
Abstract
Even with optimal treatment, some persons with severe and persistent mental illness do not achieve a level of mental health, psychosocial functioning and quality of life that is acceptable to them. With each unsuccessful treatment attempt, the probability of achieving symptom reduction declines while the probability of somatic and psychological side effects increases. This worsening benefit–harm ratio of treatment aiming at symptom reduction has motivated calls for implementing palliative approaches to care into psychiatry (palliative psychiatry). Palliative psychiatry accepts that some cases of severe and persistent mental illness can be irremediable and calls for a careful evaluation of goals of care in these cases. It aims at reducing harm, relieving suffering and thus improving quality of life directly, working around irremediable psychiatric symptoms. In a narrow sense, this refers to patients likely to die of their severe and persistent mental illness soon, but palliative psychiatry in a broad sense is not limited to end-of-life care. It can – and often should – be integrated with curative and rehabilitative approaches, as is the gold standard in somatic medicine. Palliative psychiatry constitutes a valuable addition to established non-curative approaches such as rehabilitative psychiatry (which focuses on psychosocial functioning instead of quality of life) and personal recovery (a journey that persons living with severe and persistent mental illness may undertake, not necessarily accompanied by mental health care professionals). Although the implementation of palliative psychiatry is met with several challenges such as difficulties regarding decision-making capacity and prognostication in severe and persistent mental illness, it is a promising new approach in caring for persons with severe and persistent mental illness, regardless of whether they are at the end of life.
Keywords
Introduction
Due to advances in psychiatry over the last decades, there are now evidence-based treatment options for nearly all mental disorders. However, in some cases of severe and persistent mental illness (SPMI; Zumstein and Riese, 2020), treatment response is not sufficiently good to alleviate patients’ suffering and improve their psychosocial functioning and quality of life to a level they deem acceptable. With each unsuccessful treatment attempt, the evidence base for further treatment becomes thinner and the probability of achieving symptom reduction declines (Kahn et al., 2018; Rush et al., 2009) while the probability of side effects increases. The latter include medication side effects (e.g. metabolic syndrome from antipsychotics contributing to the excess mortality of persons with SPMI; Correll et al., 2017) and psychological side effects (e.g. a sense of failure and hopelessness which can worsen the underlying SPMI, for instance in chronic depression; Berk et al., 2012). Thus, the benefit–harm ratio of treatment aiming at symptom reduction worsens with each failed attempt, which has prompted calls for palliative approaches in psychiatry (palliative psychiatry; Berk et al., 2012; Levitt and Buchman, 2021; Lindblad et al., 2019; Trachsel et al., 2016; Westermair et al., 2021).
Like preventive psychiatry (Trivedi et al., 2014) and rehabilitative psychiatry (Roessler, 2006), palliative psychiatry is a subdiscipline of psychiatry. The basic assumptions and principles of palliative psychiatry are as follows:
SPMI (symptoms) 1 can, in some cases, be irremediable, i.e., unresponsive to optimal treatment.
Ineffective and burdensome interventions should not automatically be continued but necessitate a careful evaluation and possibly a change of the goals of care (Westermair et al., 2021).
When symptom reduction is in all likelihood unattainable, quality of life becomes the priority and thus the yardstick for assessing possible interventions (Trachsel et al., 2016).
Of course, curative psychiatry, too, aims at improving patients’ quality of life. The difference lies in the strategies that are applied in working towards that goal: whereas curative psychiatry strives at improving quality of life by way of symptom reduction or even complete remission, 2 palliative psychiatry aims at relieving suffering and thus improving quality of life directly by working around irremediable SPMI symptoms (see Figure 1).
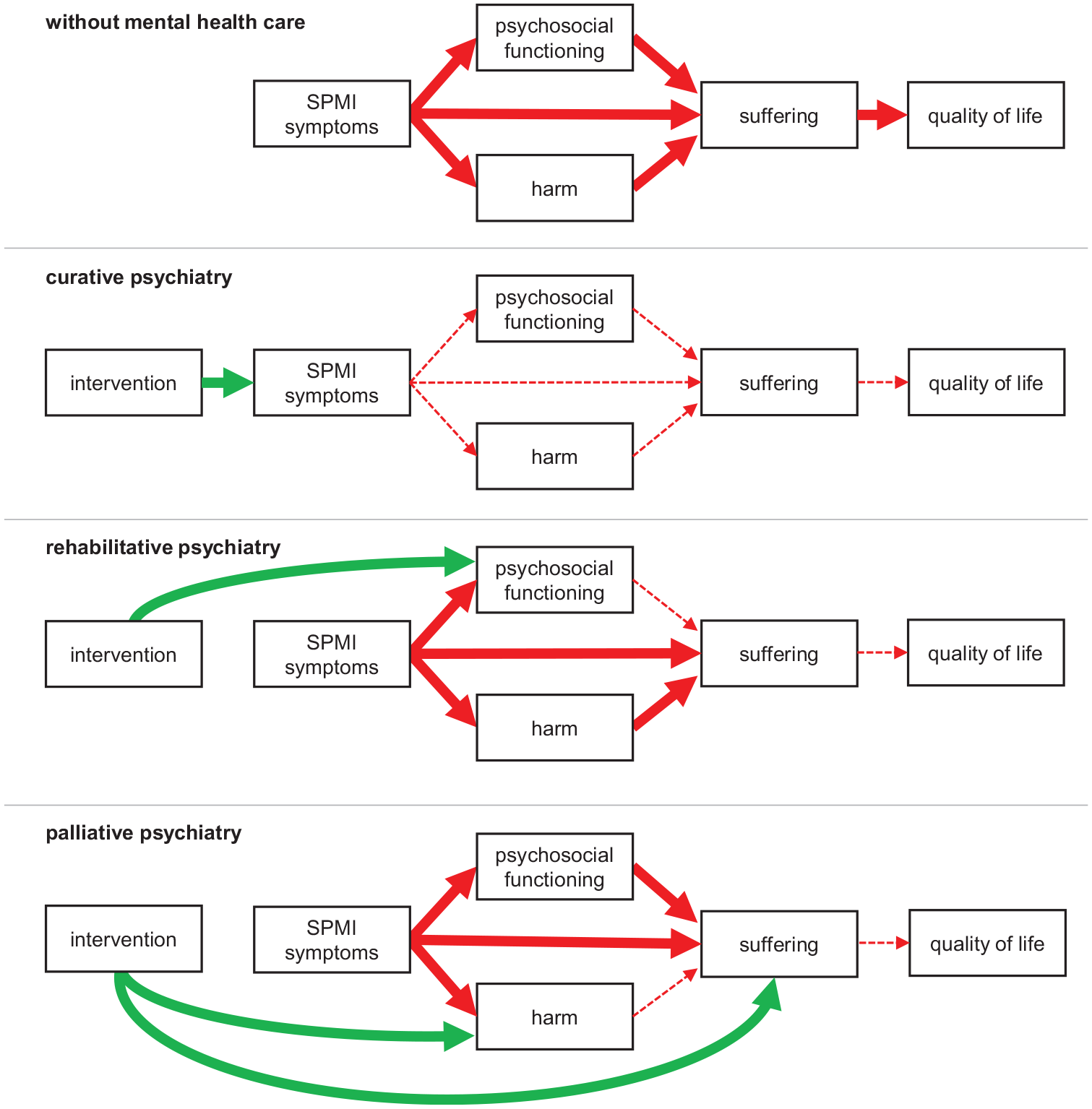
Conceptual overview of different approaches to mental health care.
The current debate about the necessity to establish palliative psychiatry (Berk et al., 2012; Lindblad et al., 2019; Trachsel et al., 2016; Trauer, 2012) should be based on conceptual clarity (Gieselmann and Vollmann, 2020). As the concept of palliative care itself has undergone considerable change since its emergence, the notion of palliative psychiatry may take on different meanings depending on which concept of palliative care one relies on. In what follows, we will summarize the early and the modern concept of palliative care and then apply them to psychiatry.
A brief history of palliative care
When Cicely Saunders founded the first modern hospice in 1967, the concept was readily embraced in high-income countries (Meghani, 2004). In the following two decades, ‘palliative care’ was used interchangeably with ‘hospice care’ and understood as care for patients dying from cancer. In line with this origin, in a recent survey, nearly half of psychiatrists in Switzerland felt that the term ‘palliative’ directly relates to end-of-life care (Trachsel et al., 2019).
However, after new health care technologies extended illness trajectories (such as dialysis for kidney failure), the concept of palliative care broadened considerably during the 1990s (Guo et al., 2012; Meghani, 2004). Palliative care was now seen as a philosophy of care and set of strategies that not only guide care for patients at the end of life, but all patients with life-threatening illnesses:
Palliative care is an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual. (Sepúlveda et al., 2002: 94)
In a recent Delphi process, the target population of palliative care was defined even broader as ‘individuals across all ages with serious health related suffering because of severe illness and especially of those near the end of life’ (Radbruch et al., 2020: 8). Severe illness, in turn, is ‘a condition that carries a high risk of mortality, negatively impacts quality of life and daily function, and/or is burdensome in symptoms, treatments, or caregiver stress’ (Kelley, 2014: 985). Thus, while the diagnosis of a life-threatening illness remains a sufficient eligibility criterion for palliative care, it is no longer necessary; palliative care includes, but goes beyond end-of-life care. Similarly, palliative care is no longer seen as incompatible with curative approaches and early integration of palliative care with disease-modifying care is now the gold standard, e.g., in oncology (Ferrell et al., 2017; Jordan et al., 2018). Indeed, in recent surveys, half of the respondents of psychiatrists in India found the term ‘palliative’ to not directly relate to end-of-life care, as did a third of the respondents in Switzerland (Stoll et al., 2022; Trachsel et al., 2019).
Importantly, in none of these definitions is eligibility for palliative care limited to specific diagnoses, and palliative care ‘should be delivered based on need rather than prognosis’ (Radbruch et al., 2020). Accordingly, some persons suffering from SPMI may be eligible for palliative care (Berk et al., 2012; Lindblad et al., 2019; Trachsel et al., 2016). About three in four psychiatrists in Switzerland and India indicated that palliative approaches are important in caring for some persons with mental disorders, even in the absence of life-threatening somatic illnesses (Stoll et al., 2022; Trachsel et al., 2019).
Palliative psychiatry in a narrow sense
Like palliative care for patients with advanced dementia 3 (Eisenmann et al., 2020), palliative psychiatry in a narrow sense refers to the provision of end-of-life care for persons dying from a mental illness. An example is hospice care for persons dying from anorexia nervosa (Lopez et al., 2010; O’Neill et al., 1994; Trachsel et al., 2015). In these case reports, further curative treatment such as artificial refeeding was deemed futile and adding to the patients’ suffering. 4 The goal of care was changed to optimizing quality of life, and the patients were referred to hospice care.
Another example comes from the case of a patient with schizophrenia and severe chronic agitated/malignant catatonia who, over several months of hospitalization, repeatedly required intubation and sedation to manage behavioural and mental symptoms. Considering the lack of appreciable clinical benefit from treatment and his irremediable suffering, the patient’s parents (as appointed substitute decision-makers) ultimately decided to forgo further life-sustaining treatment, and the patient died of aspiration pneumonia (Trachsel et al., 2022).
Two adjacent but distinct areas should be distinguished from palliative psychiatry in a narrow sense: palliative care psychiatry and assisted dying for persons with SPMI. Palliative care psychiatry (Fairman et al., 2016) or psychiatry in palliative medicine (Chochinov and Breitbart, 2009) is the care for persons with mental disorders or psychiatric symptoms who are receiving palliative care for a life-threatening somatic illness. Thus, palliative care psychiatry is concerned with persons dying with psychiatric symptoms or mental disorders, while palliative psychiatry in a narrow sense is concerned with persons dying from mental disorders.
Regarding assisted dying, some have argued that SPMI can cause irremediable, unbearable suffering and that in these cases, a wish to die may be rational, competent and voluntary (Dembo et al., 2018). However, a defining characteristic of palliative care is that it ‘intends neither to hasten nor to postpone death’ and ‘affirms life’ (Radbruch et al., 2020: 8). As the practice of palliative psychiatry develops, assisted dying may come to be seen as at the end of the spectrum of approaches for the relief of suffering in persons with SPMI, or considered entirely separate. It is beyond the scope of this article to discuss its potential merits and pitfalls further.
Palliative psychiatry in a broad sense
While palliative psychiatry in a narrow sense is limited to patients likely to die of their SPMI in the near future, palliative psychiatry in a broad sense refers to all approaches aiming at improving quality of life by means other than reduction of SPMI symptoms, namely harm reduction and relief of suffering. Palliative psychiatry in a broad sense is exemplified by supervised injectable heroin (SIH) treatment for refractory opioid use disorder. SIH treatment is intended for patients ‘who have not responded to standard treatments such as oral methadone maintenance treatment (MMT) or residential rehabilitation’ (Strang et al., 2015: 6), i.e., when curative treatments (aiming at abstinence or at least reduction of consumption) have not been successful. In SIH treatment, the goal of care is no longer reduction of heroin use per se, but reduction of use of street heroin with its associated harm, 5 which improves quality of life (Palis et al., 2017; Strang et al., 2015). Of note, emerging evidence suggests that SIH treatment reduces the ultimate harm, mortality (Levengood et al., 2021; Strang et al., 2015). Together with the high intensity and high costs of SIH treatment, this illustrates that palliative psychiatry is far from ‘giving up’ hope and/or patients. It is about letting go of curative goals of care – if and when they are in all likelihood unattainable and their pursuit burdensome – and redirecting hope towards palliative goals of care, such as harm reduction and relief of suffering.
Another example for palliative psychiatry in a broad sense is the Community Outreach Partnership Program (COPP) for anorexia nervosa (Williams et al., 2010). In cases where treatments focusing on symptom reduction have failed, the authors propose ‘a shift away from focusing on the eating disorder and towards increasing quality of life, reducing distress and increasing hope for the future’ (Williams et al., 2010: 91; italics in the original). Interventions are tailored to the individual and can, e.g., consist of accompanying a fearful person to an art class she finds pleasurable. Of note, while describing their approach as an alternative to treatments aiming at symptom reduction, the authors themselves declare that ‘COPP does not provide palliative care’ (Williams et al., 2010: 93). However, the programme is based on ‘setting the eating disorder aside’ (Williams et al., 2010: 90), i.e., letting go of curative goals of care (reduction of eating disorder symptoms) that are in all likelihood unattainable. Instead, relief of suffering and improvement of quality of life are the main goals of care in COPP. Thus, COPP is a palliative psychiatry approach in the broad sense. We assume that the authors wished to express that their programme does not provide end-of-life care when they distanced themselves from palliative care. This would imply that they referred to what we termed ‘palliative psychiatry in a narrow sense’, exemplifying the need for concept clarification regarding non-curative approaches in psychiatry.
Similar, but different
As with palliative psychiatry in a narrow sense, we now offer some differentiations and clarifications for palliative psychiatry in a broad sense. First, approaches like SIH and COPP are often labelled harm reduction approaches (Bianchi et al., 2021; Kleinig, 2008). In COPP, harm may be reduced by not bingeing on raw meat or food from the rubbish bin (without necessarily reducing the frequency or duration of bingeing, i.e., without symptom reduction). The palliative elements in both SIH and COPP clearly include harm reduction. But ‘harm reduction by itself is insufficient to reduce suffering in [SPMI] patients and to attend to their associated physical, mental, social, and existential needs’ (Westermair et al., 2021: 60). Therefore, palliative psychiatry includes but goes beyond harm reduction, e.g., by ‘offering unconditional therapeutic support even to patients who choose to not engage in harm reduction’ (Westermair et al., 2021: 61).
Second, palliative psychiatry shares some characteristics with rehabilitative psychiatry and (personal) recovery, such as shifting the focus away from the disorder and setting individual, realistic goals that are valued by the patient. A mental health professional with experience in palliative (or rehabilitative) psychiatry is likely to be a good fit for a SPMI patient interested in recovery. However, in contrast to palliative psychiatry, the overarching goal in rehabilitative psychiatry is to help SPMI patients ‘develop the emotional, social and intellectual skills needed to live, learn and work in the community with the least amount of professional support’ (Roessler, 2006: 151). Thus, where palliative psychiatry focuses primarily on suffering and quality of life, rehabilitative psychiatry focuses on psychosocial functioning (see Figure 1). Regarding (personal) recovery, the main difference to palliative psychiatry is one of perspective and initiative: while palliative psychiatry is an approach that mental health professionals can propose to SPMI patients, recovery is a journey that persons undertake in order to live a personally fulfilling life in the face of SPMI. Mental health professionals can (and, in our opinion, should) support persons with SPMI in their pursuit of personal recovery, but cannot initiate it or take the lead. Also, both concepts can stand alone: persons with SPMI do not require a mental health professional to undertake their recovery journey, and mental health professionals can take a palliative approach to caring for SPMI patients that are currently not interested in recovery. And while some final recovery stages map onto palliative goals of care (such as ‘improving quality of life’), others map onto rehabilitative goals (such as ‘successful occupational performance’) or do not map onto any of the traditional goals of medicine, namely prevention, curation, rehabilitation and palliation (such as ‘personal growth’; Leamy et al., 2011).
Third, palliative psychiatry is ‘defined by its goals and not by the use of specific treatments’ (Strand et al., 2020: 6). Most interventions used in palliative psychiatry are already established in psychiatry and frequently used with the goal of symptom reduction, i.e., with curative intent. For example, building a therapeutic relationship with a person with anorexia nervosa can both be a means to working on core symptoms such as restrictive eating (i.e. an intervention with curative intent) and a means to alleviating existential loneliness (Yager, 2020; that is, an intervention with palliative intent). Thus, palliative psychiatry differs from curative psychiatry mainly in when and for what purpose interventions are applied. In fact, palliative psychiatry may be most clearly distinguished from curative psychiatry by acts of omission (such as not coercing artificial refeeding, not terminating psychotherapy in a patient whose SPMI does not improve) than by acts of commission.
Fourth, and most importantly, palliative psychiatry in a broad sense can – and often should – be integrated with curative and rehabilitative approaches to provide optimal care, as is the gold standard in palliative care for somatic illnesses (Radbruch et al., 2020). For example, in the COPP programme for eating disorders detailed above, interventions aiming at symptom reduction (such as keeping food records and meal planning) and psychosocial functioning (general life skills such as budgeting and social skills such as conflict resolution) are used in parallel with treatment focusing directly on distress and quality of life (Williams et al., 2010). Another example might be prescribing benzodiazepines to relieve anxiety induced by therapy-refractory delusions (palliative intent) while switching to an antipsychotic combination treatment to try and reduce the delusions (curative intent) and initiating supported employment to train cognitive and self-management abilities (rehabilitative intent). Importantly, such a combination of palliative, rehabilitative and curative aspects of care is never fixed but should be constantly adapted to current psychopathology, psychosocial functioning, risk and severity of harm, and patients’ wishes. Shifts from more palliative approaches back to more curative approaches are likely to be more common in SPMI than in somatic illnesses due to differences in disorder trajectories and life expectancy. In addition, as interventions in mental health care tend to be pleiotropic, even if interventions are ‘only’ intended to relief suffering, they might still result in symptom reduction and/or improved psychosocial functioning. For example, a referral to a palliative care unit can, unexpectedly, help a person with anorexia nervosa realize that she does prefer eating over dying after all (Mishra, 2012).
Conclusion
Palliative psychiatry is an emerging subdiscipline of psychiatry, born out of compassion for SPMI patients and humility considering the limitedness of curative psychiatry in alleviating their suffering. In a broad sense, palliative psychiatry refers to any approach aiming at reducing harm and/or relieving suffering directly rather than via reduction of SPMI symptoms (curative psychiatry) or improvement of psychosocial functioning (rehabilitative psychiatry). In a narrow sense, palliative psychiatry refers to such approaches in patients likely to die of their SPMI in the near future.
As with somatic illnesses, palliative approaches are neither first-line nor second-line treatments. If curative treatment options have a reasonable benefit–harm ratio, they should be preferred in general. However, in some cases of SPMI, further treatment attempts aiming at symptom reduction will – in all likelihood – be ineffective and burdensome. In these cases, palliative psychiatry may be the best possible form of management, distinct from but integratable with other approaches such as curative and rehabilitative psychiatry and (personal) recovery.
The implementation of palliative psychiatry is met with several challenges, among them the stigmatization of palliative care in general, difficulties regarding decision-making capacity and prognostication in SPMI, and lack of established staging models for SPMI. We firmly believe that these challenges are worth overcoming so that mental health care can be improved and completed, just as cancer care was improved and completed by the emergence of palliative care.
Footnotes
Acknowledgements
We thank Ulrich Schweiger, MD (University of Lubeck, Germany) and Sascha Weber, MD (University of Aachen, Germany) for their feedback provided on an earlier draft of this manuscript. No compensation was provided.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.