
Abstract
Objective:
Understanding the impact of lifestyle on mental illness symptoms is important for informing psycho-education and developing interventions which target mental and physical comorbidities. Obsessive-compulsive and related disorders can have a significant impact on health-related quality of life and physical health. However, our understanding of the impact of lifestyle on obsessive-compulsive symptoms and broader compulsive and impulsive problematic repetitive behaviours is limited.
Aims:
We investigated whether lifestyle factors predicted change in obsessive-compulsive symptoms and problematic repetitive behaviours in a general population sample over a 3-month period.
Methods:
Eight hundred thirty-five participants completed an online questionnaire battery assessing lifestyle and mental health. Of these, 538 participants completed the same battery 3 months later. We conducted negative binomial regressions to analyse the association of lifestyle factors at baseline with future (1) obsessive-compulsive symptoms, (2) compulsive problematic repetitive behaviours and (3) impulsive problematic repetitive behaviours, adjusting for baseline obsessive-compulsive symptoms and problematic repetitive behaviours.
Results:
Lower vegetable (p = 0.020) and oily fish (p = 0.040) intake and lower moderate intensity physical activity (p = 0.008) predicted higher obsessive-compulsive symptoms at follow-up. Higher intake of high-fat foods (p < 0.001) predicted higher compulsive problematic repetitive behaviours at follow-up. No lifestyle factors significantly predicted impulsive problematic repetitive behaviours at follow-up.
Conclusion:
Our results speak to the potential importance of lifestyle quality screening, education and lifestyle interventions (e.g. an anti-inflammatory diet) for individuals experiencing compulsivity-related behaviours and/or symptoms. Further research into potential mechanisms of action will allow for more targeted approaches to lifestyle interventions for transdiagnostic compulsive behaviours.
Introduction
The concept of lifestyle and related interventions has traditionally been considered within a medical framework, due to the association between lifestyle and chronic disease outcomes, such as future cardiac events (Fontenelle et al., 2018). Yet, the impact of lifestyle on mental illness symptoms is a growing area of interest. Lifestyle factors involved in mental health models include diet quality, sleep quality, physical activity, social connection and stress management (Firth et al., 2019a, 2019b, 2020). This research is now informing an evidence-based and diversified approach to patient education, prevention and treatment through alterations to lifestyle, or more formally, through ‘lifestyle psychiatry’ (Noordsy, 2019). Indeed, the most recent clinical practice guidelines from the Royal Australian New Zealand College of Psychiatry have, for the first time, placed lifestyle as a core element of treatment for mood disorders alongside evidence-based psychological therapies (Malhi et al., 2021).
When used alongside existing evidence-based therapies, lifestyle interventions have been utilised for the prevention and treatment of depression and anxiety disorders (Firth et al., 2020), as well as the symptom management of conditions known to be more pervasive and typically difficult to treat including bipolar disorder (Sylvia et al., 2011), schizophrenia and psychosis (Fernández-Abascal et al., 2021). While there is now robust evidence that lifestyle interventions can provide symptom relief across a range of affective mental health issues, the same cannot be said for the prevention and treatment of obsessive-compulsive and related disorders (OCRDs) and other problematic repetitive behaviours (PRBs).
OCRDs are distressing and debilitating psychiatric conditions characterised by persistent preoccupations (e.g. ‘obsessions’) causing anxiety and/or distress and are often accompanied by repetitive (‘compulsive’) behaviours in attempts to minimise distress (American Psychiatric Association, 2013). In addition to obsessive-compulsive disorder (OCD), OCRDs include body dysmorphic disorder (BDD), hoarding disorder (HD), trichotillomania (‘hair-pulling disorder’; TTM) and excoriation disorder (‘skin-picking disorder’; SPD). Considerable comorbidity exists within OCRDs (Fontenelle et al., 2005; Hollander et al., 2008) and other PRBs characterised by impulsive (e.g. substance use, trichotillomania and physical aggression) and compulsive behaviours (e.g. grooming, shopping, hoarding or collecting) (Cuzen et al., 2014; Guo et al., 2017). Given comorbidity, overlapping neurocircuitry across OCRDs (Fineberg et al., 2017) and evidence of reactivity to lifestyle factors (Brierley et al., 2021a), it may be the case that there are similar lifestyle factors associated with obsessive-compulsive symptoms (OCS) and other PRBs.
The poorer physical health and multi-morbidity experienced by many individuals with an OCRD underscores the importance of this research area. People living with OCRDs are known to have poorer physical health including metabolic and cardiovascular complications (Isomura et al., 2018; Nutley et al., 2021), lower quality of life (Singh et al., 2016; Stein et al., 2016; Tolin et al., 2019) and reduced life expectancy (Meier et al., 2016). These factors may indicate engagement in unhealthy lifestyle activities. Understanding lifestyle behaviours in this population will help to inform lifestyle interventions which may improve both physical and mental well-being.
While there are some empirical indications of a link between lifestyle behaviours and the presence and severity of OCRDs, these are largely based on cross-sectional analyses. The distinct gut microbial profiles between individuals with OCD and people without mental illness could be a reflection of poor dietary patterns (Turna et al., 2020). Moreover, individuals with both OCD (Sallet et al., 2010) and HD (Raines et al., 2015) have reported greater binge eating behaviours, which is likely indicative of poorer diet and higher intake of calorie-rich foods. There is also a significant overlap between OCS and restrictive-type disordered eating psychopathology. It is possible that a resulting dietary pattern which is low in nutrient variation may influence OCS and PRBs through gut microbiome dysfunction (Di Lodovico et al., 2021).
Strong links between greater physical exercise and improved mental health indicators in large general population samples provides the impetus for further exploration into its effect on OCS and PRBs. For instance, the evidence base for exercise as both a preventive and treatment strategy for depression and anxiety is extensive (Schuch et al., 2018; Stubbs et al., 2017). Yet, cross-sectional studies have not supported a link between OCS/PRBs and exercise to date (Freedman and Richter, 2021). One single-arm exercise intervention utilising moderate intensity physical exercise showed acute but significant decreases in OCD symptoms (for a review, see Brierley et al., 2021b). Further research into the relationship between exercise with OCS and PRBs, including in the general population, is required.
A somewhat greater body of knowledge exists when considering sleep and circadian disruptions and OCS. There is evidence of positive relationships between sleep disturbance with OCS and hoarding (Cox et al., 2019). Links between sleep with SPD and TTM have previously been explained by psychological distress markers (Cox et al., 2019), and thus, accounting for distress in future analyses is important to continue to understand this relationship. What remains to be seen is whether other lifestyle factors may impact OCS and PRBs over and above the impact that sleep and psychological distress have. Longitudinal and intervention studies are required in order to investigate the potential causative effect of lifestyle on OCS and PRBs, to hypothesise on mechanistic relationships and to identify the best possible targets for intervention.
A further lifestyle factor pertinent to mental health is social connection. Individuals with clinical OCD have reported perceived lower social supports than non-psychiatric controls (Subramaniam et al., 2020). Lower social support leads to greater psychological distress (Holahan and Moos, 1981) which can serve to worsen OCS and PRBs. Assessment of social support in the current study may shed light on the existence of a relationship between OCS and PRBs in the general population and when controlling for psychological distress.
There are several reasons why it is important to assess OCS and PRBs across the community. First, compulsive behaviours are common and occur in the general as well as the clinical populations (Guo et al., 2017); indeed, the prevalence of OCS symptomatology in the population is estimated at approximately 13–21% (Adam et al., 2012). Subclinical levels of OCS (i.e. the presence of significant symptomatology that does not meet a diagnostic threshold) can impair function and cause distress (de Bruijn et al., 2010).
Teasing apart the role of different lifestyle factors in OCS and PRBs is important in order to identify those factors most pertinent to symptom severity change. This then allows for the provision of evidence-based lifestyle education and health behaviour change support, and informs lifestyle interventions. In the current 3-month longitudinal study, we investigated the association between four baseline lifestyle factors (diet quality, sleep quality, physical activity and social support) in the general population and the severity of (1) OCS, (2) compulsive PRBs and (3) impulsive PRBs. We aimed to determine whether baseline lifestyle factors predicted higher levels of these outcomes at follow-up.
Methods
We conducted an online longitudinal study of adults in a general population sample with assessments made at two timepoints over a 3-month period. At baseline and follow-up, participants provided demographic information including their age and gender, and completed a series of questionnaires related to psychological distress, OCS, PRBs and lifestyle. A 3-month time interval allowed us to monitor changes in OCS and PRBs while being short enough to manage uncontrolled variables, such as significant life events, which may have confounded the impact of lifestyle on the study outcomes.
Ethics
We conducted the current study in accordance with the Declaration of Helsinki. The Monash University Human Research Ethics Committee approved the study.
Participants
We have previously discussed the baseline sample for the current study (Albertella et al., 2021). We recruited 992 participants from May to July 2020 primarily through Prolific (n = 698), an online crowdsourcing platform (Palan and Schitter, 2018). We used the Custom Pre-screening function to specifically enrol participants residing in Australia. The remaining participants (n = 294) were recruited through social media advertisements. Participants recruited through Prolific received reimbursement of £7.50 per hour. Participants completing the questionnaire through other means were offered entry into a draw to win one of 50 AU$100 vouchers. Three months later (July–September 2020), we invited participants who completed the baseline questionnaire to participate in a second questionnaire. Participants again received reimbursement of £7.50 per hour.
Measures
Obsessive-compulsive experiences
Obsessive-Compulsive Inventory–Revised
The Obsessive-Compulsive Inventory–Revised (OCI-R) is an 18-item scale assessing OC-related symptoms and experiences. Participants endorse how distressed or bothered they have been by particular experiences over the previous month on a 5-point Likert-type scale (Foa et al., 2002). We referred to the total OCI-R scores from the first and second timepoints in analyses, whereby higher scores across a 0–72 range indicate greater OCS.
Problematic repetitive behaviours
Impulsive-Compulsive Behaviours Checklist
The Impulsive-Compulsive Behaviours Checklist (ICBC) is a 33-item list relating to PRBs with underlying links to impulsivity and compulsivity (Guo et al., 2017). In the current study, we referred to the compulsive behaviours (ICBC-C) and impulsive behaviours (ICBC-I) subscales. These assess engagement in behaviours specifically linked with compulsivity across 18 items, and impulsivity across a separate 15 items, respectively. On a 4-point Likert-type scale, participants rated whether they and/or others believe they have experienced problems with listed behaviours. On each subscale, higher scores indicate more problems associated with the respective behaviours. At the baseline survey, participants were asked to rate this question considering the past 12 months, while at follow-up participants were asked this in relation to the previous 3 months.
Lifestyle factors
Short Form Food Frequency Questionnaire
The Short Form Food Frequency Questionnaire (SF-FFQ) measures diet quality based on reported food and drink intake over a typical week in the past month (Cleghorn et al., 2016). Responses are given on a 6- to 8-point Likert-type scale, depending on the item. We adapted the measure and employed language more appropriate to use in Australia. For the current study, we referred to baseline diet quality subscale scores including fruit, vegetable, fat (relating to intake of high-fat foods), oily fish and non-milk extrinsic sugars (NMES; also known as ‘added’ or ‘free’ sugars) intake. Fat and sugar intake scores are reverse scored and therefore across all scales, greater scores (ranging 1–3) indicate a healthier diet.
Pittsburgh Sleep Quality Index
The Pittsburgh Sleep Quality Index (PSQI) is a widely used measure of sleep quality considering several domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of medication and daytime dysfunction (Buysse et al., 1989). Scoring is based on a 4-point Likert-type scale and total scores range from 0 to 42 with higher scores indicating poorer sleep quality. We referred to the baseline PSQI total score in analyses.
International Physical Activity Questionnaire (adapted)
The International Physical Activity Questionnaire (IPAQ) is a brief measure of physical activity based on participant recall from the 7 days prior (Craig et al., 2003). Participants are asked to provide the number of days they engaged in vigorous intensity physical activity, moderate intensity physical activity and walking, with examples of each of these provided. In the original IPAQ, participants are asked to record how long they spent doing each of these activities, with reference to one of the days in the past 7 days. We made additions to the IPAQ whereby for each day that participants reported engaging in an activity, they were asked to record an estimate of the time spent undertaking physical activity, rather than considering only one of these days as per the original measure. We converted participant responses in minutes to metabolic equivalent of task (MET) minutes and referred to the baseline MET minutes for vigorous and moderate intensity activity.
Campaign to End Loneliness Measurement Tool (CTEL)
The Campaign to End Loneliness Measurement Tool (CTEL) is a three-item measure of loneliness/social support. We referred to the baseline total scores, whereby higher scores (ranging 0–12) indicate greater loneliness (and lower social support).
Psychological distress
K10
The K10 is a 10-item measure of psychological distress over the past month (Kessler et al., 2002). Participants are asked to rate their level of distress (e.g. ‘About how often did you feel hopeless’) on a 5-point Likert-type scale ranging from 1 to 5. The baseline K10 total score (ranging 10–50) was the measure of interest for our study.
COVID-19 events
COROTRAS
We used an abbreviated eight-item checklist of the COROTRAS, a checklist of potentially stressful COVID-19-related events (Fontenelle et al., 2021). Participants were asked to endorse whether or not they had experienced any of these events. ‘Yes’ responses were rated with a score of 1 and totalled across the checklist.
Data analysis
We performed statistical analyses using SPSS Version 27. We only included participants for whom all relevant baseline data was completed and managed missing data from timepoint two using multiple imputations. Multiple imputations reduce bias by increasing data precision, even when the data is not missing at random (Sterne et al., 2009). We imputed 20 datasets using the following baseline variables: OCI-R, ICBC subscales, K10, COROTRAS, age, gender, SF-FFQ subscales, IPAQ vigorous and moderate MET minutes scores, PSQI and CTEL.
We obtained descriptive statistics for the sample including age and gender. To address our research questions, we entered the variables of interest into three negative binomial regressions. In the first model, we entered the OCI-R at timepoint two (OCI-R2) as the outcome variable and the baseline lifestyle variables (SF-FFQ, PSQI, IPAQ and CTEL), K10, OCI-R (OCI-R1), COROTRAS, age and gender as predictor variables. In the next model, we entered the ICBC-C at timepoint two (ICBC-C2) as the outcome variable and the baseline lifestyle variables, K10, ICBC-C (ICBC-C1), COROTRAS, age and gender as predictor variables. In the final model, we entered the ICBC-I at timepoint two (ICBC-I2) as the outcome variable and the baseline lifestyle variables, K10, ICBC-I (ICBC-I1), COROTRAS, age and gender as predictor variables. All negative binomial regressions were run using imputed data analyses (as presented in the ‘Results’ section) as well as using complete case analyses (please see supplementary material).
We adopted an error rate of p < 0.05 to determine significance. No variables showed multicollinearity as measured by the variance inflation factor exceeding 5. We determined effect sizes using the unstandardised coefficient beta.
Results
Eight hundred and thirty-six participants completed the baseline questionnaire, and 538 participants completed the second timepoint questionnaire (35% attrition). Following the removal of missing baseline data, we included data of 836 participants in statistical analyses. Please refer to Table 1 for participant characteristics. On average, participants completed the follow-up questionnaire 92.32 days (SD = 6.93) following the baseline questionnaire.
Participant characteristics.
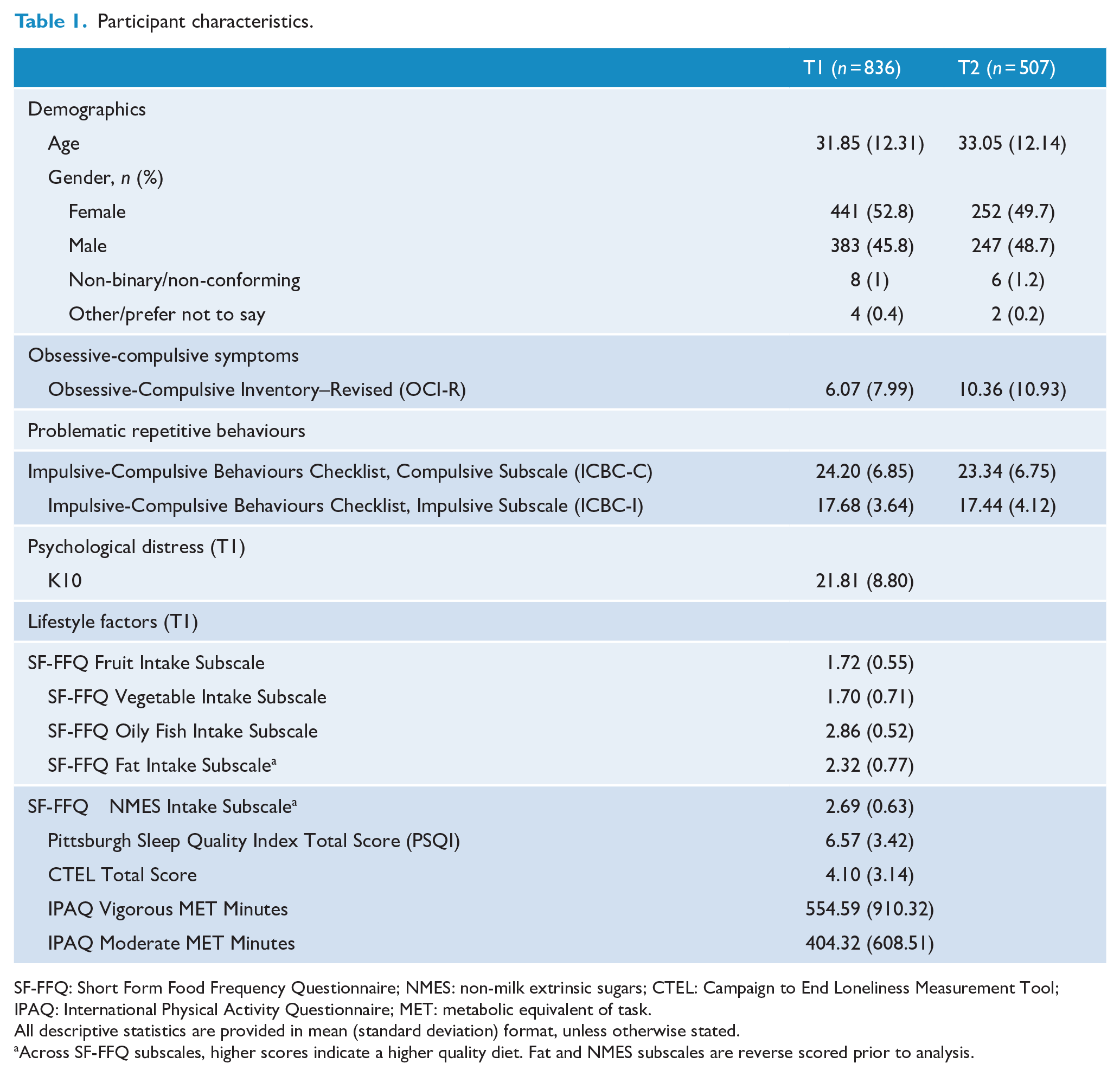
SF-FFQ: Short Form Food Frequency Questionnaire; NMES: non-milk extrinsic sugars; CTEL: Campaign to End Loneliness Measurement Tool; IPAQ: International Physical Activity Questionnaire; MET: metabolic equivalent of task.
All descriptive statistics are provided in mean (standard deviation) format, unless otherwise stated.
Across SF-FFQ subscales, higher scores indicate a higher quality diet. Fat and NMES subscales are reverse scored prior to analysis.
Predictors of OCS
As seen in Table 2, negative binomial regression analyses showed greater OCS at follow-up to be significantly predicted by lifestyle factors of lower vegetable intake (B = −0.118, p = 0.020), lower intake of oily fish (B = −0.101, p = 0.040) and lower moderate intensity physical activity (B = −0.001, p = 0.021) at baseline. Of the covariates, greater OCS (B = 0.051, p < 0.001) and psychological distress (B = 0.013, p = 0.007) at baseline predicted higher OCS at follow-up. Complete case analysis is provided in the supplementary Table 1.
Lifestyle predictors of OCS (OCI-R2).
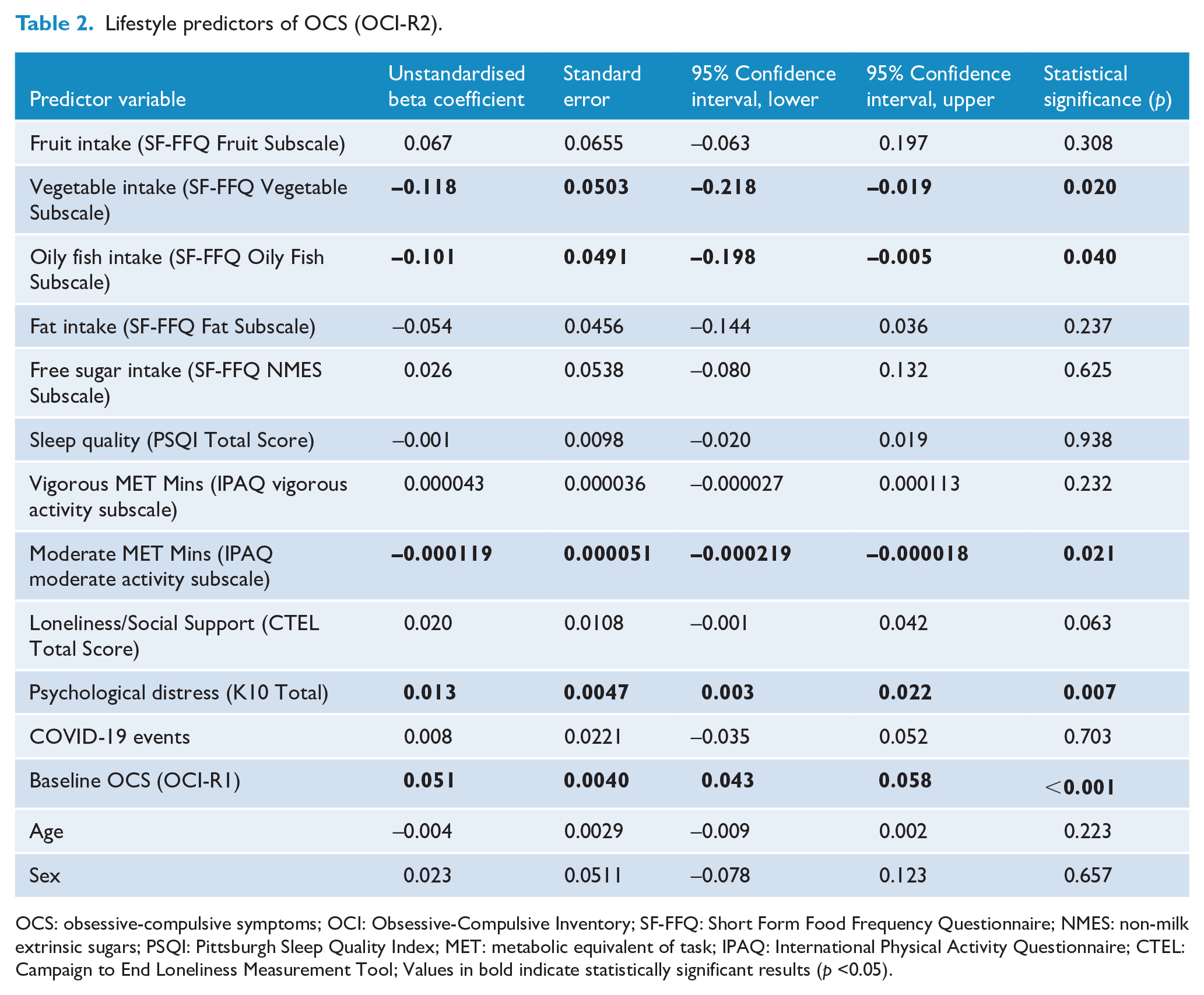
OCS: obsessive-compulsive symptoms; OCI: Obsessive-Compulsive Inventory; SF-FFQ: Short Form Food Frequency Questionnaire; NMES: non-milk extrinsic sugars; PSQI: Pittsburgh Sleep Quality Index; MET: metabolic equivalent of task; IPAQ: International Physical Activity Questionnaire; CTEL: Campaign to End Loneliness Measurement Tool; Values in bold indicate statistically significant results (p <0.05).
Predictors of compulsive PRBs
Higher compulsive PRBs at follow-up was significantly predicted by higher intake of high-fat foods (B = −0.049, p < 0.001) at baseline. In addition, higher baseline compulsive PRBs (B = 0.020, p < 0.001) and more COVID-19 events (B = −0.018, p = 0.011) predicted higher compulsive PRBs at follow-up. Results are presented in Table 3. The complete case analysis is provided in supplementary Table 2.
Lifestyle predictors of compulsive PRBs (ICBC-C2).
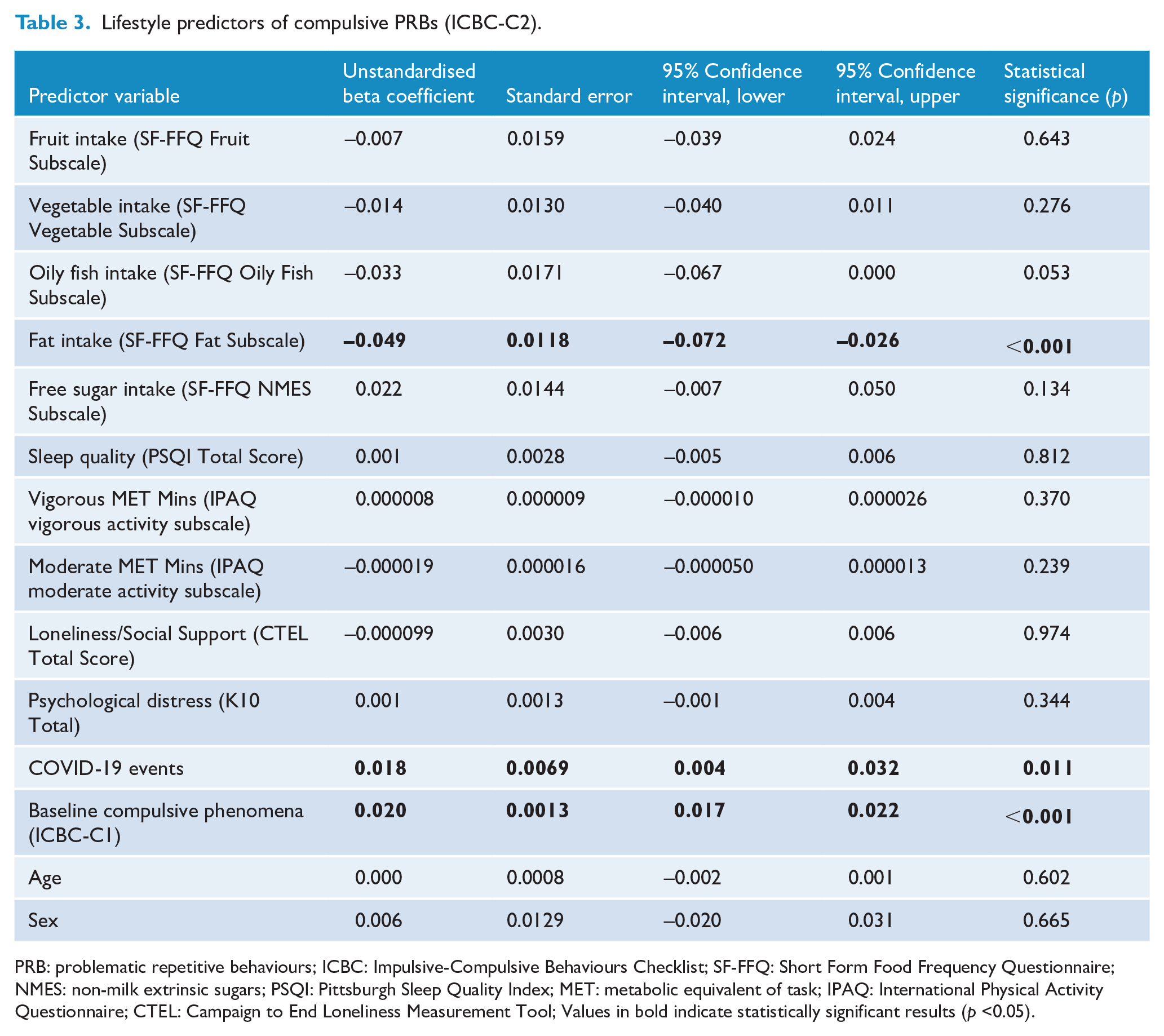
PRB: problematic repetitive behaviours; ICBC: Impulsive-Compulsive Behaviours Checklist; SF-FFQ: Short Form Food Frequency Questionnaire; NMES: non-milk extrinsic sugars; PSQI: Pittsburgh Sleep Quality Index; MET: metabolic equivalent of task; IPAQ: International Physical Activity Questionnaire; CTEL: Campaign to End Loneliness Measurement Tool; Values in bold indicate statistically significant results (p <0.05).
Predictors of impulsive PRBs
No lifestyle factors were associated with impulsive PRBs at follow-up. Among covariates, higher baseline impulsive behaviours (B = 0.024, p < 0.001) predicted an increase in impulsive behaviours at follow-up. Results are presented in Table 4. The complete case analysis is provided in supplementary Table 3.
Lifestyle predictors of impulsive phenomena (ICBC-I2).
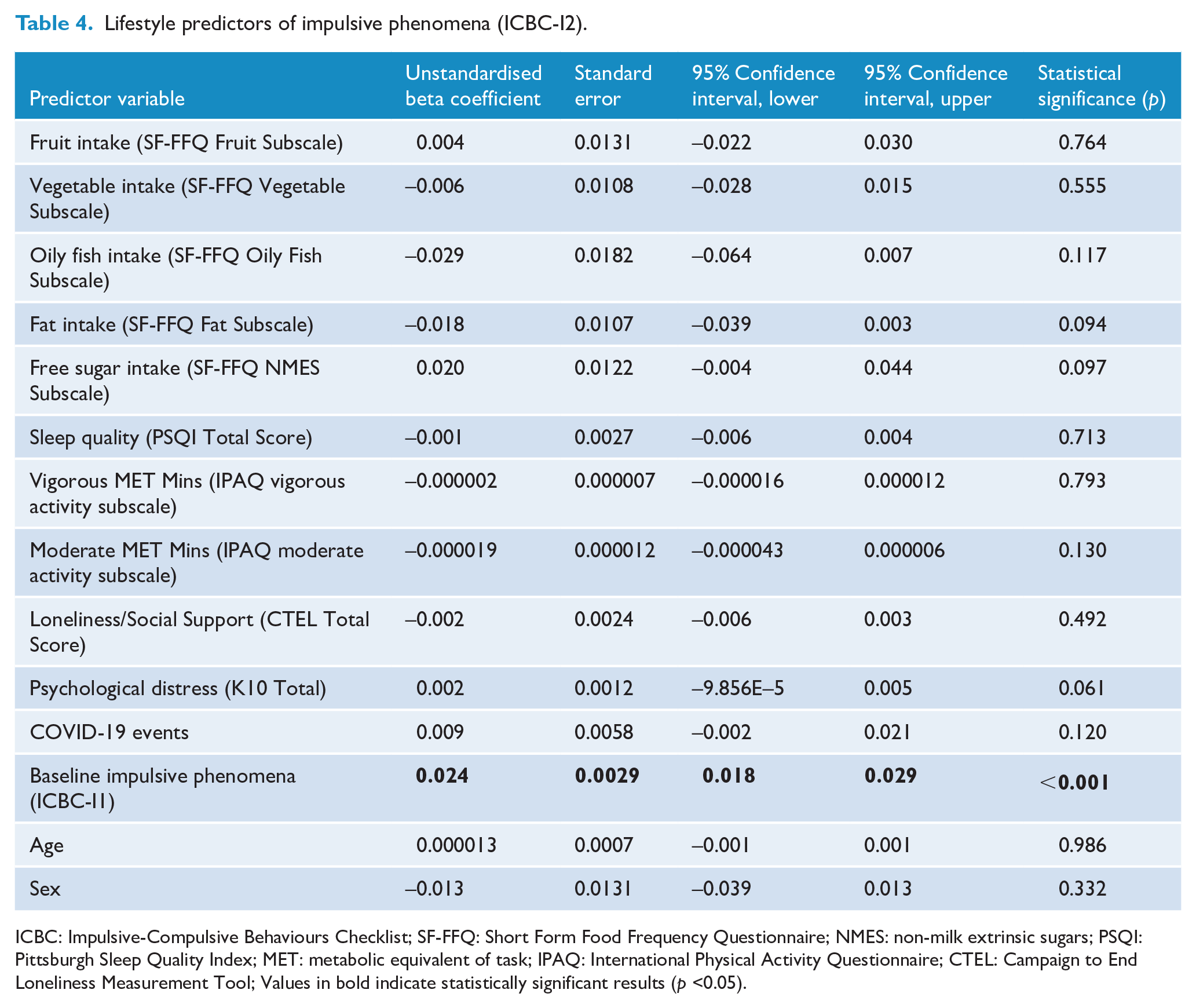
ICBC: Impulsive-Compulsive Behaviours Checklist; SF-FFQ: Short Form Food Frequency Questionnaire; NMES: non-milk extrinsic sugars; PSQI: Pittsburgh Sleep Quality Index; MET: metabolic equivalent of task; IPAQ: International Physical Activity Questionnaire; CTEL: Campaign to End Loneliness Measurement Tool; Values in bold indicate statistically significant results (p <0.05).
Discussion
We investigated the longitudinal lifestyle risk factors predicting OCS and related PRBs. Across OCS and compulsive PRBs, we predominantly found that poorer adherence to some aspects of a healthy diet predicted poorer outcomes. Specifically, lower vegetable and oily fish intake as well as lower engagement in moderate intensity physical activity significantly predicted higher OCS. Higher intake of high-fat foods at baseline was associated with greater problems associated with compulsive PRBs at follow-up. As would be expected, higher reported problems with OCS and compulsive PRBs at baseline were longitudinally associated with higher levels of these problems. No baseline lifestyle factors significantly predicted greater impulsive PRBs at follow-up. Only higher baseline impulsive PRBs this change.
Dietary aspects of higher vegetable and oily fish intake and lower intake of high-fat foods are related to lower inflammation (Lopez-Garcia et al., 2004). Meta-analysis has suggested that an anti-inflammatory diet may promote good mental health and lower the risk of developing a number of health conditions (Marx et al., 2021b). Existing research into mental health outcomes has reported that following a Mediterranean Diet, a dietary pattern associated with lower inflammation (Murphy and Parletta, 2018), may be effective in reducing depressive symptoms in non-clinical community samples (Parletta et al., 2019) and in individuals with moderate to severe major depressive episodes (Jacka et al., 2017) compared to social support control conditions.
Our findings extend existing literature by showing that dietary quality may be associated with compulsivity-related behaviours specifically. It may be interpreted from the current study that an anti-inflammatory diet is protective against OCS and compulsive PRBs. This supports previous findings in particular relation to OCS whereby Briguglio and colleagues (2019) reported on nine paediatric cases (all males aged 11–18) with a diagnosis of OCD who received nutritional counselling in order to promote greater Mediterranean Diet adherence (Briguglio et al., 2019). After 1 month, increased adherence to a Mediterranean Diet was associated with a significant reduction in their OCD symptoms and PRBs (tics, specifically).
Our findings showed that higher moderate intensity physical activity predicted lower OCS 3 months later, although this finding was not replicated in the analysis of PRBs. These findings indicate that moderate intensity physical activity may be beneficial in managing OCS and related symptoms which lead to OCD. The link between moderate intensity physical activity and OCS supports previous intervention studies whereby moderate intensity exercise interventions have shown an acute decrease in OCS (Abrantes et al., 2019; Brown et al., 2007; Rector et al., 2015). Compared to vigorous intensity exercise which places excessive stress on the body, cerebral perfusion is optimised during moderate intensity exercise (Smith and Ainslie, 2017), and this may explain more positive shifts in OCS and problematic behaviours through moderate intensity exercise. Moreover, moderate intensity exercise improves cognitive function, while the same effect has not been shown following vigorous intensity exercise (Chang et al., 2012). More recently, it has been shown that moderate intensity exercise, and not vigorous intensity exercise, improves inhibitory control (Dhir et al., 2021), an important ability for managing distressing thoughts and resisting behavioural urges common to OCS and PRBs (Chamberlain et al., 2005). This, too, may indicate that moderate intensity physical activity in our sample was protective of cognitive functioning and prevented the worsening of OCS and PRBs.
While dietary intake and physical activity engagement are different aspects of lifestyle, they may involve specific mechanisms of action which protect mental health and, in this context, protect against the worsening of OCS and symptoms. One important mechanism of action may be related to inflammation and the gut microbiome via the gut-brain axis. Poor diet quality and low physical activity engagement have been linked to increased psychological stress which, in turn, heightens an inflammatory immune response (Marx et al., 2021a). Indeed, higher levels of inflammation are noted transdiagnostically across mental illness. An anti-inflammatory dietary pattern and regular engagement in moderate intensity physical activity may improve the health of the gut microbiome (Conlon and Bird, 2014) and in turn reduce the severity of OCS, symptoms and related behaviours.
Brain-derived neurotrophic factor (BDNF), a brain molecule positively associated with neuroplasticity, learning and mental well-being, may also be implicated in the relationship between lifestyle and compulsive behaviours (Fontenelle et al., 2018). OCD patients, regardless of treatment engagement status, have lower levels of BDNF compared to healthy controls (Fontenelle et al., 2012; Maina et al., 2010; Wang et al., 2011). While cognitive inflexibility and psychological stress are drivers of OCS severity (Chamberlain et al., 2006; Den Ouden et al., 2020), increased BDNF is associated with greater cognitive flexibility and resilience to stress (Giese et al., 2013; Schmitt et al., 2016). Therefore, it seems reasonable to speculate that lifestyle behaviours such as physical activity (Dinoff et al., 2017), stress-management activities (Cahn et al., 2017), probiotic use (Haghighat et al., 2021; Kim et al., 2021) and adherence to a Mediterranean diet (with a particular supplementation of nuts) (Sánchez-Villegas et al., 2011) may ameliorate OCD symptoms through increased BDNF and resulting cognitive flexibility.
Despite the anti-inflammatory effect of lower added sugar and higher fruit intake, they were unrelated to higher OCS at follow-up. Reasons for this may be twofold. First, the COVID-19 pandemic is likely to have disrupted symptoms of contamination/cleaning and harm/checking (Fontenelle et al., 2021; Perkes et al., 2020), due to increased fears of virus spread and illness impacting on the individual and their loved ones. This may have led to a reduction in the power of the OCI-R scoring longitudinally and therefore the importance of certain lifestyle factors may have been compromised in our statistical analyses. Second, lifestyle may affect OCS dimensions in different ways. The heterogeneity observed across cases of OCD – as well as related compulsive phenomena – adds a level of complexity to OCS and requires us to develop a deeper understanding of the mechanisms influencing not only symptom severity but also different presentations with relation to the content of obsessions and compulsions.
Our study presents several strengths. First, we assessed the relationship between lifestyle and OCS as well as transdiagnostic compulsive behaviours. This allows the clinical implications resulting from our findings to target several problem symptoms and behaviours. Our holistic consideration of lifestyle factors allowed us to pinpoint those most pertinent to OCS and compulsive PRBs, and to identify targets for education and intervention. We gathered longitudinal data across different lifestyle domains from a large sample, allowing us to determine modifiable lifestyle factors to intervene in worsening OCS and compulsive PRBs. Our findings on the relationship between diet quality and OC behaviours and symptoms are novel and have not been documented in any previous literature, although they add weight to the growing evidence base supporting the utility of anti-inflammatory dietary patterns in aiding physical and emotional well-being.
Our findings should also be considered in light of the study’s limitations. A drawback of collecting a large online sample is the reliance on self-report measures. The use of self-report dietary measures has also been shown to be less accurate than more comprehensive clinician-administered food frequency questionnaires (Cleghorn et al., 2016). We also saw a high attrition rate between timepoints which may be associated with a bias in participant’s responses. However, our multiple imputation method should have counter-acted any bias due to dropout. Furthermore, we collected the data during the COVID-19 pandemic, and related disturbances to lifestyle and mental health have likely impacted results. While we controlled for potentially stressful COVID-19-related events as well as broader psychological distress, we cannot expect to have controlled for the wide range of impacts of the pandemic across a general population sample. Finally, it is not completely clear whether these findings are generalisable to clinical samples, as these individuals tend to show earlier and more insidious onset of OCD symptoms and are more likely to be prescribed medications that may affect lifestyle.
Our findings present important clinical implications. The fact that many aspects of a healthy diet were shown to protect against higher OCS and compulsive PRBs suggests that holistic dietary interventions, focusing on an anti-inflammatory dietary pattern, may be an effective lifestyle intervention for at-risk groups. In contrast to other OCRD treatments (such as serotonin reuptake inhibitors and cognitive behavioural therapy), lifestyle interventions are scalable and relatively free of side effects (Fontenelle et al., 2018). While these findings have immediate relevance in an epidemiological context and are important for prevention and early intervention, they should be replicated in clinical and treatment-seeking settings. In assessing clinical samples which, as discussed, are known to be highly heterogeneous, it would be important to consider individual genetic and epigenetic differences in order to understand potentially differing reactivity to lifestyle factors, as has been previously discussed in relation to environmental risk factors (Bellia et al., 2021). Finally, prior to the implementation of lifestyle interventions, it is important to consider its potential uptake by consumers and thus understanding the acceptability of lifestyle interventions to this group and co-design are important areas for future exploration. This is particularly important, as previous dietary interventions for mood have shown low adherence and minimal dietary quality improvement (Bot et al., 2019; Sánchez-Villegas et al., 2013).
Our study findings are novel and speak to the importance of healthy lifestyle behaviours as potentially protective factors against OCS and compulsive PRBs. An anti-inflammatory diet and moderate intensity physical activity are promising candidates in the prevention, early intervention and possible adjunct treatments for symptoms of compulsive disorders. These findings contribute to a broader field of literature which has, thus far, emphasised the importance of a healthy lifestyle to promote good mental health. Moreover, these findings provide the impetus for several promising areas of future research in lifestyle factors and intervention across OCRDs.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221085923 – Supplemental material for Lifestyle risk factors for obsessive-compulsive symptoms and related phenomena: What should lifestyle interventions target?
Supplemental material, sj-docx-1-anp-10.1177_00048674221085923 for Lifestyle risk factors for obsessive-compulsive symptoms and related phenomena: What should lifestyle interventions target? by Mary-Ellen E Brierley, Lucy Albertella, Erynn Christensen, Kristian Rotaru, Felice N Jacka, Rebecca A Segrave, Karyn E Richardson, Rico SC Lee, Edouard Kayayan, Sam Hughes, Murat Yücel and Leonardo F Fontenelle in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: M.-E.E.B. is supported by an Australian Government Research Training Program (RTP) Scholarship. M.Y.’s role on this paper was funded through a National Health and Medical Research Council Fellowship (NHMRC; #APP1117188). M.Y. also receives funding from other NHMRC schemes, Monash University and Australian Government funding bodies such as the Australian Research Council (ARC), Australian Defence Science and Technology (DST), and the Department of Industry, Innovation and Science (DIIS). He has also received philanthropic donations from the David Winston Turner Endowment Fund, Wilson Foundation (which supported this study), as well as payments in relation to court-, expert witness- and/or expert review-reports. L.F.F. is supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (# 302526/2018-8), Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (#E 26/203.052/2017), the D’Or Institute of Research and Education (no grant number) and the David Winston Turner Endowment Fund (no grant number). None of the above funding bodies were involved in the study design, management, data analysis and interpretation of results, or writing of the manuscript.
Data Availability Statement
Data available on request from the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.