
Abstract
Objective:
Identifying women at risk of depression and anxiety during pregnancy provides an opportunity to improve health outcomes for women and their children. One barrier to screening is the availability of validated measures in the woman’s language. Afghanistan is one of the largest source countries for refugees yet there is no validated measure in Dari to screen for symptoms of perinatal depression and anxiety. The aim of this study was to assess the screening properties of a Dari translation of the Edinburgh Postnatal Depression Scale.
Methods:
This cross-sectional study administered the Edinburgh Postnatal Depression Scale Dari version to 52 Dari-speaking women at a public pregnancy clinic in Melbourne, Australia. A clinical interview using the depressive and anxiety disorders modules from the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders (5th ed.) was also conducted. Interview material was presented to an expert panel to achieve consensus diagnoses. The interview and diagnostic process was undertaken blind to Edinburgh Postnatal Depression Scale screening results.
Results:
Cronbach’s alpha coefficient for the Edinburgh Postnatal Depression Scale Dari version was good (α = 0.79). Criterion validity was assessed using the receiver operating characteristics curve and generated excellent classification accuracy for depression diagnosis (0.90; 95% confidence interval [0.82, 0.99]) and for anxiety diagnosis (0.94; 95% confidence interval [0.88, 1.00]). For depression, a cut-off score of 9, as recommended for culturally and linguistically diverse groups, demonstrated high sensitivity (1.00; 95% confidence interval [0.79, 1.00]) and specificity (0.88; 95% confidence interval [0.73, 0.97]). For anxiety, a cut-off score of ⩾5 provided the best balance of sensitivity (1.00; 95% confidence interval [0.72, 1.00]) and specificity (0.80; 95% confidence interval [0.65, 0.91]).
Conclusion:
These results support the use of this Edinburgh Postnatal Depression Scale Dari version to screen for symptoms of depression and anxiety during pregnancy as well as the use of a lowered cut-off score.
Introduction
Pregnancy can be a time of increased risk for developing or re-experiencing mental illnesses, most commonly depression and anxiety (Smith et al., 2011). Depression during pregnancy is associated with poor birth outcomes such as premature birth, low birth weight and low Apgar score, which is a measure of newborn health (Marcus, 2009; Räisänen et al., 2014). Maternal mental health conditions can impact family functioning and disrupt crucial mother–child attachment, affecting infant and later child development and behaviour (Austin et al., 2011; Śliwerski et al., 2020). There is also substantial financial burden associated with perinatal depression and anxiety. Long-term costs, which include health care expenses, losses to well-being, productivity and intergenerational impact, have been assessed at $5.2 billion (Pricewaterhouse Coopers Ltd., 2019) in Australia and £8.1 billion in the United Kingdom (Bauer et al., 2014). Given depression during pregnancy has been identified as one of the strongest risk factors for developing postpartum depression (O’Hara and Wisner, 2014), the need for mental health screening during this period is critical, particularly as it has been shown to increase referrals and service usage (Reilly et al., 2020).
The perinatal period can be defined as including the antenatal period (conception through to birth) and the first 12 months following birth (Austin et al., 2011). Prevalence of perinatal depression and anxiety varies across countries, with high co-morbidity between these two disorders (Austin et al., 2010). In high-income countries, perinatal depression is reported to affect between 8.5% and 12.9% of women and anxiety 12.3% and 13.0% of women (Gavin et al., 2005; Howard et al., 2014). A systematic review of 40 studies assessing perinatal depression in women living in low- and middle-income countries reported a pooled prevalence of 31% for any depressive disorder (Fellmeth et al., 2017), which is more than double the reported rate in high-income countries. This systematic review also highlighted a paucity of studies on perinatal anxiety disorders, which are an important consideration for pregnancy care, particularly with traumatised populations, as it can impact foetal development and neonatal outcomes (Dayan et al., 2002).
Women of refugee background are at even higher risk of perinatal mental health disorders due to refugee experiences such as exposure to violence, trauma, displacement, and postmigration stressors such as poverty and social isolation (Collins et al., 2011). Accessing antenatal care in pregnancy can often be the first regular contact with the host nation’s health system, making antenatal services a key opportunity to provide for mental health needs and other social needs (Yelland et al., 2014). It is vital that maternity services acknowledge the impact of refugee experiences on pregnancy and the challenges that women of refugee background face as they adapt to parenthood within the context of a new culture and often without support from family (Rogers et al., 2020). Clinical guidelines recommend mental health screening in pregnancy for all women (Austin et al., 2017; NICE, 2018); however, screening remains a common gap in the implementation of best-practice pregnancy care (Yelland et al., 2009). The gap is likely to be even larger for women of refugee background not only due to issues of low health literacy, availability of interpreters, cross-cultural limitations of Western medical models and stigma regarding disclosure of mental illness, but also a lack of access to translated and validated screening measures (Nithianandan et al., 2016).
The enduring conflict in Afghanistan has resulted in one of the largest refugee populations globally, second only to the Syrian Arab Republic (UNHCR, 2019). A combination of prolonged exposure to conflict and a lack of mental health care provision within Afghanistan has seen an increase in the risk of mental illnesses for this population, specifically depression and Posttraumatic Stress Disorder (PTSD; Alemi et al., 2014). Refugees and asylum seekers from Afghanistan continue to resettle across many countries, including Iran, Pakistan, United States and Australia (Alemi and Stempel, 2018). To date, the Dari version of the Edinburgh Postnatal Depression Scale (EPDS) (Cox et al., 1987), one of the most widely used depression and anxiety screening measures during pregnancy, has not been validated against clinical diagnosis. There is a clear need for the availability of culturally specific perinatal mental health screening measures.
The EPDS has been validated for use during pregnancy and translated into a number of different languages (Ing et al., 2017; Kheirabadi et al., 2012). The English version of the EPDS, when administered during pregnancy, performs with moderate sensitivity (0.76–0.88) and high specificity (0.88–0.92) (Austin et al., 2017). However, its psychometric properties vary across translations and settings, with the variability in performance attributed to the use of different cut-off scores and varying translation standards. A review comparing seven screening measures reported that the EPDS was the most suitable perinatal depression screening tool, particularly in low-resource settings, due to its superior level of sensitivity (Chorwe-Sungani and Chipps, 2017).
Optimal cut-off points for the EPDS, which balance sensitivity and specificity, are required in order to accurately identify women at risk of depression and anxiety across different populations. When administering the English version of the EPDS, the recommended cut-off score for use is ⩾15 during the antenatal period and ⩾13 during the postpartum period (Matthey et al., 2006). When screening women from other cultures and non-English-speaking backgrounds, a lower cut-off score of ⩾9 is recommended in order to account for language and cultural differences that may reduce the specificity of the measure (Austin et al., 2011). The EPDS also provides a sub-scale score for symptoms of anxiety. This can be calculated from items 3, 4 and 5. A study by Swalm et al. (2010) reported that a cut-off score of 4 or more was optimum in capturing the top quartile of scores in a large sample of Australian pregnant women.
The objective of the present study was to investigate the screening properties of the EPDS with a sample of Dari-speaking women seeking antenatal care. This study assesses the ability of the EPDS to detect depressive and anxiety disorders in this population of women of refugee background.
Methods
Setting
This cross-sectional study was conducted at a public antenatal clinic at one of Australia’s largest health services. This health service provides health care in one of the most culturally diverse localities in Australia (over 100 languages spoken), including a large Dari-speaking population (City of Greater Dandenong, 2018). One day per week, the clinic operates as a designated refugee antenatal clinic. Women are allocated to this clinic following referral from their general practitioner (GP) for maternity care based on availability and preference. All women attending the service completed the EPDS as part of their standard maternity care.
Participants and recruitment
Participants were recruited between July 2016 and November 2018. Permission was granted by the health service to approach women identified from clinic appointment lists if Dari was listed as their preferred language. A few days prior to their scheduled appointment, a member of the research team (R.B.) phoned the women, with the assistance of a female interpreter experienced in health care. Women were asked to participate in a one-on-one interview to discuss their emotional health during pregnancy and to talk about their experience of arriving in Australia. The interviews were booked on the same day as their clinic appointment. Women aged 18 years and over; currently pregnant; and arrived to Australia on a humanitarian visa, asylum seeker or spousal visa were invited to attend. Women presenting with an acute psychotic episode, intellectual impairment or any serious complications with their pregnancy resulting in termination were excluded from participating in this study.
Measures
EPDS
The EPDS is a 10-item, self-report questionnaire used to detect symptoms of depression and anxiety. Each item uses a 4-point Likert-type response scale, ranging from 0 to 3, asking women to rate how they have been feeling over the past 7 days. The final item (item 10) on the EPDS assesses the risk of self-harm and suicidal ideation.
Structured Clinical Interview for DSM-5 Research Version
The Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) Research Version (SCID-5-RV) is a semi-structured interview designed to assess and determine current and lifetime mental health diagnoses in line with internationally recognised diagnostic criteria (DSM-5) (First et al., 2015). It has been used in validation studies with refugee populations (Brink et al., 2015; Ing et al., 2017). It is designed to be administered by a clinician or trained mental health professional with experience of the DSM-5 diagnostic criteria. The Research Version is the most comprehensive of the versions as it contains more disorders than the clinical version. To our knowledge, there is currently no literature available on the psychometric properties of the research version of the SCID-5. However, the clinician version of the SCID-5 is reported to have good diagnostic sensitivity (>0.70) and specificity (>0.80) (Osório et al., 2019). For the purposes of this study, the modules pertaining to depressive and anxiety-related disorders were administered in English with the assistance of interpreters where required. The trauma module was also administered; however, this was part of a separate study.
In addition to the researcher who conducted the interviews (R.B.), two other members of the project team (psychologists; G.M. and K.M.G.) joined with R.B. to form an expert panel to review all clinical interview material for each participant, in order to determine consensus DSM-5 diagnoses. All of these researchers were blind to the screening results of the EPDS.
Adaption and translation
The process used to translate this Dari version was developed and described elsewhere (Shafiei et al., 2015). In summary, Shafiei et al. (2015) reported the English version EPDS was translated into Dari by an accredited professional translator, the translation was then reviewed and discussed by a group of professional translators, bilingual mothers from the community and members of the research team, and then pilot tested. For the purposes of this study, the EPDS Dari version was also back translated.
Procedure
On the day of their appointment, women completed the EPDS in Dari on a tablet device using the digital platform iCOPE, which was developed by the Centre of Perinatal Excellence (COPE, 2019). The iCOPE platform calculates the scores and provides instant reports to both the woman and the health professional. The clinical report provides the item responses, total EPDS score and anxiety sub-scale score, and highlights the response to item 10, which assess for risk of self-harm. A member of the research team experienced in risk assessment provided training to all staff as well as the availability of flowcharts in each clinic room detailing the referral process depending on level of risk. Women completed the EPDS screening in the clinic waiting room. Accredited female interpreters employed by the health service were used if required by the woman.
Following completion of their appointment, women attended an interview with the researcher (R.B.), who was blinded to their EPDS screening scores, in order to complete the SCID-5-RV (American Psychiatric Association, 2013). The researcher (R.B.) is a registered psychologist and had received training in refugee health, trauma and administering the SCID-5-RV. During the interview, the depressive, anxiety and trauma disorder modules were administered, along with the Harvard Trauma Questionnaire (HTQ) (Mollica et al., 1992). Women who received a diagnosis of a current mental illness were offered a referral to a refugee-focussed counselling service or to their GP according to their preference. This study was approved by the Monash Health Human Research Ethics Committee (14475L). Participants provided written informed consent via consent forms translated into Dari. A witness signature was also collected from the interpreter if required to complete the interview. Women were able to end the interview at any time and withdraw their participation without any effect on their maternity care. Women received a $20 gift card for their participation and taxi vouchers, if required. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines (Elm et al., 2007).
Statistical analyses
The total sample was divided into those who received a DSM-5 diagnosis for any current depressive or anxiety disorder and those who did not. The screening efficacy of the EPDS Dari version was then evaluated, using the recommended cut-off score of 9. The effect of increasing the cut-off score to 10 and decreasing to 8 was also investigated, as well as the recommended cut-off score of 13 used in English-speaking populations. For each cut-off, we calculated sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV). Sensitivity is the ability of the EPDS to correctly identify all women with depressive and/or anxiety disorders (Altman and Bland, 1994a). Specificity is the ability of the EPDS to correctly identify all women who do not have depressive or anxiety disorders (Altman and Bland, 1994a). PPV refers to the proportion of women who screen positive on the EPDS and receive a diagnosis of depression or anxiety (Altman and Bland, 1994b). NPV is the proportion of women who screen negative on the EPDS and do not have a current diagnosis of depression or anxiety (Altman and Bland, 1994b). Cronbach’s alpha was calculated to determine the internal consistency of the Dari adaptation of the EPDS. A receiver operating characteristic (ROC) curve was used to assess the accuracy of the EPDS (Metz, 1978; Zweig and Campbell, 1993). Accuracy of the EPDS (proportion of results correctly identified) was estimated by the area under the ROC curve (AUC). Statistical significance was set at p < 0.05, and all analyses were conducted using the DAG_stat spreadsheet designed specifically for the assessment of diagnostic tests (Mackinnon, 2000).
Sample size estimation
A statistical power analysis was performed for sample size estimation based on the expected prevalence of 28% of women of refugee background being diagnosed with a depressive disorder (Collins et al., 2011). With an alpha = 0.5 and power = 0.80, the projected sample size needed was approximately n = 47.
Results
Fifty-two women were interviewed. EPDS screening using the iCOPE digital platform took approximately 6–14 minutes to complete and the interviews lasted between 60 and 90 minutes.
The mean age was 27.56 years (SD 5.196). Forty-four (84.6%) of the interviews were conducted with the assistance of a female interpreter experienced in health care. All 52 women were married or in de facto relationships. Women were assessed between 13 and 39 weeks gestation. Further socio-demographic details of the women are provided in Table 1.
Socio-demographic characteristics of the study population (N = 52).
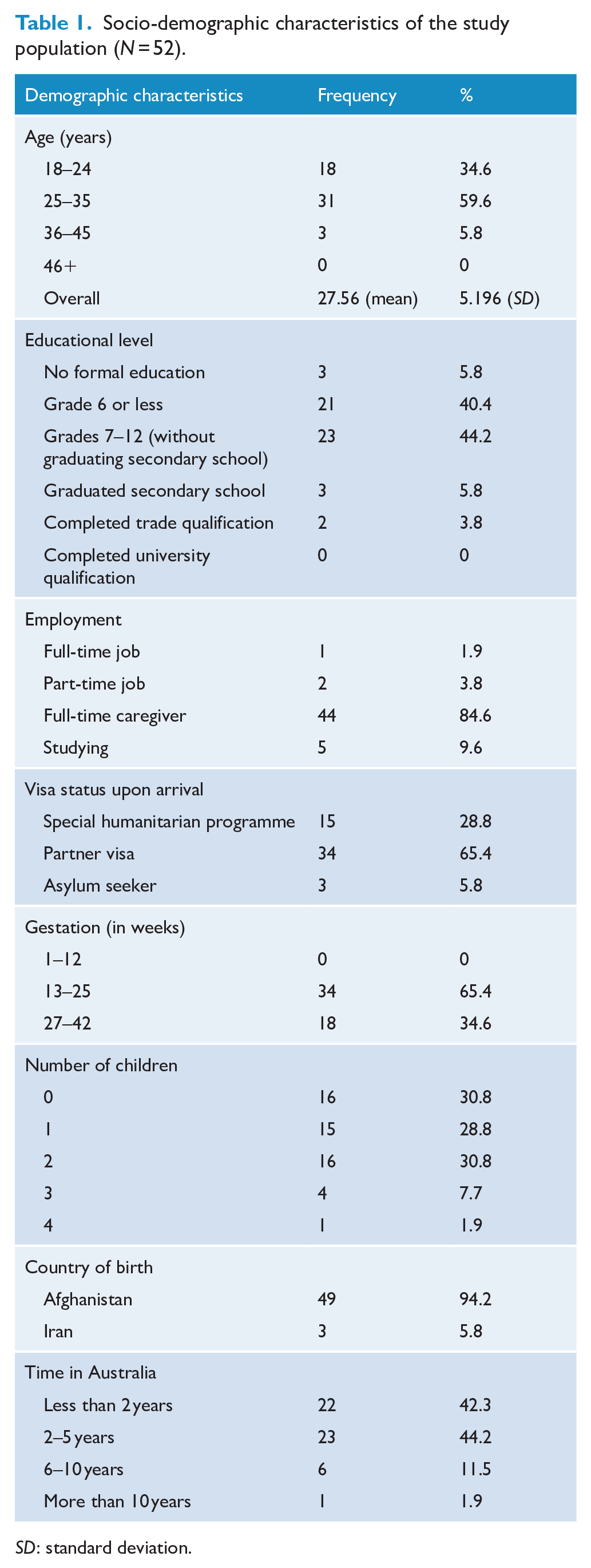
SD: standard deviation.
Seventy-three women were approached in the clinic and 20 (27%) declined to participate. Most women cited lack of time or caring responsibilities as the reason for non-participation, and for three women, their husbands refused their participation. There was no significant difference between mean EPDS scores of the women who participated and those who declined. One woman agreed to participate but was later excluded due to serious medical complications with her pregnancy resulting in termination. There were no dropouts and all interviews were completed.
Screening scores and mental health diagnoses
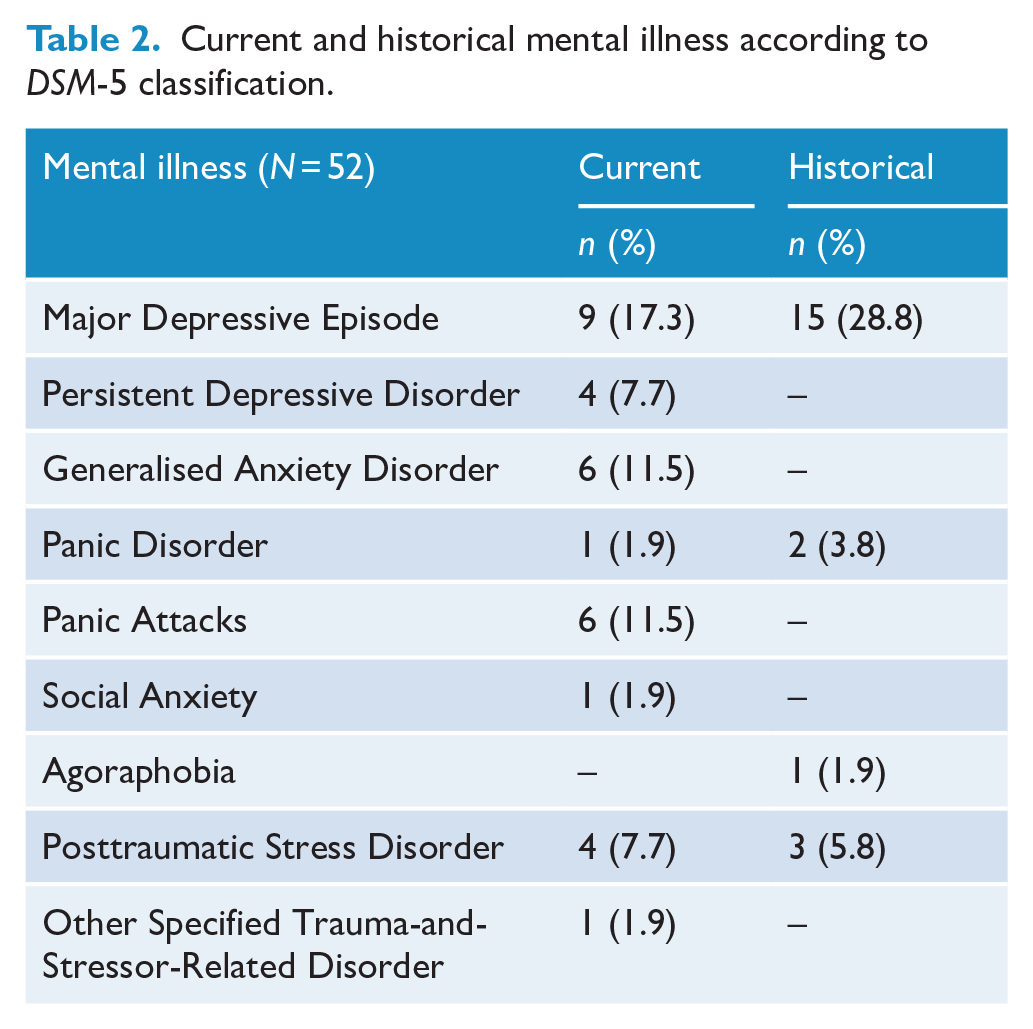
The mean EPDS score of the total sample was 7.04 (SD 5.48). Nine women (17%) responded with either a score of 1 or 2 for item 10 and received a referral for counselling. None of the women responded with a score of 3 for item 10. Eighteen women (34.6%) met criteria for at least one current depressive, anxiety or trauma-related disorder and 28 (53.8%) met criteria for a historical depressive, anxiety or trauma-related disorder. Thirteen women (25%) received a diagnosis of a current depressive episode. The mean score of the EPDS for women diagnosed with a current depressive disorder was 12.77 (SD 2.42) and for women without depression 4.78 (SD 4.78). Eleven women (21%) received a diagnosis of a current anxiety disorder. The mean EPDS anxiety sub-scale score for women diagnosed with an anxiety disorder was 5.82 (SD 0.75) and for women without an anxiety disorder 2.38 (SD 2.17). Eight women received a comorbid diagnosis of depression and anxiety, one woman was diagnosed with Generalised Anxiety Disorder and Panic Disorder, and one woman received a diagnosis of PTSD and depression. Seven women (13.5%) were diagnosed as experiencing episodes of both current and historical mental illness. Table 2 provides a list of current and historical mental illness diagnoses according to the DSM-5 classification.
Current and historical mental illness according to DSM-5 classification.
Internal consistency
The internal consistency of the translated EPDS was assessed using Cronbach’s alpha and the result was α = 0.79. Item-total scale correlations displayed three items with a correlation below 0.40 (see Table 3): item 2 ‘I have looked forward with enjoyment to things’ (0.33), item 7 ‘I have been so unhappy that I have had difficulty sleeping’ (0.365) and item 10 ‘the thought of harming myself has occurred to me’ (0.233).
Internal consistency (Cronbach’s α) of the Dari translation of the EPDS.
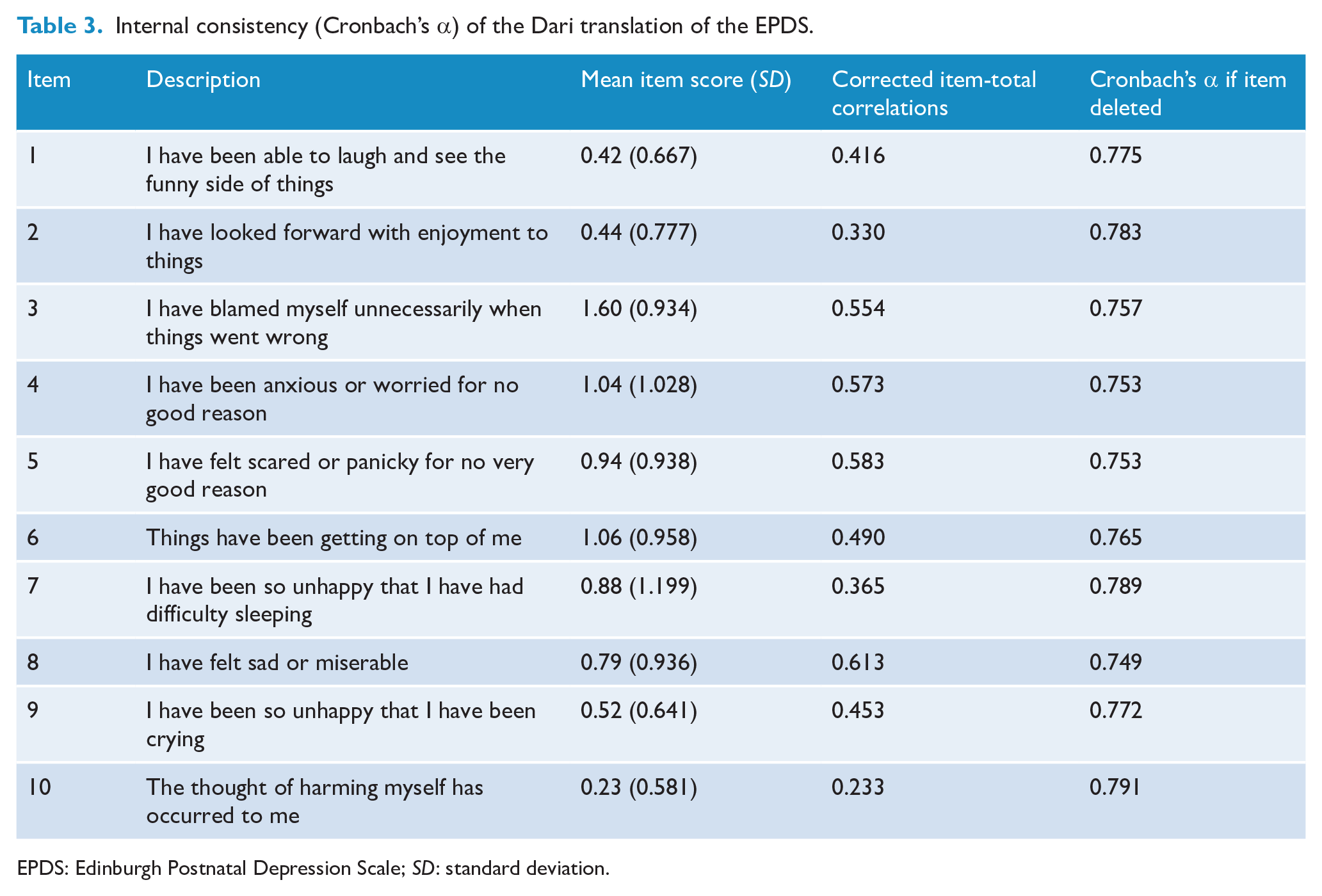
EPDS: Edinburgh Postnatal Depression Scale; SD: standard deviation.
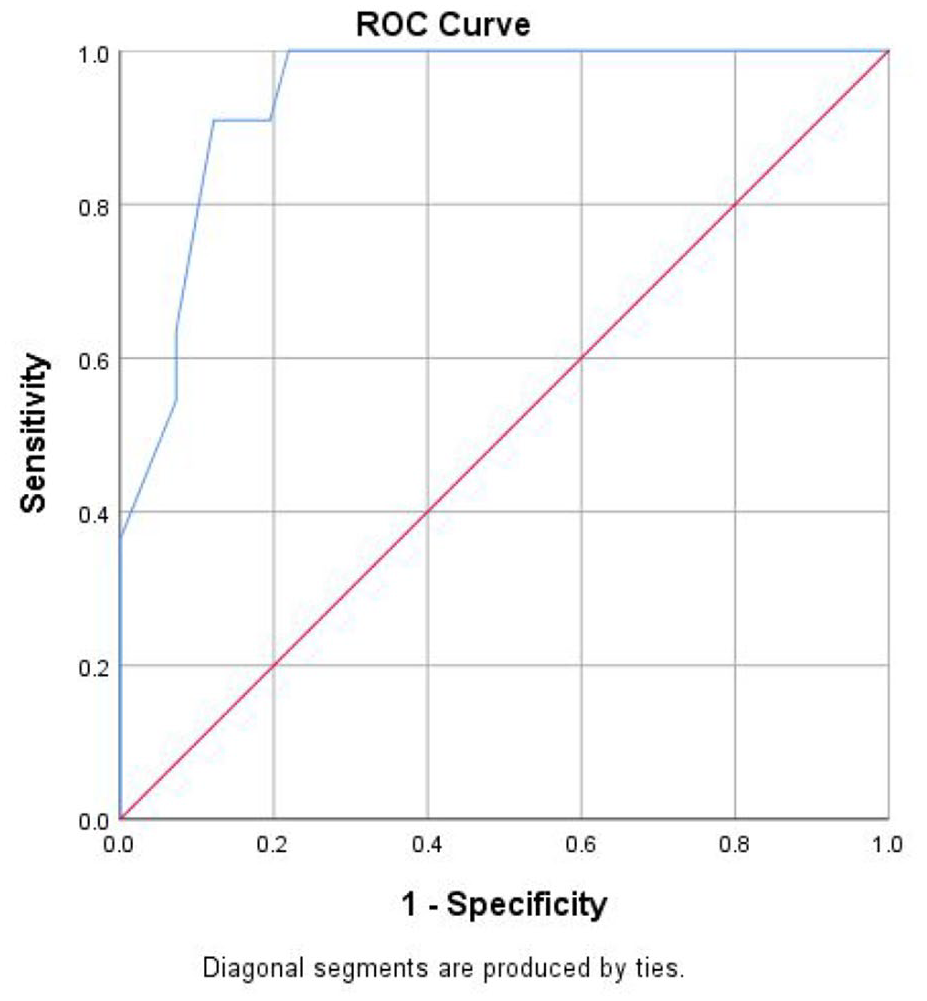
A ROC curve analysis was used to assess the diagnostic ability of the EPDS for both current depression and current anxiety diagnosis. Accuracy of the EPDS is estimated by the AUC. The AUC for the EPDS and current depression diagnosis was 0.90 (95% confidence interval [CI] [0.82, 0.99]) and for current anxiety diagnosis 0.94 (95% CI [0.88, 1.00]). For both depression and anxiety, the AUC was close to 1, indicating high discriminative power of the EPDS. Figure 1 presents the ROC plot for the EPDS and current depression diagnosis and Figure 2 presents the ROC plot for the EPDS and current anxiety diagnosis.
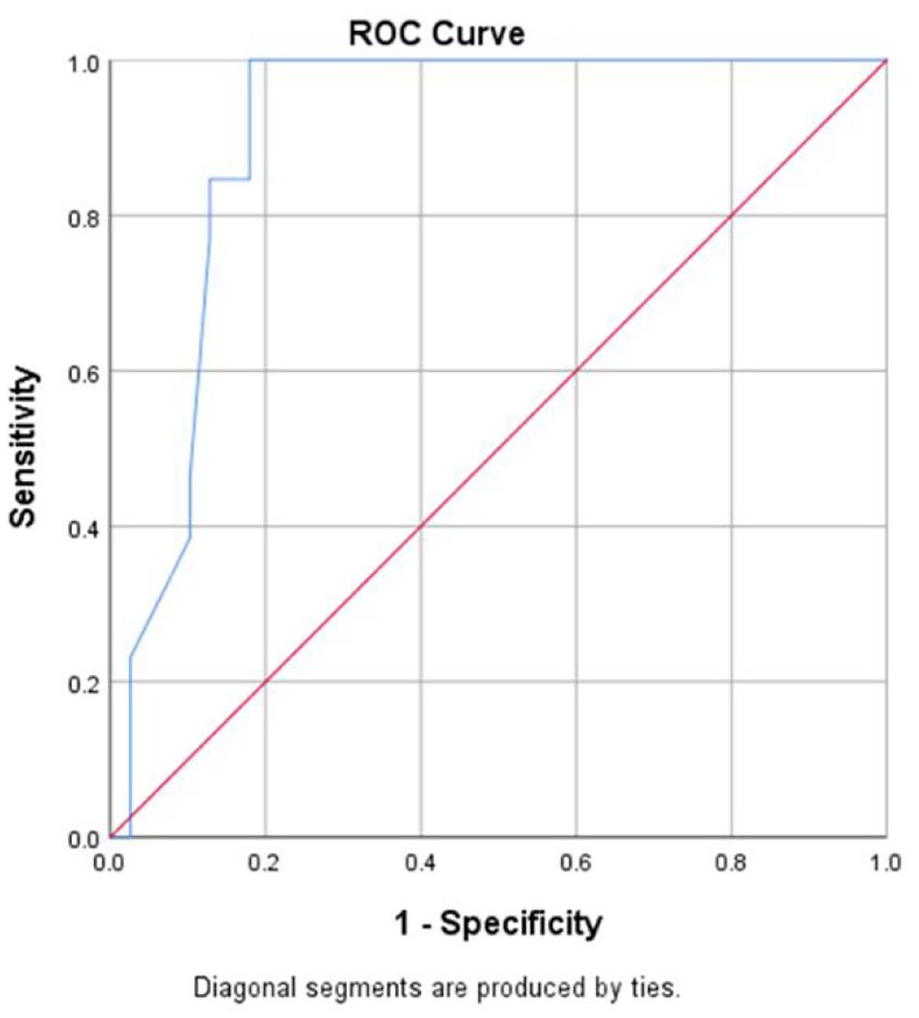
Receiver Operating Characteristic (ROC) plot for the EPDS and current depression diagnosis.
Receiver Operating Characteristic (ROC) plot for the EPDS and current anxiety diagnosis.
Screening efficacy
The sensitivity, specificity and predictive values of the EPDS Dari version are presented in Tables 4 and 5. Using the cut-off score of ⩾8, 24 women screened positive on the EPDS while 28 screened negative. Of those who screened positive, 16 (67%) received a diagnosis of either current depression or anxiety, while 8 (33%) did not. This resulted in a sensitivity of 1.00 (95% CI [0.79, 1.00]) and a specificity of 0.78 (95% CI [0.61, 0.90]).
EPDS cut-off scores and screening efficacy for the diagnosis of DSM-5 current depressive illness.
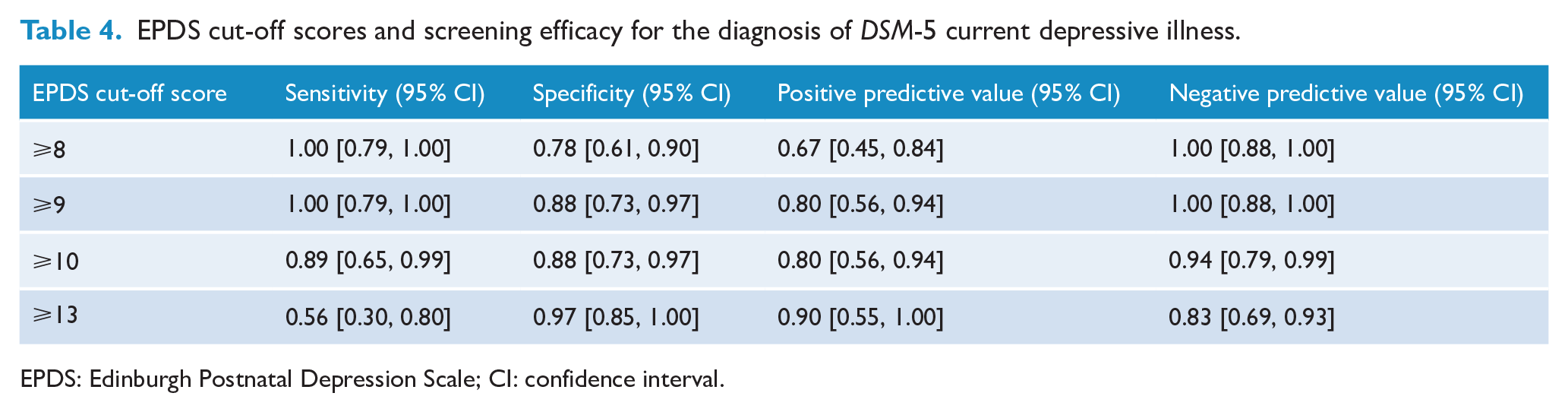
EPDS: Edinburgh Postnatal Depression Scale; CI: confidence interval.
EPDS cut-off scores and screening efficacy for the diagnosis of DSM-5 current anxiety disorders.
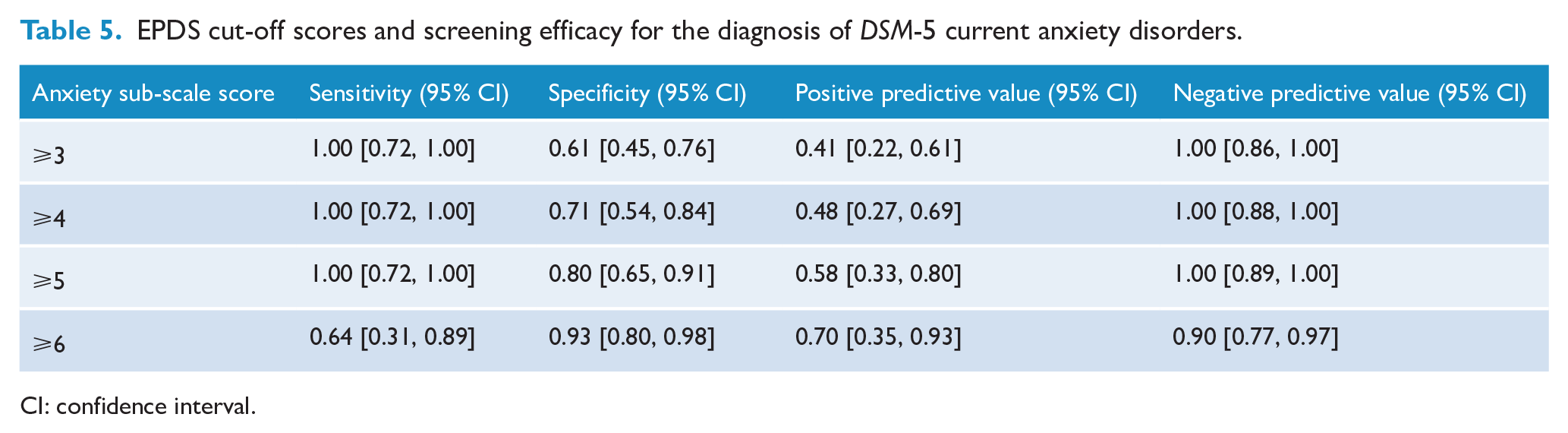
CI: confidence interval.
Using the recommended cut-off score of ⩾9, 20 women screened positive on the EPDS while 32 screened negative. Of those who screened positive, 16 (80%) received a diagnosis of either current depression or anxiety, while 4 (25%) did not. This resulted in a sensitivity of 1.00 (95% CI [0.79, 1.00]) and specificity of 0.89 (95% CI [0.74, 0.97]). Increasing the cut-off score to ⩾10 resulted in 20 women screened positive on the EPDS while 32 screened negative. Of those who screened positive, 16 (80%) received a diagnosis of either current depression or anxiety, while 4 (20%) did not. Of those who screened negative, two (6.25%) women received a diagnosis of current depression. This resulted in a sensitivity of 0.89 (95% CI [0.65, 0.99]) and specificity of 0.88 (95% CI [0.73, 0.97]).
Using the cut-off score of ⩾13, 10 women screened positive on the EPDS while 42 screened negative. Of those who screened positive, nine (90%) received a diagnosis of either depression or anxiety, while one (10%) did not. Of those who screened negative, seven (17%) received a diagnosis of depression or anxiety. This resulted in a sensitivity of 0.56 (95% CI [0.30, 0.80]) and a specificity of 0.97 (95% CI [0.85, 1.00]).
The sensitivity, specificity and the predictive values of the anxiety sub-scale score in accurately detecting those diagnosed with an anxiety disorder are presented in Table 5. The cut-off score of ⩾5 provided the optimum balance of sensitivity and specificity.
Discussion
The objective of the present study was to investigate the screening properties of the EPDS with a sample of Dari-speaking women and its ability to determine the presence of depression and anxiety in women of refugee background seeking antenatal care. This paper presents the psychometric properties of a commonly used screening measure, the EPDS, with a Dari-speaking population of women of refugee background. To the best of our knowledge, this is the first study to investigate the clinical utility of administering the EPDS for screening during pregnancy with Dari-speaking women.
Overall, the internal consistency as measured by the Cronbach’s alpha coefficient was good (α = 0.79). However, the results of this study raised some issues with the performance of a few items on the EPDS; items 2, 7 and 10. Item 2 asks whether respondents ‘have looked forward with enjoyment to things’; item 7 asks whether the respondent has been ‘so unhappy they have had difficulty sleeping’; and item 10 assesses risk of self-harm and suicide, which is critical in determining the need for an acute referral. It could be speculated that issues with translating may have resulted in the poor performance of these items. Poorer performing items are an important consideration for health professionals when administering this translated version of the EPDS. Understanding cultural sensitivities and translation difficulties with particular items may require additional clinical judgement and further discussion with the woman during screening. Future research could investigate whether the wording used for these items on the EPDS could be altered in order to improve cross-cultural use.
The Dari translation of the EPDS has shown favourable sensitivity and specificity characteristics in its ability to detect both depression and anxiety. The results from the comparison of cut-off scores support the use of the lowered cut-off score of ⩾9, which is recommended for culturally and linguistically diverse groups, when using the EPDS to screen for depression. At this cut off, the measure demonstrated high sensitivity 1.00 (95% CI [0.79, 1.00]) and specificity 0.88 (95% CI [0.73, 0.97]). Recommended cut-off scores vary across translations, settings and timing. The Persian and Arabic versions of the EPDS recommend a cut-off score of 12/13 (Mazhari and Nakhaee, 2007 ; Naja et al., 2019). However, both of these translations were administered postpartum and to non-refugee populations. A validation study of the EPDS in Karen and Burmese with women of refugee background reported recommended cut-off scores of ⩾10 (Ing et al., 2017). When using the EPDS to screen for anxiety, a cut-off score of ⩾4 has been suggested for English-speaking women (Swalm et al., 2010). Based on the results of this study, when using the EPDS to screen for anxiety disorders, a cut-off score of ⩾5 provided the best balance of sensitivity 1.00 (95% CI [0.72, 1.00]) and specificity 0.80 (95% CI [0.65, 0.91]).
A systematic review of the evidence on the validity of the EPDS in detecting perinatal depression reported noticeable variability between the 37 included studies with a range of 0.34–1.00 for sensitivity and 0.44–1.00 for specificity (Gibson et al., 2009). This variability was mostly attributable to differences in language, populations sampled, diagnostic measures and methods, and study methodology (Gibson et al., 2009). The performance of this Dari version of the EPDS is similar to other translations of the EPDS for languages from refugee source countries. In detecting depression, using the lowered cut-off score of ⩾9, the Burmese version reports a sensitivity of 1.00 and specificity of 0.95 and the Karen version reports a sensitivity of 1.00 and specificity of 0.98 (Ing et al., 2017).
Applying the best cut-off score during administration is vital in optimally identifying women at risk of depression and anxiety. In our study, the previously recommended cut-off score of ⩾9 produced the best balance of sensitivity, specificity and predictive values. Applying the cut-off score of ⩾13, recommended for the general population, resulted in a concerning number of false negatives. This has serious implications for how mental health screening is implemented in clinical practice. Applying one cut-off score across a multicultural service population may limit the efficacy of mental health screening programmes during pregnancy, highlighting the importance of the use of culturally specific cut-off scores. Without applying appropriate cut-off scores, women who require treatment may not be identified or offered the necessary intervention, which is likely to result in a worsening of prognosis.
The importance of having a validated Dari version of the EPDS is supported by the high proportion of women in this study who met DSM-5 criteria for a current depressive or anxiety disorder. These results are consistent with the current body of literature which suggests that perinatal depression and anxiety are more prevalent in women of refugee background compared to women from general populations (Fellmeth et al., 2017). With the continued increase in global numbers of refugees, combined with the specific vulnerabilities faced by these women during pregnancy, there is a need to develop and implement perinatal mental health screening programmes which can be delivered across a range of health care settings and to populations experiencing adversity. Given the impact of perinatal depression and anxiety on pregnancy health, birth outcomes and mother–infant bonding, it is critical that health-equity in perinatal care is prioritised so that women of refugee background can receive appropriate screening in order to provide early management and treatment of symptoms. Elements of trauma-informed practice should be integrated into models of pregnancy care for those health services in areas of refugee resettlement.
In order to best provide for the specific health needs of resettled women of refugee background, it is vital that health services be able to correctly identify these women. More than half of the women who participated in this study arrived to Australia on a partner visa. At the time of booking clinic appointments, these women were not identified as formal refugees and were selected for the study based on their language preference. Throughout the clinical interviews, it became very apparent that all of these women had experienced exposure to potentially traumatic events, grief, conflict, isolation and extreme poverty; common hallmarks of refugee experiences. Even in high-income host nations, most health services do not have access to immigration data and therefore country of birth is often the only way of identifying those individuals who may have been exposed to the stressors of forced displacement (Gibson-Helm et al., 2014). This highlights the issues surrounding the identification and formal recognition of women of refugee background which is crucial if health services are to adequately manage the increased risks to mental health problems for this population of women, particularly during pregnancy.
This study has several strengths worthy of note. First, a standardised clinical interview was conducted, and consensus diagnosis approach by a panel of experienced psychologists and researchers was used to determine diagnoses. Second, this process was conducted blind to the EPDS scores. The EPDS screening scores were compared to consensus clinical diagnosis according to DSM-5 criteria. We were also able to report the number of women who declined to participate in the study, along with a comparison of their mean EPDS scores. Few validation studies within the EPDS literature have reported participation rates (Smith-Nielsen et al., 2018). Despite these strengths, there are some limitations. Even though the cohort of women came from one of Australia’s largest maternity services, which serves a substantial migrant and refugee population, recruitment occurred at one clinic only. This may limit the generalisability to the whole population of Dari-speaking women. Finally, although the DSM-5 has made attempts to enhance cultural validity and incorporate cultural aspects of symptom presentation, it is still a framework of mental illness that has been developed within a Western population, resulting in limitations when applied cross-culturally. The EPDS was originally developed with a population of English-speaking women from the United Kingdom and although translated into many languages and validated, it was not developed specifically for refugee populations or cross-cultural use.
The EPDS Dari version is a valid and reliable screening instrument for detecting women at risk of depression and anxiety during pregnancy. It should be noted, however, that there are some poorer performing items; items 2 and 7, which may have implications for clinical practice, and particularly item 10 which assesses risk of self-harm. Importantly, these results further support the use of a lowered overall cut-off score (⩾9) and consideration of an anxiety sub-scale cut-off score of ⩾5 when screening this population of women.
Perinatal health services provide an opportune setting to screen pregnant women who might be at risk of depression or anxiety. If screening can be provided with simple and validated measures, such as the EDPS, then a major barrier to improving access to mental health care will be addressed. Perinatal mental health screening has been shown to be acceptable and supported by women of refugee background (Willey et al., 2020). Providing appropriate and timely intervention during this period of vulnerability, particularly for women of refugee background, has the potential to not only improve mental health and birth outcomes, but to also have a long-term positive impact across generations.
Footnotes
Acknowledgements
We would like to thank all the women who participated in this research project for providing their time and invaluable input.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M.G.-H. and J.A.B. are supported by fellowships from the National Health and Medical Research Council. R.B. is supported by scholarships from Australian Rotary Health, Windermere Foundation, and Monash Centre for Health Research and Implementation (MCHRI).