
Abstract
Objective:
Suicide rates in rural Australia are higher than in urban areas. No existing research has explored the long-term patterns and predictors of change in suicidal ideation within rural areas. This report uses longitudinal data and multiple time points to determine predictors of the trajectory of suicidal ideation in rural Australia.
Method:
Participants in the Australian Rural Mental Health Study (ARMHS) completed self-report surveys at baseline, 12 and 36 months, reporting their psychological and social well-being, and suicidal ideation. Generalised linear mixed models explored these factors as correlates and predictors of suicidal ideation across 3 years using multiple data points.
Results:
A total of 2135 participants completed at least one wave of ARMHS, and hence were included in the current analysis. Overall, 8.1% reported suicidal ideation during at least one study wave, 76% of whom reported suicidal ideation intermittently rather than consistently across waves. Across the three time points, suicidal ideation was significantly associated with higher psychological distress (OR 1.30, 95% CI 1.23 to 1.37), neuroticism (OR 1.15, 95% CI 1.04 to 1.27), and availability of support (OR 0.80, 95% CI 0.69 to 0.92), with a non-significant association with unemployment (OR 1.73, 95% CI 0.93 to 3.24) even after controlling for the effects of perceived financial hardship. Future suicidal ideation was significantly predicted by distress (OR 1.16, 95% CI 1.09 to 1.23) and neuroticism (OR 1.17, 95% CI 1.03 to 1.32), with a non-significant association with unemployment (OR 2.11, 95% CI 0.41 to 2.27). Predictive effects for marital status, social networks, sense of community and availability of support did not remain significant in the full multivariate analysis.
Conclusions:
Fluctuations in suicidal ideation are common, and may be associated with changes in psychological and social well-being. Public health strategies, focusing on encouraging help-seeking among those with higher psychological distress, lower social support, and unstable or absent employment opportunities, may be a useful long-term initiative to reduce the prevalence of suicidal ideation in the general rural community.
Introduction
Suicide rates in rural Australia are higher than those in urban areas (Australian Bureau of Statistics, 2011), and may be associated with a unique range of risk factors (Taylor et al., 2005). Previous longitudinal research in an urban Australian sample has shown that fluctuations in suicidal ideation are common, with new occurrences accounting for approximately half of the reported suicidal ideation rate at a given point in time (Fairweather-Schmidt et al., 2010). This has implications for suicidality research, implying that suicidal thoughts in many cases may be transient, and may not be accurately identified if measured in cross-sectional research. To our knowledge there is no existing research exploring long-term patterns of change in suicidal ideation within rural Australia.
We have previously reported that after controlling for a range of demographic, social and psychological factors, baseline suicidal ideation is the strongest predictive factor of suicidal ideation at 12-month follow-up (Handley et al., 2012). However, a number of other important risk factors were also observed, namely high psychological distress, low availability of social support and current unemployment. We also found that psychological distress and availability of social support predict the development, but not remission, of suicidal ideation over a 12-month period. The current analysis extends these findings, using additional data from the third wave of the Australian Rural Mental Health Study (ARMHS) to explore the patterns and course of suicidal ideation in a rural sample over multiple time points, including the persistence and development of suicidal thoughts, and longitudinal predictors of suicidal ideation. By using multiple follow-ups, the power to detect significant effects is greatly enhanced, increasing the potential to observe effects that are not apparent in cross-sectional studies or those with a single follow-up. There is limited existing research utilising this approach to explore suicidal ideation, and, to our knowledge, none in an Australian context.
The current report explores patterns of suicidal ideation over 36 months, using longitudinal data and multiple time points to determine predictors of the trajectory of suicidal ideation. Utilising the same variables as our previous analysis (Handley et al., 2012), we aim to explore the long-term association between suicidal ideation and a range of social and psychological factors, incorporating multiple phases of data to increase statistical power to detect effects. Based on our previous findings, we expected that psychological distress, availability of social support, and employment status would be independent predictors of the course of suicidal ideation. We also expected that incorporating three phases of data would identify more predictors of suicidal ideation than when using only two time points.
Methods
Participants
The present analysis uses data from the ARMHS, a longitudinal study of mental health and well-being in rural and remote NSW, Australia. Following the baseline data collection phase (detailed in Kelly et al., 2011), the sample completed follow-up surveys at 12 and 36 months. Ethical approval was obtained from the Human Research Ethics Committees of the Universities of Newcastle and Sydney, and the relevant health service research ethics committees.
Measures
The measures in the current paper are only briefly described here as they mirror those used in our original analysis (Handley et al., 2012), with the additional requirement that they were measured at each of the three study phases. Suicidal ideation was measured using item 9 of the Patient Health Questionnaire-9 (PHQ-9) (Kroenke et al., 2001). This question asks respondents to rate the frequency of ‘thoughts that you would be better off dead, or of hurting yourself in some way’ during the past 2 weeks, on a 0 to 3 scale from ‘not at all’ to ‘nearly every day’. For the purposes of the present analysis, responses were dichotomised into a ‘yes/no’ variable. Consequently, the primary focus was on associations with the presence versus absence of suicidal ideation within the 2-week timeframes, rather than the frequency of these thoughts.
Sociodemographic information including age, gender, marital status, employment status and perceived financial hardship were assessed by single-item questions. The geographical classification of participants was determined using the Accessibility/Remoteness Index of Australia Plus (ARIA+). This was used to divide them into Australian Standard Geographical Classification (ASGC) categories of inner regional, outer regional, remote or very remote.
Current psychological distress was measured using the Kessler-10 (K10) scale (Kessler et al., 2002) and recent alcohol use was measured using the Alcohol Use Disorders Identification Test (AUDIT) (Saunders et al, 1993). Higher scores on these scales are indicative of higher distress and higher alcohol use, respectively.
The Berkman Syme Social Network Index (Berkman and Syme, 1979) assessed involvement in organised groups within the community (such as social/recreational groups, church groups, or charity groups), ranking overall involvement in one of four categories from ‘low’ to ‘high’. Perceived availability of interpersonal social support was reported on the Interview Schedule for Social Interaction – Availability of Attachment Scale (ISSI) (Henderson et al., 1980); higher scores indicate a higher perceived availability of interpersonal social support. Sense of belonging in the community (including feelings of attachment and responsibility towards the land and community) was determined by the Sense of Community Index (Chipuer and Pretty, 1999). Concerns related to rural infrastructure and services were measured by a unique set of questions developed for the ARMHS project (see Kelly et al., 2010). Predispositional variables included neuroticism items from the 12-item Eysenck Scale – brief form (Eysenck et al. (1985)), with higher scores indicating higher neuroticism. As neuroticism is presumed to be a trait variable, it was measured at baseline only.
Data analysis
Data were analysed using Stata (Release 11; College Station, TX: StataCorp LP). Generalised linear mixed models were used to explore two concepts: factors that are associated with suicidal ideation over a long-term timeframe, and factors that are predictive of suicidal ideation over a long-term timeframe.
The analysis strategy involved several sequential components. Firstly, individual generalised linear mixed models were conducted to explore the relationship between each variable and suicidal ideation over time, controlling for the effects of study phase. Participants were included in this analysis if they had completed at least one ARMHS survey (baseline, 12 or 36 months). Secondly, variables that were statistically significant in the analysis controlling for study phase only were then included in a multiple linear mixed model controlling for all significant predictor variables. Thirdly, this analysis was repeated after time-lagging the predictor variables. That is, baseline independent variables were used to predict 12-month suicidal ideation, while 12-month independent variables were used to predict 36-month suicidal ideation. Participants were required to have completed baseline and at least one ARMHS follow-up survey (12 or 36 months) to be included in the time-lagged analysis. These models also controlled for the effects of study phase and baseline suicidal ideation. Fourthly, variables that were statistically significant in the analysis controlling for study phase and baseline suicidal ideation only were then included in a full multivariate model controlling for all significant predictor variables. Gender interactions were also explored in all multivariate models.
Results
Of the 2639 participants recruited at baseline, 1794 (68.0%) completed at least one follow-up survey; of these, 1448 completed all demographic, psychological and social measures included in the present analysis. The flow of participants through the three waves of the survey is depicted in Figure 1. At baseline, 39.9% (n = 639) of our sample were male, with a mean age of 56.9 years (SD = 13.5). Seventy-six per cent (n = 1214) were married or in a de facto relationship.
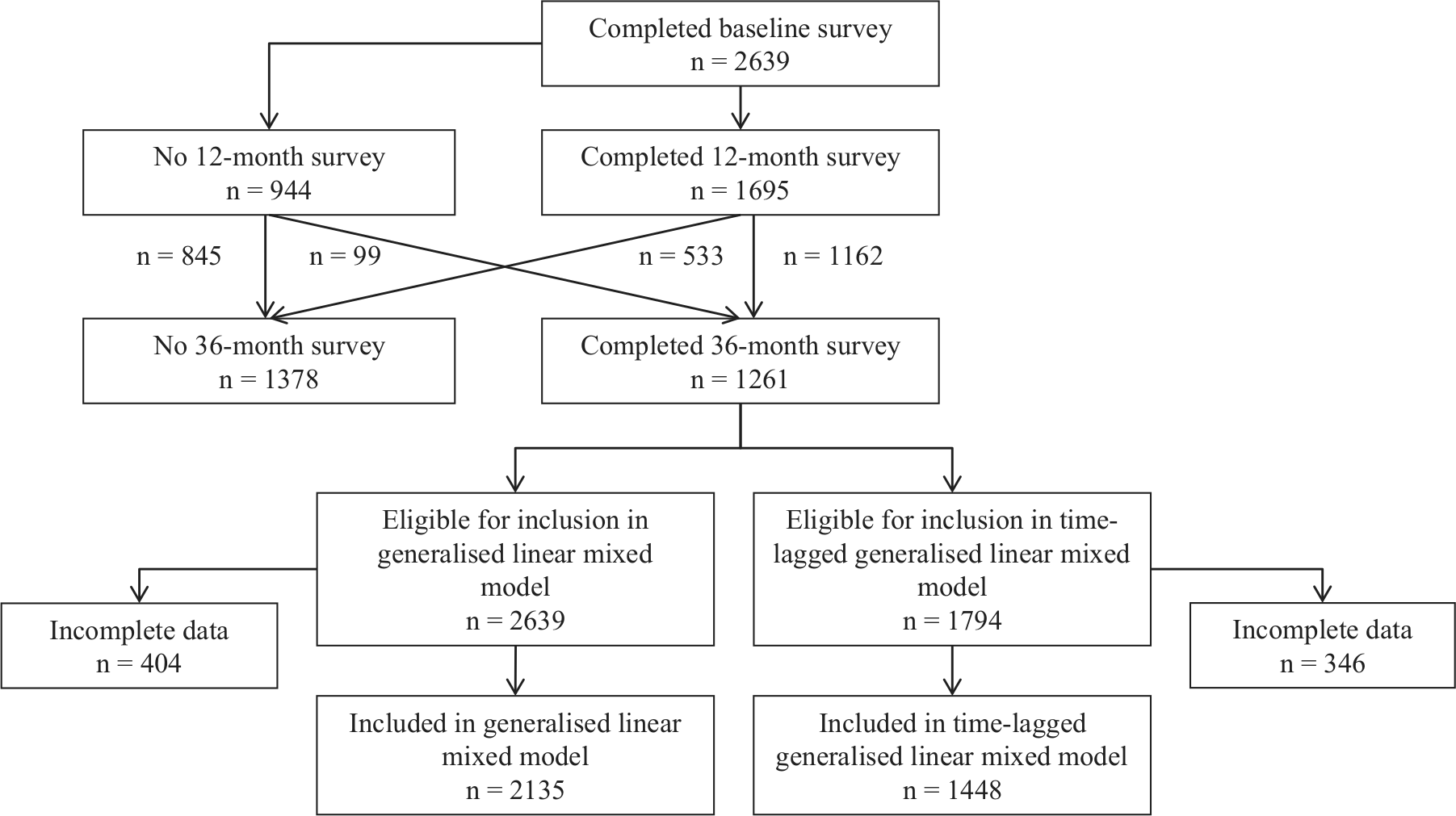
Flow of participants through the three waves of the ARMHS survey.
Compared to people who were included in our time-lagged analysis, those who did not complete a follow-up survey were younger [52.2 (SD = 13.9) vs 56.9 (SD = 13.5) years, F(1, 2638) = 65.8, p < 0.001]. Participants who completed follow-up had lower psychological distress than those who were not retained [K10: 14.5 (SD = 5.1) vs 15.7 (SD = 6.4), F(1, 2607) = 26.9, p < 0.001]. Employed participants were also more likely to complete follow-up than unemployed people (62.5% vs 52.9%, χ2(1) = 12.3, p < 0.001). Participants who were retained for at least one follow-up were less likely to report baseline suicidal ideation than those who were not (5.1% vs 8.6%, χ2(1) = 8.7, p = 0.003).
Patterns of suicidal ideation
Across the 3-year period, 8.1% (n = 117) of the 1448 participants who completed at least one follow-up indicated experiencing suicidal ideation in at least one survey. Twenty-eight participants (1.9%) reported consistent suicidal ideation in each survey, while 40 (2.8%) reported suicidal ideation at baseline which had resolved by 36 months. Thirty-three participants (2.3%) who reported no suicidal ideation at baseline had developed it over the 36 months, while 16 participants (1.1%) fluctuated between suicidal ideation and an absence of suicidal ideation at each time point.
Associations with suicidal ideation
Table 1 depicts the associations between suicidal ideation and predictor variables across the three phases of data collection. Over the 3 years of the ARMHS study, females were significantly less likely than males to experience thoughts of suicide, while people who were currently unmarried were more likely than married participants to report suicidal ideation. Unemployed participants had higher odds of ideation than employed people, while people who were financially ‘just getting along/poor’ had significantly increased odds compared to those who were ‘prosperous/very comfortable’. Higher psychological distress, alcohol use, neuroticism, and infrastructure/services distress were all associated with increased odds of suicidal ideation over the 3 years, while higher engagement with social networks, sense of community and availability of support were each associated with decreased odds of ideation.
Associations between predictor variables and suicidal ideation across the three waves of the ARMHS study.
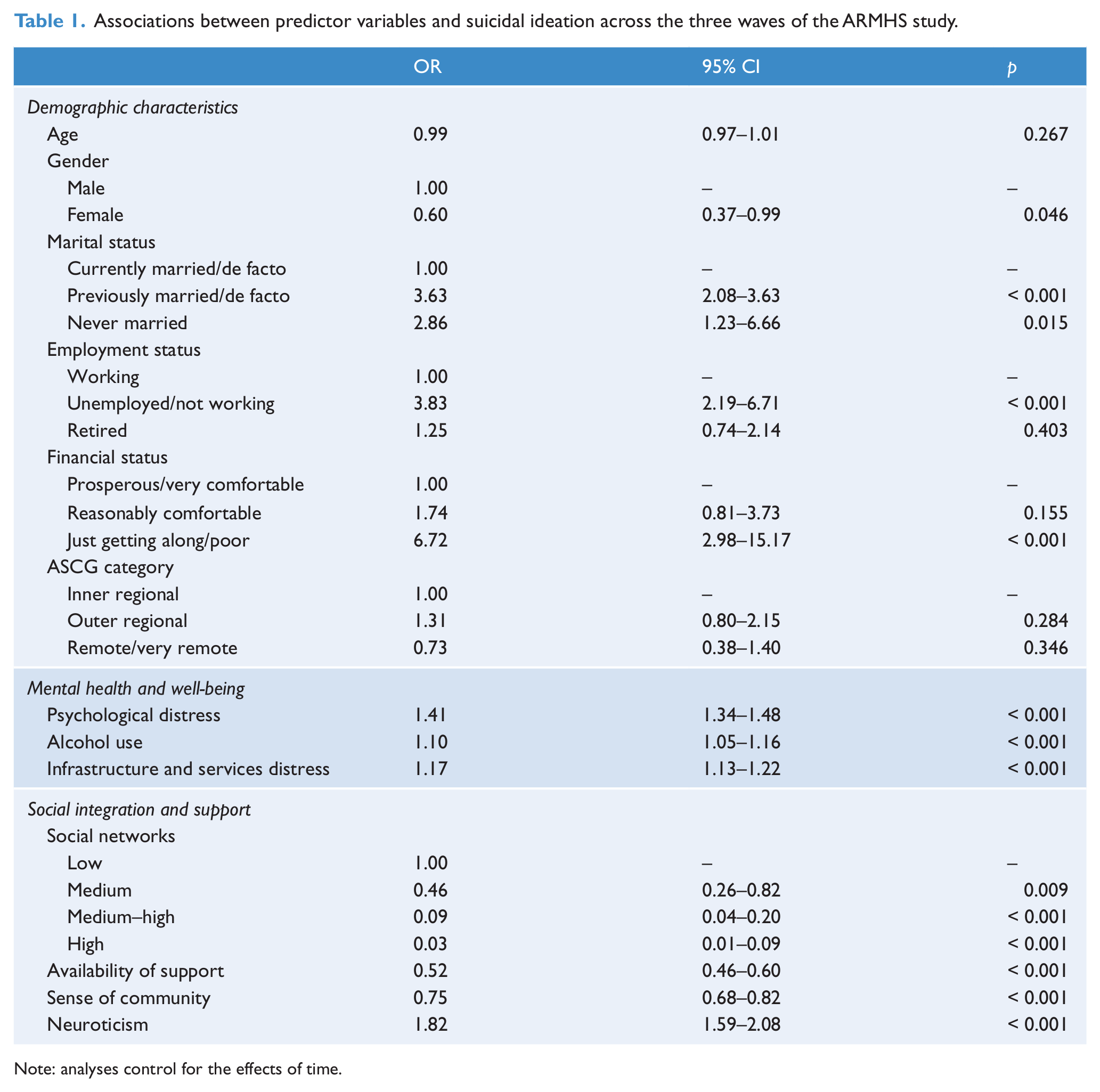
Note: analyses control for the effects of time.
In the multivariate analysis, higher psychological distress (OR 1.30, 95% CI 1.23 to 1.37, p < 0.001) and higher neuroticism (OR 1.15, 95% CI 1.04 to 1.27, p = 0.005) were associated with higher odds of suicidal ideation, while higher availability of social support was associated with significantly decreased odds of ideation (OR 0.80, 95% CI 0.69 to 0.92, p = 0.002). A non-significant trend was observed for participants who were unemployed compared with those who were employed (OR 1.73, 95% CI 0.93 to 3.24, p = 0.085). A significant interaction between psychological distress and availability of support was also observed (OR 1.02, 95% CI 1.00 to 1.03, p = 0.034); this indicates that the effects of social support were stronger among participants with higher psychological distress. There were no significant interactions with gender.
Predictors of suicidal ideation
Table 2 shows the results of the time-lagged analysis, controlling only for study phase and baseline suicidal ideation. Participants who had never been married had approximately four times the odds of future suicidal ideation compared to currently married participants, with a similar effect observed for unemployed participants compared with those currently working. Higher psychological distress and higher neuroticism were associated with significantly increased odds of future suicidal ideation, while higher sense of community and higher availability of support were significant protective factors. A small effect was observed for social networks, with participants with medium–high social networks having significantly lower odds of future suicidal ideation than those with low social networks.
Time-lagged analysis to predict future suicidal ideation during the 12- and 36-month waves of the ARMHS study.
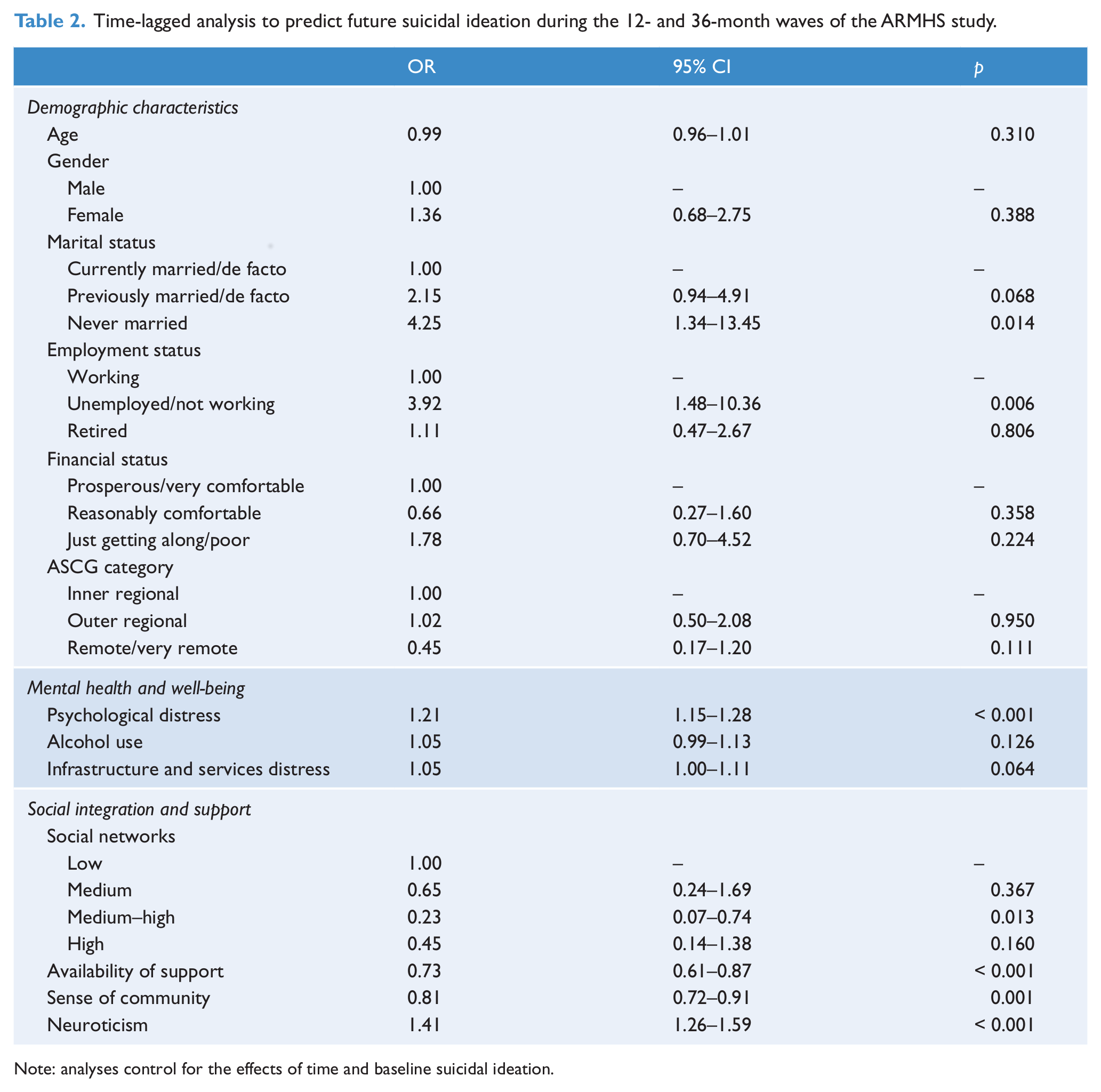
Note: analyses control for the effects of time and baseline suicidal ideation.
When all significant factors were controlled for, each one point increase in psychological distress was associated with increased odds of future suicidal ideation (OR 1.16, 95% CI 1.09 to 1.23, p < 0.001). Each one point increase in neuroticism was also associated with a significant increase in the likelihood of future suicidal ideation (OR 1.17, 95% CI 1.03 to 1.32, p = 0.013). A non-significant trend was observed for unemployed compared with currently employed participants (OR 2.11, 95% CI 0.41 to 2.27, p = 0.069). There were no significant gender interactions.
Discussion
Overall, the generalised linear mixed models using three data time points revealed similar results to our previous 12-month analysis (Handley et al., 2012), in that psychological distress, availability of social support, and employment status were all found to have significant associations with suicidal ideation across a long-term follow-up. We also identified several additional factors, including neuroticism and sense of community, which did not reach significance in our previous study.
Approximately three-quarters of participants who reported suicidal ideation during the study did not do so consistently over the time points of assessment, indicating a high degree of fluctuation in this symptom. This has important implications clinically in that it indicates that treating suicidal ideation as it arises, and monitoring suicidal ideation even among people who have not reported such thoughts in the past, is important, as this state may be transient and change frequently. Our findings in regards to rates of persistence, remission and development of suicidal ideation are similar to those reported in previous Australian-based longitudinal research in urban areas (Fairweather-Schmidt et al. 2010), indicating that they may be comparable across geographical areas. From a research perspective, these findings emphasise the strength and importance of longitudinal studies when exploring changeable states such as suicidality.
The high degree of variability in suicidal ideation observed across the three phases of this analysis has implications from a public policy perspective. The variations observed raise concerns about when interventions are necessary, and most likely to be successful. The risk factors for suicidal ideation identified in the present analysis offer a potential preventative focus in that they provide more general targets for public health campaigns. Focusing attention towards factors such as psychological distress and low social support, which are associated with multiple negative outcomes in addition to suicidality, is likely to have positive effects at a community level, and may be a more effective approach in terms of resource allocation. For example, psychological distress is a risk factor not only for suicidality, but also a clinical indicator of common psychiatric conditions such as affective, anxiety and substance use disorders (Andrews and Slade, 2001). While these diagnoses are also associated with suicidal thoughts and behaviours (Cavanagh et al., 2003; Sareen et al., 2005), they pose a considerable concern in their own right. Enhancing the focus of population-level strategies towards psychological distress may therefore be a highly resource-efficient means of reducing a range of negative outcomes in the Australian community. This suggestion aligns well with the strategy recently proposed by the Australian Government to increase population-level approaches to suicide prevention, while also acknowledging the multidimensional nature of suicidality and the need for prevention campaigns to target multiple outcomes (Commonwealth of Australia, 2010). The present analysis usefully identifies important factors for such programmes to consider.
Individuals with higher levels of suicidal ideation reported higher psychological distress across the three surveys, confirming previous cross-sectional research in the wider Australian community (Chamberlain et al., 2009). Psychological distress was also a significant predictor of future suicidal ideation, aligning with our previous finding of a temporal relationship between these constructs, indicating that the K10 may usefully identify the likelihood of suicidal ideation as far as 3 years into the future.
The generalised linear mixed models showed that baseline neuroticism was significantly positively associated with suicidal ideation across our multiple time points, confirming previous Australian findings from a primarily urban sample (Batterham and Christensen, 2012). We also observed a significant effect for neuroticism in the time-lagged analysis, supporting the use of this factor as an indicator of future, as well as current, suicidal ideation. Neuroticism was not significant in our previous analysis, demonstrating the advantages of utilising multiple follow-up points to enhance statistical power to detect effects. The implications of this finding are more likely to apply in clinical settings. The presence of higher neuroticism may indicate higher risk for suicidal ideation over the long term (perhaps aligned to models of stress sensitivity), and indicative of the potential benefits of psychotherapeutic interventions targeting such predisposing factors. Evidence suggests that individual trait characteristics including neuroticism and similar constructs (e.g. stress sensitivity) may be established during adolescence and remain relatively stable across the lifespan (Soldz and Vaillant, 1999), with evidence of a genetic contribution to susceptibility to these traits (Caspi et al., 2010); hence the importance of early therapeutic interventions targeting such characteristics to modify future risk of psychiatric morbidity, including suicidal ideation. The National Mental Health Plan also emphasises the development of resilience and coping skills at a population level, as an important component of maintaining the mental health of the nation (Department of Health and Aging, 2009).
The associations observed between aggregate suicidal ideation and aggregate availability of support also reflected our previous findings over a longer time period, suggesting that lower availability of support (as measured by the ISSI) was associated with higher suicidal ideation across 3 years. However, this effect was not significant in the full multivariate time-lagged model, contrasting with our previously reported findings. This may reflect a weakening of the effect over time, in that availability of support did not present a strong enough long-term predictive effect to remain significantly independent from variables such as neuroticism and psychological distress over 3 years. As this was a subjective measure of social support, it is possible that our findings relate to personality characteristics (such as neuroticism) which may cause some individuals to perceive lower levels of available support (Henderson, 1981). Additionally, we observed a significant interaction between availability of support and psychological distress, emphasising the important moderating role that social support may play. Availability of support may therefore be most usefully conceptualised as a concurrent protective factor, particularly among people experiencing high levels of distress, and enhancing opportunities for social interaction in rural areas may be beneficial. This finding aligns with the strategies proposed by the National Suicide Prevention Program, a key aim of which is to enhance national and community-level resources for rural and remote residents as a means of suicide prevention (Commonwealth of Australia), and may provide direction for such resources.
Unemployment was significantly associated with both current and future suicidal ideation in the initial analyses, however this became a non-significant trend when all significant factors were controlled for. Across the three time points, participants who were employed either consistently or inconsistently reported lower suicidal ideation than those with persistent unemployment, suggesting that employment is an important protective factor against suicidal ideation. Importantly, while employment was a significant factor in our time-lagged analyses, financial status was not, suggesting that this effect may be associated with the social aspects of employment, or the associated sense of purpose. This is an important issue in rural areas, with higher geographical isolation and environmental adversities associated with lower employment opportunities and job stability (Cheers, 1990; Fraser et al., 2005). Likewise, decreasing rates of migration into rural areas of Australia have been associated with declining opportunities for both employment and socialisation, particularly for young people (Davies, 2008). It is likely that the non-significant effects for employment status observed in the multivariate analyses are therefore partly attributable to the influence of social support; as employment may be a key source of social support and networking among rural residents, the declining rural employment opportunities indicate a potential for the prevalence of suicidal ideation to increase among rural residents in the coming years. The lack of an independent impact of unemployment in the multivariate analyses may also be due to the effects of psychological distress, which has been found to have a significantly higher effect among the rural unemployed that those with consistent job opportunities (Fragar et al., 2010). The current National Mental Health Plan specifies the necessity to improve employment opportunities and outcomes for people experiencing mental health problems in general (Department of Health and Ageing, 2009), and the present findings emphasise the importance of this approach in rural and remote areas. The specific challenges related to increasing rural employment in the context of declining vocational opportunities warrant particular consideration by policy makers.
Although suicide rates are consistently higher in males than females (Australian Bureau of Statistics, 2013), particularly in rural areas (Kõlves et al., 2012), the present study found little difference between genders. Males were more likely to report suicidal ideation in the univariate analysis, but this effect did not remain significant when psychological and social factors were considered. Likewise, there were no significant gender interactions, indicating that the magnitude of effects did not differ between males and females.
This analysis has several limitations, including our use of the PHQ-9 to detect suicidal ideation. As this measure explores suicidal ideation during only a 2-week period, it provides a relatively crude measure of the persistence of suicidal ideation over time. This also limits the comparability of the present findings with other relevant Australian (largely urban-based) research (Fairweather-Schmidt et al., 2010; De Leo et al., 2005), which has used a longer timeframe for the outcome measure. Several important predictor variables, including unemployment, psychological distress and baseline suicidal ideation, were associated with a higher attrition rate from ARMHS, suggesting that we may have underestimated the magnitude of the observed effects. Despite this, our use of generalised linear mixed models ensured that data availability was maximised, limiting the effects that participant attrition had on statistical power. The use of this powerful statistical technique may, however, enable highly predictive variables such as psychological distress to override the smaller effects of variables such as availability of support and unemployment, which were not significant predictors of future suicidal ideation in time-lagged multivariate analysis despite predicting 12-month suicidal ideation in our previous paper. This emphasises the importance of cautious data analysis and interpretation when using models with high statistical power. Finally, we measured only thoughts of suicide rather than suicidal behaviours, and therefore cannot determine whether the risk factors we identified may also apply to more severe suicidality. Although suicidal ideation is among the most significant risk factors for a suicide attempt or fatality (Brown et al., 2000; Nock et al., 2008), the relatively high proportion of the sample (8%) that reported suicidal ideation over the study period suggests that this indicator and the associated risk and protective factors may lack utility for more severe outcomes. Future research is necessary to further explore this.
Overall, our findings support previous results suggesting that lower psychological distress, higher perceived availability of social support, and to a lesser extent current employment, may be effective protective factors against suicidal ideation. As this was a community-based study, the present findings support the notion that public health strategies, focusing on encouraging help-seeking among those with higher psychological distress, lower social support, and unstable or absent employment opportunities, may be a useful long-term initiative to reduce the prevalence of suicidal ideation in the general rural community.
Footnotes
Acknowledgements
We wish to recognise the contribution of the ARMHS chief investigators: Professor David Lyle, Assistant Professor David Perkins, Assistant Professor Lyn Fragar, Professor John Beard, Professor Vaughan Carr, Professor Jeffrey Fuller, Assistant Professor Helen Stain, Professor Prasuna Reddy and Senior Project Co-ordinator Dr Clare Coleman. We wish to acknowledge the support of Directors of Mental Health Services in the relevant Local Health Districts during the course of this phase of the study: Drs Russell Roberts, Richard Buss and Dinesh Arya and particularly acknowledge the research site coordinators in each site: Jan Sidford, John Ogle (Broken Hill), Trim Munro, Amy Strachan (Moree), Louise Holdsworth, Kath O’Driscoll (Lismore), Cheryl Bennett, Jannelle Bowler (Orange), along with Fleur Hourihan, Dr Gina Sartore and Denika Novello. Tonelle Handley is supported by a PhD scholarship from Australian Rotary Health/Rotary Club of Parramatta City, which is acknowledged with gratitude.
Funding
The study was funded by the National Health and Medical Research Council (Project Grants #401241, #631061), and also supported by a Research Capacity Building Grant to the Australian Rural Health Research Collaboration. Funding and/or grant number: NHMRC Project Grants #401241, #631061.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.