
Abstract
Objective:
The aim of the study was to explore the range of psychiatric diagnoses seen in pregnant women who score above the ‘cut-off’ on the Edinburgh Postnatal Depression Scale when this is used as a routine screening instrument in the antenatal period.
Method:
Subjects were all pregnant women referred to and seen by the Perinatal Consultation-Liaison Psychiatry Team of a tertiary public hospital over a 14-month period. Edinburgh Postnatal Depression Scale score at maternity ‘booking-in’ visit, demographic and clinical data were recorded and diagnoses were made according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.) criteria following clinical interview(s) and review of documented past history. Data were analysed using descriptive statistics.
Results:
A total of 200 patients who had completed the Edinburgh Postnatal Depression Scale were seen for assessment; 86 (43%) scored ⩾13 on Edinburgh Postnatal Depression Scale. Of those scoring 13 or more on Edinburgh Postnatal Depression Scale, 22 (25.6%) had a depressive disorder. In total, 12 patients (14%) had an anxiety disorder, 14 (16.3%) had borderline personality disorder and 13 (15.1%) had a substance use disorder. An additional 23 women (26.7%) had two or more borderline personality traits.
Conclusion:
Psychiatric assessment of women who scored 13 or more on the Edinburgh Postnatal Depression Scale at routine antenatal screening identified a significant number with borderline personality disorder or borderline personality traits rather than depressive or anxiety disorders. Clinical Practice Guidelines note the importance of further assessment for all women who score 13 or more on the Edinburgh Postnatal Depression Scale. The findings here suggest that this assessment should be made by a clinician able to identify personality pathology and organise appropriate and timely interventions.
Keywords
Introduction
Depressive disorders are one of the most common causes of disability worldwide. These disorders are prevalent in the perinatal period, with studies suggesting antenatal depression occurs in up to 1 in 10 women (Buist and Bilsztra, 2006) and postnatal depression in up to 1 in 6 women (Woolhouse et al., 2012). The negative impacts of perinatal depression are well-documented and can be far-reaching. For example, maternal antenatal depression has been linked to poor nutrition and use of harmful substances (Zuckerman et al., 1989), adverse obstetric and neonatal outcomes (Alder et al., 2007; Chung et al., 2001) including low birth weight and premature birth (Eastwood et al., 2017; Stein et al., 2014). A range of adverse outcomes associated with perinatal depression and anxiety may persist into childhood and adolescence, including emotional, behavioural and cognitive problems (Kersten-Alvarez et al., 2012; Murray et al., 2011; Stein et al., 2014; Van Batenburg-Eddes et al., 2013).
In Australia and many other developed countries, the prevalence and possible adverse outcomes linked to perinatal depression led to a focus on detection and management of depression in the perinatal period. In Australia, in 2008, the Australian government, together with the state and territory governments, agreed to collaborate on the development of a National Perinatal Depression Initiative – an AUD$85 million collaboration, which aimed to improve the detection and management of perinatal depression. Thereafter, came the beyondblue Clinical Practice Guidelines for depression and related disorders, released in 2011 (Austin et al., 2011). These initiatives encouraged, and the guidelines endorsed, routine universal screening with the Edinburgh Postnatal Depression Scale (EPDS) (Cox et al., 1987) to detect perinatal depression as well as enquiry about psychosocial factors in all women, in both the antenatal and postnatal periods.
New Australian Clinical Practice Guidelines were released in October 2017 (Austin et al., 2017) which in addition to continuing the focus on perinatal depression have an increased emphasis on anxiety, on severe mental illness (schizophrenia, postpartum psychosis and bipolar disorder) and borderline personality disorder (BPD) and emotional dysregulation. These guidelines again recommend screening for perinatal depression and anxiety in the perinatal period with the EPDS, with the addition of psychosocial risk screening using the Antenatal (Psychosocial) Risk Questionnaire (ANRQ) (Austin et al., 2013).
The 2011 Clinical Practice Guidelines (Austin et al., 2011) noted that the score for detecting possible major depression in the antenatal period varies from 13 to 15 and stated that ‘the evidence is not robust’. Thus, the guidelines recommended a score of 13 or more as a ‘flag’ for further follow-up, with watchful waiting and repeat administration of the EPDS after 2–4 weeks. By contrast, the 2017 Guidelines (Austin et al., 2017) recommend that further assessment should be arranged for all women who score 13 or more on the EPDS. The guidelines are not explicit regarding the most appropriate type of further assessment and note this will of necessity vary according to the setting and the access to services available in the area.
The EPDS is a self-rated, 10-item instrument that focuses on symptoms of depression in the preceding 7 days (Cox et al., 1987). It deliberately excludes somatic symptoms which can be misleading as indicators of depression given the physiological changes of childbearing, overcoming some of the limitations of other self-report scales (Cox et al., 1987; Milgrom and Gemmill, 2014). While it was initially developed to detect clinical depression in women in the postnatal period (Cox et al., 1987), it has also been validated for use to detect depression in the antenatal period (Bergink et al., 2011; Bunevicius et al., 2009; Murray and Cox, 1990) as well as for detection of anxiety (Matthey et al., 2013; Swalm et al., 2010). It has good psychometric properties (Boyce et al., 1993) and is quick, easy and acceptable to most women and health professionals (Buist et al., 2006). The 2017 Australian Clinical Practice Guidelines note that a score of 13 or more on the EPDS has moderate sensitivity (0.61 [0.5–0.72]) and high specificity (0.94 [0.92–0.96]) for detecting possible minor and major depression in pregnant women and recommend using this cut-off score (Austin et al., 2017).
Very few studies have examined the range of diagnoses other than depression and anxiety seen in antenatal women who score above threshold on screening with the EPDS. A study by Lydsdottir et al. (2014), in which women were invited into a study of mental health in the perinatal period, investigated the extent to which pregnant women who screen positive on the EPDS at 16 weeks gestation actually have serious mental disorders other than depression. Interviews were conducted using the Mini-International Neuropsychiatric Interview-Plus (MINI-Plus) to diagnose women according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria. The MINI-Plus (Sheehan et al., 1998) is a brief diagnostic tool used for research purposes and covers many, but not all, DSM-IV psychiatric diagnoses – and particularly does not include personality disorders other than antisocial personality type. Screen-positive women (n = 152, EPDS 12 or higher) had a mix of DSM-IV diagnoses: 31% had major depressive disorder, 13% had bipolar disorder, 60% had anxiety disorders, 5% had dysthymia, 12% had somatoform disorder, 2% had eating disorders and about 5% had current substance abuse.
An Australian study (Harvey and Pun, 2007) examined the prevalence of antenatal depression and other psychiatric conditions in 52 women referred to the consultation-liaison service of a tertiary maternity hospital with ‘positive’ EPDS scores (12 or higher). Clinical interviews were used to diagnose women according to DSM-IV and International Classification of Diseases (10th Revision; ICD-10) diagnoses. A broad cross section of diagnoses was found, including over a third with adjustment disorder and over 30% with depressive disorders of various types. Two percent (n = 1) of their population had post-traumatic stress disorder (PTSD), 2% had BPD and 2% had alcohol dependence in remission. In total, 10% had no psychiatric diagnosis but primarily problems with their support systems causing distress, and 15% had no psychiatric or behavioural diagnosis at all.
Aim
The aim of the study, to explore the range of psychiatric diagnoses seen in pregnant women who score above the ‘cut-off’ on the EPDS when this is used as a routine screening instrument in the antenatal period, was designed in response to the clinical experience of those working in the Perinatal Consultation-Liaison Psychiatry (PCLP) Team in Hobart, namely, that many women referred to the Team with an EPDS score ⩾13 did not have a depressive or anxiety disorder. A cut-off of 13 or more, as recommended in the 2017 Clinical Guidelines (Austin et al., 2017), was used.
Method
Setting
The study was undertaken at the Royal Hobart Hospital (RHH), a tertiary public hospital in Tasmania, which services a population of over 250,000 (Australian Bureau of Statistics, 2017a). This is the only public maternity service for the South of Tasmania. There are approximately 2000 deliveries per year. A single Mental Health Service (MHS) based in Hobart provides child and adolescent, adult inpatient and community mental health services to the same population.
The hospital maternity service introduced routine antenatal screening using the EPDS in 2013. At their antenatal ‘booking-in’ visit, all women are asked a series of questions relating to their psychosocial circumstances and to complete the EPDS. Booking-in visits occur at varying gestations, but the mean gestational age at the RHH for this initial visit is 8–9 weeks. When routine screening with the EPDS was first introduced, women who scored 13 or more were referred to their general practitioner for review and follow-up, but after the establishment of a hospital PCLP Team in late 2014, women scoring 13 or more are now offered assessment by the PCLP Team. Approximately 50% of those who score above cut-off at their screening visit accept referral to and are subsequently seen by the PCLP Team (some decline referral, others cancel or do not attend appointments). The wait time for ‘non-urgent’ referrals is 4–6 weeks. Women referred to the Team are seen antenatally as frequently as clinically indicated, may be reviewed on the maternity ward when admitted for their baby’s delivery, and for follow-up in the early postnatal period.
Participants
Participants were all pregnant women referred in the antenatal period and seen by the PCLP Team between 17 April 2016 and 31 May 2017, yielding 200 women who had completed the EPDS at their ‘booking in visit’. These women were referred for one or more of the following reasons:
Scored 13 or more on the EPDS;
Described currently experiencing problems with their mental health;
Reported a past history of anxiety or depression;
Reported a history of schizophrenia, bipolar disorder or personality disorder;
Currently prescribed antipsychotic or mood stabiliser medication.
Procedure
All women were seen for assessment by the consultant psychiatrist or psychiatric registrar. Demographic data collected included patient age, relationship status (partner/no partner) and number of other children. The clinician also recorded whether the pregnancy was planned, current and past psychiatric treatment, substance use prior to and during pregnancy and any previous involvement with Child Safety Services (CSS).
Following clinical interview(s) and review of the woman’s past psychiatric history including involvement with the MHS Child and Adolescent Team, Adult In-Patient Unit and Community Teams and any mental health presentations to the Emergency Department at RHH, diagnoses were made according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) criteria and grouped as follows:
Depressive disorder (included major depressive disorder, persistent depressive disorder, adjustment disorder with depressed mood or with mixed anxiety and depressed mood);
Anxiety disorder (including social phobia, panic disorder, agoraphobia, generalised anxiety disorder, adjustment disorder with anxiety);
Trauma and stressor-related disorders (including acute stress disorder and PTSD);
Obsessive compulsive disorder (OCD);
Schizophrenia;
Bipolar disorder;
Personality disorder (types: borderline, antisocial, narcissistic, other);
Personality traits (types: borderline, antisocial, dependent, other),
Eating disorder (including anorexia nervosa, bulimia nervosa and binge eating disorder);
Intellectual disability;
Substance use disorders (including alcohol, cannabis, amphetamines, benzodiazepines and opiates);
Other.
Statistical analysis
Descriptive statistics were used to study the socio-demographic and clinical characteristics of the sample. Data processing and frequency analyses were performed using SPSS v17.0.
Ethics
Approval for the study was received from the University of Tasmania Human Research Ethics Committee.
Results
Over the study period, a total of 334 antenatal women accepted referral to the PCLP Team and 216 (65%) were seen for assessment. In total, 52 women (15.6%) despite accepting referral declined an offer of appointment with the PCLP Team and 66 women (19.8%) did not attend scheduled appointments.
EPDS scores were recorded for 200 of the 216 women in our sample; the EPDS was declined in 16 cases. Mean (SD) EPDS score for the sample was 11.6 (5.9) with a range of 0–28. In total, 86 women (43%) scored above cut-off of 13 or more.
Demographic and clinical features of sample
Characteristics of the 200 women who completed the EPDS are shown in Table 1. The mean ± SD age of women was 27 ± 6.3 years, 43.5% (n = 87) were expecting their first child, almost two-thirds of pregnancies were unplanned (n = 125; 62.5%) and just under one in five women (n = 37: 18.5%) was without a partner. In total, 30 women (15%) had involvement with CSS as a child, and 26 women (13.0%) had CSS involvement in a previous pregnancy. High rates of substance use (n = 30; 15%), especially cannabis use (n = 21; 10.5%), continuing during pregnancy were reported at the initial assessment interview.
Sample characteristics.
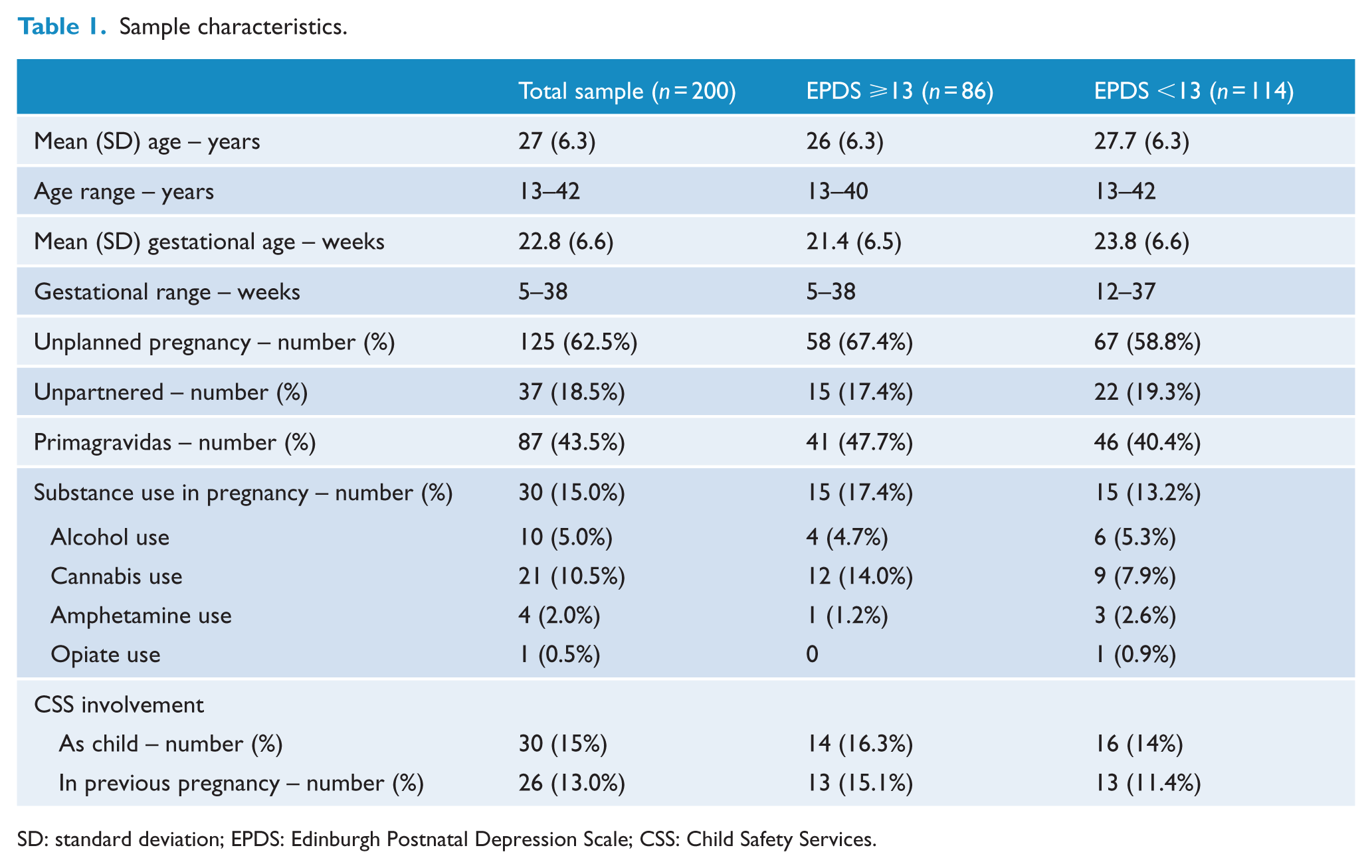
SD: standard deviation; EPDS: Edinburgh Postnatal Depression Scale; CSS: Child Safety Services.
As shown in Table 2, many of the women seen reported both current and past psychiatric treatment (one or more of psychotropic medication, psychologist, psychiatrist, MHS). One-third of women (n = 65; 32.5%) were currently engaged in psychiatric treatment, and the majority (n = 158; 79%) had received psychiatric treatment in the past. Almost half (n = 95; 47.5%) had received psychiatric treatment only in the past, and only a minority of those seen reported neither current nor past treatment (n = 40; 20%). Women with EPDS <13 were more likely to be currently receiving psychiatric treatment than those with EPDS ⩾13.
Current and past psychiatric treatment.
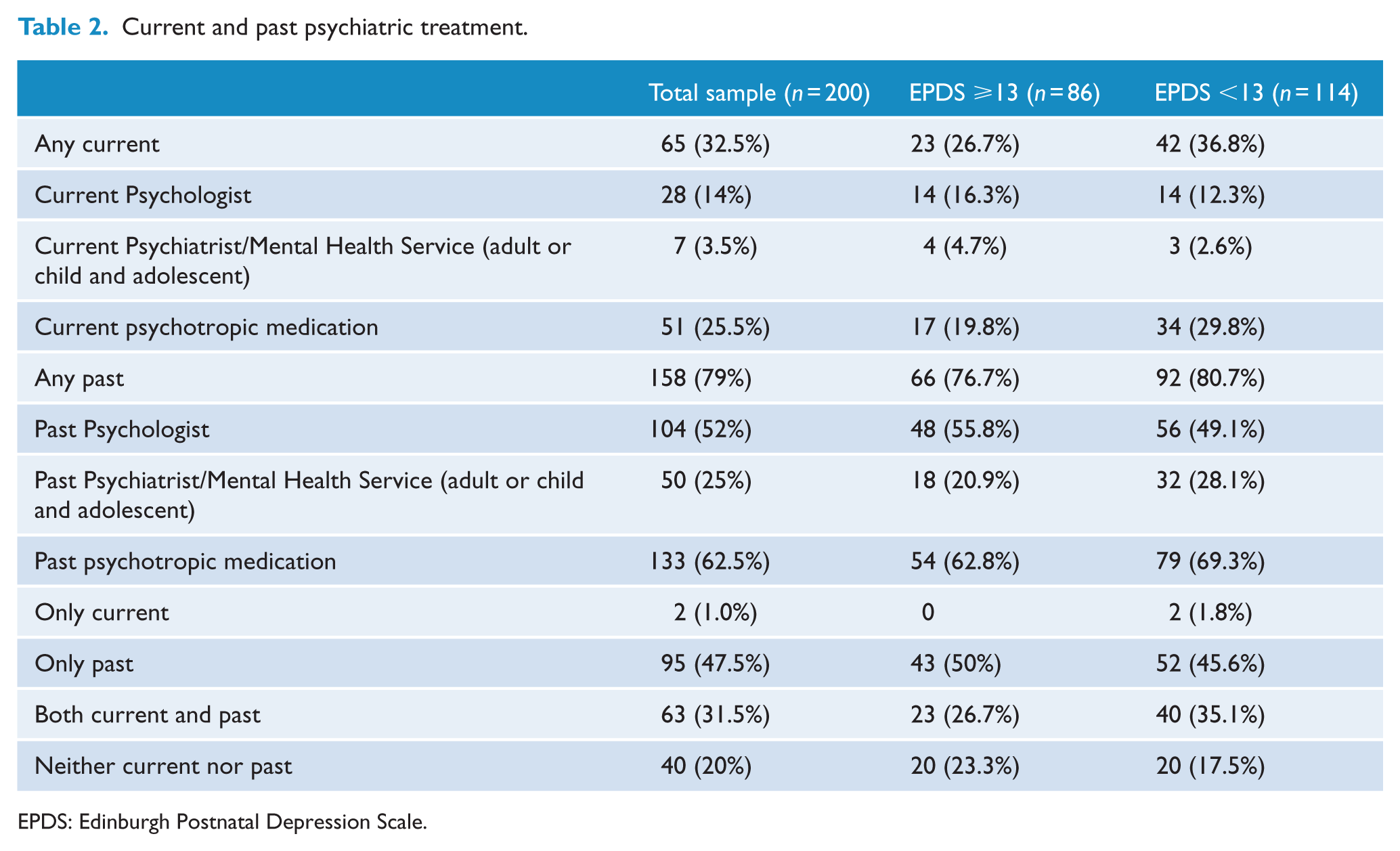
EPDS: Edinburgh Postnatal Depression Scale.
Reasons for referral and diagnoses of women scoring above cut-off on the EPDS
Reasons for referral of those who scored above and below cut-off are shown in Table 3. Frequently, more than one reason was given and for those who scored 13 or more on the EPDS, an additional reason for referral was often identified, most commonly a past history of anxiety or depression, current symptoms of anxiety or depression or ‘social issues’.
Reasons for referral.
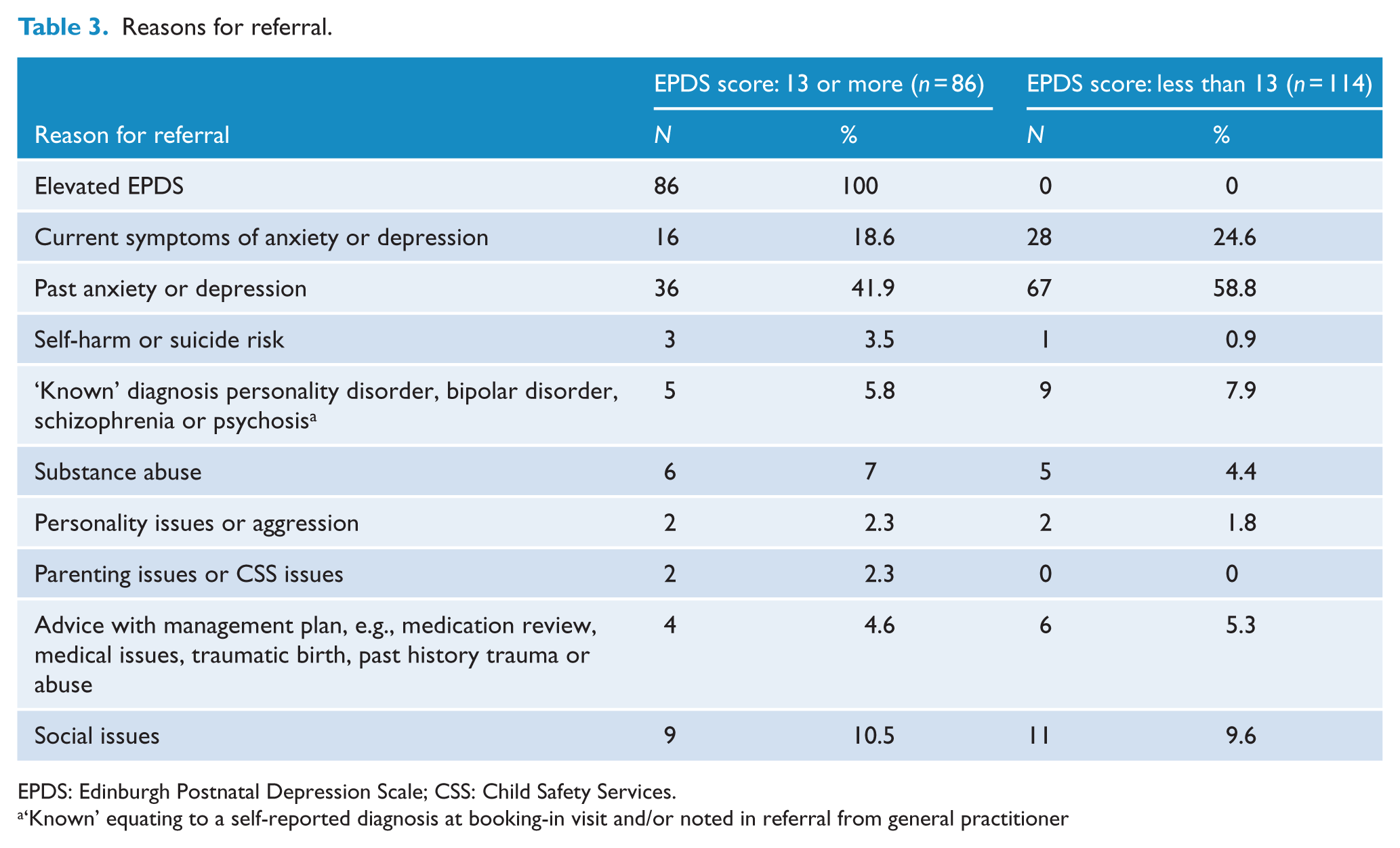
EPDS: Edinburgh Postnatal Depression Scale; CSS: Child Safety Services.
‘Known’ equating to a self-reported diagnosis at booking-in visit and/or noted in referral from general practitioner
Table 4 provides a breakdown of the diagnoses made, as per the DSM-5, for those who scored above and below cut-off on the EPDS. Of note, comorbidity was common. Women with a diagnosis of anxiety or depression were divided into two groups – those with ‘adequately treated’ anxiety or depression, i.e., no change to medication dosage or referral for psychological treatment deemed necessary, and those with ‘untreated’ depression or anxiety, i.e., nil or inadequate current treatment.
Diagnostic categories.
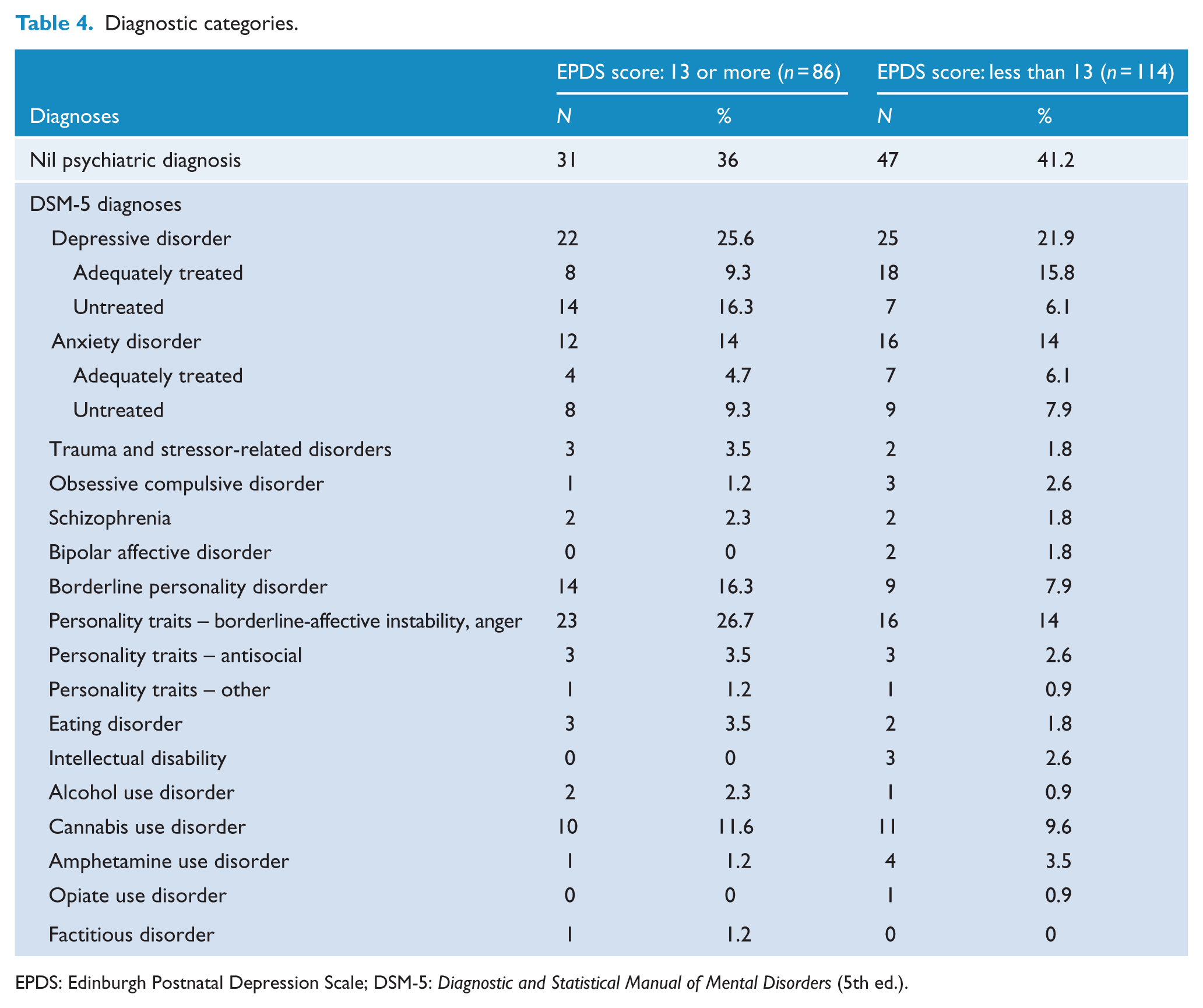
EPDS: Edinburgh Postnatal Depression Scale; DSM-5: Diagnostic and Statistical Manual of Mental Disorders (5th ed.).
Of those who scored above the EPDS cut-off, 12 (14%) had anxiety disorders and 22 (25.6%) had depressive disorders. The numbers with ‘untreated’ disorders were 8 (9.3%) and 14 (16.3%), respectively. Considering the whole sample of 200 who completed the EPDS, this yielded a prevalence of ‘untreated’ depression of 10.5%, a sensitivity for the EPDS of 66% and a specificity of 60% for detection of ‘untreated’ depression.
A range of other psychiatric diagnoses were also made in this group; BPD (n = 14; 16.3%) and substance use disorders (n = 13; 15.1%) were common. Many women also had borderline personality traits (n = 23; 26.7%) sub-threshold for disorder. These were noted in the list of diagnoses if 2 or more traits were present, most commonly these were affective instability and inappropriate intense anger. One woman with BPD and four women with borderline personality traits also had a depressive disorder, and none had a comorbid anxiety disorder. In total, 31 women (36%) who scored 13 or more on the EPDS had no DSM-5 psychiatric disorder.
Of the 114 women who scored below the EPDS cut-off, a high proportion of women (n = 47; 41.2%) had no psychiatric diagnosis, as expected. However, 16 women (14%) had untreated depressive and/or anxiety disorders undetected by the EPDS.
Discussion
At the RHH, only about 50% of all women with an EPDS score above cut-off at their maternity booking-in were seen for psychiatric assessment by the PCLP Team – some declined the offered referral, others subsequently declined the offer of an appointment, or failed to attend scheduled appointments. This is in keeping with poor attendance rates previously reported (Harvey and Pun, 2007; Kim et al., 2010; Reay et al., 2011). The reasons for such low rates of follow-up with a subsequent psychiatric assessment after screening positive are unclear, but issues relating to timing of screening (Austin and Lumley, 2003) and transient distress in pregnancy (Matthey and Agostini, 2017; Matthey and Ross-Hamid, 2012) have been posited. Other possibilities include socioeconomic problems, such as access to, availability and cost of transport, or patient factors, such as disorganisation or stigma, which have been cited by other authors as a possible reason for low attendance (Harvey and Pun, 2007).
The characteristics of the sample described here are noteworthy. A large number of women were without a partner and two-thirds of pregnancies were unplanned, which is higher than the national average of 51% (Children by Choice Association Incorporated, 2017). There were high rates of women already receiving psychiatric treatment (32.5%) or having received treatment for their mental health in the past (79%) and high rates of previous CSS involvement. These findings may reflect the sample seen, (i.e., all were public hospital patients) and/or socio-demographic features of some groups of the population in Tasmania. In comparison with the rest of Australia, Tasmanians have higher rates of unemployment, lower incomes and lower literacy and educational attainment (Australian Bureau of Statistics, 2017b; Population Health, 2013). Tasmanians also have some of the highest rates of teenage pregnancy (Australian Bureau of Statistics, 2001) and illicit substance use (Australian Bureau of Statistics, 2017c) in the country. These socio-demographic features are of note, as multiple systems surrounding an individual including social, economic and community values and norms are known to influence development (Bronfenbrenner and Ceci, 1994).
Importantly, we found that screening with the EPDS, using a cut-off of 13 or more in the antenatal population does identify women with untreated or inadequately treated depressive and anxiety disorders. Of those who screened above cut-off, 9.3% had anxiety disorders and 16.3% had depressive disorders, requiring treatment interventions.
However, the specificity of the EPDS in this sample was relatively poor. While antenatal EPDS scores ⩾13 identified a significant number of ‘true positive’ cases (depression not adequately treated), 40% of our sample tested positive for a disorder they did not have. In particular, a large number of women with BPD (16.3%) were identified, and many more were found with borderline personality traits (26.7%). Of note, only five of those with these personality diagnoses also had a diagnosis of a depressive disorder.
These findings here are in marked contrast to other studies examining characteristics of women who score 13 or more on the EPDS in the antenatal period. As Lydsdottir et al. (2014) used the MINI-Plus, they were not able to detect BPD. However, they found a high rate of bipolar disorder (13%) in their screen-positive sample, which may reflect self-selection of women with the disorder into the study, or perhaps some of these women may have had emotional dysregulation more in keeping with borderline personality pathology which was misclassified as bipolar disorder. Harvey and Pun’s (2007) study did include clinical diagnostic interviews, but only identified BPD in one woman and, as in this study, found no cases of bipolar disorder in their screen-positive sample. However, the sample examined was not comparable with the one described here, as patients were included in the study only if the EPDS score was the ‘reason for referral’ – those women referred because they had current or past depression or psychiatric symptoms at the time of midwifery assessment were excluded.
The apparent failure of the EPDS to adequately distinguish between depression and BPD or those with significant borderline personality traits is a significant clinical issue as the distinction between these two disorders has important implications. The recommended treatments for these disorders are distinct and different. So too are the potential negative impacts on obstetric and neonatal outcomes, and the longer term effects on children. Importantly, BPD has also been associated with greater likelihood of teenage pregnancy and unplanned pregnancies (De Genna et al., 2012).
Using a retrospective cohort study, which included 989 births to women with BPD, Pare-Miron et al. (2016) identified a greater risk of a range of adverse obstetric and neonatal outcomes in women with BPD compared to those without this diagnosis. Women with BPD were more likely to be overweight, have lower median household incomes, to smoke and to consume illicit drugs and alcohol. Women with BPD had a greater risk of obstetric complications including pre-eclampsia, gestational diabetes and placental abruption. They also had higher rates of neonatal complications including greater risk of preterm birth, growth restriction and intrauterine foetal death.
Women with BPD frequently have a history of early relational trauma, poor attachment relationships and difficulties in emotional regulation and impulse control (Agrawal et al., 2004; American Psychiatric Association, 2013; Fonagy and Target, 1997). Thus, these women have been identified as likely to have difficulties in fulfilling their parenting role and in promoting secure attachment with their children (Newman and Stevenson, 2005). Studies have identified a range of parenting behaviours which are seen more commonly in mothers with BPD including insensitive, overprotective and hostile parenting (Eyden et al., 2016; Newman et al., 2007). These behaviours have led to women with BPD being identified as ‘high-risk’ caregivers, i.e., caregivers at risk of traumatising interactions with their children (Judd et al., 2018; Newman et al., 2015). Adverse outcomes identified in children have included internalising and externalising problems, insecure attachment patterns and emotional dysregulation (Eyden et al., 2016).
Sved Williams (2018) notes there are no prospective studies regarding the prevalence of BPD in antenatal clinics. The data reported here suggest this diagnosis is not uncommon among women who report distress or symptoms of mood disturbance and thus have elevated scores on the EPDS. Clinical Practice Guidelines note the importance of further assessment for all women who score 13 or more on the EPDS. Our findings suggest that this assessment should be made by a clinician able to identify personality pathology and organise appropriate interventions. While acknowledging that the type of further assessment will of necessity vary according to the setting, and the access to services available in the area (Austin et al., 2017), we suggest that psychiatric assessment should be undertaken if possible in order to differentiate women with BPD from those with a depressive disorder. Early identification of women with BPD is key to assisting women to access services where appropriate interventions can reduce the risk of trauma and maltreatment of their children and provide a means of breaking the transgenerational cycle of development of severe personality disturbance (Judd et al., 2018; Sved Williams, 2017).
Strengths and limitations
This study was conducted in a health service which includes both public general health and mental health services for all of Southern Tasmania. This enabled comprehensive review of the past psychiatric history of any woman referred for assessment by the PCLP Team. In addition, women were generally seen for more than a single assessment interview, many were seen over several months, enabling ongoing review of the diagnosis made. The major limitations of the study are that the study population was a convenience sample and that diagnoses were not made using operational definitions or a structured clinical interview for personality disorders, but by clinical interview, and interviewer bias cannot be excluded. However, to some extent, the latter is mitigated by the strengths described above.
Conclusion
Psychiatric assessment of women who scored 13 or more on the EPDS at routine antenatal screening identified a significant number with BPD or borderline personality traits rather than depressive or anxiety disorders. Early identification of women with these personality difficulties is essential to enable interventions designed to reduce the potential negative impact of BPD on obstetric and neonatal outcomes and long-term effects on children.
Footnotes
Acknowledgements
The authors thank Drs Anisha Grover, Daya Sadiq and Kishor Sivasankaran for assistance with psychiatric assessment of women in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Psychiatry trainee S.L. received financial support for data analyses initially undertaken for the RANZCP Consultation-Liaison Scholarly Project through the Specialist Training Programme: Training more Specialist Doctors in Tasmania.