
Abstract
Objective:
Each year, around one million people die by suicide. Despite its recognition as a public health concern, large-scale research on causal determinants of suicide attempt risk is scarce. Here, we leverage results from a recent genome-wide association study (GWAS) of suicide attempt to perform a data-driven screening of traits causally associated with suicide attempt.
Methods:
We performed a hypothesis-generating phenome-wide screening of causal relationships between suicide attempt risk and 1520 traits, which have been systematically aggregated on the Complex-Traits Genomics Virtual Lab platform. We employed the latent causal variable (LCV) method, which uses results from GWAS to assess whether a causal relationship can explain a genetic correlation between two traits. If a trait causally influences another one, the genetic variants that increase risk for the causal trait will also increase the risk for the outcome inducing a genetic correlation. Nonetheless, a genetic correlation can also be observed when traits share common pathways. The LCV method can assess whether the pattern of genetic effects for two genetically correlated traits support a causal association rather than a shared aetiology.
Results:
Our approach identified 62 traits that increased risk for suicide attempt. Risk factors identified can be broadly classified into (1) physical health disorders, including oesophagitis, fibromyalgia, hernia and cancer; (2) mental health-related traits, such as depression, substance use disorders and anxiety; and (3) lifestyle traits including being involved in combat or exposure to a war zone, and specific job categories such as being a truck driver or machine operator.
Conclusions:
Suicide attempt risk is likely explained by a combination of behavioural phenotypes and risk for both physical and psychiatric disorders. Our results also suggest that substance use behaviours and pain-related conditions are associated with an increased suicide attempt risk, elucidating important causal mechanisms that underpin this significant public health problem.
Introduction
Suicide claims more than 700,000 lives yearly. It is considered among the leading causes of preventable deaths for young adults (Geneva: World Health Organization, 2021). Despite substantial research the risk for suicide attempt, it remains a remarkably difficult phenomenon to predict. A recent meta-analysis of 3428 risk factor effect sizes from 365 studies published over the last 50 years concluded that our ability to predict suicide attempts has not improved is currently slightly better than chance (Franklin et al., 2017). Identifying novel independent risk factors for suicide attempt is of vital importance, not only to gain a better understanding of this complex behaviour but also to increase the specificity of suicide risk prediction models, which currently lack clinical predictive utility (Turecki et al., 2019).
Correlates of suicide attempt identified in the literature include psychiatric conditions (e.g. anxiety, depression), substance use disorders, physical health ailments (e.g. chronic pain) and lifestyle behaviours such as job occupations (McClatchey et al., 2017; Milner et al., 2013; Pompili et al., 2010; Turpin et al., 2020). However, findings from these studies have yielded inconsistent results regarding whether these factors cause suicide attempt or are a consequence of suicide or other confounders (Franklin et al., 2017). For instance, while findings from a meta-analysis have linked smoking to a greater risk of suicide attempt (Poorolajal and Darvishi, 2016), other work has shown that smoking is not associated with attempt when adjusting for confounders (Kessler et al., 2007). Discrepant findings across the literature may be due to differences in study methodology, including the assessment of suicide attempts, sample size, cultural differences to the reporting of suicide behaviours and heterogeneity often observed in the implementation of case-control studies. Finally, an alternative explanation to causation is selection, which argues that people that are genetically predisposed to suicide are also predisposed to a specific behaviour. This scenario can be thought of as genetics-based reverse causation. Identifying causal risk factors for a given behaviour, such as suicide attempt, typically requires a controlled interventional study, or at the very least, a longitudinal cohort study, to avoid potential confounders and establish the direction of effects. These approaches are either unethical or unfeasible due to low base rates of suicide attempts, small sample sizes and challenges with conducting longitudinal studies.
Genetics influence suicide attempt and offers insights into its causal mechanisms. The International Suicide Genetics Consortium has recently published the largest genome-wide association study (GWAS) on lifetime suicide attempt, including cases of death by suicide (Mullins et al., 2020). Briefly, this effort identified two genome-wide associated loci in chromosomes six and seven, one of which was associated with suicide attempt over and above depression. Overall, the GWAS results explained ~7% of the variance of suicide attempt on the liability scale.
GWAS results, such as the one discussed above, are an invaluable contribution to the field; the genetic effect sizes identified can be used as unconfounded instrumental variables to pinpoint potentially causal associations between two traits. The most common way of conducting such a study is through Mendelian randomisation (MR) analysis (Zhu, 2020). However, this approach requires the GWAS to have identified several associations with robust statistical evidence and is thus of limited application in traits for which GWAS has not identified several independent loci. A new method, named the latent causal variable (LCV) (O’Connor and Price, 2018) analysis, leverages the GWAS results to estimate whether two traits are causally associated. Notably, the LCV method accounts for and is less biased by horizontal pleiotropy, which refers to the scenario where two traits share genetic factors without any true causal association. Horizontal pleiotropy is known to be a limitation of MR methods potentially biasing them. There are several strengths of the LCV method, including that: it is unconfounded by horizontal pleiotropy, it can account for sample overlap (i.e. GWAS samples do not need to be independent) and uses information aggregated throughout the genome, which increases statistical power and allows phenotypes that would be considered ‘underpowered’ for traditional MR methods to be tested (O’Connor and Price, 2018).
Here, we leverage GWAS summary statistics for suicide attempt, as well as publicly available GWAS summary statistics for 1520 phenotypes including those on mental health, substance use, physical health and lifestyle behaviours to perform a hypothesis-free screening for factors causally associated with suicide attempt. This approach has the ability to pinpoint causal relations without running an impractical (and sometimes impossible) interventional and longitudinal study. Our results represent testable hypotheses that can be prioritised in future research. Knowledge gained from this work has the potential to inform targeted preventions and interventions by teasing apart true casual factors that influence suicide attempt manifestation, as well as potential sequelae associated with suicide attempt.
Methods
Suicide attempt GWAS summary statistics
We employed the most recent GWAS summary statistics available for suicide attempt, obtained through application to the International Suicide Genetics Consortium (ISGC). This GWAS has been previously described in detail elsewhere (Mullins et al., 2020). Briefly, a coordinated standard error–based meta-analysis for lifetime suicide attempts was performed on 29,782 cases and 519,961 controls. Cases were defined using a range of distinct approaches including self-reports, structured clinical interviews, hospital records and medical examiner offices or death registers. Participants who attempted suicide regardless of underlying psychiatric disorders were classified as cases. Controls were defined as participants with a psychiatric disorder screened and negative for lifetime suicide attempt or unscreened participants from population-based cohorts where suicide attempt rates are expected to be low. In addition, the ISGC performed a conditional analysis removing the effects of depression (Mullins et al., 2020). In this study, the main unconditional analysis which best reflects the true nature of suicide attempt was used. Post-meta-analysis quality control consisted of removing variants with a weighted minor allele frequency of <1%, weighted imputation INFO score <0.6 or with a small representation (N < 80% of total effective sample size).
Other GWAS summary statistics
We included GWAS for all traits available in the Complex Traits Genomics Virtual Lab (CTG-VL) catalogue, a database of GWAS summary statistics with a web interface to perform downstream analyses. These GWAS have been curated from international collaborations and consortia as well as from public releases of whole phenome GWAS data (i.e. The Neale Biobank GWAS). The CTG-VL Inclusion criteria consists of a nominally significant Single Nucleotide Polymorphism (SNP)-based heritability based on Linkage Disequilibrium (LD)-score regression. As of this study, 1520 traits are available.
Latent causal variable
Assessing causality typically requires randomised interventional studies. The motivation for this design is that randomisation removes the effect of any confounders and enables to test for the specific effect of an intervention. Running an interventional study is costly, time consuming and sometimes impractical or unethical (e.g. when the exposure is potentially dangerous). In such situations, one can test for the causal effect of an exposure on an outcome if there is an unconfounded instrumental variable that adequately represents the exposure. Results from genome-wide association studies have revolutionised instrumental variable analysis through MR. MR is a method whereby genetic variants associated with an exposure are used to test for causality with an outcome. Since genetic variants are randomly segregated at birth, one can mimic a randomised trial by testing whether individuals with variants increasing risk for the exposure also show increased risk for an outcome (Gagliano Taliun and Evans, 2021). Recent developments have extended this framework to adjust for potential sources of bias such as horizontal pleiotropy and sample overlap.
If two traits are causally related, the genetic variants that increase the risk for the exposure should also proportionally increase the risk for the outcome. Note that this proportionality factor may be negative so negative (protective) associations are also identifiable. This induces a correlation of the effect sizes identified through GWAS for these traits, which are then considered to be genetically correlated. Given that two traits may have common genetic causes (i.e. horizontal pleiotropy), the existence of a genetic correlation is not sufficient evidence for a causal association between traits. The LCV method tests whether a genetic correlation between two traits may be explained by a causal association rather than by horizontal pleiotropy (O’Connor and Price, 2018). Thus, the first step requires estimating the genetic correlation between two traits and, in our case, filtering those without significant evidence of a genetic correlation. We corrected for multiple testing using Benjamini-Hochberg’s False Discovery Rate (FDR < 5% for genetic correlations).
The LCV method can be conceptualised by a model in which a latent variable L represents the causal component that mediates the genetic correlation between two traits. Given a causal exposure and an outcome, all of the genetic effects for the exposure will be proportional on the outcome. Nonetheless, the genetic effects of the outcome are not expected to be proportional for the exposure. Assuming no bi-directional causality, one could argue such an observation to be evidence of horizontal pleiotropy. The LCV approach estimates a genetic causal proportion statistic (GCP) based on the estimated effects of the causal component L on both traits. The ratio between the normalised effects of L for both traits is then modelled as a function of the genetic correlation elevated to the GCP. A GCP value of zero, which emerges when the proportionality of effect sizes is observed in both directions, implies no evidence for genetic causality (García-Marín et al., 2020). Thus, the genetic correlation is fully explained by a direct effect of the same variants on both traits rather than by causality between traits. Conversely, a GCP value near 1 or −1 implies full genetic causality of the first trait on the second or vice versa, respectively. Intermediate values can be considered evidence of partial genetic causality, which can be considered a relationship including both pleiotropic effects and a causal association. For more details, we refer the reader to Haworth et al. (2021). Notably, LCV uses the summary statistics across the whole genome and is not limited to genome-wide significant hits only.
We performed genetic correlation analysis for suicide attempt and 1520 traits. Traits with a significant genetic correlation were further investigated using LCV. Traits were excluded if they were too underpowered (no significant SNP-based heritability) or showed no evidence of a genetic correlation with suicide attempt risk (FDR > 5%). Analyses were carried out using the phenome-wide analysis pipeline available at the Complex-Traits Genomics Virtual Lab (www.genoma.io) web platform (Cuellar-Partida et al., 2019). A detailed description of the approach is available elsewhere (García-Marín et al., 2020; Haworth et al., 2021; O’Connor and Price, 2018). Statistical significance was defined as FDR < 1% for the genetic causal proportion, as we wanted to be more strict when inferring causality. Importantly, the LCV approach does not yield an intuitive value (i.e. an odds ratio) of the strength of the causal association. Keeping the GCP equal, associations based on higher genetic correlations would have stronger effects compared with those between traits with smaller genetic correlations. A causal architecture plot based on both genetic correlation and GCP was used to depict the LCV results.
Sensitivity Mendelian randomisation analyses
As mentioned above, MR is a type of instrumental variable analysis that can test for causality so long as three key assumptions are met. The first one is that the genetic variants are a valid proxy for the exposure of interest, which translates into identifying variants with strong evidence of association with the exposure. The second assumption is that there is no confounder that could mediate the association between the instrumental variable and the outcome and the third assumption is that the genetic variants do not directly affect the outcome of interest, that is, their effect is completely mediated through the exposure they approximate (Gagliano Taliun and Evans, 2021). Here, we sought to perform MR as sensitivity analyses for the associations identified. To fulfil the assumptions, we performed linkage disequilibrium–based clumping to identify independent genome-wide SNPs for each causal trait identified by the LCV. We selected only traits with more than 10 independent SNPs passing the genome-wide significance threshold and tested for their causal effect on suicide attempt using five different MR methods that test or relax different assumptions. Clumping was performed on plink v1.9, and MR analyses were performed using the MR Base package in R.
Results
Of the 1520 traits under study, 606 showed significant evidence (FDR < 5%) of a genetic correlation with suicide attempt. After applying LCV to these, 73 showed strong statistical evidence (FDR < 1%) of a predicted causal association with suicide attempt. Finally, 65 traits had an absolute GCP value higher than 0.6, a cutoff suggested for causal inference (Supplementary Table 1).
Overall, 62 (95%) of the traits mentioned above were predicted to be risk factors (i.e. modifying the risk) for suicide attempt, whereas three were predicted as causal consequences of suicide attempt including No weight change during the worst episode of depression, frequency of solarium or sun lamp use and intelligence (IQ). Suicide attempt was negatively associated with these characteristics such that greater likelihood of suicide attempt predicted reduced risk for, or a reduction of, these traits. For example, one would interpret the IQ result as a suicide attempt resulting in an IQ reduction (Figure 1 and Supplementary Figure 1).
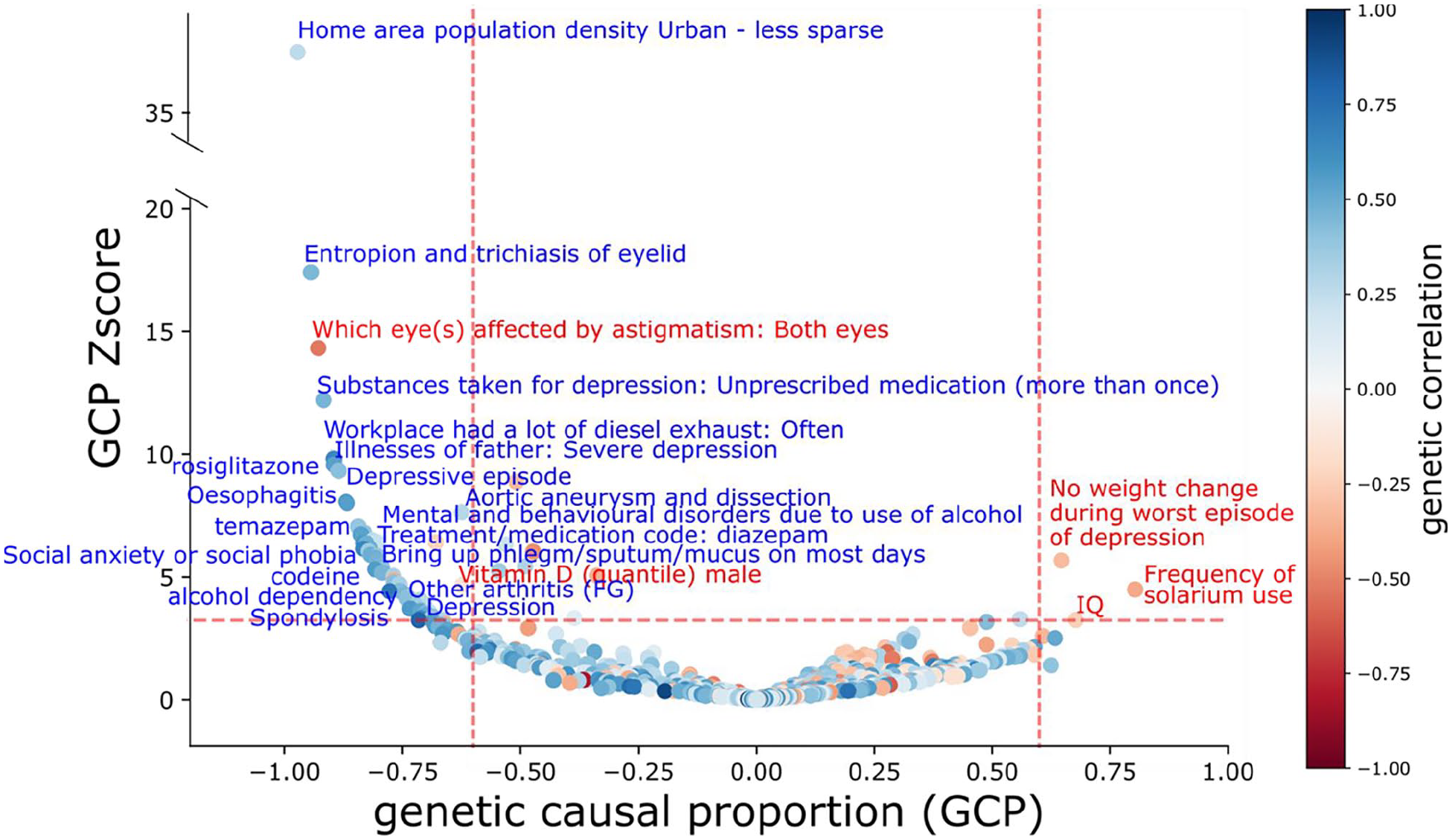
Causal architecture plot illustrating results for the latent causal variable phenome-wide results. The x-axis shows the genetic causal proportion (GCP) statistic, while the y-axis shows the GCP z-score as a measure of statistical significance. Statistical significance threshold (FDR < 1%) is represented by the horizontal red dashed lines, whereas the vertical red dashed lines represent the threshold for strong estimates (|GCP| > 0.60).
Within the traits identified as causal influences of suicide attempt, four were predicted protective factors, whereas 58 were predicted to be risk factors. Risk factors could be broadly grouped into three distinct categories: (1) psychiatric or mood-related traits such as depression, alcohol and other substance misuse or abuse and anxiety (as proxied by the use of diazepam and temazepam); (2) physical health conditions including spondylopathies, hernia, reflux disease, arthritis, diabetes (i.e. medication code rosiglitazone) and oesophagitis; and finally, (3) lifestyle behaviours and environmental exposures such as been involved in combat or exposed to war-zone, being part of the armed forces, occupations such as heavy goods driver, lorry or truck driver, machine operator, processor and foreman. A remarkable risk factor identified was International Classification of Diseases, Tenth Revision (ICD-10) diagnosis poisoning by nonopioid analgesics, antipyretics and antirheumatics (rg = 0.8, GCP = −0.71, p = 0.0012), which be considered a proxy for a type of suicide attempt.
Four protective factors were inferred based on having a negative genetic correlation and a negative GCP. The first one was vitamin D quantile measured in males. The second one was never being recommended to stop or reduce alcohol consumption which is consistent with risk factors related to substance use mentioned above. Finally, vision-related conditions such as astigmatism in both eyes and myopia were also identified as protective factors that buffered risk for suicide attempt (Figure 1).
MR sensitivity analyses
After LD clumping, only four traits associated as causally associated with suicide attempt had 10 or more independent genome-wide significant variants. These traits were ‘IQ’, ‘Hernia’, ‘vitamin D quantile measured in males’ and ‘reasons for glasses myopia’. The LCV results suggest potential changes in IQ as a consequence of a suicide attempt. As the suicide attempt GWAS has very few genome-wide loci, we could not test this association using MR (see methods). We tested for the causal effect of the remaining three traits on suicide attempt using MR. None of these associations showed evidence for a causal association through MR after multiple testing correction (Supplementary Table 2). Hernia showed a nominally significant evidence of increasing risk for suicide attempt but only through the MR Egger method (p = 0.049).
Discussion
The current study aimed to generate testable hypotheses regarding suicide attempt risk and protective factors. To this end, we employed the LCV analysis, a powerful approach to test whether the genetic correlation between two traits can be explained by a causal association while modelling potential horizontal pleiotropy. This approach allows one to disentangle whether two traits share the same genetic variants because of causality rather than common pathways. Our results identified 65 traits with evidence (FDR < 0.01; absolute GCP > 0.6) of a causal association with suicide attempt, of which 62 were risk factors while only 3 were inferred outcomes.
Three outcomes or sequelae associated with suicide attempt were identified, including ‘stayed about the same weight or was on a diet during worst episode of depression’ and decreases in ‘frequency of solarium use’ and intelligence. Medical and psychological interventions usually follow a suicide attempt and some antidepressant and psychotropic medications increase photosensitivity, which would be consistent with a decrease in the frequency of solarium use. However, the frequency of solarium use is also positively correlated with measures of intelligence in the UK Biobank. It is unclear whether this association holds true after accounting for the relationship with intelligence as a previous study observed cognitive impairments after a suicide attempt (Gujral et al., 2016).
We found that depression and anxiety were antecedents of suicide attempt, consistent with some work showing that these conditions were precursors of suicidal behaviours (Franklin et al., 2017; Mann and Rizk, 2020; Nepon et al., 2010). For instance, around ~70% of individuals who report a lifetime history of suicide attempt suffered from an anxiety disorder (Nepon et al., 2010). Causality has been difficult to infer due to cross-sectional designs and lack of information on the temporal relationship between suicide and psychopathology. In the present study, depression and experiencing a depressive episode (ICD10) were identified as risk factors for suicide attempt. Similarly, experiencing the death of a close friend or relative in the last 2 years, which is considered a potential risk factor for depression and anxiety (Keyes et al., 2014), was found to increase risk for suicide attempt. In addition, our results show a causal association in which social anxiety or social phobia and diazepam, a common treatment medication for anxiety (Pringle et al., 2016), increases the risk of suicide attempt.
In our study, substance use–related phenotypes such as ever addicted to any substance or behaviour, alcohol dependency, codeine intake, a highly addictive opioid, and poisoning by nonopioid analgesics, antipyretics and antirheumatics (ICD10) were identified as risk factors for suicide attempt. Both acute and chronic substance use may hamper decision making and contribute to poorer self-control and neurocognitive deficits, which may exacerbate risk for suicide behaviours (Connery et al., 2020). Also, never had known a person that recommends a reduction of alcohol consumption was observed as a protective factor for suicide attempt. Furthermore, phenotypes involving addictions co-occurring with psychiatric disorders, including mental and behavioural disorders due to the use of alcohol (ICD10) and taken drugs or alcohol for anxiety more than once, were also found to potentially increase suicide attempt risk. The co-occurrence of substance use disorders with psychiatric disorders, including mental and behavioural disorders due to the use of alcohol (ICD10) and taken drugs or alcohol for anxiety more than once, was also found to be potent risk factors for suicide attempt risk, which is consistent with work showing that suicide behaviours are often intensified when substance use and mental health disorders are comorbid (Esang and Ahmed, 2018). Alcohol dependence is known to co-occur with psychiatric conditions such as depressive disorders (McHugh and Weiss, 2019) and more frequent, heavy use of alcohol in this population could lead to suicide attempts by contributing to disinhibition, impulsiveness and impaired judgement (Pompili et al., 2010). Overall, substance has been associated with increased suicide attempt rates after adjusting for psychiatric comorbidities but causality remained to be tested (Nock et al., 2009). A recent report (Marees et al., 2020) showed the presence of genetic correlations between SES and several substance use phenotypes. The direction of such correlations was specific to each trait. For example, alcohol consumption frequency was positively correlated with SES, whereas alcohol consumption quantity was negatively associated with SES. Lower SES has been linked to increased risk for suicidal behaviours (see below). Thus, we cannot rule out the possibility that the associations between substance use and suicide attempt identified here are driven through residual SES signals.
Several occupations and work environments were shown to exacerbate risk for suicide attempt. Previous studies have shown that rural areas are associated with a higher risk for suicide death (Goldman-Mellor et al., 2018; San Sebastián et al., 2020), whereas urban areas increase the risk for non-fatal suicide behaviours (Goldman-Mellor et al., 2018). Our results support that living in an urban home area increases the risk for suicide attempt, which is also consistent with work showing that residing in urban communities is associated with heightened risk for mental health conditions such as schizophrenia (Colodro-Conde et al., 2018). We also found that occupations involving a physical or chemical hazard such as machine operator, being at a workplace that had a lot of diesel exhaust, and food, drink and tobacco process operatives were identified as causal for suicide attempt. These associations are consistent with reports of occupation-related higher suicide rates, which are typically explained by access to lethal means increasing the capability to enact self-harm (Milner et al., 2013, 2017). To date, there are two hypotheses compatible with these types of risk factors, causation, or selection. For example, causation suggests an urban environment increases the risk of schizophrenia (Colodro-Conde et al., 2018). Selection, on the other hand, proposes individuals with a higher genetic loading to psychiatric illness move into urban areas. Our study would favour the causation hypothesis, as almost the whole genetic correlation between urban living and suicide attempt can be explained via a latent causal component. However, the causal associations between the occupation of an individual and suicide attempt could also be mediated by SES, perhaps as a consequence of chronic stress or the development of a mental health condition (Reiss et al., 2019). Indeed, previous studies have described the relationship between socioeconomic status (SES) and suicidality, showing that individuals in the lowest income level have higher rates of suicide behaviour (Kim et al., 2016; Taylor et al., 2005) and are more likely to encounter adverse working conditions in which they are exposed to physical and chemical hazards (Clougherty et al., 2010). Future research should explore the specific mechanism through which occupational exposures augmented risk for suicide attempt.
In the present study, been involved in combat or exposed to war-zone and working in armed forces were identified as causal for suicide attempt. Going through a combat or war experience could influence the development of psychiatric conditions such as post-traumatic stress disorders (PTSD), potentially leading to suicidality (Griffith, 2012). PTSD is known to overlap with major depressive disorder and other psychiatric comorbidities (Gros et al., 2012), but has been reported to be associated with suicide attempt, possibly through greater rumination, in fully adjusted models accounting for other psychopathologies (Batterham et al., 2018).
Medical risk factors for suicide attempt included musculoskeletal phenotypes such as fibromyalgia related comorbidities, spondylopathies, spondylosis (ICD10), hernia and spine arthritis or spondylitis. These conditions are characterised by acute or chronic pain. Moreover, previous findings have shown an overlap between fibromyalgia and PTSD, suggesting that experiencing traumatic events is a risk factor for fibromyalgia in genetically predisposed individuals (Conversano et al., 2019). In addition, chronic pain has been associated with a higher risk for depression, suicide attempt and use of alcohol, tobacco and misuse of painkillers (Roughan et al., 2021). Similarly, fibromyalgia and spondylosis have been shown to correlate with suicidal ideation among those with psychiatric comorbidities (Lan et al., 2016; Levine and Horesh, 2020; Triñanes et al., 2015), whereas young adults with arthritis are more likely to report a suicide attempt (Fuller-Thomson et al., 2016). Our results align with the hypothesis that the causal relationship between musculoskeletal phenotypes and suicide attempt is mediated by chronic pain and psychiatric comorbidities, which in turn could be influenced by experiencing a stressful life event.
Conditions related to physical illness also increased risk for suicide attempts. These include endocrine, nutritional and metabolic diseases, oesophagitis (ICD10), entropion and trichiasis of eyelid, aortic aneurysm and dissection (ICD10), pneumonia (ICD10) as well as malignant neoplasm of the respiratory system and intrathoracic organs. Furthermore, medications such as rosiglitazone, serevent and propranolol were also found to be associated with suicide attempt and can be used as proxies for chronic diseases including diabetes, asthma and hypertension or angina pectoris, respectively. Our results suggest that individuals with a chronic disease are at an increased risk of a suicide attempt, perhaps a consequence of hopelessness (Goodwin, 2011; Racine, 2018) reduction of life quality, disruptions in daily activity (Onyeka et al., 2020) or facing a future believed to be of further loss. Nonetheless, given that chronic pain, regardless of its type, is considered an independent risk factor for suicidality (Racine, 2018), we cannot rule out the possibility of chronic pain and psychiatric comorbidities (Roughan et al., 2021) being the causal factor mediating the relationship between physical illness and suicide attempt. More research is required to determine the extent to which chronic pain and psychological distress resulting from a clinical diagnosis could increase suicide risk. Finally, our study found vitamin D was a protective factor for suicide attempt. Consistently, recent studies have reported vitamin D deficiency to correlate with suicide attempt (Gokalp, 2020) and ideation (Kim et al., 2020), our study suggests causality drives these associations. Thus, the mechanisms underlying the association of vitamin D with suicidality should be further studied to identify potential new interventions.
A myriad of risk factors for suicide attempt, including occupations and behaviours, have been investigated (McClatchey et al., 2017). Nonetheless, all of these studies have to be, by design, observational and retrospective. As such, there is little to no evidence to claim causality and establish the direction of effects truly. This is the first study to systematically infer potential risk factors for suicide attempt using a hypothesis-free, genetically informed approach. Many of our findings, such as depression- and anxiety-related traits, could be viewed as evidence that the LCV method is recapitulating known risk factors. We further unveiled potentially interesting protective factors such as vitamin D levels and reduction of alcohol intake.
Our results should be considered within certain limitations. First, the GWAS meta-analysis for suicide attempt focused on lifetime suicide attempt measured through a variety of instruments. The GWAS results may be affected by reporting biases inherent to studying suicidal behaviours such as reduced disclosure (Klimes-Dougan et al.,2007). These biases have been shown to correlate with psychometric measures. For example, participants that forgot a previous suicidal behaviour showed improved mental health compared to those who recalled the suicidal behaviour (Goldney et al., 2009). Sensitivity MR analyses were only possible for three of the traits identified in this study. None of the sensitivity analyses identified evidence for a causal association. We attribute these findings to the fact that LCV has been shown to have higher power than MR when there is differential power between the exposure and the outcome (O’Connor and Price, 2018). LCV identified phenotypes such as psychiatric traits and chronic pain, which are known risk factors for suicide attempt. This could be taken as evidence that LCV is converging into known risk factors. Finally, lack of evidence for an association with MR is not strong evidence for a lack of association. Future studies should aim at generating well-powered GWAS for these traits and perform a set of targeted causal association studies to assess the findings presented herein.
Although the LCV method increases statistical power by aggregating information throughout the genome, the GCP estimate is tied to the power of the GWAS used (García-Marín et al., 2020; O’Connor and Price, 2018). The suicide attempt GWAS results are still underpowered and we cannot rule out differential power affecting these results. We aimed to perform a hypothesis-free unbiased exploration of potential risk factors for suicide attempt. Therefore, we did not filter out any of the traits in the database based on their interpretability. Nonetheless, upon inspection of the results, some traits lack a straightforward interpretation, especially as outcomes of a GWAS. For instance, medication use GWAS in the present study was considered as a proxy for the disease they are commonly prescribed for. However, common non-specific medications lack such a clear interpretation. Another example is ‘both eyes affected by astigmatism’ which is a case-case GWAS within participants with astigmatism. Thus, the fact that it appeared to be a protective factor might be due to collider bias induced by comparing the samples with astigmatism in one eye against the sample with astigmatism in both eyes. Participation or ascertainment biases will affect GWAS and their downstream results.
Many of the GWAS used here are from the UK Biobank, which does not necessarily represent the UK population. Biases related to population stratification and SES may lower the quality of the GWAS, and false positive associations may occur if these biases are persistent across discovery and target samples. Finally, in GWAS involving different samples, our capability to detect genetic overlap and downstream causality could be limited by differential exposures in the samples. In the worst-case scenario, one sample is completely naive to an exposure and therefore a genetic overlap will not be recapitulated (Rabinowitz et al., 2021). We envision this effort as a hypothesis-generating study; the causal associations identified here should be tested in follow-up studies, either through longitudinal and interventional studies or through using MR leveraging the most powered GWAS available. There is, to date, no suicide attempt GWAS with enough power to perform bi-directional MR studies.
In summary, we assessed causal relationships between suicide attempt and 1520 phenotypes, of which 65 were identified as causal determinants, 62 as precedents and three as causal outcomes. Our findings highlight the role of psychiatric disorders such as depression, anxiety and PTSD as risk factors for suicide attempt. We show the causal influence of alcohol consumption and substance abuse on an increased risk for suicide attempt. We provide evidence for a causal association whereby urban living increases an individual’s risk for a suicide attempt, an observation where causality has so far remained controversial. Similarly, we uncover specific occupations and work environments that may increase suicide attempt risk. Also, we show the relevance of physical illness, particularly chronic disease and pain, in the increase of suicide attempt risk. We further unveiled potentially protective factors such as vitamin D levels and reduction of alcohol intake. Overall, our results confirm findings from previous studies and pinpoint new insights and testable hypotheses with the objective to inform the design of emerging studies, interventions and prevention programmes. Future analyses should use multivariate causal association methods to assess to what extent each of these factors contribute independently to suicide attempt risk.
Supplemental Material
sj-csv-2-anp-10.1177_00048674221091499 – Supplemental material for Genomics-driven screening for causal determinants of suicide attempt
Supplemental material, sj-csv-2-anp-10.1177_00048674221091499 for Genomics-driven screening for causal determinants of suicide attempt by Adrian I Campos, Luis M Garcia-Marin, Helen Christensen, Philip J Batterham, Laura S van Velzen, Lianne Schmaal, Jill A Rabinowitz, Neda Jahanshad, Nicholas G Martin, Gabriel Cuellar-Partida, Douglas Ruderfer, Niamh Mullins and Miguel E Rentería in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-1-anp-10.1177_00048674221091499 – Supplemental material for Genomics-driven screening for causal determinants of suicide attempt
Supplemental material, sj-docx-1-anp-10.1177_00048674221091499 for Genomics-driven screening for causal determinants of suicide attempt by Adrian I Campos, Luis M Garcia-Marin, Helen Christensen, Philip J Batterham, Laura S van Velzen, Lianne Schmaal, Jill A Rabinowitz, Neda Jahanshad, Nicholas G Martin, Gabriel Cuellar-Partida, Douglas Ruderfer, Niamh Mullins and Miguel E Rentería in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-3-anp-10.1177_00048674221091499 – Supplemental material for Genomics-driven screening for causal determinants of suicide attempt
Supplemental material, sj-docx-3-anp-10.1177_00048674221091499 for Genomics-driven screening for causal determinants of suicide attempt by Adrian I Campos, Luis M Garcia-Marin, Helen Christensen, Philip J Batterham, Laura S van Velzen, Lianne Schmaal, Jill A Rabinowitz, Neda Jahanshad, Nicholas G Martin, Gabriel Cuellar-Partida, Douglas Ruderfer, Niamh Mullins and Miguel E Rentería in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-xlsx-4-anp-10.1177_00048674221091499 – Supplemental material for Genomics-driven screening for causal determinants of suicide attempt
Supplemental material, sj-xlsx-4-anp-10.1177_00048674221091499 for Genomics-driven screening for causal determinants of suicide attempt by Adrian I Campos, Luis M Garcia-Marin, Helen Christensen, Philip J Batterham, Laura S van Velzen, Lianne Schmaal, Jill A Rabinowitz, Neda Jahanshad, Nicholas G Martin, Gabriel Cuellar-Partida, Douglas Ruderfer, Niamh Mullins and Miguel E Rentería in Australian & New Zealand Journal of Psychiatry
Footnotes
Author Contributions
A.I.C. and M.E.R. designed this study. A.I.C. and L.M.G.-M. wrote the first version of the manuscript. A.I.C. performed the analyses with input from, G.C.-P., L,M.G.-M., M.E.R. and N.G.M. N.M. and D.R. led the international suicide genetics consortium effort to produce GWAS of suicide attempt. H.C., P.J.B., L.S., L.S.V., J.A.R., N.J. and N.G.M. critically appraised the study and interpretation and helped drafting the manuscript. All co-authors provided feedback and approved the manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A.I.C. is supported by a UQ Research Training Scholarship from The University of Queensland (UQ). M.E.R. thanks the support of NHMRC and the Australian Research Council (ARC), through a NHMRC-ARC Dementia Research Development Fellowship (GNT1102821) and NHMRC Centre for Research Excellence in Suicide Prevention (GNT1042580 and GNT1152952). H.C. is supported by a NHMRC Senior Principal Fellowship (GNT1155614). L.S. and L.v.V. are supported by the MQ Brighter Futures Award (MQBFC/2) and the National Institute of Mental Health of the National Institutes of Health under Award Number (R01MH117601). P.J.B. is supported by NHMRC Fellowship (1158707) . We gratefully acknowledge all the studies and databases that made GWAS summary data available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.