
Abstract
Objective:
Depression is one of the most prevalent and disabling mental health conditions among young people worldwide. The health and economic burdens associated with depressive illness are substantial. Suicide and depression are closely intertwined, yet a diagnosis of depression itself lacks predictive specificity for suicidal behaviour. To better inform suicide prevention and early intervention strategies for young people, improved identification of modifiable intervention targets is needed. The objective of this review was to identify clinical, psychosocial and biological correlates of suicidality in young people diagnosed with a broad range of unipolar and bipolar depressive disorders.
Method:
Systematic searches were conducted across MEDLINE, Embase and PsycINFO to identify studies of young people aged 15–25 years diagnosed with unipolar or bipolar depressive disorders. An assessment of suicidality was required for inclusion. Reporting followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 and Synthesis Without Meta-analysis guidelines.
Results:
We integrated findings from 71 studies including approximately 24,670 young people with clinically diagnosed depression. We identified 26 clinical, psychosocial and biological correlates of suicidality. Depression characteristics (type and severity), psychiatric comorbidity (particularly anxiety and substance use disorders) and neurological characteristics emerged as having the most evidence for being associated with suicidal outcomes. Our ability to pool data and conduct meaningful quantitative synthesis was hampered by substantial heterogeneity across studies and incomplete reporting; thus, meta-analysis was not possible.
Conclusion:
Findings of this review reinforce the notion that suicidality is a complex phenomenon arising from the interplay of multiple contributing factors. Our findings question the utility of considering a diagnosis of depression as a specific risk factor for suicidality in young people. Suicidality itself is transdiagnostic; adoption of a transdiagnostic approach to investigating its aetiology and treatment is perhaps warranted. Future research investigating specific symptoms, or symptom networks, might help to further our understanding of suicidality among young people experiencing mental illness.
Mid-adolescence to young adulthood is a particularly vulnerable period for the onset of mental disorders (Bilsen, 2018; Gore et al., 2011; Solmi et al., 2021). Depression is one of the most common mental disorders experienced by young people and globally is one of the leading causes of illness and disability among those aged <24 years (Vos et al., 2020). Depression is associated with a host of adverse outcomes, including suicidality (Davey and McGorry, 2019; Jaffee et al., 2002). Suicidality can be defined as encompassing suicidal ideation (SI) (passive and active thoughts of death) and suicidal behaviour (preparatory suicidal acts, and both non-fatal and fatal suicide attempts) (Bridge et al., 2006; Bursztein and Apter, 2009; Pelkonen and Marttunen, 2003). While suicide is a leading cause of mortality among young people worldwide (World Health Organization [WHO], 2018), death due to suicide is nevertheless a relatively low prevalence outcome, even among young people receiving psychiatric care (McHugh et al., 2019). However, due to the psychosocial morbidity and increased use of health services associated with suicidality, the health and economic burdens associated with it are substantial (Islam et al., 2020; Pirkis et al., 2001; Torok et al., 2019; Whitlock et al., 2014). It is therefore essential to consider the entire spectrum of suicidality, and not only suicide deaths, in suicide prevention and early intervention efforts.
Our focus in this review is on young people aged 15–25 years, diagnosed with depressive disorders. Depression is the most common feature among young people who experience suicidality (Hetrick et al., 2012; Nock et al., 2008) and is the most common type of mental disorder associated with suicide deaths, indicated in over 60% of cases (Cavanagh et al., 2003; Werbart Törnblom et al., 2020). Nevertheless, depression itself lacks specificity as a suicidality predictor (Franklin et al., 2017). Numerous other factors are associated with suicidality in young people, including psychological and physical trauma, psychiatric comorbidity, family adversity, social isolation, non-heterosexual orientation, substance use and non-suicidal self-injury (NSSI) (Bridge et al., 2006; Cha et al., 2018; Hawton et al., 2012; Pelkonen and Marttunen, 2003); however, these factors also lack specificity and are not reliable predictors of suicidality at an individual level (Franklin et al., 2017; Goldney et al., 2000). Developing a better understanding of the complexities of suicidality and its contributory factors in young people with depression could help inform more effective prevention strategies and assist in identifying targets for early intervention (O’Connor and Portzky, 2018), with the aim of helping to reduce the health burden associated with suicidality.
Although numerous systematic reviews have been published on suicidality in young people, previous reviews have focused on particular aspects, such as interventions (Daniel and Goldston, 2009; Ougrin et al., 2015), prevention efforts (Calear et al., 2016; Robinson et al., 2011, 2018; Torok et al., 2019), screening methods (Harris et al., 2019), prespecified aetiological or risk factors (Castellví et al., 2017; Kim et al., 2014; King and Merchant, 2008; McHugh et al., 2019; Memon et al., 2018), specific stages of the suicidal spectrum (De Crescenzo et al., 2017), specific populations such as non-clinical samples (Evans et al., 2005; Miranda-Mendizabal et al., 2019) or specific sociocultural groups (Wyatt et al., 2015). These systematic reviews provide important insights into certain aspects of suicidality; however, there are no recent comprehensive systematic reviews that provide a broad characterisation of suicidality correlates in young people with a range of clinically diagnosed depressive disorders. In this review, we have included both unipolar and bipolar depressive disorders and have encompassed a wide range of clinical, psychosocial and biological factors that are potentially associated with suicidal outcomes. Many existing reviews in this area focus on young people with depressive symptoms in the general community (Evans et al., 2004, 2005; Miranda-Mendizabal et al., 2019), and we have therefore sought to encompass evidence from a variety of clinical and non-clinical settings.
Objectives
We aimed to systematically review the literature to characterise correlates of suicidality in young people with clinically diagnosed unipolar and bipolar depressive disorders. We wanted to know what clinical, psychosocial and biological factors are associated with suicidality in young people (aged 15–25 years) with depressive disorders, and whether these factors vary between clinical and non-clinical settings.
Methods
This review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology for systematic reviews of aetiology and risk (Moola et al., 2020). Reporting of this systematic review conforms with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) statement (Page et al., 2021) and the Synthesis Without Meta-analysis (SWiM) reporting guideline (Campbell et al., 2020). The SWiM guideline serves as an extension to PRISMA 2020 for systematic reviews in which meta-analysis is not possible. The objectives, inclusion criteria and methods of analysis for this review were specified in advance; registered with PROSPERO (CRD42020151612); and published in an a priori protocol (Moller et al., 2021). Deviations from the published protocol are described in Appendix 1.
Eligibility criteria
This review included studies involving individuals aged 15–25 years with a current or lifetime diagnosis of any unipolar or bipolar depressive disorder, made in accordance with any edition of either the WHO International Classification of Diseases (ICD) or the Diagnostic and Statistical Manual of Mental Disorders (DSM). This age range encompasses the peak onset of mood disorders, and the period when there is a rapid increase in suicidality from childhood (Bridge et al., 2006; Davey and McGorry, 2019). This aligns with the definition adopted by the WHO (1986) which classifies young people as those aged 10–24 years; however, in this review, we have excluded ages 10–14 years where suicidality is relatively uncommon (Roh et al., 2018). In some instances, extracted data include participants slightly outside our stated age range, but in all instances, the great majority of participants were between 15 and 25 years old (see Table 1). Diagnosis of a depressive disorder must have been made on the basis of a standardised structured clinical interview or be received through standard clinical practice. The diagnosis of depression may be either a primary or a secondary diagnosis. Individuals with psychiatric disorders and/or personality disorders comorbid with depression were also eligible for inclusion. Included studies had to encompass an assessment of suicidality, made using either standardised or non-standardised tools. Suicidality occurring at any timepoint up to the time of assessment was eligible for inclusion.
Characteristics of all included studies (N = 71) grouped by study design.
$: estimated or calculated based on information provided in the publication; SI: suicidal ideation; NR: not reported; ?: lack of clarity in source; ~: approximately.
NB: sample size is based on those who met our stated inclusion criteria; this figure may be equivalent to or smaller than the total sample size of the study in question.
DSM: Diagnostic and Statistical Manual of Mental Disorders; ICD: International Statistical Classification of Diseases and Related Health Problems.
CIDI: Composite International Diagnostic Interview; DIS(C): Diagnostic Interview Schedule (for Children); (K-)SADS: (Kiddie) Schedule for Affective Disorders and Schizophrenia; (-E): Epidemiological version; (-P): Present version; (-PL): Present and Lifetime version; LIFE: Longitudinal Interval Follow-up Evaluation; MINI: Mini International Neuropsychiatric Interview; SCID: Structured Clinical Interview for DSM Disorders.
ADDM: adjustment disorder with depressed mood; BD: bipolar disorder/s; DD: depressive disorder; DD-NOS: depressive disorder not otherwise specified; DYS: dysthymia/dysthymic disorder; MD: major depression; MDD: major depressive disorder; MDE: major depressive episode; MnD: minor depression.
Information sources and search strategy
Three databases were searched in this review: MEDLINE, Embase and PsycINFO. All searches were conducted through the Ovid interface. A multi-step search strategy was employed. Initially, a limited search of MEDLINE was conducted to identify articles pertaining to suicide in young people with depression. Key words in the titles and abstracts, and the index terms used to describe these articles, were used to develop a preliminary search string using Medical Subject Headings (MeSH terms) related to suicide and depression in young people. MeSH terms were identified using the US National Library of Medicine (NLM) ‘MeSH on Demand’ tool, and further refined using the NLM MeSH Browser database to map relevant key words onto the MeSH tree structure. Expanded MeSH terms were also included in the search string as free-text search terms. This search string was adapted as necessary to the syntax and subject headings of each database. The complete search strategies for all three databases are reproduced in Appendix 2. Searches using these refined search strategies were first conducted across all included databases on 16 April 2020. Searches were conducted again on 8 December 2021 to identify any new articles published since the initial searches. No upper or lower limitations were placed on the date of publication. Searches were limited to peer-reviewed primary sources containing original data, published in English. The search excluded books, case reports, meta-analyses, reviews, letters, editorials, comments, conference abstracts and conference papers. All database searches were conducted by the lead author (CM).
Selection process
The screening process was managed using Covidence (Veritas Health Innovation, 2021). All records were double screened at both the title/abstract and full-text stages. Screening was conducted independently by the lead author and at least one other review author. Initially, titles and abstracts of all publications were screened against the stated inclusion criteria. Those that appeared to meet these criteria were retained and the full-texts of these studies were retrieved for further screening. In the case of a disagreement between reviewers at the title/abstract screening stage, the study was retained for full-text screening. If the title/abstract contained insufficient information for a decision to be made regarding the study’s eligibility for inclusion, it was likewise retained for full-text screening.
At the second screening stage, the full texts of all publications included at the first screening stage were screened to determine eligibility for inclusion. A decision flowchart (Appendix 3) was employed to assist reviewers in the process of determining whether a study met the review’s criteria for inclusion and if not, the most appropriate reason for exclusion. Inclusion and exclusion decisions at this stage were recorded by each reviewer in Covidence. There were 54 screening conflicts at the full-text stage, representing a conflict rate of approximately 3%. Screening conflicts arose for a multitude of reasons, the most common being a lack of clarity around whether the age characteristics of a given study’s cohort sufficiently met our selection criteria. All conflicts were resolved through consultation between reviewers.
Data collection process
The data collection process was also managed using Covidence. All data collection was conducted independently by the lead author and at least one other review author. A data extraction form was created in accordance with the JBI data extraction methodology for systematic reviews of aetiology and risk (Moola et al., 2020) and used to enter data extracted from eligible studies. Any discrepancies between data extracted by reviewers were resolved by the lead author, in consultation with reviewers if necessary; however, such discrepancies were infrequent and predominantly related to the amount of detail that was extracted from the source article, rather than errors in the extracted data. There were no instances where it was deemed necessary to contact authors of included studies to obtain further information.
Data items
Suicidality outcomes
Outcomes assessed in this review cover the full spectrum of suicidality. This encompasses SI (including passive and active thoughts of death) and suicidal behaviour (including preparatory suicidal acts and both non-fatal and fatal suicide attempts). Any method of assessing suicidality was eligible for inclusion, including standardised or non-standardised tools, which could be either self-reported or clinician administered. Recent systematic reviews (Goodfellow et al., 2018, 2020) have highlighted a lack of consensus in the literature regarding terminology and definitions of suicidality; thus, we expected that definitions and assessment criteria of suicidality would vary substantially across studies. We accepted any definition that incorporated the element of death (such as thinking about death or wanting to die), but excluded from our definition of suicidality NSSI (i.e. harm inflicted without the intent to die) (Nock, 2010). 1 We extracted data according to the following outcome domains: suicidality assessment method; aspects of suicidality reported; prevalence of SI; prevalence of suicide attempt; and prevalence timeframe. If suicidality outcome data were available in a study at multiple timepoints (e.g. in longitudinal analyses), we extracted data for all available timepoints. No restrictions were placed on the study duration or the number of timepoints at which outcomes were assessed.
Correlates of suicidality
A broad range of clinical, psychosocial and biological factors were considered. Factors in the clinical domain included attributes of depressive illness such as type of depression diagnosis, depression duration and recurrence, depression severity and comorbid psychiatric and/or personality disorders. The psychosocial domain included attributes such as age, sex, alcohol consumption, NSSI, sexual orientation, social support, living situation, engagement in work or study and stressful life events. Biological factors included inflammatory biomarkers, and structural and functional neuroimaging findings.
Risk of bias assessment
Risk of bias was assessed using a modified version of the JBI critical appraisal checklist for analytical cross-sectional studies (Moola et al., 2020). This modified checklist included the checklist for analytical cross-sectional studies in its entirety, plus selected items from both the JBI critical appraisal checklist for case series, and critical appraisal checklist for cohort studies; this modified checklist is provided in Appendix 4. Responses to these additional checklist items were extracted as appropriate for the design of each included study. All included randomised controlled trials (RCTs) and case–control trials were assessed using the critical appraisal tool for cohort studies, as aspects relating to interventions were not within the scope of this review of aetiology and risk. We did not aim to assess the effects of interventions on suicidality; thus, RCTs were only included if pre-intervention data could be extracted from the publication.
The JBI critical appraisal checklist for analytical cross-sectional studies incorporates critical evaluation of numerous important aspects, including sampling strategy, sample and setting characteristics, assessment of exposure variables, identification of and adjustment for confounding factors, reliability and validity of outcome assessment methods and the appropriateness of statistical methods employed. Items relating to cohort studies assess appropriateness of follow-up interval/s, assessment of any loss to follow-up and strategies to address incomplete follow-up. Items relating to case series assess the extent to which complete and consecutive inclusion of participants was achieved. Each checklist item comprises a question (e.g. ‘Were the criteria for inclusion in the sample clearly defined?’) and is scored either ‘Yes’, ‘No’, ‘Unclear’ or ‘Not Applicable’. More items scored ‘Yes’ is interpreted as lower risk of bias; however, the JBI checklist approach does not set a priori criteria for determining high, low or unclear risk of bias. Results of the risk of bias assessment were not used to exclude studies from this review. The risk of bias assessments were conducted by the lead author and at least one other review author, independently of each other. Any disagreements were resolved by the lead author in consultation with review authors; however, discrepancies were infrequent.
Grouping studies for synthesis
Studies were initially grouped according to their design: (1) prospective cohort studies; (2) cross-sectional and case series studies. The strength of evidence provided by prospective studies is potentially higher than that provided by retrospective/cross-sectional studies (Grimes and Schulz, 2002). Suicidality correlates (i.e. factors associated with suicidal outcomes) were also grouped together, under five overarching domains: demographic, psychiatric, psychosocial, neurological/neuropsychological and biological. This was an iterative process, with additional correlates being added to each group throughout the process of data extraction. Finally, studies were grouped by setting type (clinical or community) to explore if the identified suicidality correlates varied across these settings.
Synthesis method
Effect estimates were incompletely reported across studies, limiting the extent to which quantitative synthesis was possible. In addition, studies were highly heterogeneous with respect to setting, study design, participant characteristics, methods of assessing and reporting outcomes and follow-up periods. This diversity limits any meaningful estimation of effects across studies. There were also many gaps in reporting with regard to sample variation, sampling error and statistical significance, further reducing our ability to pool data. For these reasons, meta-analysis was not possible. We have provided a narrative synthesis of findings, structured according to the probable strength of evidence provided by each group of studies, according to study design.
Results
Study selection
Our combined searches identified a total of 4828 records across the three included databases. The Ovid multifile search function was used to automatically de-duplicate this set of records, which removed 1768 duplicates. This de-duplicated set of 3060 records was exported to Covidence, where a second de-duplication of records was automatically conducted, which identified and removed a further 31 duplicates. From this set of 3029 records, 1406 were excluded following title and abstract screening, leaving 1623 records for full-text screening. A further 1547 records were excluded through full-text screening, leaving 76 studies for data extraction. Reasons for exclusion are detailed in the PRISMA diagram (Figure 1). A further five studies were excluded in the data extraction phase as they did not satisfy the inclusion criteria, resulting in a final total of 71 studies included in this review.
PRISMA 2020 flow diagram.
Study characteristics
Of the 71 included studies, 32 were cross-sectional, 24 were prospective cohort studies and 15 were case series. Three case–control studies were also included and were classified as cross-sectional studies for the purposes of this review; aspects relating to interventions were outside the scope of this review and only pre-intervention data were extracted from these three studies. Two prospective studies (Moller et al., 2021; Wunderlich et al., 1998) reported baseline data only and were also classified as being cross-sectional studies. Hart et al. (2001) reported the findings of an RCT, but only included data for those who did not receive the intervention and was classified as a prospective cohort study rather than an RCT. Table 1 presents an overview of the characteristics of all 71 included studies. Note that the sample size and age characteristics for each study only relate to participants meeting our stated inclusion criteria; this could represent a study’s entire cohort, or a subsample.
With respect to study location, the United States was overrepresented; approximately half of the studies (49%; n = 35) were conducted in the United States. The second most common location was Finland (8%; n = 5), followed by Canada, China, Israel, New Zealand and the United Kingdom (three studies each); Hungary, Italy, Norway, South Korea and Switzerland (two studies each); and Australia, Germany, Japan, Poland, Russia and Turkey (one study each). Studies were roughly equally split between clinical (n = 37) and non-clinical settings (n = 31); the latter we termed ‘community settings’. Three studies (4%) (Fan et al., 2019; Johnston et al., 2017; Lippard et al., 2019) did not provide details of the study setting; these were all neuroimaging studies. Of the studies conducted in clinical settings, 17 exclusively involved outpatient settings (Csorba et al., 2010a, 2010b; Fonseka et al., 2015; Gårdvik et al., 2021; Gulec et al., 2010; Janiri et al., 2021; Kutcher et al., 1990; MacPherson et al., 2021; Moller et al., 2021; Rudd et al., 1993; Smith et al., 2005; Spalletta et al., 1996; Tuisku et al., 2006, 2012, 2014; Urrila et al., 2014; Yule et al., 2018), 13 exclusively involved inpatient settings (Barrash et al., 1993; Beautrais et al., 1998; Deykin and Buka, 1994; Gabbay et al., 2009; Gmitrowicz and Kołodziej-Meciejewska, 2002; Hong et al., 2021; Méan et al., 2005; Patten et al., 2003; Righini et al., 2005; Salazar de Pablo et al., 2020; Sher et al., 2007; Shoval et al., 2006; Zhu et al., 2021) and 7 involved both outpatient and inpatient settings (Beglyankin et al., 2019; Gibbons, 2007; Joiner et al., 2009; Koeda et al., 2012; Rudd et al., 1996; Seo et al., 2015; Zhang et al., 2016) (one of the latter also included community participants). Studies conducted in community settings were defined as those which were not explicitly inpatient or outpatient settings, and those that did not explicitly target participants who were receiving either outpatient or inpatient medical or mental health treatment. Community settings included school and university studies, studies conducted in private homes and studies conducted in military and youth justice settings. Psychological autopsy 2 studies of general population samples were also included in the ‘community setting’ category. Table 1 provides a summary of each study’s setting and population.
Participant characteristics varied substantially across studies. Community-based studies (n = 31) included general population samples (Connor and Rueter, 2009; Kasen and Chen, 2020; Kessler and Walters, 1998; Wunderlich et al., 1998), school and university samples (Dinges and Duong-Tran, 1992; Esposito and Clum, 2003; Hart et al., 2001; Kang et al., 2012; Leventhal et al., 2008; Lewinsohn et al., 2001; Miranda et al., 2008; Nrugham et al., 2008; Rohde et al., 2013; Vrshek-Schallhorn et al., 2011), birth cohorts (Fergusson et al., 2007; Fergusson and Woodward, 2002; Hammerton et al., 2015; Nelson et al., 2000),3,4 military personnel 5 (both voluntary enlistments and conscripts) (Phillips et al., 2017; Shelef et al., 2015, 2018), incarcerated young people (Alessi et al., 1984) and general population samples of individuals who died by suicide (Brent et al., 1993; Gagnon et al., 2009; Houston et al., 2001; Marttunen et al., 1991; Ren et al., 2013; Renaud et al., 1999; Rich et al., 1990; Shaffer et al., 1996).6,7 Clinical studies (n = 37) also encompassed a wide variety of participant cohorts, such as young people in specialist treatment programmes (e.g. for drug or alcohol dependence) (Deykin and Buka, 1994; Patten et al., 2003; Yule et al., 2018), young people who had attempted suicide (Beautrais et al., 1998; Méan et al., 2005; Righini et al., 2005) and those receiving outpatient mental health care (Csorba et al., 2010a, 2010b; Fonseka et al., 2015; Gibbons, 2007; Gulec et al., 2010; Kutcher et al., 1990). Data on the mean age of participants within our age range of interest could be extracted from 56 studies (79%); the reported mean age across these studies varied from 15.5 (SD = 1.3) (Miranda et al., 2008) to 24.6 (SD = 0.61) years (Leventhal et al., 2008).
Depression and comorbid diagnoses
Nearly all included studies (85%; n = 60) used versions of the DSM as their chosen diagnostic classification standard. Only eight studies (11%) used versions of the ICD (Beglyankin et al., 2019; Gibbons, 2007; Houston et al., 2001; Koeda et al., 2012; Phillips et al., 2017; Shelef et al., 2015, 2018; Zhu et al., 2021). Two studies (Csorba et al., 2010a, 2010b) did not specify the diagnostic framework they employed but used the Mini International Neuropsychiatric Interview (MINI Plus) as a diagnostic tool, so could have adopted either DSM or ICD diagnostic criteria. Finally, one study (Gmitrowicz and Kołodziej-Meciejewska, 2002) stated that both the DSM-IV and ICD-10 were employed, but did not provide any description of how or why this was done, or any details of the diagnostic tools used.
Most studies (80%; n = 57) used standardised diagnostic tools to assess and diagnose depression. Fourteen studies (20%) derived diagnoses through standard clinical practice but did not provide details on specific diagnostic tools employed (Barrash et al., 1993; Beglyankin et al., 2019; Gibbons, 2007; Gmitrowicz and Kołodziej-Meciejewska, 2002; Houston et al., 2001; Koeda et al., 2012; Marttunen et al., 1991; Patten et al., 2003; Phillips et al., 2017; Rich et al., 1990; Shelef et al., 2015, 2018; Yule et al., 2018; Zhu et al., 2021); these were predominantly studies of patients hospitalised due to psychiatric illness, or military personnel undergoing standardised health screening. Of the standardised diagnostic tools employed, versions of the Schedule for Affective Disorders and Schizophrenia (SADS and K-SADS) were the most popular, being used in 25 studies (35%). Versions of the Structured Clinical Interview for DSM Disorders (SCID) were the next most common, being used in 19 studies (27%).
With respect to specific diagnoses, most studies (68%; n = 48) reported outcomes for participants with major depressive disorders (we combined diagnoses described as major depressive disorder [MDD], major depressive episode [MDE] and major depression [MD] together in this category). Outcomes for participants with bipolar I and II disorders were reported in 23 studies (32%), dysthymic disorders in 18 studies (25%) and adjustment disorder with depressed mood in 5 studies (8%). Thirteen studies (21%) did not specify particular diagnoses, but instead reported broad diagnostic categories such as ‘affective disorders’ (Gagnon et al., 2009; Méan et al., 2005; Righini et al., 2005), ‘mood disorders’ (Shelef et al., 2015; Shoval et al., 2006) or simply ‘depression’ (Dinges and Duong-Tran, 1992; Phillips et al., 2017; Zhang et al., 2016).
Approximately half (44%; n = 31) of the included studies reported data relating to psychiatric comorbidities in those with depression. It was not possible to extract prevalence data for specific comorbid diagnoses from all these studies; information was either not reported or not reported specifically for participants within our age range of interest. Comorbid anxiety disorders were the most frequently reported (n = 28 studies; 39%), followed by substance use disorders (SUDs) (n = 20; 28%), behavioural disorders (n = 12; 17%), eating disorders (n = 11; 15%), neurodevelopmental disorders (n = 8; 11%), psychotic disorders (n = 6; 10%) and somatoform disorders (n = 2; 3%). Note that these findings reflect the frequency with which specific comorbidities were assessed and reported, not the actual prevalence of these psychiatric comorbidities in young people with depression. One-third of studies (n = 21; 30%) reported data on comorbid personality disorders or sub-clinical personality disorder features. Only 18% of studies (n = 13) reported data on NSSI among young people with depression. Terminology relating to NSSI was very inconsistent across studies and included terms such as deliberate self-harm, self-aggression, self-mutilation, self-inflicted injury, self-damaging behaviour, self-injuring and auto-aggression, and acts of apparent attempted suicide where the individual did not want to die.
Suicidality outcomes
Methods of assessing and reporting suicidality varied considerably across studies (see Table 2). The majority of studies (63%; n = 45) reported using at least one standardised assessment tool for suicidality, although some studies employed modified or abbreviated versions of standardised measures. Versions of the SADS and K-SADS were the most commonly used standardised measures, being used in 14 studies (20%). Fourteen studies appeared to assess suicidality through standard clinical practice and did not provide details on specific assessment tools employed (Gagnon et al., 2009; Gibbons, 2007; Gmitrowicz and Kołodziej-Meciejewska, 2002; Houston et al., 2001; Koeda et al., 2012; Marttunen et al., 1991; Méan et al., 2005; Patten et al., 2003; Phillips et al., 2017; Shaffer et al., 1996; Shelef et al., 2015, 2018; Zhang et al., 2016; Zhu et al., 2021), while four studies used non-standardised measures that did not appear to form part of standard clinical practice (Fergusson et al., 2007; Hammerton et al., 2015; Janiri et al., 2021; Righini et al., 2005). Eight studies did not describe the methods used to assess suicidality (Beautrais et al., 1998; Beglyankin et al., 2019; Fergusson and Woodward, 2002; Fonseka et al., 2015; Ren et al., 2013; Renaud et al., 1999; Rich et al., 1990; Yule et al., 2018).
Summary of suicidality findings across all included studies (N = 71) grouped by study design.
NR: not reported; SA: suicide attempts; SD: suicide deaths; SI: suicidal ideation; ?: lack of clarity in source; $: follow-up point/s within our age range of interest; SUD: substance use disorder; DSM: Diagnostic and Statistical Manual of Mental Disorders; GM: grey matter; WM: white matter.
ASI: Adolescent Suicide Interview; BMLS: Beck Medical Lethality Scale; BPSS-P: Bipolar Prodrome Symptom Interview and Scale-Prospective; BSS: Beck Scale for Suicidal Ideation; C-CASA: Columbia Classification Algorithm of Suicide Assessment; CIDI: Composite International Diagnostic Interview; CSHF: Columbia Suicide History Form; CSPS: Childhood Suicide Potential Scale; DIS(C): Diagnostic Interview Schedule (for Children); HDRS: Hamilton Depression Rating Scale; IPDE: International Personality Disorder Examination; LIFE: Longitudinal Interval Follow-up Evaluation; MINI: Mini International Neuropsychiatric Interview; MSSI: Modified Scale for Suicidal Ideation; OSI: Ottawa Self-Injury Inventory; SCID: Structured Clinical Interview for DSM Disorders; SIS: Suicide Intention Scale; SPS: Suicide Probability Scale; SSAGA: Semi-Structured Assessment for the Genetics of Alcoholism; YRBS: Youth Risk Behaviour Survey; YSIS: Youth Suicide Ideation Scale; (K-)SADS: (Kiddie) Schedule for Affective Disorders and Schizophrenia; (-E): Epidemiological version; (-P): Present version; (-PL): Present and Lifetime version.
ADDM: adjustment disorder with depressed mood; BD: bipolar disorder/s; DYS: dysthymia/dysthymic disorder; MD: major depression; MDD: major depressive disorder; MDE: major depressive episode; SP: social phobia.
Reports lifetime prevalence of ‘suicidal behaviour’ (39.8%) which includes an unspecified proportion with history of suicide attempt.
We were able to extract suicidality prevalence data from 54% (n = 38) of the included studies. Prevalence data could not be extracted from the remaining 33 studies as suicidality was either an inclusion criterion (e.g. all subjects were individuals who had died by suicide) or the study did not report suicidality prevalence among participants with depression separately to other participants. Twenty-three studies (32%) provided data on the prevalence of SI, 26 studies (37%) provided prevalence data regarding suicide attempt and only 1 study provided prevalence data on suicide deaths (excluding psychological autopsy studies) (see the ‘Results of individual studies’ section and Table 2 for detailed prevalence findings). Prevalence timeframes varied greatly, ranging from past week to lifetime. Twenty studies (28%) did not clearly state the prevalence timeframe; in many of these cases, we inferred the timeframe based on the assessment tool employed (e.g. Tuisku et al., 2006 did not state an assessment timeframe, but employed the K-SADS-PL, which assesses lifetime prevalence).
Data relating to suicidality severity could only be gleaned from 20 studies (28%). Severity was assessed through a variety of standardised scales, the most common being the Beck Scale for Suicidal Ideation (BSS) (Beck et al., 1979) which was used in four studies (Fan et al., 2019; Gabbay et al., 2009; Johnston et al., 2017; Seo et al., 2015). Suicidality frequency was reported in 15 studies (21%), of which only 7 (Alessi et al., 1984; Hong et al., 2021; Joiner et al., 2009; Rudd et al., 1996; Seo et al., 2015; Shelef et al., 2018; Sher et al., 2007) reported data on the number of suicide attempts among participants with depression.
Risk of bias in studies
A summary of the risk of bias assessment, including the items assessed and consensus ratings for each item, is provided in Appendix 4. While the quality of reporting across studies was highly variable, all studies were included in the review, regardless of the outcome of the critical appraisal process. Only six studies (Deykin and Buka, 1994; Gårdvik et al., 2021; MacPherson et al., 2021; Moller et al., 2021; Tuisku et al., 2006, 2014) satisfied criteria for all eight core critical appraisal checklist items. Over half (58%; n = 41) of the studies satisfied five or more of these core criteria. Many studies did not adequately report basic information such as inclusion criteria, or provide a detailed description of the study’s subjects and setting; only 25 studies (35%) adequately described all these fundamental aspects. Over half (61%; n = 43) of all studies were judged to have measured the primary outcome (suicidality) in a valid and reliable way. There was uncertainty with respect to this aspect in 28 studies (39%) due to the adoption of abbreviated, modified or non-standardised suicidality assessment tools, or a lack of detail in reporting the methods used to assess suicidality. Most studies (80%, n = 57) were judged as having assessed depression in a valid and reliable way, through employing standardised, validated diagnostic tools.
Results of individual studies
Prevalence of suicidality
We grouped suicidality prevalence findings into three categories, as follows:
SI and behaviour not including suicide attempt
Suicide attempt
Suicide death
SI and behaviour (preparatory acts, not including attempt) were grouped together as many studies did not clearly differentiate between SI and suicidal behaviour, or provided vague descriptors for suicidal outcomes which we felt likely encompassed aspects of both ideation and behaviour, such as ‘suicidal’ (Csorba et al., 2010b), ‘suicidal tendency’ (Alessi et al., 1984) and ‘active suicidality’ (Gabbay et al., 2009). Twenty-three studies (32%) provided data on the prevalence of SI and non-attempt-related behaviour (SI) in young people with diagnosed depressive disorders. The lowest reported SI prevalence was found for a birth cohort of young people from New Zealand (Fergusson et al., 2007); of those who experienced five to nine depressive episodes between ages 16 and 21 years, only 12.5% would go on to experience SI between ages 21 and 25 years. 8 The highest reported prevalence was from a cohort of adolescents aged 15–19 years in a residential drug and alcohol treatment programme in the United States; among those diagnosed with depression, 99% (77/78) experienced SI (Deykin and Buka, 1994).
Twenty-six studies (37%) provided prevalence data regarding suicide attempt. Again, these findings varied considerably. The lowest reported prevalence was among US military veterans (aged 18–25 years) with unipolar depressive disorders who were not receiving any anti-depressant treatment (N = 1242); there were 17 individuals (1.36%) who attempted suicide over an approximately 1-year period (Gibbons, 2007). The highest reported prevalence was among a population of incarcerated serious juvenile offenders in the United States; in those with ‘major affective disorders’, 72% (8/11) had made one or more suicide attempts over the past year (Alessi et al., 1984). Prevalence data relating to suicide deaths could only be extracted from a single study, 9 which examined suicide deaths that occurred among US enlisted marines during active-duty military service; among 9247 individuals diagnosed with depression, 16 (0.17%) died by suicide during their period of service (which is usually 4 years in duration) (Phillips et al., 2017).
Correlates of suicidality
Factors associated with suicidality among young people with diagnosed depressive disorders were investigated in 46 studies (65%) and are presented in detail in Table 3. Such associations were not reported in the remaining 25 studies (35%); while many of these studies investigated associations with suicidality for their cohorts of young people, they did not report these relationships for those with depressive disorders specifically. Factors statistically associated with suicidality included depression characteristics (18 studies), comorbid psychiatric or personality disorders (12 studies), psychosocial factors (9 studies), neurological/neuropsychological factors (7 studies) and demographic attributes (5 studies).
Correlates of suicidality in young people with depression according to reported statistical associations (n = 46 studies).
$: cell sizes are too small for analysis; %: calculated based on data presented in source.
ADHD: attention deficit hyperactivity disorder; ASD: autism spectrum disorder; GM: grey matter; NSSI: non-suicidal self-injury; SI: suicidal ideation; SUD: substance use disorder; WM: white matter; BD: bipolar disorder/s; OR: odds ratio; CI: confidence interval.
Tuisku et al. (2012, 2014) ratings are combined as these studies utilise overlapping samples drawn from the same study, ‘The Adolescent Depression Study (ADS)’.
Compared across three BD-spectrum groups; no comparison to unipolar depression.
Borderline significance (p = 0.055, Fisher’s exact test).
Comorbid anxiety was associated with a slightly lower risk of suicide attempt (OR = 0.23, 95% CI = [0.06, 0.90], p = 0.035) but there was no association with SI.
Family support only. Friend support and significant other support were not significant predictors of SI.
Depression characteristics associated with suicidality included depression type (Brent et al., 1993; Kessler and Walters, 1998; Lewinsohn et al., 2001; Nrugham et al., 2008; Smith et al., 2005; Spalletta et al., 1996; Wunderlich et al., 1998; Yule et al., 2018), depression severity (Gabbay et al., 2009; Hong et al., 2021; Moller et al., 2021; Tuisku et al., 2006, 2012, 2014), depression frequency (Fergusson et al., 2007; Seo et al., 2015) and psychomotor features associated with depression (Leventhal et al., 2008). Unipolar depression emerged as having the most evidence for an association with suicidality; seven studies (Brent et al., 1993; Kessler and Walters, 1998; Lewinsohn et al., 2001; Nrugham et al., 2008; Spalletta et al., 1996; Yule et al., 2018; Zhu et al., 2021) reported that unipolar depression was more strongly associated with suicidality compared to bipolar depressive disorders or dysthymia. Conversely, only one study (Smith et al., 2005) reported that bipolar depression was the depression type most strongly associated with suicidality.
The existence of comorbid psychiatric diagnoses was assessed in 31 studies (44%), though only 17 of these investigated comorbidity as a suicidality correlate. Comorbid conditions associated with suicidality included anxiety disorders (Brent et al., 1993; Lippard et al., 2019; Nelson et al., 2000; Rudd et al., 1993; Tuisku et al., 2006), behavioural disorders (Brent et al., 1993), somatoform disorders (Wunderlich et al., 1998), SUDs (Brent et al., 1993; Dinges and Duong-Tran, 1992; Nelson et al., 2000; Sher et al., 2007; Wunderlich et al., 1998) and general psychiatric comorbidity (Rudd et al., 1996; Tuisku et al., 2012; Wunderlich et al., 1998). Twenty-two studies reported data on comorbid personality disorders (or sub-clinical symptoms), but again most of these did not investigate personality disorders as a suicidality risk factor in young people with depression. Only three studies reported such findings; borderline personality-spectrum symptoms (BPSS) (Fonseka et al., 2015) and unstable personality disorder (Barrash et al., 1993) were both reported as being associated with increased risk of suicidality, while Kutcher et al. (1990) failed to find an association between personality disorders and suicide attempt; however, this study was hampered by small sample size.
Psychosocial factors associated with suicidality included alcohol consumption (non-SUD) (Tuisku et al., 2012, 2014), NSSI (Tuisku et al., 2012, 2014), personality traits (extraversion, novelty seeking) (Csorba et al., 2010b; Vrshek-Schallhorn et al., 2011), sleep disruption (Urrila et al., 2014), social support (Esposito and Clum, 2003; Moller et al., 2021; Tuisku et al., 2014) and stressful or negative life events (Dinges and Duong-Tran, 1992; Esposito and Clum, 2003) and temperament (Janiri et al., 2021). Two of these factors, social support and extraversion, were inversely related to suicidality. We investigated several other psychosocial factors which were either found to have no statistically significant association with suicidality (living alone, impulsivity, years of education) or were not reported in the included studies (employment status, sexual orientation).
Neurological characteristics associated with suicidality included both structural and functional changes in prefrontal, subcortical and cerebellar regions (Fan et al., 2019; Hong et al., 2021; Huber et al., 2019; Johnston et al., 2017; Lippard et al., 2019; Zhang et al., 2016). Evidence suggests suicidality is associated with decreased grey matter volume in left prefrontal regions (Fan et al., 2019; Hong et al., 2021; Huber et al., 2019; Lippard et al., 2019), right prefrontal regions and the hippocampus (Fan et al., 2019; Hong et al., 2021; Johnston et al., 2017) and the cerebellum (Johnston et al., 2017). Fan et al. (2019) also reported increased grey matter volume in orbitofrontal cortex (BA47) as a risk factor among those with MDD specifically. Reduced connectivity in left frontotemporal white matter (Fan et al., 2019; Johnston et al., 2017) and certain subcortical regions (Lippard et al., 2019) were also associated with suicidality. One study (Zhang et al., 2016) reported increased connectivity in the left cerebellum and a neighbouring posterior cerebral region (lingual gyrus), and decreased connectivity in a right parietal region (precuneus) as risk factors. Evidence relating to biological characteristics was limited to two studies (Gabbay et al., 2009; Gmitrowicz and Kołodziej-Meciejewska, 2002) which reported associations between suicidality and inflammatory biomarkers.
Results of syntheses
Correlates of suicidality – prospective studies
Outcomes of the synthesis process are presented in Table 3 (grouped by study design) and Table 4 (grouped by setting). Of the 24 prospective studies included in this review, only 12 (50%) reported statistically significant associations with suicidality. The typical follow-up period across theses 12 studies was 1 year, while the maximum period was 8 years (Tuisku et al., 2014). Across these prospective studies, the most commonly reported correlates were sex (female) (Gårdvik et al., 2021; Tuisku et al., 2012), depression type (unipolar) (Lewinsohn et al., 2001; Nrugham et al., 2008), depression severity (Tuisku et al., 2012, 2014), comorbid anxiety disorders (Lippard et al., 2019; Nelson et al., 2000), alcohol consumption (non-SUD) (Tuisku et al., 2012, 2014) and NSSI (Tuisku et al., 2012, 2014). The following correlates were reported to be statistically associated with suicidality in a single prospective study each (details provided in Table 3): age, depression frequency/recurrence, psychomotor features, personality disorders, SUDs, general psychiatric comorbidity, extraversion, sleep disruption, social support and neurological characteristics. With respect to the association of sex and suicidality, these findings were not unequivocal, with five prospective studies reporting no statistical association between female sex and suicidality (Fergusson and Woodward, 2002; Lewinsohn et al., 2001; Rohde et al., 2013; Tuisku et al., 2014; Vrshek-Schallhorn et al., 2011). A smaller number of prospective studies found no statistically significant association between suicidality and age (Tuisku et al., 2012, 2014), depression type (unipolar) (Vrshek-Schallhorn et al., 2011), depression frequency/recurrence (Hart et al., 2001), psychotic disorders, SUDs, impulsivity and years of education (Lippard et al., 2019).
Factors significantly associated with suicidality in young people with depression, by setting type (n = 38 studies).
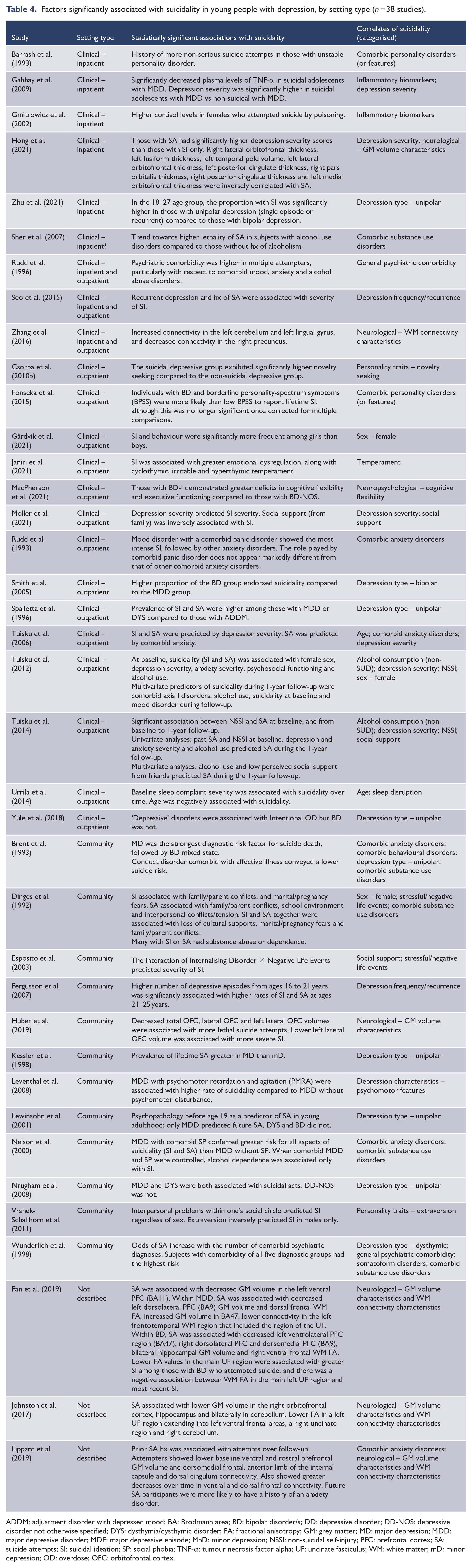
ADDM: adjustment disorder with depressed mood; BA: Brodmann area; BD: bipolar disorder/s; DD: depressive disorder; DD-NOS: depressive disorder not otherwise specified; DYS: dysthymia/dysthymic disorder; FA: fractional anisotropy; GM: grey matter; MD: major depression; MDD: major depressive disorder; MDE: major depressive episode; MnD: minor depression; NSSI: non-suicidal self-injury; PFC: prefrontal cortex; SA: suicide attempts; SI: suicidal ideation; SP: social phobia; TNF-α: tumour necrosis factor alpha; UF: uncinate fasciculus; WM: white matter; mD: minor depression; OD: overdose; OFC: orbitofrontal cortex.
Correlates of suicidality – cross-sectional and case series studies
The majority of evidence in this review derived from cross-sectional (n = 32) and case series (n = 15) studies (henceforth jointly referred to as cross-sectional studies). Of these 47 studies, 26 (55%) reported statistically significant associations with suicidality. The pattern of findings across these cross-sectional studies was broadly similar to that derived from prospective studies, with a few exceptions. The most commonly reported suicidality correlates from cross-sectional studies were depression type (unipolar) (Brent et al., 1993; Kessler and Walters, 1998; Spalletta et al., 1996; Yule et al., 2018; Zhu et al., 2021), depression severity (Gabbay et al., 2009; Hong et al., 2021; Moller et al., 2021; Tuisku et al., 2006), SUDs (Brent et al., 1993; Dinges and Duong-Tran, 1992; Sher et al., 2007; Wunderlich et al., 1998), neurological characteristics (Fan et al., 2019; Hong et al., 2021; Huber et al., 2019; Johnston et al., 2017; Zhang et al., 2016), general psychiatric comorbidity (Rudd et al., 1996; Wunderlich et al., 1998), social support (Esposito and Clum, 2003; Moller et al., 2021), stressful/negative life events (Dinges and Duong-Tran, 1992; Esposito and Clum, 2003) and inflammatory biomarkers (Gabbay et al., 2009; Gmitrowicz and Kołodziej-Meciejewska, 2002). The following correlates were reported to be statistically associated with suicidality in a single cross-sectional study each (details provided in Table 3): age, sex (female), depression type (bipolar), depression type (dysthymic), depression frequency/recurrence, behavioural disorders, personality disorders (or features), somatoform disorders, personality traits (novelty seeking), temperament and cognitive flexibility.
As was seen among the prospective studies, numerous cross-sectional studies (Fan et al., 2019; Gabbay et al., 2009; Hong et al., 2021; Huber et al., 2019; Janiri et al., 2021; Johnston et al., 2017; Moller et al., 2021; Tuisku et al., 2006; Zhang et al., 2016) reported no statistical association between female sex and suicidality, with only one study reported a positive association (Dinges and Duong-Tran, 1992). Overall, there was less concordance of findings across the cross-sectional studies compared to the prospective studies. Most notably, a number of cross-sectional studies reported no statistically significant associations between suicidality and depression severity (Gulec et al., 2010; Seo et al., 2015; Zhang et al., 2016), or SUDs (Fan et al., 2019; Johnston et al., 2017; Rudd et al., 1993). Other correlates with discordant findings across the cross-sectional studies include age, depression type, depression frequency/recurrence, behavioural disorders, personality disorders, somatoform disorders, general psychiatric comorbidity, temperament and inflammatory biomarkers (see Table 3 for details).
Correlates of suicidality by setting type
Of the 38 studies that reported statistically significant associations with suicidality, 23 were conducted in clinical settings (6 inpatient, 14 outpatient, 3 both inpatient and outpatient), 12 involved community settings, while the remaining 3 did not describe the study setting. Table 4 provides a summary of the reported factors that were significantly associated with suicidality, grouped by setting type. Among the 23 studies conducted in clinical settings, depression severity was the most frequently reported correlate (6 studies), followed by depression type (4 studies). Age (higher), alcohol consumption, comorbid anxiety disorders, comorbid personality disorders, inflammatory biomarkers, neurological characteristics, NSSI, sex (female) and social support were reported as statistically significant correlates of suicidality in two clinical studies each. Comorbid SUDs, depression frequency, general psychiatric comorbidity, neuropsychological characteristics, personality traits (novelty seeking), sleep disruption and temperament were reported in one clinically based study each.
A broadly similar pattern of findings was seen among the 12 community-based studies. Here, depression type was the most frequently reported correlate of suicidality (five studies), followed by comorbid SUDs (four studies). Comorbid anxiety disorders and stressful or negative life events were reported as statistically significant correlates in two studies each. Comorbid behavioural disorders, depression frequency and characteristics, general psychiatric comorbidity, neurological characteristics, personality traits (extraversion), sex (female), social support and somatoform disorders were reported as being associated with suicidality in one community-based study each.
Discussion
In this review we have employed rigorous, evidence-based guidelines (Campbell et al., 2020; Moola et al., 2020; Page et al., 2021) to provide a current, comprehensive overview of suicidality correlates among young people with depressive disorders. We identified 26 clinical, psychosocial and biological factors that are associated with suicidality in young people diagnosed with a range of unipolar and bipolar depressive disorders. Depression characteristics (type, severity and recurrence), psychiatric comorbidity and neurological characteristics emerged as having the most evidence for being associated with an increased risk of suicidality. Social support emerged as the clearest protective factor, although it was only reported in three studies. The pattern of evidence was similar across prospective and cross-sectional studies, although the majority of evidence was derived from the latter. There was little to suggest that the identified correlates varied between clinical and non-clinical settings, although our analysis is necessarily limited by which factors authors chose to assess and report. Small differences in the pattern of findings across settings are therefore difficult to interpret. Findings of this review show that there is a wide range of clinical, psychosocial and biological factors associated with suicidal outcomes in young people with depression, supporting the notion that suicide is a complex phenomenon arising from the interplay of multiple contributing factors (De Berardis et al., 2018; Roh et al., 2018).
Unipolar depression appeared to have the most evidence for an increased risk of suicidality, compared to bipolar depressive disorders. The greatly elevated risk of suicide in individuals with bipolar disorders compared to the general population is well documented (Plans et al., 2019), but studies comparing suicide risk between bipolar and unipolar depressive disorders have yielded inconsistent findings (Malhi et al., 2018; Pompili et al., 2013). Both higher and lower rates of suicidality have been reported in those with bipolar vs unipolar depressive disorders, perhaps influenced by factors such as symptom severity, illness duration, age and sex (Holma et al., 2014; Malhi et al., 2018; Zalsman et al., 2006). In light of the inconsistent results presented in the literature, our finding may not be surprising, but there are other aspects that should be taken into consideration in its interpretation. First, nine studies explicitly excluded participants with bipolar disorders, thus reducing the number of comparisons that could be made between unipolar and bipolar disorders in our synthesis. Difficulties in accurately diagnosing bipolar disorders, particularly in young people, are also an important factor (Rabelo-da-Ponte et al., 2020). Bipolar disorders are frequently misdiagnosed as MDD and other unipolar depressive conditions (Bowden, 2001; Phillips and Kupfer, 2013; Zhang et al., 2017). Multiple episodes of depression typically precede the onset of manic or hypomanic symptoms, which may not emerge for many years after the onset of depression (O’Donovan and Alda, 2020). Polarity of the initial presenting episode is typically depression and individuals are more likely to present for treatment when experiencing depression as opposed to mania or hypomania (Berk and Dodd, 2005; Perugi et al., 2000). Over the course of illness, the prevalence of depressive episodes is also typically higher than manic or hypomanic episodes, particularly in individuals with bipolar II disorder (Phillips and Kupfer, 2013). Consequently, there is often a lengthy delay between the onset of the first affective episode and appropriate diagnosis and treatment of bipolar disorders (Baldessarini et al., 2007; Dagani et al., 2017; Goldberg and Ernst, 2002; Lublóy et al., 2020). As a result, there is likely a proportion of participants in the included studies who have been misdiagnosed as having unipolar depression rather than a bipolar depressive disorder, or have latent bipolar disorder that is yet to declare itself, potentially obfuscating the relationship between depression type and suicidality. Only two included studies (Hong et al., 2021; Seo et al., 2015) acknowledge the likelihood of such a misdiagnosis among their participants.
Depression severity and recurrence were positively associated with suicidality. These findings are congruent with a large body of existing literature (Avenevoli et al., 2015; Handley et al., 2018; Hetrick et al., 2012; Serra et al., 2021; Stewart et al., 2019; Xu et al., 2018), though it must be noted that several included studies (Gulec et al., 2010; Hart et al., 2001; Rudd et al., 1996; Seo et al., 2015; Zhang et al., 2016) failed to find statistically associations between these aspects and suicidality. In young people, it is likely that associations between depression severity and suicidality are influenced by psychological factors such as resilience, emotion regulation, and hopelessness (Bilgiç et al., 2017; Bridge et al., 2006; Tamás et al., 2007; Teismann et al., 2018) and psychosocial factors such as social support and negative life events (Esposito and Clum, 2003; Kerr et al., 2006; Siegmann et al., 2018). The interplay of such factors with respect to suicidality in depressed young people warrants further investigation.
Psychiatric comorbidity was also associated with suicidality, particularly comorbid anxiety and SUDs. Anxiety is frequently comorbid with depression in young people and there is a substantial degree of overlap between these two diagnostic categories in terms of characteristics and risk factors (Cummings et al., 2014; Hankin et al., 2016). There is inconsistency in the literature around relationships between depressive disorders, anxiety disorders and suicidality in young people (Cummings et al., 2014; Esposito and Clum, 2002). Whether the additional suicidality risk imposed by comorbid anxiety is due to features of anxiety per se or is due to increased psychiatric illness burden more generally is unclear. There was some evidence to suggest that it is particular symptoms of anxiety, rather than categorical diagnoses of anxiety disorders, which drive observed associations between anxiety and suicidality in young people with depression (Ghaziuddin et al., 2000; Tuisku et al., 2006). Considering the amount of symptomatological overlap and high degree of comorbidity between depression and anxiety, disentangling unique contributions from these diagnoses to suicidal risk may be difficult.
Associations between substance use and suicidality in young people are well documented in the literature (Bridge et al., 2006; Evans et al., 2004; Galaif et al., 2007; Hawton et al., 2012; McManama O’Brien and Berzin, 2012; Wong et al., 2013). This was reflected in our synthesis, which demonstrated that SUDs and alcohol consumption not meeting SUD criteria were associated with suicidality. Depression and substance use frequently co-occur in young people (Kaminer et al., 2007; Lai et al., 2015). Substance use (particularly alcohol use) may be construed as a culturally acceptable form of self-destructive behaviour (Lewinsohn et al., 2001) which can serve as a precursor to more serious self-injury (Nock, 2010). Substance use can develop as method of attempting to cope with psychological distress (the self-medication hypothesis) (Khantzian, 1997); there is evidence supporting a longitudinal association between SI and substance use in young people (Marschall-Lévesque et al., 2017; Rioux et al., 2021). The disinhibitory effects of alcohol and heightened tolerance for pain may also play important facilitatory roles in suicidal behaviour (Bridge et al., 2006; Deykin and Buka, 1994; Esposito and Clum, 2002; Grimmond et al., 2019; Reifman and Windle, 1995) and intoxication (with alcohol or other substances) is found in a high proportion of suicide attempts and suicide deaths among young people (Bohaterewicz et al., 2020; Lahti et al., 2014; Méan et al., 2005; Pelkonen and Marttunen, 2003). Given the relatively high comorbidity of depression and substance use in young people, non-judgmental screening and assessment for substance use could be a useful component of depression treatment approaches (Brown et al., 2016; Winters and Kaminer, 2008). Evidence demonstrates the effectiveness of integrated treatment approaches that target both substance use and psychiatric conditions in young people (Brewer et al., 2017). There is also evidence for the efficacy of combined substance use and depression prevention approaches for young people (Teesson et al., 2020), which is an area that deserves further investigation.
In our synthesis, neuroimaging findings demonstrated that suicidality in bipolar and unipolar depression is associated with both structural and functional changes in ventral prefrontal regions, particularly orbitofrontal cortex, and connections to subcortical regions including the amygdala (Fan et al., 2019; Johnston et al., 2017; Lippard et al., 2019). These neural circuits play a central role in emotion regulation processes and reward-based decision-making (Fettes et al., 2017; Rolls, 2016) and are often reported to be associated with suicidality (Balcioglu and Kose, 2018; Schmaal et al., 2020); however, much of this evidence comes from adult cohorts. Findings included in our synthesis also showed white matter and grey matter abnormalities in the cerebellum (Johnston et al., 2017; Zhang et al., 2016). There is growing evidence that the cerebellum is involved in emotional processing and mood disorders (Adamaszek et al., 2017; Balcioglu and Kose, 2018; Schmaal et al., 2020). Emotion dysregulation is known to be closely associated with affective disorders and suicidality (Cardoso de Almeida and Phillips, 2013; Cha et al., 2018; Klonsky et al., 2018; Phillips and Kupfer, 2013), which is reflected in these neuroimaging findings. Psychotherapeutic interventions that include developing emotional regulation capacity have shown some promise in reducing suicidality in young people, but the evidence for their effectiveness is still somewhat limited (Busby et al., 2020; Calear et al., 2016; Cha et al., 2018; Plans et al., 2019).
The diversity of suicidality risk factors that emerged from this synthesis is perhaps reflective of the diversity inherent in young people with depression. For example, there are 227 possible symptom combinations that can fulfil the DSM-IV-TR and DSM-5 diagnostic criteria for MDD; this rises to 14,528 possible symptom combinations if each component symptom of the six compound criteria is considered separately (Olbert et al., 2014; Zimmerman et al., 2015). Such heterogeneity is evident in clinical samples; for instance, Zimmerman et al. (2015) found that a sample of 1566 individuals with MDD met the diagnostic criteria in 170 different symptom combinations. Similarly, Park et al. (2017) identified 119 different symptom combinations among a sample of 853 individuals with MDD. The most frequent symptom combinations were seen in only around 7% (Park et al., 2017) to 10% (Zimmerman et al., 2015) of patients. A study which disaggregated compound symptoms of MDD found that a sample of 84,103 individuals with MDD met the diagnostic criteria in 1811 unique combinations (Olbert et al., 2014). The resultant possibility is that any population of young people with MDD could be so dissimilar among themselves in symptom profile that any effect of risk or protective factors on a given outcome (in this case, suicidality) could be difficult to determine at the group level. In addition to symptomatological diversity, the high base rate of depression among young people means that this diagnostic cohort is also highly heterogeneous with respect to a host of biopsychosocial factors, including those considered in this review as risk factors for suicidality (Fried and Nesse, 2015; Schubert et al., 2017).
This high degree of within-group heterogeneity is problematic from the perspective of both research and treatment (Jaffee et al., 2002). It does raise the question of how useful it is to consider a diagnosis of depression as a specific risk factor for suicidality in young people. That is, if there is likely to be substantial variability underlying the mechanisms for suicidality (and thus potential treatment targets) from one depressed young person to the next, perhaps an alternative approach to identifying aetiological mechanisms of suicidality is warranted (Cha et al., 2018). A specific symptom approach to assessment has been proposed in the literature, which facilitates a more fine-grained analysis of potential aetiological mechanisms and a transdiagnostic approach to assessment and treatment of mental ill-health (Cha et al., 2018; Cummings et al., 2014; Fried, 2017). Suicidality itself is transdiagnostic (Besch et al., 2020; O’Connor and Portzky, 2018); adoption of a transdiagnostic approach to investigating its aetiology and treatment is warranted.
Perhaps due to the large number of studies included in this review, the extent to which findings could be synthesised was hampered by heterogeneity across studies with respect to study settings, study designs, participant characteristics, follow-up periods and methods of defining, assessing and reporting outcomes. Inconsistent reporting of effect estimates, sample variation, sampling error and statistical significance further limited the extent to which quantitative synthesis was possible. As a result, we have provided a narrative synthesis of findings to suggest where there is evidence of an association of a given correlate with suicidality; however, unlike meta-analysis, this approach provides no analysis of the magnitude of such effects.
Limitations of the evidence included in this review have been mentioned but some aspects deserve further critique. The lack of consistency across studies with respect to definitions and methods of assessing suicidality outcomes is perhaps the most problematic. In part, this is due to changes over time in how suicidality has been conceptualised and described in the literature. Nevertheless, there is a clear need for standardised ways of defining, describing and assessing suicidality, to better facilitate comparisons across studies, settings and time (Batterham et al., 2015). Recent systematic reviews of both suicidality nomenclature and classification systems highlight a lack of consensus around definitions and terms used to describe SI and behaviour, pointing to the need for international collaboration in the development of a standardised, validated classification system (Goodfellow et al., 2018, 2020).
Another limitation of this review is the lack of consistency in suicidality correlates that were investigated and reported in the literature. The result is some notable gaps where important correlates were not captured in our synthesis. Naturally, the coverage of correlates is highly dependent on what authors chose to report and the list of correlates presented in our synthesis is not exhaustive. For instance, we included sexual orientation as a grouping in the synthesis process, as previous reviews of population-based studies (Bridge et al., 2006; Cha et al., 2018; Evans et al., 2004) have identified non-heterosexual orientation as a risk factor for suicidality among non-clinical samples of young people. Nevertheless, none of the included studies in our review investigated associations between sexual orientation and suicidality outcomes in young people diagnosed with depression. Given the well-established elevated risk of suicidality among non-heterosexual young people more broadly (Miranda-Mendizabal et al., 2017; Rimes et al., 2019), this suggests a gap in the evidence-base with respect to suicidality and sexual orientation in young people with depression that deserves investigation. Similarly, none of the included studies investigated associations between autism spectrum disorder (ASD) and suicidality in young people with depression. There is a small but growing body of evidence showing that young people with ASD are at increased risk of suicidal outcomes (Chen et al., 2017; Howe et al., 2020) and that ASD is possibly associated with greater depression symptom severity and functional impairment (Masi et al., 2020; Schwartzman and Corbett, 2020). There is a clear need for further investigation of the interrelationships between ASD, depression and suicidality in young people.
There were some limitations inherent in the methodology employed for this review. The age range of 15–25 years is not commonly employed in the mental health literature and resulted in exclusion of many otherwise relevant studies. For instance, many studies employed the age range 13–18 years; if participants in the range 15–18 years were not presented separately in these studies, they were excluded from this review. Similarly, for studies investigating adults aged 18+ years, if participants in the range 18–25 years were not presented separately, these studies were also excluded. Another limitation is that we did not consider history of suicidality as a risk factor for later suicidality, for the following reasons. A large proportion of the included studies only assessed lifetime prevalence of suicidality, meaning that temporal relationships of suicidality could not be assessed. In other studies, the assessment timeframe was often unclear; thus, interpretation of such temporal relationships was not possible. Therefore, all suicidality data were considered as outcomes, rather than risk factors. This review was limited to sources published in English, introducing a potential source of bias which could unduly influence the validity of our conclusions (Jackson and Kuriyama, 2019). Whether the findings of this review are generalisable to a broader range of non-English-speaking settings certainly deserves further investigation.
The findings of this review suggest that suicidality in young people with diagnosed depressive disorders is associated with numerous clinical, psychosocial and biological factors. Findings suggest that it is features of psychiatric illness that have the most evidence for being associated with suicidality. Considering the high degree of heterogeneity within the diagnostic category of ‘depression’, shared symptomatology between depression and other psychiatric diagnoses and the transdiagnostic nature of suicidality, this suggests that an alternative approach to investigating potential aetiological mechanisms of suicidality is warranted. Perhaps future research comprising a transdiagnostic meta-analysis of specific symptoms, or symptom networks, would help to further our understanding of suicidality among young people experiencing mental illness.
Footnotes
Appendix 1
Appendix 2
Appendix 3
Appendix 4
Risk of bias assessment consensus ratings for all included studies (N = 71).
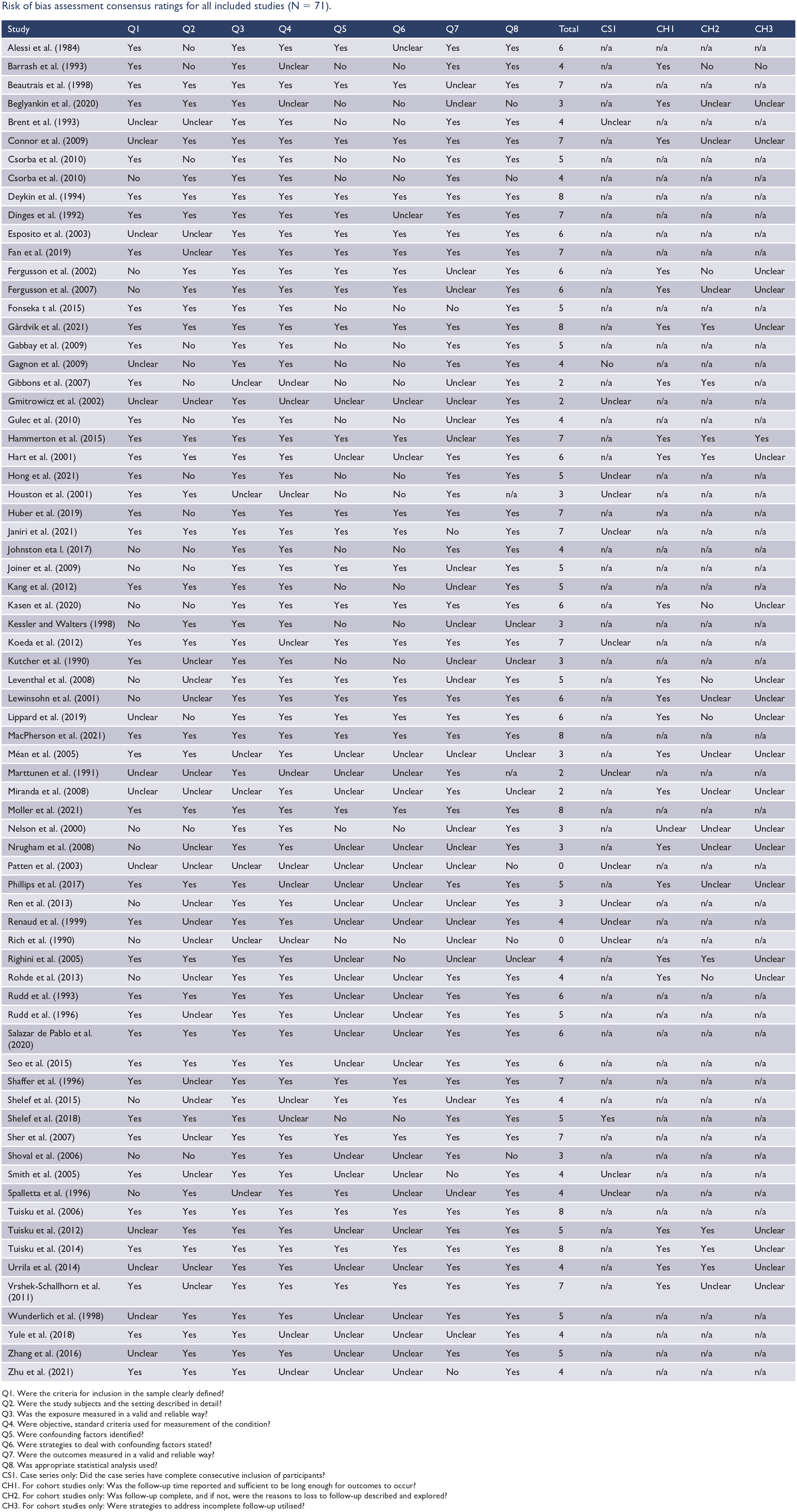
| Study | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Total | CS1 | CH1 | CH2 | CH3 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alessi et al. (1984) | Yes | No | Yes | Yes | Yes | Unclear | Yes | Yes | 6 | n/a | n/a | n/a | n/a |
| Barrash et al. (1993) | Yes | No | Yes | Unclear | No | No | Yes | Yes | 4 | n/a | Yes | No | No |
| Beautrais et al. (1998) | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 7 | n/a | n/a | n/a | n/a |
| Beglyankin et al. (2020) | Yes | Yes | Yes | Unclear | No | No | Unclear | No | 3 | n/a | Yes | Unclear | Unclear |
| Brent et al. (1993) | Unclear | Unclear | Yes | Yes | No | No | Yes | Yes | 4 | Unclear | n/a | n/a | n/a |
| Connor et al. (2009) | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 7 | n/a | Yes | Unclear | Unclear |
| Csorba et al. (2010) | Yes | No | Yes | Yes | No | No | Yes | Yes | 5 | n/a | n/a | n/a | n/a |
| Csorba et al. (2010) | No | Yes | Yes | Yes | No | No | Yes | No | 4 | n/a | n/a | n/a | n/a |
| Deykin et al. (1994) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 | n/a | n/a | n/a | n/a |
| Dinges et al. (1992) | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | 7 | n/a | n/a | n/a | n/a |
| Esposito et al. (2003) | Unclear | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | 6 | n/a | n/a | n/a | n/a |
| Fan et al. (2019) | Yes | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | 7 | n/a | n/a | n/a | n/a |
| Fergusson et al. (2002) | No | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 6 | n/a | Yes | No | Unclear |
| Fergusson et al. (2007) | No | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 6 | n/a | Yes | Unclear | Unclear |
| Fonseka t al. (2015) | Yes | Yes | Yes | Yes | No | No | No | Yes | 5 | n/a | n/a | n/a | n/a |
| Gårdvik et al. (2021) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 | n/a | Yes | Yes | Unclear |
| Gabbay et al. (2009) | Yes | No | Yes | Yes | No | No | Yes | Yes | 5 | n/a | n/a | n/a | n/a |
| Gagnon et al. (2009) | Unclear | No | Yes | Yes | No | No | Yes | Yes | 4 | No | n/a | n/a | n/a |
| Gibbons et al. (2007) | Yes | No | Unclear | Unclear | No | No | Unclear | Yes | 2 | n/a | Yes | Yes | n/a |
| Gmitrowicz et al. (2002) | Unclear | Unclear | Yes | Unclear | Unclear | Unclear | Unclear | Yes | 2 | Unclear | n/a | n/a | n/a |
| Gulec et al. (2010) | Yes | No | Yes | Yes | No | No | Unclear | Yes | 4 | n/a | n/a | n/a | n/a |
| Hammerton et al. (2015) | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 7 | n/a | Yes | Yes | Yes |
| Hart et al. (2001) | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | 6 | n/a | Yes | Yes | Unclear |
| Hong et al. (2021) | Yes | No | Yes | Yes | No | No | Yes | Yes | 5 | Unclear | n/a | n/a | n/a |
| Houston et al. (2001) | Yes | Yes | Unclear | Unclear | No | No | Yes | n/a | 3 | Unclear | n/a | n/a | n/a |
| Huber et al. (2019) | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | 7 | n/a | n/a | n/a | n/a |
| Janiri et al. (2021) | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | 7 | Unclear | n/a | n/a | n/a |
| Johnston eta l. (2017) | No | No | Yes | Yes | No | No | Yes | Yes | 4 | n/a | n/a | n/a | n/a |
| Joiner et al. (2009) | No | No | Yes | Yes | Yes | Yes | Unclear | Yes | 5 | n/a | n/a | n/a | n/a |
| Kang et al. (2012) | Yes | Yes | Yes | Yes | No | No | Unclear | Yes | 5 | n/a | n/a | n/a | n/a |
| Kasen et al. (2020) | No | No | Yes | Yes | Yes | Yes | Yes | Yes | 6 | n/a | Yes | No | Unclear |
| Kessler and Walters (1998) | No | Yes | Yes | Yes | No | No | Unclear | Unclear | 3 | n/a | n/a | n/a | n/a |
| Koeda et al. (2012) | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | 7 | Unclear | n/a | n/a | n/a |
| Kutcher et al. (1990) | Yes | Unclear | Yes | Yes | No | No | Unclear | Unclear | 3 | n/a | n/a | n/a | n/a |
| Leventhal et al. (2008) | No | Unclear | Yes | Yes | Yes | Yes | Unclear | Yes | 5 | n/a | Yes | No | Unclear |
| Lewinsohn et al. (2001) | No | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | 6 | n/a | Yes | Unclear | Unclear |
| Lippard et al. (2019) | Unclear | No | Yes | Yes | Yes | Yes | Yes | Yes | 6 | n/a | Yes | No | Unclear |
| MacPherson et al. (2021) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 | n/a | n/a | n/a | n/a |
| Méan et al. (2005) | Yes | Yes | Unclear | Yes | Unclear | Unclear | Unclear | Unclear | 3 | n/a | Yes | Unclear | Unclear |
| Marttunen et al. (1991) | Unclear | Unclear | Yes | Unclear | Unclear | Unclear | Yes | n/a | 2 | Unclear | n/a | n/a | n/a |
| Miranda et al. (2008) | Unclear | Unclear | Unclear | Yes | Unclear | Unclear | Yes | Unclear | 2 | n/a | Yes | Unclear | Unclear |
| Moller et al. (2021) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 | n/a | n/a | n/a | n/a |
| Nelson et al. (2000) | No | No | Yes | Yes | No | No | Unclear | Yes | 3 | n/a | Unclear | Unclear | Unclear |
| Nrugham et al. (2008) | No | Unclear | Yes | Yes | Unclear | Unclear | Unclear | Yes | 3 | n/a | Yes | Unclear | Unclear |
| Patten et al. (2003) | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | No | 0 | Unclear | n/a | n/a | n/a |
| Phillips et al. (2017) | Yes | Yes | Yes | Unclear | Unclear | Unclear | Yes | Yes | 5 | n/a | Yes | Unclear | Unclear |
| Ren et al. (2013) | No | Unclear | Yes | Yes | Unclear | Unclear | Unclear | Yes | 3 | Unclear | n/a | n/a | n/a |
| Renaud et al. (1999) | Yes | Unclear | Yes | Yes | Unclear | Unclear | Unclear | Yes | 4 | Unclear | n/a | n/a | n/a |
| Rich et al. (1990) | No | Unclear | Unclear | Unclear | No | No | Unclear | No | 0 | Unclear | n/a | n/a | n/a |
| Righini et al. (2005) | Yes | Yes | Yes | Yes | Unclear | No | Unclear | Unclear | 4 | n/a | Yes | Yes | Unclear |
| Rohde et al. (2013) | No | Unclear | Yes | Yes | Unclear | Unclear | Yes | Yes | 4 | n/a | Yes | No | Unclear |
| Rudd et al. (1993) | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | 6 | n/a | n/a | n/a | n/a |
| Rudd et al. (1996) | Yes | Unclear | Yes | Yes | Unclear | Unclear | Yes | Yes | 5 | n/a | n/a | n/a | n/a |
| Salazar de Pablo et al. (2020) | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | 6 | n/a | n/a | n/a | n/a |
| Seo et al. (2015) | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | 6 | n/a | n/a | n/a | n/a |
| Shaffer et al. (1996) | Yes | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | 7 | n/a | n/a | n/a | n/a |
| Shelef et al. (2015) | No | Unclear | Yes | Unclear | Yes | Yes | Unclear | Yes | 4 | n/a | n/a | n/a | n/a |
| Shelef et al. (2018) | Yes | Yes | Yes | Unclear | No | No | Yes | Yes | 5 | Yes | n/a | n/a | n/a |
| Sher et al. (2007) | Yes | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | 7 | n/a | n/a | n/a | n/a |
| Shoval et al. (2006) | No | No | Yes | Yes | Unclear | Unclear | Yes | No | 3 | n/a | n/a | n/a | n/a |
| Smith et al. (2005) | Yes | Unclear | Yes | Yes | Unclear | Unclear | No | Yes | 4 | Unclear | n/a | n/a | n/a |
| Spalletta et al. (1996) | No | Yes | Unclear | Yes | Yes | Unclear | Unclear | Yes | 4 | Unclear | n/a | n/a | n/a |
| Tuisku et al. (2006) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 | n/a | n/a | n/a | n/a |
| Tuisku et al. (2012) | Unclear | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | 5 | n/a | Yes | Yes | Unclear |
| Tuisku et al. (2014) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8 | n/a | Yes | Yes | Unclear |
| Urrila et al. (2014) | Unclear | Unclear | Yes | Yes | Unclear | Unclear | Yes | Yes | 4 | n/a | Yes | Yes | Unclear |
| Vrshek-Schallhorn et al. (2011) | Yes | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | 7 | n/a | Yes | Unclear | Unclear |
| Wunderlich et al. (1998) | Unclear | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | 5 | n/a | n/a | n/a | n/a |
| Yule et al. (2018) | Yes | Yes | Yes | Unclear | Unclear | Unclear | Unclear | Yes | 4 | n/a | n/a | n/a | n/a |
| Zhang et al. (2016) | Unclear | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | 5 | n/a | n/a | n/a | n/a |
| Zhu et al. (2021) | Yes | Yes | Yes | Unclear | Unclear | Unclear | No | Yes | 4 | n/a | n/a | n/a | n/a |
Q1. Were the criteria for inclusion in the sample clearly defined?
Q2. Were the study subjects and the setting described in detail?
Q3. Was the exposure measured in a valid and reliable way?
Q4. Were objective, standard criteria used for measurement of the condition?
Q5. Were confounding factors identified?
Q6. Were strategies to deal with confounding factors stated?
Q7. Were the outcomes measured in a valid and reliable way?
Q8. Was appropriate statistical analysis used?
CS1. Case series only: Did the case series have complete consecutive inclusion of participants?
CH1. For cohort studies only: Was the follow-up time reported and sufficient to be long enough for outcomes to occur?
CH2. For cohort studies only: Was follow-up complete, and if not, were the reasons to loss to follow-up described and explored?
CH3. For cohort studies only: Were strategies to address incomplete follow-up utilised?
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by a Higher Degree Research Scholarship awarded to the lead author (CM) by Suicide Prevention Australia through the National Suicide Prevention Research Fund. The funding body had no role in the study design, data collection, data analysis, data interpretation or writing of this report. This study did not receive any other specific grant from funding agencies in the public, commercial or not-for-profit sectors.