
Abstract
Background:
Perinatal depression is often underdiagnosed; consequently, many women suffer perinatal depression without follow-up care. Screening for depressive symptoms during the perinatal period has been recommended in Australia to increase detection and follow-up of women suffering from depressive symptoms. Screening rates have gradually increased over the last decades in Australia.
Objective:
To explore trends in referrals of women to community mental health services during the perinatal period, and prenatal and postnatal admissions to psychiatric units, among those who gave birth in Queensland between 2009 and 2015.
Method:
Retrospective analyses of data from three linked state-wide administrative data collections. Trend analyses using adjusted Poisson regression models examined 426,242 births. Outcome variables included referrals to specialised mental health services; women admitted with a mood disorder during the second half of their pregnancy and during the first 3 months of the postnatal period; and women admitted with non-affective psychosis disorders during the second half of their pregnancy and during the first 3 months of the postnatal period.
Results:
We found an increase in mental health referrals during the perinatal period over time (adjusted incidence rate ratio, 1.07; 95% confidence interval, [1.06, 1.08]) and a decrease in admissions with mood disorders during the first 3 months of the postnatal period (adjusted incidence rate ratio, 0.95; 95% confidence interval, [0.94, 0.98]). We did not find any changes in rates of admission for other outcomes.
Conclusion:
Since the introduction of universal screening in Queensland, referrals for mental health care during the perinatal period have increased, while admissions for mood disorders in the first 3 months after delivery decreased.
Keywords
Introduction
Perinatal depression is a public health concern that affects around 12% of women during and after pregnancy (Gavin et al., 2005). During the early postpartum period, women are at an increased risk of psychiatric admissions, with the most common diagnosis for admission being nonpsychotic depression and puerperal psychosis (Langan Martin et al., 2016). Despite its prevalence, perinatal depression is underdiagnosed (Marcus et al., 2003; Smith et al., 2004) with around 50% of antenatal or postnatal cases going undetected and only 20% receiving treatment (Marcus, 2009). In some countries, one response has been to administer universal screening for depression during the perinatal period (Austin et al., 2017; Austin and Highet, 2011; Siu and US Preventive Services Task Force, 2016). In Australia, antenatal and postnatal routine screening using the Edinburgh Postnatal Depression Scale (EPDS) has been supported by the National Perinatal Depression Initiative (NPDI) since 2008 and recommended by clinical guidelines since 2011(Austin and Highet, 2011; Highet and Purtell, 2012). As a result, rates of screening in Australia have gradually increased in the last decades (Moss et al., 2020). In 2000, before the guidelines were released, around 30% of women were screened for antenatal and postnatal depressive symptoms; this percentage increased to 79% in 2017 (Moss et al., 2020).
Although universal screening appears to increase identification, referral and service use, and may reduce the prevalence of depression (O’Connor et al., 2016; Reilly et al., 2020), there is still no consensus on its benefits. Australia and the United States recommend universal screening for depressive symptoms during the perinatal period (Austin et al., 2017; Siu and US Preventive Services Task Force, 2016), but other countries such as Canada and the United Kingdom do not (Joffres et al., 2013; National Institute for Health and Care Excellence (NICE), 2014). This lack of consensus on the value of universal screening guidelines highlights the importance of research into its effectiveness. We therefore explored trends in referrals to community mental health services and admissions to psychiatric units in a 7-year period. We hypothesised that gradual increases in EPDS screening over time might be reflected in greater referrals to specialised mental health services during the perinatal period, but lower admissions as a result of more early interventions.
Methods
Data sources
We followed the reporting guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement checklist. Retrospective analyses were conducted using linked administrative data. Data were taken from the ‘Born in Queensland’ study, a linkage study of state-wide population-based administrative data based in Queensland (QLD), Australia. For this analysis, we used three linked data collections: the Queensland Hospital Admitted Patient Data Collection (QHAPDC) (Queensland Health, 2015a), the Queensland Perinatal Data Collection (QPDC) (Queensland Health, 2015b) and the Consumer Integrated Mental Health Application (CIMHA) (Queensland Government, 2016). Data Linkage of these three data collections was performed by the Statistical Services Branch at the Queensland Department of Health; more information about the process of linkage can be found elsewhere (Queensland Health, 2016).
Study population
The QPDC includes all births of at least 20 weeks of gestation or 400 g birth weight in Queensland. It contains sociodemographic and clinical information of mothers and neonates. The QHAPDC includes any inpatient admission of the mother or offspring from the first antenatal care visit onwards. The CIMHA is a state-wide electronic medical record of contact with government primary mental health services. This study included all births in Queensland in the period from 1 January 2009 to 31 December 2015. Probabilistic record linkage was performed by the QLD Department of Health. Individuals were matched across the three data collections, resulting in a sample comprising 429,058 births between January 2009 and December 2015. Births with missing information in any variables of interest for multivariable analyses were excluded.
Outcomes
The outcome variable for referral to a specialised mental health service was whether women were referred at least once for further assessment during pregnancy and the first 3 months of the postnatal period (Conception until 12 weeks after birth) as recorded in CIMHA. For this particular outcome, we only included public patients as we do not have information on referrals to private mental health practitioners, and we only considered the first referral of each pregnancy during the study period. Prenatal and postnatal referrals were grouped together as ‘Perinatal referrals’ because birth dates are only expressed as months and year, if referral were initiated the same month as the birth we were not able to classify them as prenatal or postnatal.
The outcome variable for psychiatric admissions was whether women were admitted with a psychiatric diagnosis (‘Principal’ or ‘Other diagnosis’) identified using the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM) diagnosis codes. Two categories were examined: ‘Mood disorders’ (F30-F39, F53.0, F53.1, F53.8 and F53.9) and ‘Non-affective psychosis’ disorders (F20, F22-F29). We created four binary outcome variables: (1) women admitted with a mood disorder during the second half of their pregnancy; (2) women admitted with non-affective psychosis disorders during the second half of their pregnancy; (3) women admitted with a mood disorder during the first 3 months of the postnatal period; and (4) women admitted with non-affective psychosis disorders during the first 3 months of postnatal period. We only considered the first admission of each pregnancy during the study period. The admissions were counted on the year the woman gave birth; only the first admission was considered per mother during the study period, as some mothers have more than one admission. To explore the possible effect of screening, we considered only admissions during the second half of the pregnancy period, because antenatal screening is recommended as early as practical during pregnancy, and the first antenatal visit typically occurs around the 10th week of pregnancy. In the case of admissions, we were able to identify whether the episode of admission was before or after the episode of delivery, and therefore, we were able to classify them as prenatal or postnatal admission.
Covariates
The predictor variable was the birth year, from 2009 to 2015, centred on 2009. The variable was treated as continuous. Other covariates included the following: maternal age (coded as ‘less than or equal to 25 years old’, ‘26 to 35 years old’ and ‘36 or more years old’); private or public patient status; Australian Indigenous status (‘yes’ if a woman identified herself as being Indigenous); marital status (coded as ‘married or in a de facto relationship’ and ‘not married or separated’); country of birth (‘Australia’ or ‘not Australia’); and socioeconomic status (SES) from the Socio-Economic Index for Areas (SEIFA) (Australian Bureau of Statistics, 2011) derived from place of residence, based on the Index of Relative Socioeconomic Disadvantage (IRSD) (SEIFA scores of 1 and 2 being most disadvantaged, 3–4, 5–6, 7–8 and 9–10 being least disadvantaged).
Statistical analysis
We ran descriptive analyses to explore characteristics of the sample and chi-square tests to explore the associations between different sociodemographic characteristics and years. Admission rates were explored through frequency distributions and chi-square for trends to examine the difference in referrals and admission rates across time. Admission rates are given as the proportion of the total number of women who gave birth that year. Confounding variables were selected for inclusion in the multivariable models based on the literature on sociodemographic predictors of psychiatric conditions during the perinatal period (Betts et al., 2020; Rich-Edwards et al., 2006). We conducted Poisson regression analyses using robust standard errors for each outcome variable and adjusted these models for relevant confounders as identified above. Using incident rate ratio (IRR) obtained from unadjusted and adjusted models, we derived the mean annual change for each outcome. In order to specifically explore mood disorders other than bipolar diagnoses, we ran a sensitivity analysis including only ICD-Codes F32 to F39 during the first 3 months of the postnatal period. Since women who have multiple pregnancies in the study period lead to non-independent outcomes, we ran sensitivity analyses including only the first birth episode/pregnancy for each woman over the study period.
Ethics
Ethical approval was granted by Children’s Health Queensland (HREC Reference number: HREC/16/QRCH/231) and ratified by the University of Queensland Ethics Committee (Clearance Number: 2016001629). The ‘Born in Queensland’ study was approved by the office of the Director-General of QLD Health (Reference: QCOS/029817/RD006796).
Results
Of the 429,058 births that occurred in Queensland between January 2009 and December 2015, 426,242 (99.3%) had complete information for all variables included in the multivariable models (Figure 1). Of those 0.7% births with missing information, 70% concerned SEIFA and 24% private or public patient status. Over 75% of the missing information was from the first 3 years of the study. Sixty per cent of women with missing information were private patients, 10.1% unmarried, 23% born outside Australia, 4.5% Indigenous and 24 were aged 35 years or older. Sociodemographic characteristics of the sample included in the analysis are provided in Table 1. Chi-square tests showed that the frequencies of predictor variables changed over time (Table 1). Over the 6-year period of the study, the proportion of women who were not married or separated; Australian Indigenous; public patients; and born overseas increased over time.
Flow diagram.
Sociodemographic and health characteristics of the sample.
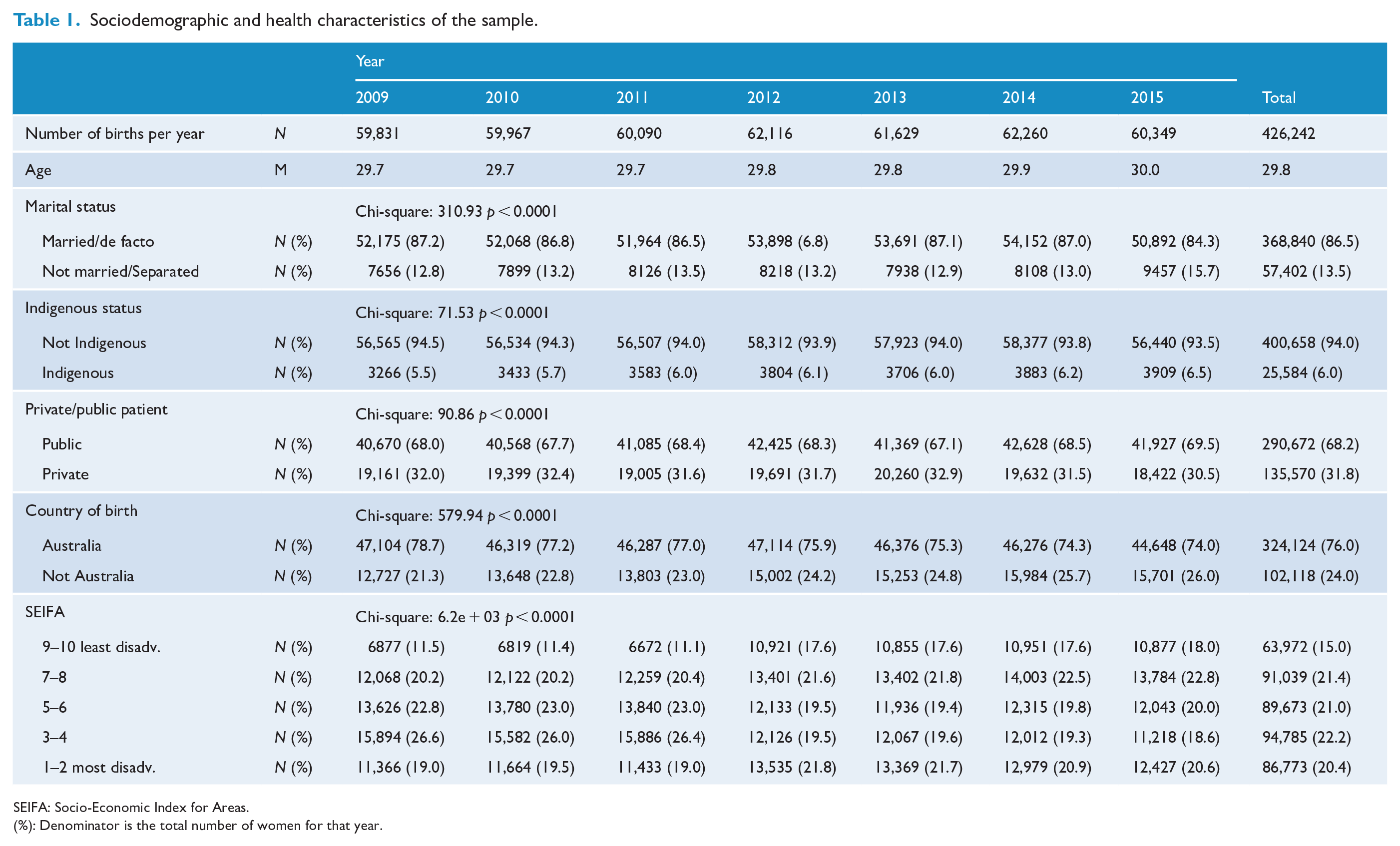
SEIFA: Socio-Economic Index for Areas.
(%): Denominator is the total number of women for that year.
Table 2 contains the frequency of referrals for mental health care in public patients during the perinatal period and the frequency of pre- and postnatal psychiatric admissions, including results from chi-square tests for trends. Mental health referrals during the perinatal period climbed from 989 to 1730 over the 6-year period. By contrast, admissions for mood disorders during pregnancy, and psychosis during pregnancy and the postnatal period were steady in the 6-year period, while postpartum depression admissions decreased from 390 to 314. Across all years, the most frequent admission was for mood disorders during the postnatal period, followed by mood disorders during pregnancy. Figure 2 shows the trends in rates per year (percentage of women from the total number of women who gave birth that year) for each of the outcomes explored.
Frequencies of mental health referrals in public patients (n = 290,672 patients) and prenatal and postnatal mood and non-affective psychosis admissions, 2009–2015 (n = 426,242 patients).
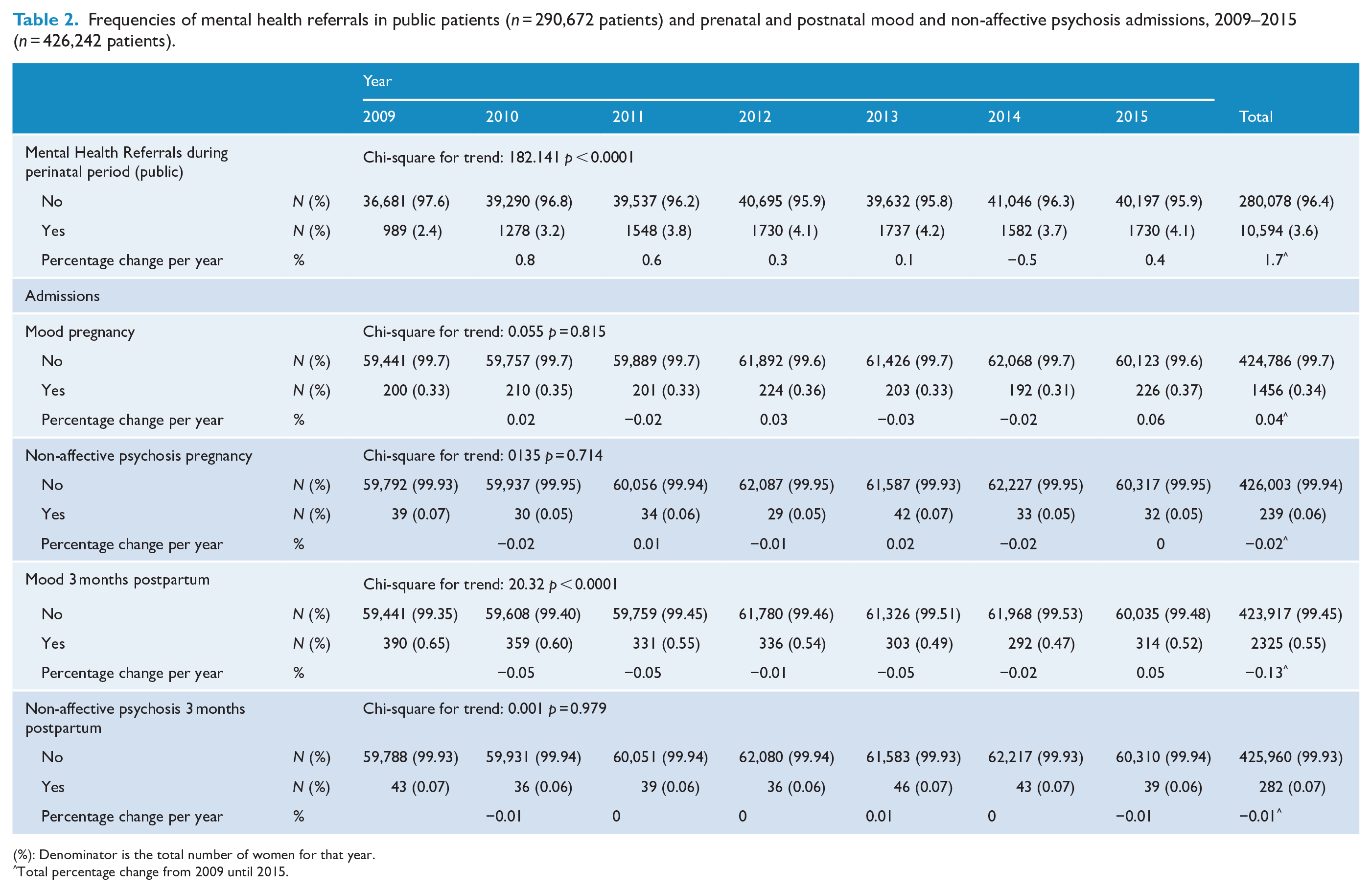
(%): Denominator is the total number of women for that year.
Total percentage change from 2009 until 2015.
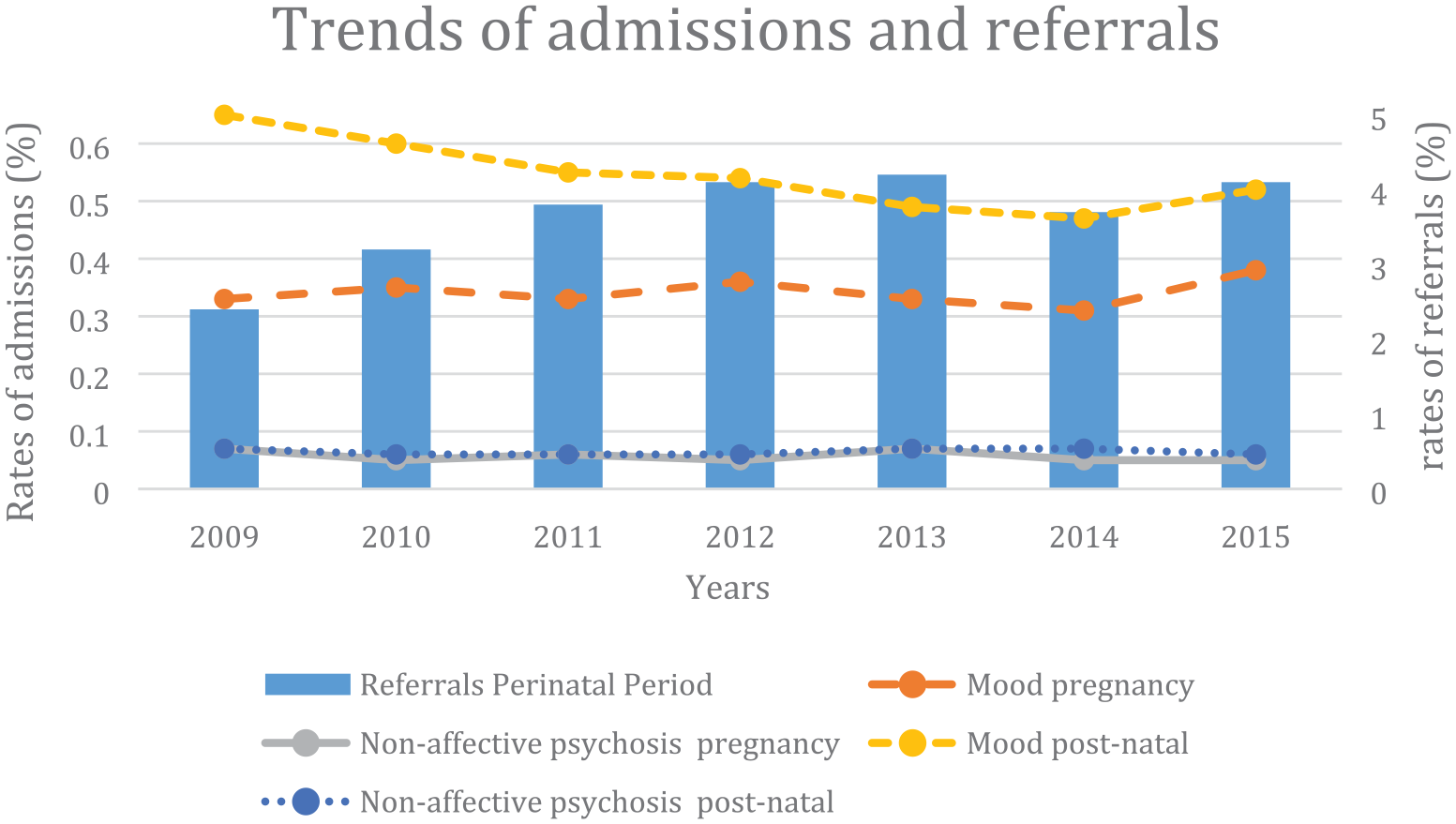
Trends in mental health admissions and referrals (express in % per year), Queensland, 2009–2015.
Unadjusted Poisson regression models showed increased rates of referral to a specialised mental health service during the perinatal period across the time period (unadjusted incidence rate ratio [uIRR], 1.07; 95% confidence interval [CI], [1.06, 1.08]). This increase remained after adjustment for relevant confounders (adjusted incidence rate ratio [aIRR], 1.07; 95% CI, [1.06, 1.08]) (Table 3). The unadjusted Poisson regression model showed a decrease over time in admissions with a diagnosis of mood disorder during the first 3 months of the postnatal period (uIRR, 0.95; 95% CI, [0.94, 0.97]). This decrease remained after adjustment for relevant confounders (aIRR, 0.95; 95% CI, [0.94, 0.98]) (Table 3). Sensitivity analysis including only mood disorders with ICD-Codes F32 to F39 during the first 3 months of the postnatal period showed similar results (aIRR, 0.95; 95% CI, [0.93, 0.97]). Admission rates for mood and non-affective Psychosis diagnosis disorders during pregnancy and for non-affective Psychosis diagnosis during the postnatal period did not show changes over time in any of the models, during any Poisson regression analyses (Table 3 and Supplementary Table S1). Unadjusted and adjusted rates of change are presented in Table 4 for each of the outcomes. Sensitivity analyses including only the first birth episode/pregnancy for each woman over the study period showed similar results (Supplementary Table S2).
Adjusted Poisson regression analysis of prenatal mental health referrals and admissions during pregnancy and the postnatal period among all births.
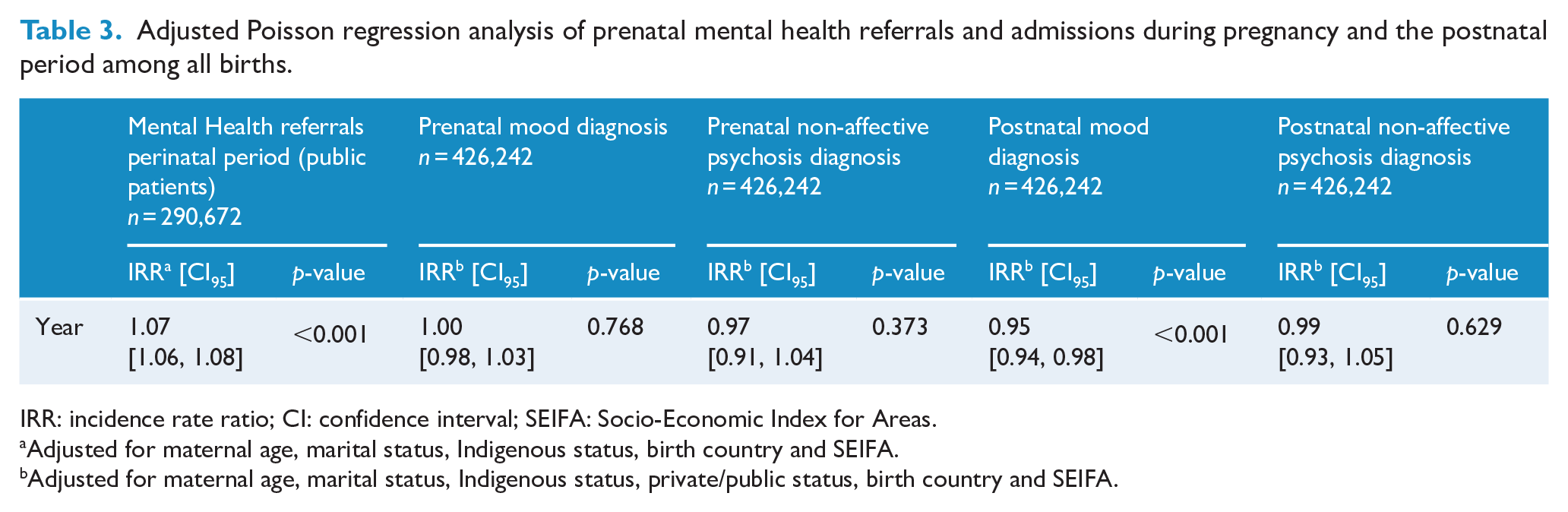
IRR: incidence rate ratio; CI: confidence interval; SEIFA: Socio-Economic Index for Areas.
Adjusted for maternal age, marital status, Indigenous status, birth country and SEIFA.
Adjusted for maternal age, marital status, Indigenous status, private/public status, birth country and SEIFA.
Mean annual change in IRR (2009–2015) for referrals and admissions.
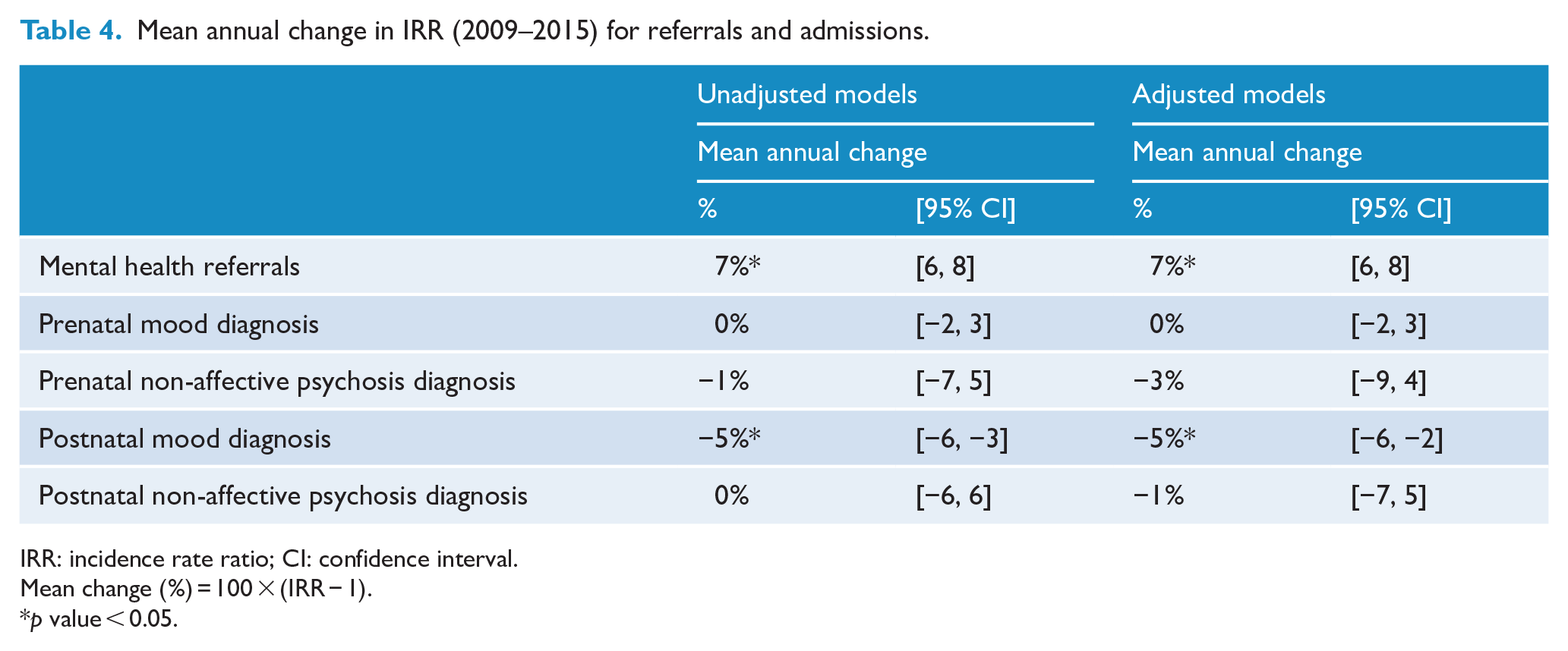
IRR: incidence rate ratio; CI: confidence interval.
Mean change (%) = 100 × (IRR − 1).
p value < 0.05.
Discussion
This is the first study to examine rates of mental health referrals and prenatal and postnatal mental health admissions in the period after perinatal universal screening recommendations were introduced by Austin and Highet, 2011; Highet and Purtell, 2012. We found an increase in mental health referrals during perinatal period over time and a decrease in the postnatal admissions of women with mood disorders. We did not find changes in the admission rates of women with mood disorders or non-affective psychosis disorders during the second half of their pregnancy nor changes in admission rates of women with non-affective psychosis diagnosis disorders during the first 3 months of the postnatal period.
The increase in mental health referrals during this period may be explained by the introduction of recommendation of routine screening in the NPDI and clinical guidelines. Previous studies have shown that asking about psychiatric history during the perinatal period is a stronger predictor of receiving a referral for mental health care (Reilly et al., 2013), and EPDS screening significantly increases referrals to social work for mental health reasons during the postpartum period (Chaudron et al., 2004). A systematic review found evidence that screening programmes during the perinatal period increase referrals and engagement with support services (Reilly et al., 2020). Australian guidelines released in 2011 recommended follow-up and further referral to appropriated care for women with a EPDS score of 13 (Austin and Highet, 2011). This increase in referrals is consistent with increases in rates of universal perinatal depression screening in Australia in the last decades (Moss et al., 2020).
We found no changes over time in the admission rates during the second half of pregnancy for mood disorders or non-affective psychosis diagnosis disorders. There may be several explanations for this finding. One may be that screening during pregnancy does not have an immediate impact on the severity of the psychiatric disorder. In addition, while screening is recommended as soon as practical, there is not a fixed time for it to occur. As a result, some women may not have benefitted from early intervention. Finally, it may reflect that the greater risk for psychiatric admission is not during pregnancy but in the initial months following childbirth (Langan Martin et al., 2016). We found no changes over time in the postpartum admission rates of non-affective psychosis diagnosis. However, the focus of this paper was examining changes in admissions based on the increase in screening for depressive symptoms during the perinatal period. Screening with the EPDS is not intended to identify diagnoses other than depression. This may explain why there were no changes in the admissions of women with a diagnosis of non-affective psychosis disorders during pregnancy or during the postnatal period.
In contrast, there was a decrease in early postnatal admissions of women with mood disorders. This is of particular importance as the early postpartum period is a period of elevated risk of psychiatric admission, particularly due to mood disorders, with nonpsychotic depression being the most common inpatient psychiatric diagnosis in the first 2 years after birth (Langan Martin et al., 2016). This finding may suggest that the reduction of mood disorder admissions during the early postnatal period may reflect previous evidence showing increased screening, which may have led to earlier detection and treatment during pregnancy and early postnatal period. Prompt detection of mood disorders during pregnancy and early postnatal period may provide scope for earlier diagnosis and treatment. These in turn may prevent these cases from escalating to severe postnatal depression and requiring inpatient treatment. Postnatal depression is highly linked to antenatal depression, with some studies suggesting that antenatal depression is the principal risk factor and the strongest predictor of postnatal depression (Leigh and Milgrom, 2008; Underwood et al., 2016). Antenatal screening does not identify women who will develop postnatal depression, about 47% women suffering postnatal depression also experienced antenatal depression, with evidence showing that postnatal depression is in these cases a continuation of antenatal depression (Underwood et al., 2016). Additionally, women who receive psychosocial or psychological treatment during the prenatal period are less likely to develop postnatal depression (Dennis and Dowswell, 2013). Therefore, early detection and treatment for prenatal depression could avoid the condition extending into the postnatal period or decrease its severity. A recent systematic review reported improved symptoms and maternal mental health outcomes of women in screening programmes (Reilly et al., 2020) and another study has found an association between antenatal screening and decreased odds of postnatal admission (San Martin Porter et al., 2021).
Our findings are supported by previous studies that found a decrease in postnatal psychiatric admissions after the introduction of the NPDI (Australian Commonwealth Government, 2008) in 2008 that also advocated for screening (Lee et al., 2019). That study suggested that this reduction in admissions was due to increased screening, and consequently increased follow-up, shifting care to earlier and more to the primary care sector (Lee et al., 2019) rather than inpatient settings. However, studies looking at admissions did not include women giving birth after the release of formal guidelines in 2011, which recommended universal screening. Therefore, the present study represents strong evidence of admission outcomes as we observed transitions encompassing the time prior to consistent screening up to the time when routine/universal screening was recommended.
Age has been found to be an important factor for increased risk of psychiatric admissions (Munk-Olsen et al., 2006). Mean age in our sample increased over time, yet admissions did not increase. Additionally, specialist mental health admissions in private and public hospitals increased between 2010–2011 and 2014–2015 in the general population (Australian Institute of Health and Welfare (AIHW), 2016): separations increased by around 7% in private hospitals and 5% in public hospitals each year between 2010 and 2015 (AIHW, 2016). However, after accounting for these demographic changes, we did not find a significant increase in admissions, indeed finding a decrease in mood-related admissions postpartum, suggesting that other factors, potentially screening and increased referrals, may be reducing the admission rates. Missing information on key confounding variables was detected in 0.7% of the births, of which 75% was from the first 3 years of the study and of whom 60% were private patients. This may have led to small underestimations of the effect.
A randomised trial would be required to establish causation between screening for depressive symptoms and increases in mental health referrals and decreases in postnatal mood admissions. Decrease in admissions may be due to a change of diagnosis classifications over time; e.g. depression often comorbid with different psychiatric diagnoses. We considered ‘Principal’ and ‘Other diagnoses’ to identify these cases. However, we cannot exclude the possibility that not all comorbid diagnoses were recorded. Finally, these data might not reflect the current situation in Queensland, as it has been more than 6 years since the study period.
Implications
Perinatal depression is an important public health issue as it is associated with detrimental short- and long-term consequences for the well-being of the mother, child and family (Stein et al., 2014). A previous study found that 40% of mothers who were admitted due to postnatal depression reported continuation of depressive symptoms for an average of 3 years (Vliegen et al., 2010). Identification of and treatment to decrease the severity of these disorders are important to prevent their consequences. While psychiatric admissions are necessary in severe cases for the mental health of the mother, they also disrupt the family unit, resulting in long-term health problems for both the mother and offspring.
Our results suggest that screening may decrease the severity of postnatal depression, as shown by reductions in admissions of women with this diagnosis. Admissions with psychiatric diagnoses place a substantial burden on the health system as patients tend to have a longer average stay (Xu et al., 2014), with psychiatric admission being the third most common readmission after delivery (Clapp et al., 2016). In 2017, there were a concerning proportion of Australian women (20%) who were still not being screened during the perinatal period as recommended by the clinical practice guidelines (Moss et al., 2020).
Strengths
The use of administrative databases allowed us to include all births that occurred in Queensland over a 7-year period which included the introduction of the recommendation of screening in Australian clinical guidelines (2011). We were also able to include 99.8% of Queensland births in the study. This allowed us to analyse a diverse group of women in the state of Queensland and produce generalisable findings.
Limitations
Our data do not contain information on private referrals and so may underestimate the total number of referrals, but the public referrals reported are likely to represent the bulk of the total. Previous studies found that private patients are less likely to be screened and to receive referral for additional care (San Martin Porter et al., 2019). We did not have information on whether psychiatric diagnoses labelled as ‘other diagnoses’ have a key role in the length of stay. Women who gave birth in Queensland but may have been living in other countries or states before or after the delivery will not have hospitalisation records in these databases. We were not able to control for previous psychiatric history because this information was not available. Amendments to Medicare items were made in 2017 to increase screening rates in the private sector; we did not have information to assess the impact of these changes. Further studies are needed to explore the role of screening in psychiatric admissions and the role of screening in the length of stay in women with a nonpsychiatric principal diagnosis comorbid with a psychiatric diagnosis.
Conclusion
We found an increase in referrals for mental health care during the perinatal period and reduced admissions for mood disorders in the first 3 months after delivery. This was consistent with the recommendation for and increase in rates of universal perinatal depression screening in Australia. If corroborated by additional evidence, these findings further support the importance of screening for referral to mental health care during perinatal period and suggest that early detection of mood disorders may reduce the severity of mental health symptoms during the postnatal period.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221080405 – Supplemental material for Trends of perinatal mental health referrals and psychiatric admissions in Queensland
Supplemental material, sj-docx-1-anp-10.1177_00048674221080405 for Trends of perinatal mental health referrals and psychiatric admissions in Queensland by Macarena A San Martin Porter, Joemer Maravilla, Steve Kisely, Kim S Betts, Caroline Salom and Rosa Alati in Australian & New Zealand Journal of Psychiatry
Footnotes
Authors’ Note
Joemer Maravilla is now affiliated to Australian Research Council Centre of Excellence for Children and Families over the Life Course, The University of Queensland, Brisbane, QLD, Australia and Institute of Nursing, Far Eastern University, Philippines and Steve Kisely is now affiliated to Departments of Psychiatry, Community Health and Epidemiology, Dalhousie University, Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.