) included in this review. The majority of the controlled studies (18/27, 67%) were medium quality, five studies (19%) were classified as high quality with low potential for bias, and four studies (15%) were of low quality, due to high risk of bias. Methodological strengths of the controlled studies included adequate randomisation as groups were predominantly similar on key baseline characteristics (26/27, 96%), use of valid and reliable measures (100%), at least 80% participant retention (19/27, 70%), and use of intention-to-treat analysis (100%). Key limitations include the lack of blinding of participants, providers and outcome assessors (26/27, 96%), insufficient sample sizes for statistical power (21/27, 78%) and a lack of reporting of intervention adherence/fidelity (13/27, 48%).
The majority of the 15 pre–post studies (10/15, 67%), were considered medium quality, four studies (27%) were high quality and one study was classified as low quality. Methodological strengths include prespecified and clear eligibility criteria, and appropriate outcome measures and statistical methods to measure pre–post changes. However, there was a lack of blinding of outcome assessors due to reliance on caregiver-reported measures (12/15, 80%), limited reporting or assessment of intervention fidelity/consistent delivery (8/15, 53%), and sample sizes were generally not large enough to provide confidence in the findings (12/15, 80%). Studies were not excluded based on their quality as this review sought to capture and synthesise the existing evidence base regardless of study quality.
Participant characteristics
All studies were conducted in Australia, primarily from Queensland (n = 16), New South Wales (n = 14) and Victoria (n = 10), and two in the Northern Territory (Ritzi et al., 2017; Wicks et al., 2018). The mean sample size of children across the 42 studies was 142 (SD = 170), ranging from 4 children (Farrell et al., 2018) to 768 (Eadie, 2017). The average age of children was 5.78 years (SD = 2.44), and 42% were female. The majority of studies were targeted to children of preschool stage (n = 15, aged 3–5 years) and school age (n = 13, aged 5+ years). Three studies were specifically targeted for toddlers (1–3 years, Kohlhoff et al., 2020, 2021; Lauw et al., 2014). The remaining 11 studies included children across various ages and stages encompassing 1–9 years. Children were exhibiting either externalising behaviours (n = 20) or internalising/emotional symptoms (n = 14) or both (n = 8). Emotional concerns included anxiety symptoms (n = 6) or a diagnosed anxiety disorder (n = 6, social anxiety, social phobia or generalised anxiety), rather than depressive symptoms (n = 1). The specific types of externalising behaviours were not reported.
The mean age of the primary caregiver reported across 22 studies was 37.20 (SD = 3.47). The large majority of caregivers (83%) who participated in the intervention and completed parent-reported questionnaires across the studies identified as the child’s mother or female primary caregiver. Less than a third of studies (n = 13) reported the ethnicity of children and caregivers. Aboriginal and/or Torres Strait Islander children and families were consistently underrepresented across these studies (7% of the overall sample), with one study evaluating a programme that was delivered specifically to Aboriginal children (Wicks et al., 2018).
Intervention characteristics
The majority of interventions were group programmes (n = 30), delivered to the child’s primary caregiver (n = 25). Programmes that were specifically delivered to the child (n = 10) also included a caregiver component, such as separate parenting sessions or coaching. Support was delivered to the whole family in eight studies. On average, support was delivered weekly for 90 minutes over 11 weeks (SD = 8.33), ranging from a one-off 2-hour session (Dittman et al., 2016) to 18 months of multidisciplinary support (Eadie, 2017). Interventions were delivered by psychologists in 40 of the 42 studies, and 2 included a multidisciplinary team (Eadie, 2017; Watt et al., 2012). The content of programmes is described herein, with interventions grouped according to their aim and type of mental health concern that they sought to address. The 42 studies evaluated 16 different types of programmes that targeted (1) externalising behaviour (n = 20 studies, n = 6 programmes), (2) internalising symptoms (n = 14 studies, n = 7 programmes) or (3) both, termed transdiagnostic programmes (n = 8 studies, n = 3 programmes).
Externalising programmes
In all, 20 of 42 studies assessed six programmes that aimed to support children exhibiting externalising behaviours. Four of the six interventions were manualised group-based parenting programmes, facilitated by psychologists. Five studies evaluated 1-2-3 Magic, where caregivers were taught various techniques to manage misbehaviour, elicit and reinforce desirable behaviour, and strengthen the parent–child relationship (Bailey et al., 2012, 2015; Chesterfield et al., 2020; Porzig-Drummond et al., 2014, 2016). In Dealing with Disobedience, parents received psychoeducation and behaviour management strategies via interactive and discussion-based sessions (Dittman et al., 2016). Six studies evaluated Tuning into Kids: a six-session manualised emotion-focused group parenting programme to help parents respond to and manage their child’s behaviours. Caregivers were taught the five steps of emotion coaching via a series of exercises, handouts, role plays, group discussion, DVD examples and psychoeducation. Three studies evaluated this standard protocol (Duncombe et al., 2016; Havighurst et al., 2013; Wilson et al., 2012), while three studies tailored the programme for fathers (‘Dads Tuning into Kids’, Havighurst et al., 2019; Wilson et al., 2016) or caregivers of toddlers (‘Tuning into Toddlers’, Lauw et al., 2014).
Two studies assessed the Positive Parenting Program (Triple P), a group programme for caregivers that covered key strategies to enhance the caregiver–child relationship, encourage desirable behaviour, and manage misbehaviour. Duncombe et al. (2016) compared the behavioural-focused Triple P programme with the emotion-focused Tuning into Kids. Stallman and Sanders (2014) adapted Triple P for families following caregiver separation/relationship breakdown. Finally, six studies evaluated PCIT, which involved in vivo coaching of caregivers. Parents were first taught interactional parent skills during 12 observed play sessions with the child in the Child-Directed Interaction phase, followed by behaviour management strategies in the Parent-Directed Interaction phase (Thomas and Zimmer-Gembeck, 2012). One study adapted PCIT for children exhibiting externalising behaviour and callous-unemotional traits (Kimonis et al., 2018); and two studies assessed PCIT for toddlers, in which only the Child-Directed Interaction phase was evaluated (Kohlhoff et al., 2020, 2021). Thomas and Zimmer-Gembeck (2012) assessed the standard protocol, Webb et al. (2017) added three motivation enhancement sessions to the standard PCIT protocol, and the final study evaluated the time-variable PCIT protocol, where treatment continued until mastery of key skills was achieved (Thomas and Zimmer-Gembeck, 2011). Finally, Watt et al. (2012) evaluated Child and Youth Mental Health Services for children with severe conduct concerns, which included a range of intensive clinical and therapeutic supports from a multidisciplinary team.
Internalising programmes
In all, 14 of 42 studies assessed seven different group programmes (five for children and two for caregivers) that aimed to support children experiencing internalising symptoms, particularly anxiety. Seven studies evaluated Cool Little Kids, a structured skills-based parenting group programme for child anxiety that involved psychoeducation, cognitive restructuring, exposure, and social and problem-solving skills (Bayer et al., 2018, 2020, 2021; Jarosz and Bayer, 2019; Lau et al., 2017; Rapee, 2013; Rapee et al., 2021). Lau et al. (2017) complemented Cool Little Kids with child-only group play sessions focused on social skills. Cobham et al. (2017) evaluated Fear-Less Triple P, a CBT group programme for parents of a child with an anxiety disorder.
For the five child-focused group programmes, two studies evaluated the Fun FRIENDS programme, which comprised 10 group sessions of play-based activities for children with an anxiety disorder (Barrett et al., 2015) or any internalising symptoms (Fisak et al., 2018). The Shy intervention was an intensive CBT-based programme for children experiencing social phobia, which included combined and separate child and caregiver groups (Donovan et al., 2015). Holmes et al. (2014) evaluated the No Worries! Program, a 10-session manualised CBT treatment for children with Generalised Anxiety Disorder. The Secret Agent Society programme was a 9-week group therapy programme for children with social anxiety, which taught emotional regulation and social interaction skills through a series of spy-theme information, activities and games (Beaumont et al., 2019). Finally, Farrell et al. (2018) evaluated single session treatment for specific phobia which incorporated play-based activities and graduated in vivo exposure tasks. These programmes were complemented by a separate parent component (i.e. group sessions or follow-up support) to reinforce the children’s implementation of learnt skills at home.
Transdiagnostic programmes
Eight studies evaluated three types of programmes for children with either or both internalising and externalising symptoms, and targeted the risk factors related to the child’s presenting concerns (e.g. parent–child attachment). Five studies examined Circle of Security, an attachment-focused group parenting programme. Huber et al. (2015a, 2015b) evaluated the standard 20-week programme comprising psychoeducation on attachment theory and exploration of individualised videos of each parent–child dyad. The other three studies evaluated the Circle of Security Parenting Program – a less-intensive eight-session adapted version of the original programme (Krishnamoorthy et al., 2020; Maxwell et al., 2021; Zimmer- Gembeck et al., 2021). Two studies assessed the impact of intensive child-centred play therapy for children who had experienced trauma with emotional and behavioural concerns (Ritzi et al., 2017; Wicks et al., 2018). The final study evaluated Evolve Therapeutic Service, a trauma-informed wrap-around model of care where a multidisciplinary team provided coordinated and systemic attachment and trauma-focused support to children in out-of-home care exhibiting severe and complex emotional and behavioural concerns (Eadie, 2017).
Control group characteristics
Twenty-seven studies included a control group. Of these, 20 studies implemented a wait-list control group where participants received the intervention after an extended waiting period during which no treatment was delivered (n = 16) or caregivers received weekly brief telephone check-ins (n = 4, Thomas and Zimmer-Gembeck, 2011, 2012; Webb et al., 2017; Zimmer-Gembeck et al., 2021). The waiting period often lasted the duration of the intervention, with an average waiting time of 12 weeks, ranging from 2 weeks (Ritzi et al., 2017) to 10 months (Havighurst et al., 2019). Six studies included standard or usual care. This encompassed access to support services in the community as needed, such as seeing a paediatrician for child behaviour management strategies (Bayer et al., 2018, 2020, 2021; Havighurst et al., 2013; Rapee, 2013). Rapee et al. (2021) used an active control group – Low Intensity Treatment, where parents received a detailed workbook describing strategies to help their child and four 30-minute telephone coaching sessions, as a control for the Cool Little Kids programme.
Intervention impact
This review examined externalising and internalising outcomes experienced by the child. The Eyberg Child Behaviour Inventory was most commonly used to assess externalising behaviours and their frequency (n = 14), followed by the Strengths and Difficulties Questionnaire (n = 10) and Child Behaviour Checklist (n = 10). For internalising outcomes, studies predominantly examined the presence of an anxiety disorder diagnosis using the Anxiety Disorders Interview Schedule for Children (n = 9), general internalising symptoms were measured by the Strengths and Difficulties Questionnaire (n = 9), anxiety symptoms were assessed by the Spence Children’s Anxiety Scale (n = 8) and depressive symptoms were measured by the Children’s Mood and Feelings Questionnaire (n = 5). No studies assessed externalising disorder or depressive disorder diagnosis. All studies relied on caregiver-report. Thirteen studies also utilised a clinician-rated measure, yet few studies incorporated child-reported (n = 6) or teacher-reported (n = 5) measures. Intervention efficacy was synthesised according to each intervention category (externalising or internalising programmes), for each outcome category in turn. The results of the meta-analyses of RCTs are presented first, followed by a narrative synthesis of findings from the remaining non-randomised studies. Meta-analyses show high rates of heterogeneity across studies, yet limited indication of publication bias.
Externalising programmes
Fourteen RCTs evaluating programmes targeting externalising behaviours were included in meta-analyses. Thirteen RCTs examined externalising symptoms, and 11 measured the frequency of externalising behaviours. Figures 2 and 3 show significant moderate mean effect sizes in favour of the intervention groups, with children experiencing significantly fewer externalising symptoms (SMD = −0.56, 95% CI = [−0.79, −0.32], p < 0.00001) and at a reduced frequency (SMD = −0.54, 95% CI = [−0.79, −0.28], p < 0.0001) in comparison to the control groups. Four RCTs, all examining PCIT, also observed significant reductions in general internalising symptoms between groups (Kohlhoff et al., 2021; Thomas and Zimmer-Gembeck, 2011, 2012; Webb et al., 2017).
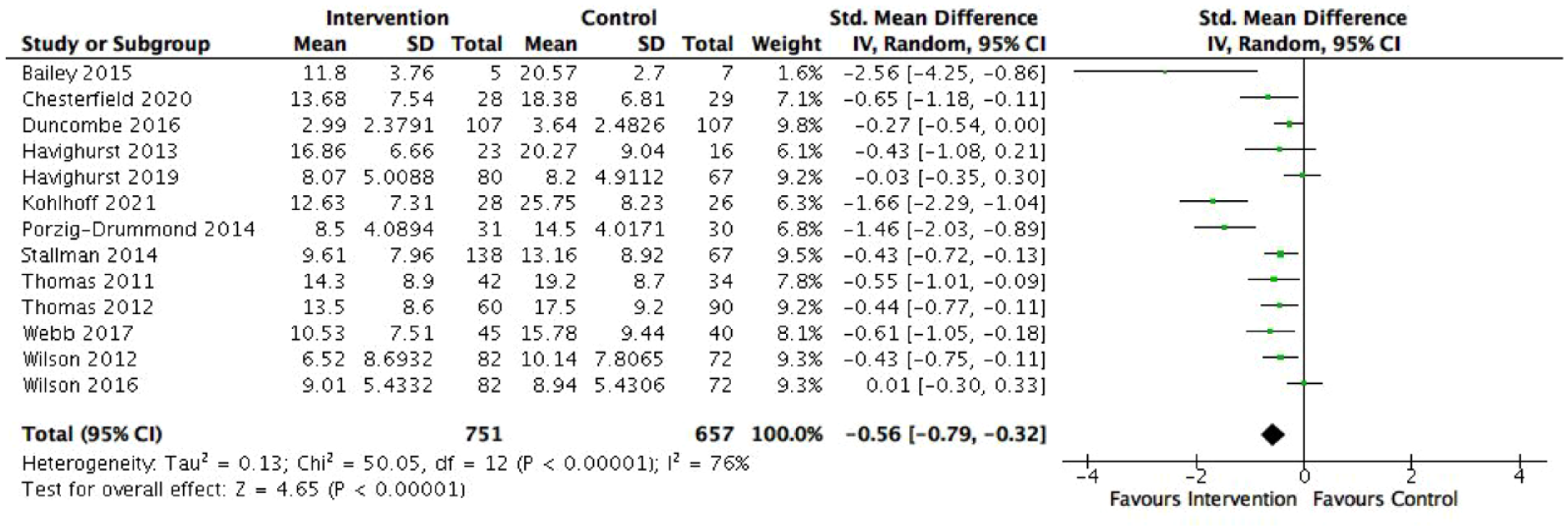
Effect of externalising programmes on externalising symptoms.
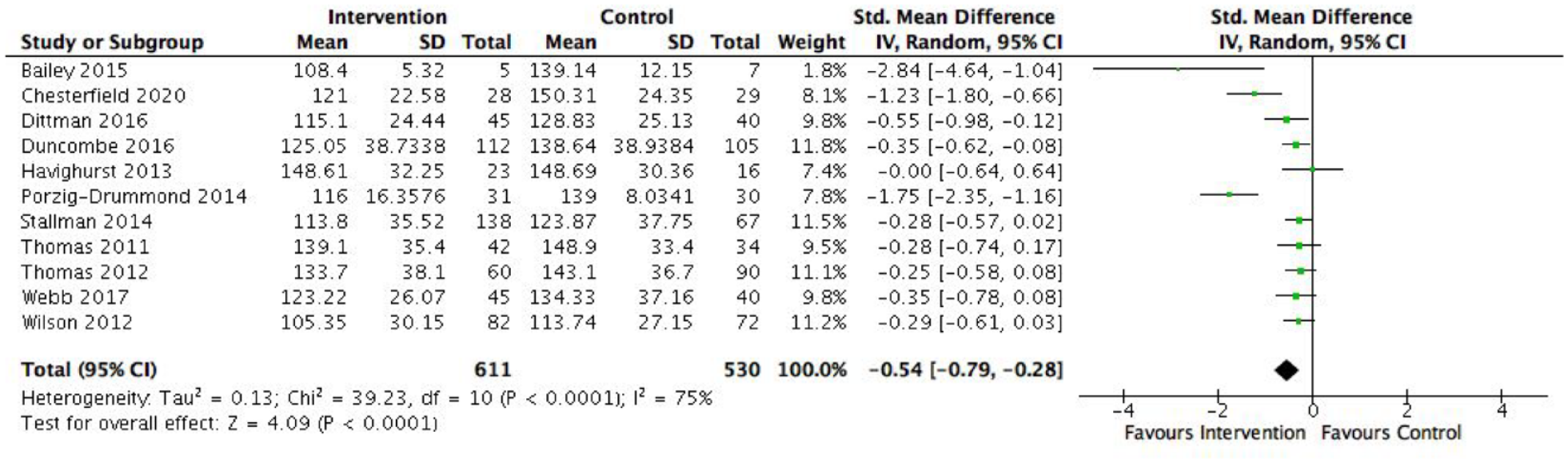
Effect of externalising programmes on the frequency of externalising behaviours.
Meta-analyses could not be conducted for the remaining studies due to limited power. Four out of the five non-RCT studies observed significant reductions in parent-reported externalising behaviours among children following the intervention, including 1-2-3 Magic (Porzig-Drummond et al., 2016), PCIT (Kimonis et al., 2018; Kohlhoff et al., 2020) and Tuning into Toddlers (Lauw et al., 2014). However, the Child and Youth Mental Health Service was not associated with significant improvements in children’s externalising behaviours (Watt et al., 2012). Kohlhoff et al. (2020) found a significant reduction in children’s general internalising symptoms following participation in PCIT.
Internalising programmes
Seven RCTs evaluating internalising programmes were included in the meta-analysis (Bayer et al., 2018, 2020, 2021; Cobham et al., 2017; Holmes et al., 2014; Lau et al., 2017; Rapee et al., 2021). All seven studies measured anxiety symptoms and anxiety disorder diagnoses. Children from the intervention groups were 57% less likely to have an anxiety disorder diagnosis following treatment than control children (OR = 0.57, 95% CI = [0.35, 0.93], p = 0.03, see Figure 4). This corresponds to an NNT of 1.35. However, the three studies that evaluated Cool Little Kids on the same sample found no significant differences in anxiety disorder diagnosis between intervention and control children immediately post-programme (Bayer et al., 2018), after 24 months (Bayer et al., 2020), nor at middle childhood follow-up (Bayer et al., 2021). Figure 5 shows a small mean effect size for the reduction of anxiety symptoms in favour of the intervention group (SMD = −0.25, 95% CI = [−0.43, −0.08], p = 0.005). Only one out of four RCTs reported statistically significant reductions in general internalising symptoms among children who received Fear-Less Triple P compared with the control group (Cobham et al., 2017). Depressive symptoms and diagnosis were not examined by the RCTs, and therefore not included in meta-analyses.
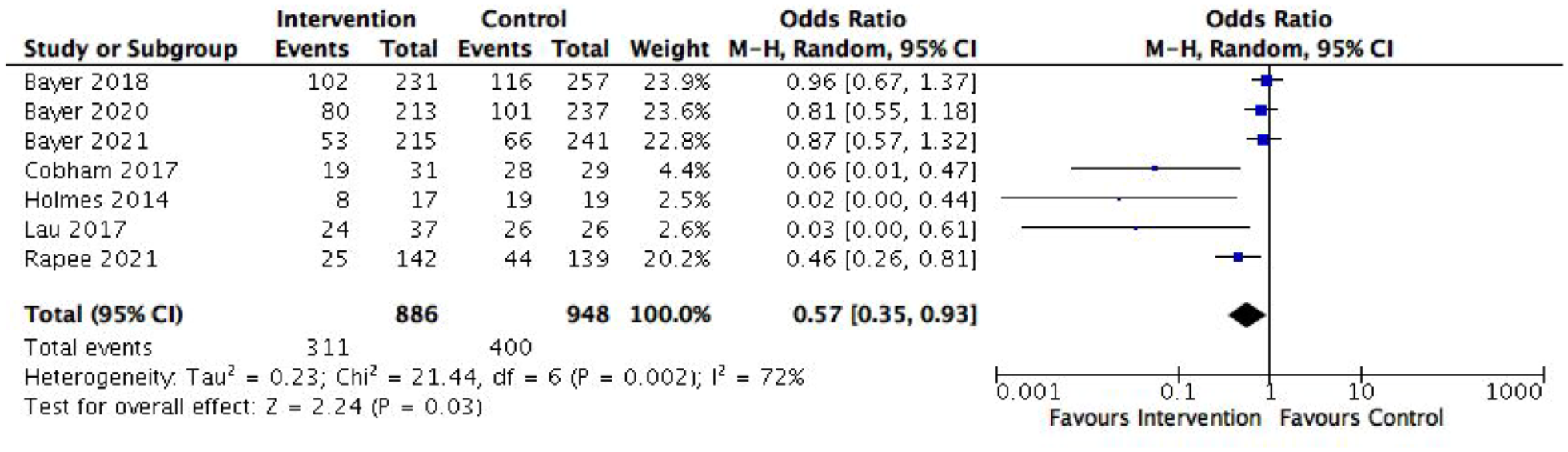
Effect of internalising programmes on anxiety disorder diagnosis.
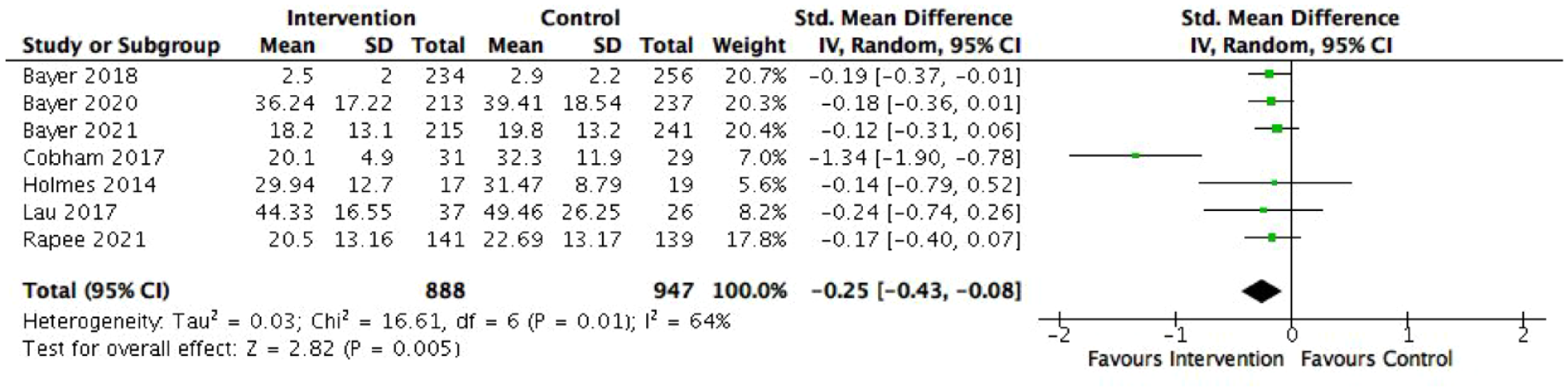
Effect of internalising programmes on anxiety symptoms.
Six uncontrolled studies were included in the meta-analysis. 2 Figure 6 shows a moderate mean effect size for the reduction of anxiety symptoms among children over time, following their engagement in the internalising programme (SMD = 0.76, 95% CI = [0.56, 0.96], p < 0.00001). Specifically, Donovan et al. (2015) found that while parents reported improvements in their children’s anxiety, there were no significant differences in children’s self-report of anxiety symptoms following participation in the Shy group programme. One study found the opposite pattern – while children self-reported a significant improvement, there were no differences in parent-report (Beaumont et al., 2019). The remaining outcomes used to evaluate the internalising programmes (i.e. anxiety disorder diagnosis, depressive symptoms and externalising behaviours) were not included in meta-analyses due to limited power. All three studies evaluating Fun Friends (Barrett et al., 2015), Shy (Donovan et al., 2015) and Cool Little Kids group programmes (Rapee, 2013) found a significant reduction in the percentage of children who met criteria for an anxiety disorder diagnosis. Rapee (2013) found that girls were less likely to meet criteria than boys. Five of six studies found a significant reduction in child anxiety symptoms from parent-reported measures (Barrett et al., 2015; Donovan et al., 2015; Farrell et al., 2018; Fisak et al., 2018; Jarosz and Bayer, 2019; Rapee, 2013). All four studies found significant improvements in general internalising symptoms (Barrett et al., 2015; Donovan et al., 2015; Fisak et al., 2018; Jarosz and Bayer, 2019). However, only one out of three pre–post studies found a significant reduction in children’s depressive symptoms (Barrett et al., 2015). The three studies that examined the effect of Fun Friends (Fisak et al., 2018) and Cool Little Kids (Barrett et al., 2015; Jarosz and Bayer, 2019) on externalising behaviours found significant improvements.

Effect of internalising programmes on general internalising symptoms.
Transdiagnostic programmes
There was insufficient data to conduct meta-analysis of the transdiagnostic programmes (i.e. only two RCTs, different outcomes and measures), so the findings have been detailed descriptively. Five of eight studies evaluating interventions for children presenting with both or either types of symptoms achieved at least one significant outcome. Six of eight studies (two RCTs, one quasi-experimental and three pre–post) evaluated externalising behaviours (Huber et al., 2015b; Krishnamoorthy et al., 2020; Maxwell et al., 2021; Ritzi et al., 2017; Wicks et al., 2018; Zimmer-Gembeck et al., 2021) and five studies (one RCT and four pre–post) assessed general internalising symptoms (Eadie, 2017; Huber et al., 2015b; Krishnamoorthy et al., 2020; Wicks et al., 2018; Zimmer- Gembeck et al., 2021). Two pre–post studies measured parent–child attachment (Huber et al., 2015a; Krishnamoorthy et al., 2020).
Three of six studies (one RCT and two pre–post) found improvements in teacher- and parent-reported externalising behaviours among children who participated in Intensive Play Therapy and Circle of Security (Huber et al., 2015b; Ritzi et al., 2017; Wicks et al., 2018). The adapted Circle of Security Parenting program did not yield any improvements in externalising behaviours via RCT (Zimmer- Gembeck et al., 2021), quasi-experimental (Maxwell et al., 2021) nor pre–post evaluation (Krishnamoorthy et al., 2020). Four of five studies (all pre–post) observed significant reductions in children’s internalising symptoms on both parent and teacher-report measures post-treatment (Eadie, 2017; Huber et al., 2015b; Krishnamoorthy et al., 2020 parent; Wicks et al., 2018). Both the standard and adapted versions of Circle of Security did not identify any significant improvements in parent–child attachment (Huber et al., 2015a; Krishnamoorthy et al., 2020).
Discussion
This is the first systematic review to synthesise the Australian evidence base of targeted community-based mental health programmes for children aged under 9 years exhibiting emotional and/or behavioural concerns. This review aimed to (1) describe the types of targeted community-based mental health programmes for Australian children aged 1–9 years exhibiting emotional/internalising symptoms and/or externalising behaviour concerns and (2) examine their impact on children’s externalising and internalising outcomes (disorder diagnosis and symptomatology). A total of 42 studies were included, which evaluated 16 targeted programmes that focused on addressing externalising symptoms (n = 20 studies, n = 6 programmes), (2) internalising symptoms (n = 14 studies, n = 7 programmes) or (3) both, termed transdiagnostic programmes (n = 8 studies, n = 3 programmes). Overall, this review highlighted the significant quantity and quality of this area of Australian research conducted in the past decade, with 24 RCT studies identified, and 88% of studies assessed as having medium or high methodological quality.
The findings from the meta-analyses indicate that the programmes which specifically targeted externalising symptoms achieved moderate reductions in children’s externalising behaviours (Bailey et al., 2015; Chesterfield et al., 2020). These findings align with the non-RCT studies, as the majority of studies observed significant reductions in children’s externalising behaviours post-programme. These findings are consistent with the extensive international evidence base that supports parenting programmes in enhancing the knowledge, skills and confidence of caregivers to address children’s behaviour problems (Sanders et al., 2014; Ward et al., 2016). For example, Uretsky and Hoffman (2017) found that group parenting programmes had a small to medium effect on American children’s externalising behaviours. The findings also provide ongoing support for the implementation and effectiveness of these parenting programmes in the Australian context. It is acknowledged that no included studies assessed externalising disorder diagnoses (e.g. child oppositional defiant disorder or conduct disorder) as an outcome. Indeed, there are numerous additional programmes being implemented across Australia that lack rigorous evaluation of disorder-related outcomes (e.g. The Getting on Track in Time GotIt! programme for children with conduct disorder, NSW Ministry of Health, 2017). Therefore, future Australian research may be needed to examine whether these interventions remain effective for young children who already meet criteria for externalising disorders, as shown internationally (Ward et al., 2016). Nonetheless, it is clear that targeted prevention and early intervention is imperative to address behavioural symptoms in early childhood, and reduce the likelihood of later mental health disorder development (Colizzi et al., 2020; Whalen et al., 2017).
The meta-analyses findings show that programmes targeting internalising symptoms were associated with small but significant reductions in anxiety symptoms, and reduced risk of anxiety disorder diagnosis (e.g. Cobham et al., 2017). Children from the intervention group had 57% reduced odds of meeting criteria for an anxiety disorder compared with the control group. This corresponded to an NNT of 1, which means that for every child who engages in an internalising programme, one additional child could be free of an anxiety diagnosis, relative to children who do not engage. This is similar to international findings, with a previous meta-analysis identifying children had 48% reduced risk of internalising disorder diagnosis (either depression or anxiety) following targeted intervention (Stockings et al., 2015). Furthermore, for the non-RCT studies, meta-analyses findings show a significant moderate mean reduction in children’s symptoms of anxiety post engagement in the internalising programmes. However, there was limited evidence for such programmes in addressing depressive symptoms, as no RCTs evaluated this outcome and only one of three non-RCTs reported significant findings (Barrett et al., 2015). This is likely due to floor effects of depressive symptoms (i.e. low baseline levels), and because the internalising programmes were predominantly focused on supporting children experiencing anxiety. Anxiety is significantly more common among young children, and can also predict later internalising distress, including depression (Whalen et al., 2017). Nonetheless, previous international reviews of targeted programmes have observed significant improvements in depressive symptoms and disorders among young children (e.g. Stockings et al., 2015). Therefore, future research is needed to evaluate the effect of such programmes on the mood and depressive symptoms among young Australian children.
There was insufficient research to conduct meta-analyses for the transdiagnostic programmes. While these studies yielded significant improvements in internalising symptoms as opposed to externalising behaviours (e.g. Eadie, 2017; Wicks et al., 2018), more evidence is needed before more definitive conclusions can be made about the effectiveness of transdiagnostic programmes for young Australian children. These programmes primarily targeted the common risk factors associated with emotional and behavioural concerns, particularly parent–child attachment. While not a primary outcome focus of this review, there was a lack of evaluation of parent–child attachment across studies, and most of the studies that did measure it did not find significant improvements in this area (e.g. Circle of Security, Huber et al., 2015a; Krishnamoorthy et al., 2020), despite promising international evidence (Yaholkoski et al., 2016). The authors propose that this may likely be due to the timing of the assessment immediately post-intervention, as a longer follow-up period may be required to capture observable changes in the parent–child relationship. Early childhood insecure attachment style is associated with mental health difficulties in adolescence and young adulthood (Clery et al., 2021). Therefore, community-based interventions that foster the development of secure attachment can not only improve attachment quality and symptomatology among children, but also reduce the likelihood of mental health difficulties in later life (Eadie, 2017). Greater commitment to addressing and measuring attachment (i.e. long-term follow-up) is recommended to ensure such programmes are addressing one of the core underpinnings of children’s emotional or behavioural difficulties.
The majority of identified targeted community-based interventions were parenting-focused programmes. The findings confirm that existing international evidence-based programmes can effectively address the internalising and externalising symptoms among Australian children (e.g. 1-2-3 Magic, PCIT, Bailey et al., 2012; Kohlhoff et al., 2020, 2021). The commonality across such programmes is that caregivers are taught various strategies to respond to and manage children’s behaviours and emotions. Caregivers are key to identifying internalising and externalising behaviours among young children, and their parenting behaviours and relationship quality with the child can heavily influence the presence and severity of these symptoms (Yap and Jorm, 2015). Programmes that include a caregiver component, either alone or in combination with a child-focused component, have become well-established as a gold-standard form of early intervention for young children exhibiting signs of mental ill health, particularly externalising behaviours (Chronis-Tuscano et al., 2015; Lau et al., 2017). The limited child-focused programmes reviewed suggest that direct intervention with young children (e.g. play therapy) is particularly effective for the reduction of internalising symptoms. These programmes also focused on promoting general wellbeing and resilience to improving children’s mental health trajectories (Barrett et al., 2015). Other reviews have found equivocal evidence about whether combined parenting education and direct child intervention provides significantly greater benefits (Chronis- Tuscano et al., 2015; Lau et al., 2017; Yap et al., 2016).
The current findings indicate that targeted community-based mental health programmes are effective in addressing internalising and externalising symptoms among young children. However, a significant gap in the dissemination and evaluation of such programmes for vulnerable and disadvantaged young children and families in Australia has been identified. There was a lack of diversity across the samples, including minimal representation of Aboriginal and Torres Strait Islander children, other culturally and linguistically diverse (CALD) children, families from low socio-economic backgrounds, rural and remote areas or experiencing other vulnerabilities (e.g. parental mental illness, family violence). As children’s difficulties often arise as a result of their environment and early family experiences (Paclikova et al., 2019), community-based programmes delivered during early childhood must target these social and intergenerational risk factors (Ritzi et al., 2017). Only one study evaluated a holistic wrap-around family support programme (Eadie, 2017). Emerging international research suggests that integrated and multidisciplinary models of mental health care that deliver early prevention and intervention for disadvantaged young children can address barriers to access/engagement and prevent ongoing mental health concerns (Ogundele, 2018). A community-driven systemic wrap-around approach may be needed to address the underpinning psychosocial determinants of early symptoms of mental ill health among Australian children (NMHC, 2020).
Limitations
The findings of this review have highlighted some limitations of this body of literature. First, a key limitation was the lack of engagement of fathers or male caregivers in the programmes reviewed. Fathers help shape their children’s emotional development, and are often less likely than mothers to talk about emotions with their children and more likely to be emotionally dismissive of their child’s emotions/behaviours (Havighurst et al., 2019). Even when both parents were invited to participate, only the mothers attended for the large majority (e.g. Cobham et al., 2017), despite evidence that fathers are more likely to engage in such programmes if their partner also participates (McKee et al., 2021). Internationally, limited evidence-based paternal-focused interventions are available, of which few have yielded promising results. Nonetheless, one programme reviewed specifically targeted fathers – Dads Tuning into Kids – facilitated significant reductions in children’s externalising behaviours (Havighurst et al., 2019; Wilson et al., 2016). Higher levels of caregiver participation predict greater improvements in caregiver–child relationship and attachment quality (Haine-Schlagel et al., 2021). Greater efforts, commitment or targeted strategies to adapt programmes to better suit and engage male caregivers are needed to enhance programme uptake and success (Hansen et al., 2019).
A third limitation was the lack of triangulation of outcome measures, with all studies predominantly relying only on caregiver-reported measures of child symptoms. For the few studies that incorporated multiple informants, there were often differences in findings between caregiver, child, clinician and teacher-report (e.g. Donovan et al., 2015; Rapee et al., 2021). Previous meta-analyses have indicated low to moderate correlation between informants on child mental health outcome measures, suggesting that children may display emotional and behavioural concerns in some contexts and not others (e.g. home vs childcare/education settings, De Los Reyes et al., 2015). Young children may provide less accurate and reliable information about their mental health contributing to nonsignificant effects on child-reported measures, particularly internalising symptoms (Donovan et al., 2015). Nonetheless, the validity of a multi-informant approach to assessing child mental health is particularly useful for assessing observable externalising symptoms (De Los Reyes et al., 2015). Future programme evaluations should ensure triangulation of outcome measures by using various informants to increase validity and better understand children’s mental health across contexts.
There was a consistent lack of reporting of implementation and adherence to intervention protocols. This reduces the quality of the literature as it was often unclear how some programmes were implemented, or whether they were delivered with fidelity. The effectiveness of a programme can be significantly diluted if participants do not receive the intervention as intended, and even manualised interventions may not necessarily translate well into real-world applications (Rojas-Andrade and Bahamondes, 2019). Authors of included studies often reported that the sample sizes of their studies were too small to provide confidence in the findings. Ensuring successful implementation and uptake is necessary when scaling-up or translating mental health programmes across various cohorts and contexts. It is necessary that future research focuses on assessing the implementation of targeted community-based mental health programmes with larger and more diverse cohorts of children, while reporting on adherence and fidelity to minimise replication failure. Finally, the heterogeneity of studies included in this review, in terms of the various outcomes, measures, types of interventions and baseline symptom severity, is a key limitation of the current findings. Given this, the results need to be interpreted with caution and with an understanding of the various factors that may have influenced or moderated such outcomes (e.g. varying participant and intervention characteristics), which could not be further explored in the current meta-analysis due to limited statistical power. Nonetheless, this review has highlighted key learnings, insights, limitations and recommendations for future work from this body of literature.
Implications
The current findings indicate that targeted community-based mental health programmes can alleviate young children’s emotional and behavioural difficulties. Externalising programmes achieved significant reductions in externalising behaviours, internalising programmes yielded small improvements in anxiety symptoms and reduced odds of anxiety disorder diagnosis, while the evidence supporting transdiagnostic programmes was inconclusive. These findings may be used to inform the adaptation, scale-up or translation of community-based mental health programmes for young children exhibiting symptoms, particularly those from vulnerable or disadvantaged cohorts who were underrepresented in the reviewed studies. This is consistent with reports that mental health supports that are available are consistently not reaching the children and families who are in greatest need (Australian Government, 2021). As these vulnerable cohorts are at higher risk of emotional and behavioural difficulties (AIHW, 2020), modifications to existing programmes may be required to reflect the complexities and adversities experienced by children to more effectively meet their needs. It is necessary that targeted community-based mental health programmes are appropriately adapted with cultural, ethnic, psychosocial, and trauma-informed competency and sensitivity for families experiencing disadvantage. While these interventions may already be delivered across Australia, there is significant need for high-quality evaluations with such cohorts to build their evidence base and inform future practice. Greater implementation and evaluation of community-driven systemic, coordinated and integrated wrap-around approach that intervenes at the child, parent, family and community level are needed (Hall et al., 2021). This approach may better identify, reach and engage vulnerable children and families to address the psychosocial determinants (e.g. adverse childhood experiences) and persistent disadvantage underpinning their emotional and behavioural concerns (Hall et al., 2021; NMHC, 2020; Sahle et al., 2021a, 2021b). These implications align with Australia’s first National Children’s Mental Health and Wellbeing Strategy for children aged 0–12 years, in which stronger holistic community-driven approaches to children’s mental health is a key priority (Australian Government, 2021).
Conclusion
This review has evaluated the types and effectiveness of targeted community mental health programmes for young Australian children. The findings confirm that parenting-focused programmes that target young children’s internalising or externalising behaviours are the most commonly evaluated intervention type and have the largest local evidence base supporting their effectiveness. Key limitations and recommendations for future research and practice have been provided, including greater engagement of fathers, triangulation of outcomes and greater transparency in implementation reporting. Against a backdrop of limited availability and use of mental health support by young children in Australia despite increasing need (Australian Government, 2021), the current findings support the necessity of adapting and improving dissemination of targeted community-based mental health programmes for vulnerable children. Tailoring, adapting, implementing and evaluating integrated and systemic community-based approaches that successfully identify, reach, engage and support Australia’s most disadvantaged cohorts of children and families is crucial to improve their trajectory.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221124506 – Supplemental material for Targeted community-based programmes for children’s mental health: A systematic review and meta-analysis of the Australian literature
Supplemental material, sj-docx-1-anp-10.1177_00048674221124506 for Targeted community-based programmes for children’s mental health: A systematic review and meta-analysis of the Australian literature by Melissa Savaglio, Marie BH Yap, Renee O’Donnell and Helen Skouteris in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Melissa Savaglio is funded by a National Health and Medical Research Council (NHMRC) Postgraduate Scholarship. The authors received no additional financial support for the research, authorship and/or publication of this article.
Data Availability
Data sharing is not applicable to this work as it is a systematic literature review, so no datasets were generated or analysed.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.