
Abstract
Objective:
Understanding the pathways to care for migrants experiencing a first episode of psychosis is important, as they are more likely to experience longer delays to treatment and negative experiences, such as involuntary treatment. Despite the increased risk of developing a psychotic illness and barriers associated with pathways to care, there are limited studies exploring pathways to care in migrants in Australia. This study seeks to examine pathways to care for young people with a first episode of psychosis to a publicly funded youth mental health service.
Methods:
This study included all young people aged 15–24 years who presented with a first episode of psychosis to the Early Psychosis Prevention and Intervention Centre (EPPIC) between 1 February 2011 and 31 December 2016. Referral sources and place of birth were recorded at the time of presentation. The severity of psychotic symptoms was rated at baseline.
Results:
A total of 1220 young people presented with a first episode of psychosis during the study period, including 293 (24.5%) first-generation migrants. First-generation migrants with a first episode of psychosis were more likely to be admitted to hospital than Australian-born youth (odds ratio = 1.67, 95% confidence interval = [1.27, 2.18], p < 0.001) and this remained significant when controlled for demographic (adjusted odds ratio = 1.41, 95% confidence interval = [1.07, 1.88], p = 0.016) and clinical factors (adjusted odds ratio = 1.38,95% confidence interval = [1.01, 1.89], p = 0.044). First-generation migrants were also more likely to have an involuntary admission (odds ratio = 1.67, 95% confidence interval = [1.26, 2.21], p < 0.001) and this remained significant when controlled for demographic (adjusted odds ratio = 1.42, 95% confidence interval = [1.05, 1.91], p = 0.022) and clinical factors (adjusted odds ratio = 1.50, 95% confidence interval = [1.08, 2.09], p = 0.017). Migrants had more severe delusions (p = 0.005), bizarre behavior (p < 0.001) and positive formal thought disorder (p = 0.003) at the time of presentation. Migrants were also more likely to attend the emergency department during their presentation with first episode of psychosis (odds ratio = 1.76, 95% confidence interval = [1.31, 2.36], p < 0.001).
Conclusion:
First-generation migrants who develop a psychotic disorder are at greater risk of experiencing negative pathways to care than the Australian-born population. Further research is needed to identify the factors that lead to migrants being involuntarily admitted to hospital for first episode of psychosis.
Introduction
Understanding the pathways to care for individuals experiencing a first episode of psychosis (FEP) is important for a number of reasons. First, any help-seeking delays or barriers to accessing the appropriate service will lead to delays in treatment, which is associated with poorer outcomes (Santesteban-Echarri et al., 2017). In addition, the actual experience of seeking help can have a lasting impact on the relationship with the mental health service and subsequent engagement (Anderson et al., 2013). Past service use predicts future patterns of service use; therefore, understanding pathways to care related to the first episode of illness is important in preventing future negative trajectories of service use (Anderson et al., 2017). Migrants, who are at higher risk of developing a FEP (Cantor-Graae and Selten, 2005; Selten et al., 2020), are more likely to experience both longer delays to treatment (Boonstra et al., 2012; Nerhus et al., 2015) and their pathways to care are more likely to involve negative experiences, such as the involvement of law enforcement or involuntary admission.
First-generation migrants to Australia are at a greater risk of developing a psychotic disorder than the native-born population, with certain minority migrant groups at further increased risk (O’Donoghue et al., 2021). There is evidence that migrant status has an influence on pathways to care, as migrants are less likely to attend primary care services prior to diagnosis of first episode psychosis (Anderson et al., 2017). It has been found that refugees in the European Union attend hospitals first to seek treatment for a mental health problem, therefore bypassing primary and community care services (Satinsky et al., 2019). In a study based in New South Wales, it was found that specific migrants groups consulted a more restricted range of professional services, with Arabic-speaking patients more likely to consult a general practitioner (GP) and Asian-born patients less likely to consult an allied health professional than the Australian-born population (Steel et al., 2006). Reduced primary care use, as well as use of a more restricted range of professional services, suggests that there is less professional involvement to assist with navigating the appropriate pathways to care, which could lead to greater risk of experiencing negative pathways to care (Anderson et al., 2013; Cole et al., 1995). This is supported by the replicated finding that migrants are more likely to have an involuntary admission when presenting with a FEP (Rodrigues et al., 2019). Among migrant groups, ethnicity has been linked to increased risk of involuntary admission, with African and Caribbean groups possibly at greater risk (Anderson et al., 2010; Rodrigues et al., 2019; Stolk et al., 2008). Caribbean migrants in Canada are less likely to access psychiatric services prior to first diagnosis of a schizophrenia illness (Anderson et al., 2017). However, social supports may have more influence on pathways to care than ethnicity (Cole et al., 1995; Steel et al., 2006), with differences possibly mediated by social supports rather than ethnicity itself (Burnett et al., 1999).
There are several proposed reasons as to how migrant status may influence pathways to care. Pathways to access psychiatric care in the country of origin may influence how migrant populations seek care in Australia. For example, Turkish individuals access community services at higher rates than Australian-born clients, which may be due to greater familiarity with these services within their country of origin (Stolk et al., 2008). There may be lack of awareness of services that exist in the host country (Satinsky et al., 2019). In addition, cultural factors perpetuating stigma against mental illness and/or encouraging misinterpretation of symptoms may influence the type of care initially sought. For example, Asian ethnicity has been linked with lower mental health service use and reluctance to accept referral to mental health services (Anderson et al., 2013; Stolk et al., 2008). Migrant groups may seek help from more culturally acceptable services, such as traditional healers or respected elders (Satinsky et al., 2019). In turn, delayed treatment may lead to increasing severity of psychotic symptoms, necessitating acute hospital care and increasing the likelihood of coercive pathways to care. Language barriers and low acculturation may also play a role in influencing pathways to care (Satinsky et al., 2019; Stolk et al., 2008). A lack of personal and professional supports to advocate for care and negotiate the health care system seems to play a more important role (Cole et al., 1995; Steel et al., 2006). Factors in the host country, such as racial discrimination or accessibility of health care services (Tarricone et al., 2012), may further influence pathways to care. Lack of awareness from GPs and other health practitioners relating to mental health presentations in migrant populations also seems to be an important factor (Anderson et al., 2013; Satinsky et al., 2019).
Despite the increased risk of developing a psychotic illness in migrant populations and barriers associated with pathways to care, there are limited studies exploring pathways to care in this population in Australia. This study seeks to examine pathways to care for young people with FEP to a publicly funded youth mental health service. The aims of this study are threefold: First, to compare referral pathways into service for first-generation migrants and Australian-born youth. Second, to compare rates of inpatient admission and involuntary status at the time of presentation to service between these two groups. Finally, to investigate whether there are differences between first-generation migrant and Australian-born groups in clinical presentation, specifically symptoms severity, on entry into service. Based on the current available literature, we hypothesize that first-generation migrants are more likely to present to services through negative pathways to care, such as via law enforcement or inpatient admission. We hypothesize that migrants will have greater rates of inpatient admission on presentation to service. The literature also leads us to hypothesize that migrants are likely to be experiencing more severe symptoms at the time of first presentation to service.
Methods
Setting
Orygen is a state-funded youth mental health service covering a defined catchment area in northern and western metropolitan Melbourne in the state of Victoria, Australia. This area contains a population of over 1 million people, including 166,760 individuals aged between 15 and 24 years at the time of recruitment to this cohort (Eaton et al., 2019). One-quarter (24.5%) of this population were born in a country other than Australia. The Early Psychosis Prevention and Intervention Centre (EPPIC) is a service within Orygen which provides treatment to young people with a FEP. This service is available to all individuals residing in the catchment area and there are no costs for the individual or their family for using the service. This applies to all individuals, regardless of visa/resident status or whether the individual is seeking asylum or a refugee. Primary care appointments are subsidized by the federal Medicare system in Australia and there are primary care practices that only charge the amount that is subsidized (termed ‘bulk billing’), thereby resulting in there being no cost to the patient. There are also specific Medicare items that cover the cost for asylum seekers to attend primary care services.
There are no other public mental health services within this catchment area that provides this service for young people aged 15 to 24 and therefore EPPIC receive all referrals for young people with a FEP. The treated incidence rate of FEP in the catchment area is 123 per 100,000 at-risk population (Eaton et al., 2019). Young people attending EPPIC receive up to 2 years treatment with the service, unless they are less than 16 years of age at the time of presentation. In this case, they can attend the service up until the age of 18 years. EPPIC provides comprehensive case management, including assertive outreach as required.
Participants
All clients registered with EPPIC between 1 January 2011 and 31 December 2016 were included in this study. To be eligible for registration with EPPIC, clients must be between 15 and 24 years of age, reside within the catchment area and have experienced FEP, defined as experiencing full-threshold psychotic symptoms daily for at least 1 week. Clients were referred from a range of sources, including local mental health services, GPs, law enforcement agencies, community support services, family members and friends, and self-referral. All psychotic disorders were included in this study, including drug-induced psychosis.
Study design and sources of information
This was a naturalistic cohort study. Information was obtained from patient clinical files, including psychiatric assessment reports, 3-monthly client reviews, inpatient admission and discharge summaries, community discharge summaries and clinical notes. Migrant status was determined according to country of birth. It was not possible to identify which of the cohort born in Australia were second-generation migrants, as we did not have data relating to place of birth for both parents. Therefore, second-generation migrants were included in the ‘Australian-born’ cohort. Young people born outside of Australia were considered to be first-generation migrants.
The postcode at which the client was residing at the time of entry to service was documented. All diagnoses, including diagnosis of psychotic illness as well as comorbid diagnoses such as substance use disorder, were made by the treating consultant psychiatrist at 3 months following entry into service. The EPPIC clinic accepted both affective (schizoaffective disorder, bipolar affective disorder and depression with psychosis) and non-affective psychotic disorders (schizophreniform disorder, schizophrenia, delusional disorder, drug-induced psychosis, brief psychotic disorder and psychosis not otherwise specified).
Information regarding source of referral was obtained from the clinical notes in the young person’s medical record. Statutory forms in the medical record were used to classify admissions as either voluntary or involuntary, as well as whether admissions occurred either at presentation or after presentation to the service. Admission at presentation was defined as being hospitalized within 30 days of the date of registration, regardless of whether inpatient admission occurred at Orygen or at another hospital’s inpatient mental health unit.
The severity of psychotic symptoms was assessed and rated at baseline. Routinely documented mental state examinations from case managers and psychiatrists were used to assess and rate positive and negative symptoms. Rating was performed using short-form Scale for the Assessment of Positive Symptoms (SAPS), which has been demonstrated to be reliable and valid instrument (Cronbach’s alpha = 0.78, sensitivity and specificity for determining remission = 86%) (Alonso et al., 2008).
Classification of countries of birth and grouping for analysis
All new clients were asked to provide information pertaining to country of birth at the time of registration with Orygen. This information was then coded using the Standard Australian Classification of Countries (SACC). Migrant groups were first coded according to the methods used by the Australian Bureau of Statistics, in which BPLP1 refers to the highest level and there are nine areas within this group, including some continents divided into two regions, for example, North-West Europe and Sothern and Eastern Europe. Analysis was conducted first with first-generation migrants as one distinct group. As there may be different outcomes for different migrant groups, analysis was repeated with a refined grouping of migrants. Our previous research has identified that the risk of developing psychotic disorders was greatest for migrants from Africa and reduced in migrants from Asia (O’Donoghue et al., 2021). These two groups represent the largest migrant groups in the cohort; therefore, analysis was repeated in these two groups.
Classification of pathways to care for analysis
For the purpose of analysis, clients were categorized into eight possible groups based on the source of referral to Orygen: self-referral, family, friend, emergency department, crisis service, community health service, police or other mental health service. Community health services included GPs and GP-based practices such as Headspace, as well as school-based services, psychologists, housing services, vocational services, child protection services and drug and alcohol services. This broad categorization serves to reflect any referral from a non-acute community service working with young people. Referrals from external public inpatient or community mental health services or private psychiatrists were categorized as ‘other mental health service’, while referrals directly from an external acute or crisis mental health service were categorized separately as ‘crisis service’. Referrals from Juvenile or Youth Justice services were categorized under ‘police’. This category reflects clients referred via all law enforcement agencies. There were a small number of young people who had both the police and emergency department involved in their pathway to care. When just one pathways of care was being examined, these individuals were coded as ‘police’. However, when separate analyses were performed for each specific pathway, they were included in both groups that included pathways to care via emergency department or police.
Ethical approval
Ethical approval for this study was granted by the Royal Melbourne Hospital Ethics Committee. A waiver of individual consent was granted to allow all cases of FEP to be included to ensure that the cohort would be representative.
Statistical analysis
Chi-square analysis was performed to determine whether there were differences in the observed outcomes compared to the expected outcomes for categorical variables and odds ratios (ORs) were presented with the 95% confidence intervals (CI). T tests were used to determine whether differences existed in the means of two independent groups. Binary logistic regression was used to determine the ORs for the outcome variables of ‘Any psychiatric admission at baseline’ and ‘Involuntary admission at presentation’ according to migrant status. Three models were performed. The first was an unadjusted model, the second model was adjusted for demographic factors (sex, age, marital status, family history) and the third model was adjusted for clinical factors (diagnosis, severity of psychotic symptoms and concurrent substance abuse). Each model was repeated for the sub-group of migrants from Africa and Asia and the results of this analysis are presented in Supplementary Tables. Analysis was performed using SPSS statistical software (IBM Corporation, 2019).
Results
Baseline characteristics of the study cohort
A total of 1220 young people were diagnosed with a FEP and received care at EPPIC during the 6-year study period. Complete data were present for 1196 young people (98%), with 24 cases missing data in relation to place of birth. Nearly one-quarter of the cohort (n = 293, 24.5%) were first-generation migrants, mostly born in North Africa and the Middle East (25.9% of the migrant cohort), sub-Saharan Africa (19.1%) and South-East Asia (16.4%). In the total cohort, the mean age at presentation was 19.6 ± 2.8 years and 41.5% (n = 496) were female. The majority had never been married (93.3%), a total of 42.4% (n = 507) were unemployed and 37.0% (n = 442) were students. A total of 18.0% (n = 215) had a positive family history of psychotic disorder in a first-degree relative. Schizophrenia-spectrum disorders were diagnosed in 41.8% (n = 500) of the cohort, while 21.4% (n = 257) were diagnosed with an affective psychotic disorder and 36.7% (n = 439) with other psychotic disorders (including drug-induced psychosis, brief psychotic disorder, psychosis Not Otherwise Specified (NOS) or delusional disorder). Within the cohort, 51.6% (n = 617) had a history of cannabis use, 27.6% (n = 330) had used methamphetamine and 17.4% (n = 208) had harmful use of alcohol. The demographic and clinical characteristics of the total cohort and a comparison of these factors between migrants and the Australian-born young people are presented in Table 1. There were a number of differences in demographic and clinical factors; in summary, first-generation migrants were older (20.2 years vs 19.4), more likely to be male (64.2% vs 56.7%), married (5.6% vs 2.9%) and were less likely to have a family history of a psychotic disorder in a first-degree relative (7.8% vs 21.3%) and concurrent cannabis (43.7% vs 54.2%) or methamphetamine abuse (16.0% vs 31.3%).
Demographic and clinical characteristics of the total cohort and comparison between migrants and Australian-born youth.
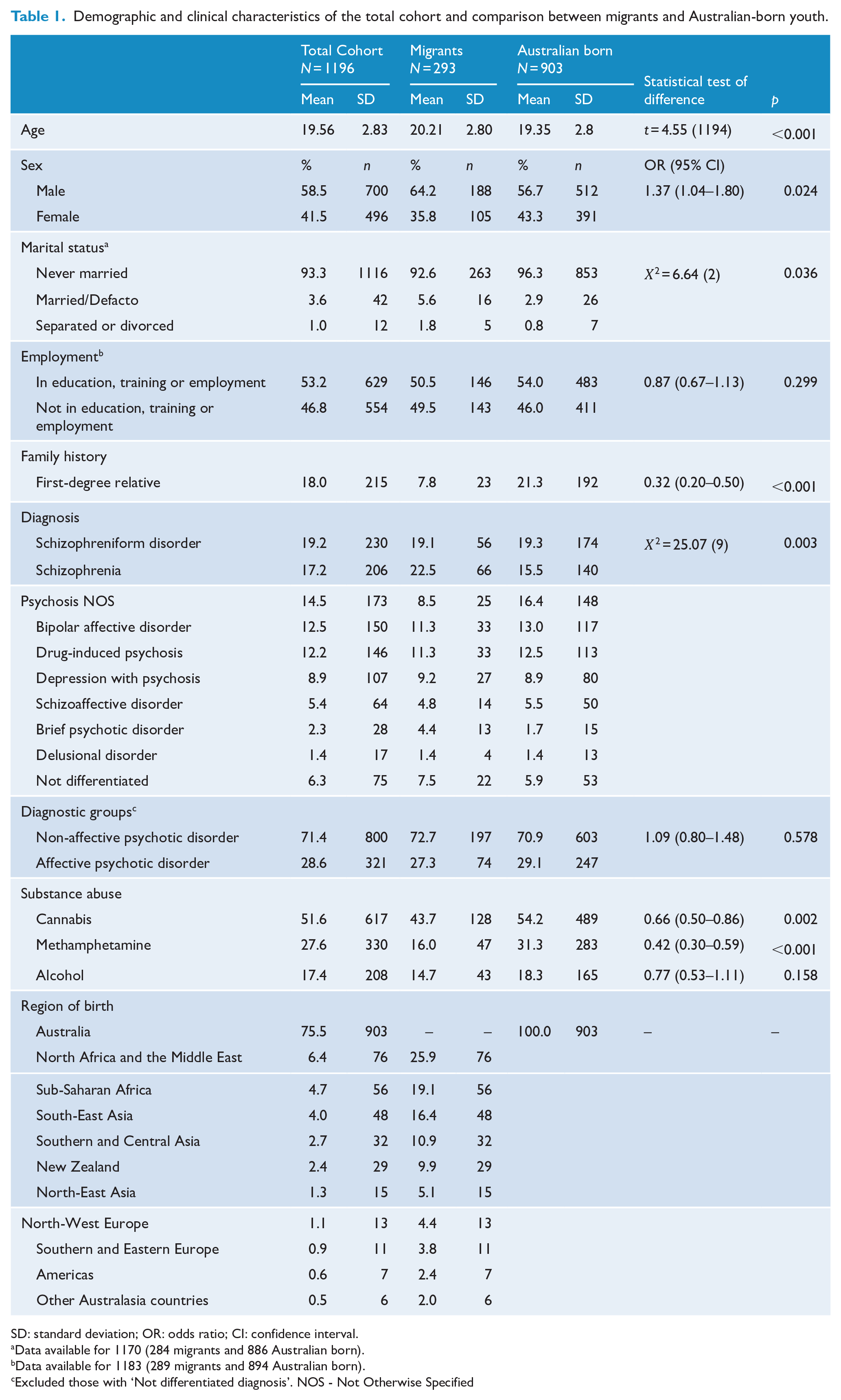
SD: standard deviation; OR: odds ratio; CI: confidence interval.
Data available for 1170 (284 migrants and 886 Australian born).
Data available for 1183 (289 migrants and 894 Australian born).
Excluded those with ‘Not differentiated diagnosis’. NOS - Not Otherwise Specified
Admission at time of presentation
Nearly half (49.7%) of the cohort were admitted to a psychiatric inpatient unit at the time of presentation (Table 2). First-generation migrants with FEP were more likely to be admitted to hospital than Australian-born youth (OR = 1.67, 95% CI = [1.27, 2.18], p < 0.001). Nearly two-thirds of admissions at the time of presentation were involuntary (64.1%, n = 381). It was found that 43.0% (n = 117) of migrants had an involuntary admission at the time of presentation, compared to 31.2% (n = 264) of Australian-born youth (OR = 1.67, 95% CI = [1.26, 2.21], p < 0.001). The ORs for any psychiatric admission and involuntary admission in migrants reduced slightly when controlled for demographic (adjusted odds ratio [aOR] = 1.41, 95% CI = [1.07, 1.88], p = 0.016) and clinic factors (aOR = 1.38, 95% CI = [1.01, 1.89], p = 0.044); however, they remained statistically significant, as presented in Table 2.
Unadjusted and adjusted odds ratio for any psychiatric admission and involuntary admission at presentation.
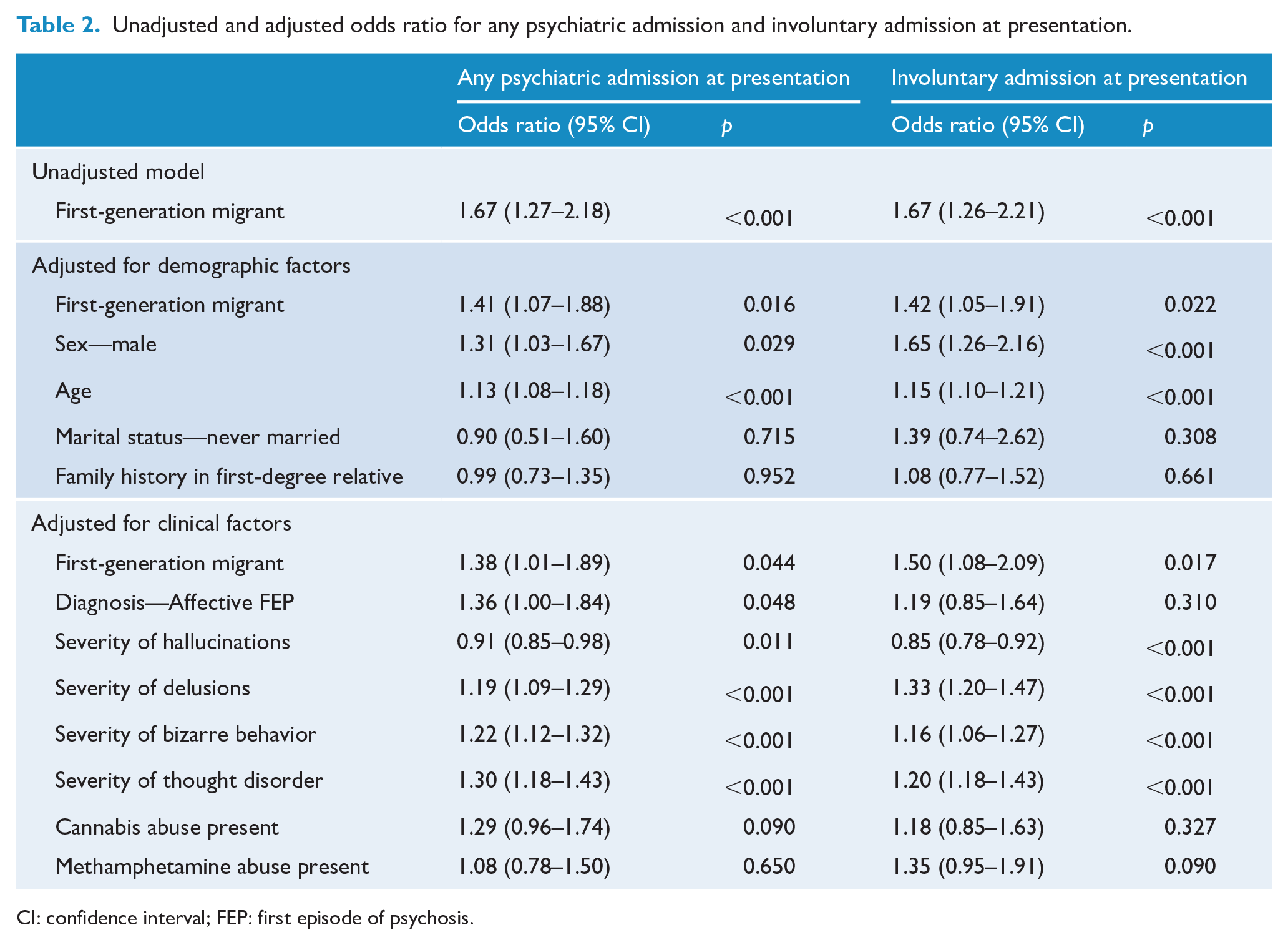
CI: confidence interval; FEP: first episode of psychosis.
Within the migrant sub-groups, 64.3% (n = 63) of African-born migrants with FEP were admitted at the time of presentation to service, significantly higher than the 47.1% (n = 422) of Australian-born youth admitted on presentation (OR = 2.02, 95% CI = [1.31, 3.12], p = 0.001). These findings remained significant when controlled for demographic (aOR = 1.68, 95% CI = [1.07, 2.64], p = 0.016) but not clinical factors (aOR = 1.53, 95% CI = [0.93, 2.50], p = 0.09) (Supplementary Table 1). Furthermore, 52.2% (n = 48) of African-born migrants had an involuntary admission at presentation compared to 31.2% of Australian-born youth (OR = 2.41, 95% CI = [1.56, 3.72], p < 0.001). This finding remained significant when controlled for demographic factors (aOR = 1.94, 95% CI = [1.22, 3.07], p = 0.005) and clinical factors (aOR = 1.85, 95% CI = [1.12, 3.06], p = 0.016).
A total of 62.1% (n = 59) of Asian-born migrants had an admission at the time of presentation (OR = 1.84, 95% CI = [1.19, 2.84], p = 0.006). This finding remained significant when controlled for demographic factors (aOR = 1.60, 95% CI = [1.02, 2.52], p = 0.04) but not clinical factors (aOR = 1.56, 95% CI = [0.93, 2.61], p = 0.09). A total of 41.8% (n = 38) of Asian-born migrants were admitted involuntarily compared to 31.2% of Australian-born youth (OR = 1.58, 95% CI = [1.02, 2.46], p = 0.04). However, when controlled for demographic factors (aOR = 1.36, 95% CI = [0.85, 2.17], p = 0.20) or clinical factors (aOR = 1.48, 95% CI = [0.87, 2.53], p = 0.15), these findings were no longer statistically significant (Supplementary Table 2).
Symptom severity at presentation
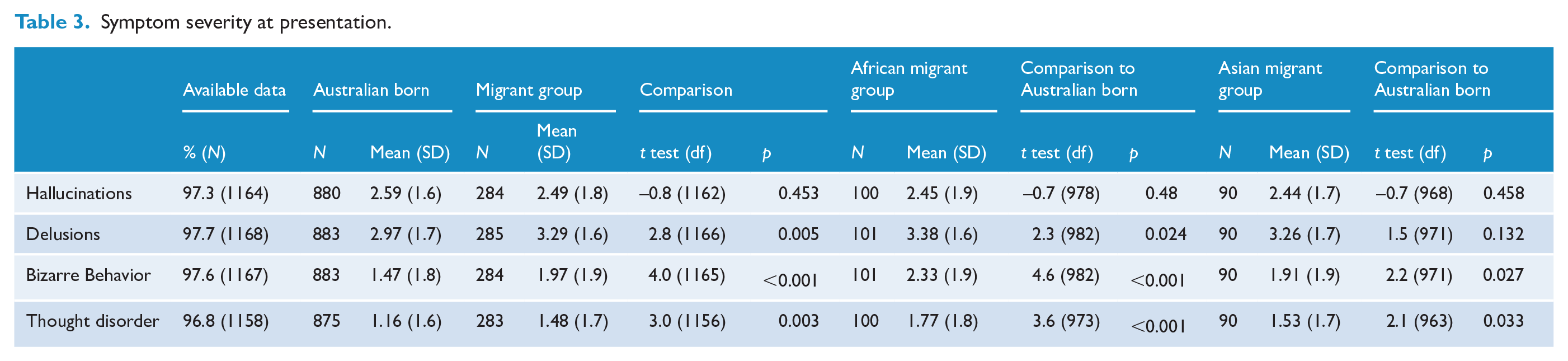
There was no difference in the mean score for the severity of hallucinations at the time of presentation between Australian-born youth and migrants (p = 0.458). However, migrants had more severe delusions (p = 0.005), bizarre behavior (p < 0.001) and positive formal thought disorder (p = 0.003) at the time of presentation compared to the Australian-born group (Table 3). These results were consistent in the African and Asian migrant sub-groups, except that Asian migrants did not have more severe delusions.
Symptom severity at presentation.
Pathways to care
Information on pathways to care was available for 1134 clients (94.8%). The pathways to care for the eligible cohort are presented in Table 4. The majority of clients were referred to Orygen via a community service (24.7%), an emergency department (24.3%) or another mental health service (18.4%). A total of 243 referrals (21.4%) came from clients themselves (3.8%), their families (15.9%) or their friends (1.8%). Police or law enforcement agencies only made up 5.6% (n = 63) of total referrals.
Pathways to care: Source of referral.
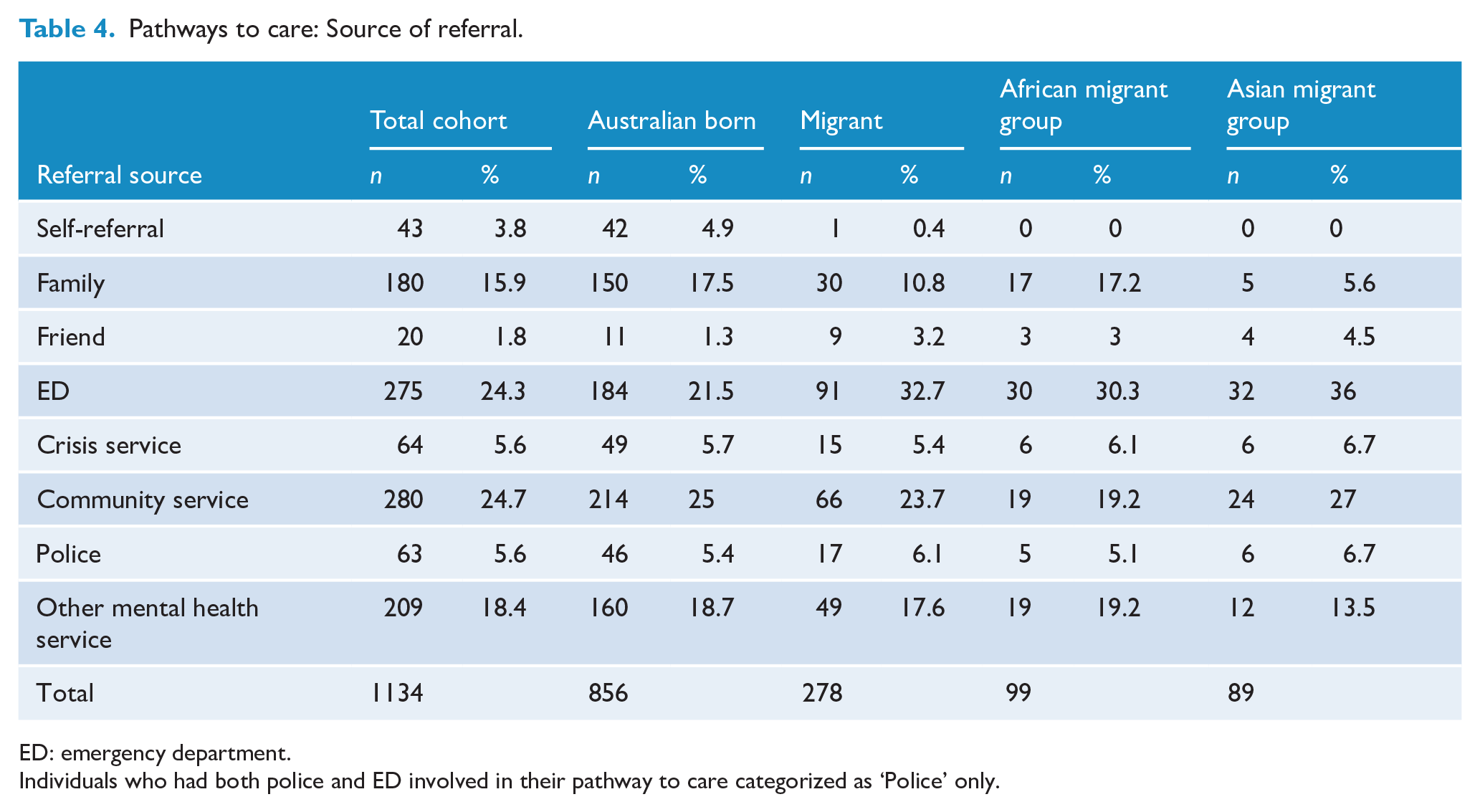
ED: emergency department.
Individuals who had both police and ED involved in their pathway to care categorized as ‘Police’ only.
Both police and emergency department were involved in the pathways to care for 1.8% (n = 16) of Australian-born youth and 2% (n = 6) of migrants, including 2.9% (n = 3) of African migrants and 3.2% (n = 3) of Asian migrants. First-generation migrants were more likely to attend the emergency department during their presentation with first episode psychosis (34.9% vs 23.4%, OR = 1.76, 95% CI = [1.31, 2.36], p < 0.001) (Table 5). This is consistent for both African migrants (33.3% vs 23.4%, OR = 1.64, 95% CI = [1.05, 2.56], p = 0.03) and Asian migrants (39.3% vs 23.4%, OR = 2.13, 95% CI = [1.35, 3.35], p = 0.001). There was no significant difference in the proportion of Australian-born youth and migrants whom had the police involved in their pathway to care (6.1% vs 5.4%, χ2 = 0.22, p = 0.64), nor was there a difference in the involvement of police in the pathways to care for African (5.1% vs 5.4%, χ2 = 0.02, p = 0.89) or Asian (6.7% vs 5.4%, χ2 = 0.29, p = 0.59) migrant sub-groups.
Pathways to care via ED or police.
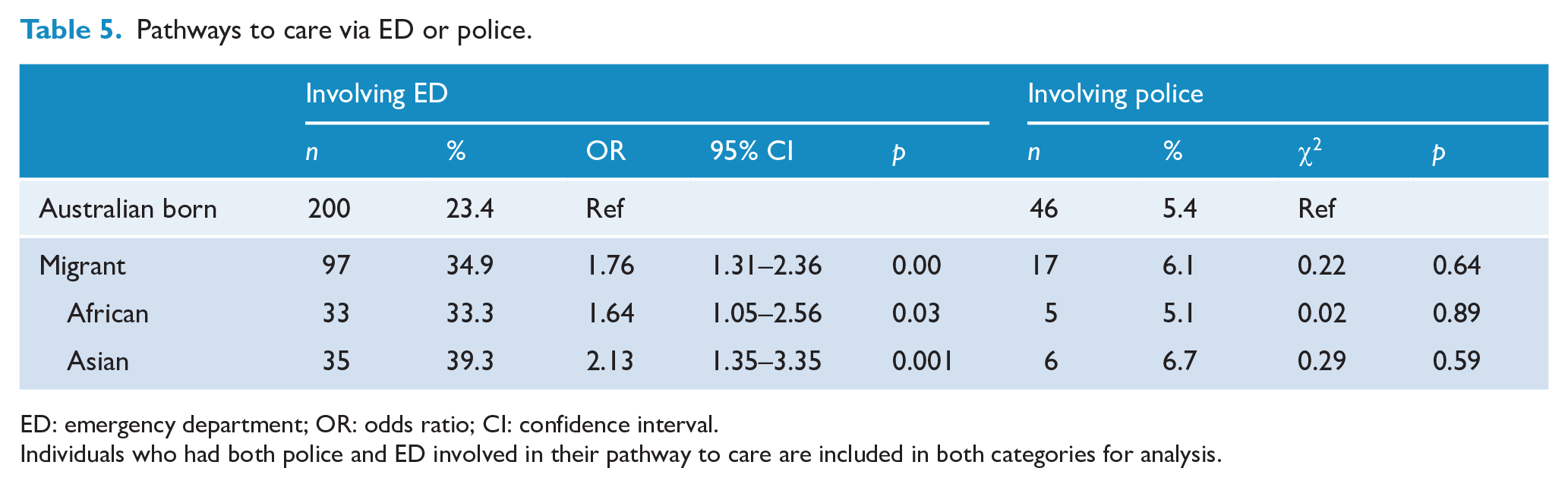
ED: emergency department; OR: odds ratio; CI: confidence interval.
Individuals who had both police and ED involved in their pathway to care are included in both categories for analysis.
Discussion
Summary of findings
This study shows that first-generation migrants with first episode psychosis are more likely to experience negative pathways to care. In addition, first-generation migrants are also more likely to present with more severe psychotic symptoms on first presentation to service. Our results suggest that first-generation migrants are more likely to be admitted on presentation with FEP, and their admission is more likely to be involuntary. First-generation migrants are also more likely to attend the emergency department prior to presentation to service. Our results did not show a significant difference in police involvement with Australian-born and migrant groups on presentation to service. The results for first-generation migrants were similar in both the African and Asian migrant sub-groups.
Strengths and limitations
As a naturalistic cohort study, this cohort was representative of the clients with FEP that would present to public mental health services in the northwestern suburbs of Melbourne, Australia. However, these results may not necessarily be generalizable to other regions. A major limitation of this study was that there was insufficient information available to differentiate second-generation migrants from the rest of the Australian-born population. Second-generation migrants are also at greater risk of psychosis than the native population and post-migration factors may play a role in this (Bourque et al., 2010). It is possible that the inclusion of second-generation migrants in the Australian-born group may have reduced the statistical differences between the migrant and Australian-born groups. Another limitation is that information relating to the SAPS rating was sourced from clinical notes and interpretation of these notes by the researchers. Finally, this study only looks at the immediate referral source as an indication of the pathway to care, based on information available from the medical record. There may be clients referred from public inpatient mental health services who accessed police and/or the emergency department prior to their inpatient admission, which is not reflected in our analysis. This would underestimate the number of clients across both groups who had police and emergency departments involved in their pathways to care.
Clinical implications
These findings support the multitude of studies suggesting that more needs to be done to improve the migrant population’s access to appropriate mental health care. Demand on inpatient mental health beds and unacceptably high rates of involuntary admission are significant issues in many parts of the world (Sheridan Rains et al., 2019). Migrants represent a high-risk group for admission on first presentation to service, which sets the stage for ongoing future admissions (Anderson et al., 2017). As displayed in Table 2, there are a number of clinical factors that are associated with admission, such as diagnosis and severity of symptoms, but migrant status remained significant when controlled for these factors. Our study also replicates the findings that migrants are also presenting in higher numbers to the emergency department, rather than via community supports (Satinsky et al., 2019). Emergency departments can be a confronting environment for individuals experiencing acute psychosis, and those with mental health presentations often experience significant waiting periods (Australian College of Emergency Medicine, 2018). Similarly, psychiatric inpatient admission can be a traumatic experience for individuals with acute psychosis (Paksarian et al., 2014) and migrant youth are already more likely to have been exposed to traumatic events than their non-migrant peers (Gatt et al., 2020).
Our findings show that migrants are presenting with more severe symptoms on first presentation. One possible reason for this may be that they are experiencing longer duration of untreated illness. This suggests that we should target migrants in programs geared toward early intervention in FEP. It is well established that a longer duration of untreated psychosis (DUP) is associated with poor outcomes and more severe psychotic symptoms (Marshall et al., 2005), which may explain the higher rates of involuntary admissions.
Migrants need to be provided with information on when and how to access mental health care in the community where appropriate. Information on recognizing symptoms of illness, accessible in the client’s own language, may help individuals and families recognize emerging mental illness and seek help earlier (Satinsky et al., 2019). Given certain migrant populations may turn to traditional healers, religious leaders or respected elders when seeking advice relating to mental health concerns (Satinsky et al., 2019), it could be valuable to liaise with and educate these key figures in at-risk communities in order to reduce the DUP (Tomita et al., 2015). Similarly, previous studies suggest that GPs may lack confidence or awareness when dealing with migrant mental health presentations, particularly where migrants present with somatic complaints that mask a mental health concern (Anderson et al., 2013; Chesney et al., 2016; Satinsky et al., 2019). GP liaison services are an existing asset in many community mental health services. These services are in a prime position to deliver pre-emptive education and support to local GP practices. Outreach services also provide an invaluable avenue for migrants to access care (WHO Regional Office for Europe, 2018). Orygen has recently established a Hospital in the Home (HiTH) program, with a similar program available in Western Australia (Orygen, 2020). This service aims to provide the equivalent of inpatient care in the community and in particular it is hoped that migrants will benefit from this service which offers a less restrictive alternative to inpatient admission on presentation.
Further research
While our research suggests how migrants with FEP present to specialty mental health services, it does not tell us why this population presents in this way. Further research is needed to investigate why migrants have higher rates of involuntary admission, present more frequently to emergency departments and present with more severe illness. It may be that these factors are driven by delays in seeking treatment. Qualitative research is needed to understand why this might be, so that the barriers to appropriate care can be addressed.
Conclusion
Migrants who develop a psychotic disorder are at greater risk of experiencing negative pathways to care than the Australian-born population. This has adverse consequences for the individual, their families and the public mental health system. Further research is needed to identify the factors that lead to migrants being involuntarily admitted to hospital for treatment for a FEP.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221075980 – Supplemental material for Pathways to care for first-generation migrants with first episode psychosis in northwestern metropolitan Melbourne
Supplemental material, sj-docx-1-anp-10.1177_00048674221075980 for Pathways to care for first-generation migrants with first episode psychosis in northwestern metropolitan Melbourne by Alexandra Waxmann, Andrew Thompson, Patrick McGorry and Brian O’Donoghue in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: B.O’D. is supported by an NHRMC Early Career Fellowship (1142045).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.