
Abstract
Objective:
Poorer mother–infant interaction quality has been identified among women with major depression; however, there is a dearth of research examining the impact of bipolar disorder. This study sought to compare mother–infant emotional availability at 6 months postpartum among women with perinatal major depressive disorder, bipolar disorder and no disorder (control).
Methods:
Data were obtained for 127 mother–infant dyads from an Australian pregnancy cohort. The Structured Clinical Interview for the DSM-5 was used to diagnose major depressive disorder (n = 60) and bipolar disorder (n = 12) in early pregnancy (less than 20 weeks) and review diagnosis at 6 months postpartum. Prenatal and postnatal depressive symptoms were measured using the Edinburgh Postnatal Depression Scale, along with self-report psychotropic medication use. Mother and infant’s interaction quality was measured using the Emotional Availability Scales when infants reached 6 months of age. Multivariate analyses of covariance examining the effects of major depressive disorder and bipolar disorder on maternal emotional availability (sensitivity, structuring, non-intrusiveness, non-hostility) and child emotional availability (responsiveness, involvement) were conducted.
Results:
After controlling for maternal age and postpartum depressive symptoms, perinatal disorder (major depressive disorder, bipolar disorder) accounted for 17% of the variance in maternal and child emotional availability combined. Compared to women with major depressive disorder and their infants, women with bipolar disorder and their infants displayed lower ratings across all maternal and child emotional availability qualities, with the greatest mean difference seen in non-intrusiveness scores.
Conclusions:
Findings suggest that perinatal bipolar disorder may be associated with additional risk, beyond major depressive disorder alone, to a mother and her offspring’s emotional availability at 6 months postpartum, particularly in maternal intrusiveness.
Introduction
The most common complication of childbearing is perinatal mental disorders (Howard and Khalifeh, 2020), with a recent systematic review identifying an overall pooled prevalence of 11.9% for perinatal depression alone (Woody et al., 2017). Reviews have also shown perinatal depression to adversely associate with maternal and child outcomes (Goodman, 2020; Rogers et al., 2020), including interaction quality during infancy (Barnes and Theule, 2019; Tichelman et al., 2019) and the mental health of offspring in adolescence and young adulthood (Lewis et al., 2014; Radke-Yarrow et al., 1992; Weissman et al., 2016). Mother–infant interactions have been suggested as a potential mediator of the transmission of psychopathology from mother to offspring (Goodman et al., 2011; Stein et al., 2014; Wan and Green, 2009) and has resulted in the mother–infant relationship becoming an integral part of perinatal care alongside maternal mental health (Austin et al., 2017; Malhi et al., 2015). While new measures and interventions targeting mother–infant interaction quality continue to emerge and circulate globally (Huang et al., 2020; Lotzin et al., 2015; Wittkowski et al., 2020), research regarding mother–infant relationship quality across the full range of perinatal mental disorders is still in its infancy (Howard and Khalifeh, 2020).
Studies examining the association between maternal mental health and mother–infant interactions primarily involve depression, at the symptom rather than at the disorder level (Beck, 1995; Goodman, 2020; Martin and Gaffan, 2000). Women with pre-existing severe mood disorders, such as bipolar disorder (BD), however, face the highest risk of inpatient psychiatric admission following childbirth (Jones et al., 2014; Wesseloo et al., 2016), and despite this, little is known about their impact on mother–infant interaction quality (Rusner et al., 2016). BD, previously known as manic depression, is characterised by at least one episode of major depression and one episode of mania (Bipolar 1) or hypomania (Bipolar 2). While the effects of perinatal BD on various child developmental outcomes have been examined (Jones et al., 2014; Santucci et al., 2017), we identified only three peer-review studies that included observations of mother–infant interactions among women with diagnosed BD, and two of the three involved the same cohort (Anke et al., 2019, 2020).
The first cohort comprised mothers with postpartum BD (n = 40), unipolar depression (n = 50) and no disorder (n = 40) and their infants, and found that dyads in the BD group displayed less maternal sensitivity and dyadic synchrony at 12 months postpartum; however, the differences did not reach significance (Logsdon et al., 2015). The second cohort comprised women with perinatal BD (n = 26) and women with no disorder (n = 30) and their infants and, in contrast to Logsdon et al., identified significant difficulties in maternal behaviour, infant behaviour and dyadic coordination at 3 months (Anke et al., 2019) and 12 months (Anke et al., 2020) postpartum among women with BD and their infants.
Logsdon et al. put forth a methodological explanation for their nonsignificant results, recommending future studies employ a larger sample of women with BD and earlier assessment of interaction quality according to multiple maternal and child qualities. However, Anke et al.’s cohort involved fewer women with BD and fewer constructs measuring relationship quality, as well as similar observation duration. Although either did not remark on the duration, they were brief: 3 minutes (Logsdon et al., 2015) and 5 minutes (Anke et al., 2019, 2020).
Perhaps, the divergence in findings resulted from a discrepancy in maternal mental disorders. In addition to Logsdon et al.’s cohort, including a unipolar depression group, the course of BD seemed to have differed between cohorts. Anke et al. measured diagnosis during pregnancy and postpartum, while Logsdon et al. measured diagnoses at 12 months postpartum only and did not provide details of the disorder’s time of onset. Prior research has shown antenatal depression to predict lower mother–infant relationship quality at 12 months of infant age, independent of postnatal depression (Hayes et al., 2013). In addition, a recent systematic review of postpartum psychoses identified chronic psychosis was associated with poorer mother–infant interactions than acute-onset (de novo or relapse) psychosis (Ramsauer and Achtergarde, 2018). While not specific to BD, these related studies highlight that onset (or course of disorder) is an important consideration when examining perinatal disorders and mother–infant relationship quality.
In sum, there is a dearth of literature regarding mother–infant interaction quality among women with BD, and as a result, our understanding of how BD compares to unipolar depression is limited. Accordingly, we investigated the impact of perinatal BD, compared to major depressive disorder (MDD) and no disorder (i.e. control), diagnosed in pregnancy and reviewed postpartum on mother–infant emotional availability (EA) at 6 months of infant age. To our knowledge, our study is the first to report on the EA of women with diagnosed BD and their infants. Furthermore, 6-month observations are a midpoint between the timing of observations in Anke et al.’s (2019) and Logsdon et al.’s (2015) studies; thus, our study contributes to building a timeline of mother–infant interaction quality over the first year of infancy. We hypothesised that after controlling for any effects of maternal age and postpartum depressive symptoms at 6 months of infant age,
Women with perinatal BD will display lower maternal EA (sensitivity, structuring, non-intrusiveness, non-hostility) towards their infants, than women with perinatal MDD and women without perinatal disorders.
Infants of women with perinatal BD will display lower child EA (responsiveness, involvement) towards their mothers, than infants of women with perinatal MDD and infants of women without perinatal disorders.
Method
Participants and procedure
Participants were drawn from an Australian pregnancy cohort study with an observational and longitudinal prospective design. Participants were recruited before the 20th week of pregnancy (Wave 1) and followed up during the third trimester (Wave 2), at the birth of their child (Wave 3) and 6 months postpartum (Wave 4). Further details can be found in a published study protocol of the original cohort (Galbally et al., 2017).
At Wave 4, 132 dyads consented to the recording of a mother–infant interaction. Mothers were told to ‘interact with your baby as you normally would at home’ beginning with face-to-face for 10 minutes and then free-play for 15 minutes with standardised age-appropriate toys. Three camcorders were used, one positioned facing the mother, one facing the infant and one behind a one-way observation mirror to capture a full view.
Measures
Maternal mental health
The Structured Clinical Interview for DSM-5–Clinician Version (SCID-5-CV; First et al., 2016) was administered at Waves 1 and 4 to assess for MDD and BD during the perinatal period (current or within 2 years of pregnancy). At Waves 1 through 5, depressive symptoms were assessed using the Edinburgh Postpartum Depression Scale (EPDS; Cox et al., 1987), and psychotropic medication use (name, dose) was obtained via self-report. The EPDS has established validity and reliability for use with Australian women during the perinatal period (Boyce et al., 1993).
Mother–infant interaction quality
The Emotional Availability Scales, 4th Edition Infancy/Early Childhood Version (EAS; Biringen et al., 2008) was used to assess the quality of mother–infant interaction at 6 months postpartum, that is, Wave 4. The EAS is a standardised observation tool that provides a global assessment of interaction quality according to multiple affective and behavioural qualities of mother and child, and their dyadic pattern (i.e. synchrony). All dimensions of the EAS were administered: maternal sensitivity (mother’s affective presence and appropriate responsiveness to infant’s signals), maternal structuring (mother’s appropriate management of interaction including setting limits in a preventive and protective manner), maternal non-intrusiveness (mother supporting autonomy and withholding interfering or overpowering behaviours), maternal non-hostility (mother interacting without being overtly or covertly hostile), child inclusiveness (child’s propensity to include mother in the interaction or play) and child responsiveness (child’s affective presence and behavioural and emotional responsiveness). The EAS has established reliability and validity across both laboratory and naturalistic settings, with intraclass correlation reliability between 0.79 for non-hostility and 0.92 for sensitivity, and short-term test–retest reliability and demonstrated stability over 18 and 24 months (Biringen et al., 2014). Recordings exceeded the 20-minute minimum recommended length for EAS observation (Biringen et al., 2008). Both coders were blind to participant characteristics, including mental health status.
In line with the recommended application of the EAS (Biringen et al., 2008), we calculated EA according to both mother (four EA dimensions) and child (two EA dimensions) and analysed them as continuous variables (minimum: 7, maximum: 29). Higher scores reflect better quality of the affective relationship between parent and child. Maternal and child EA classifications (emotionally available, complicated, detached and problematic) were also computed to provide a clear overview of participants’ EA classifications between disorder groups (Biringen et al., 2014).
Inter-rater reliability was completed using a randomly selected subsample of 23 video recordings, coded by two researchers who received training from the author of the scales, Professor Biringen, and became certified reliable coders. Both coders were blind to participant characteristics at the time of coding (i.e. mental health status, demographic data). Inter-rater reliability between coders on the EA classifications was r = 0.84 for maternal EA and r = 0.84 for child EA. Reliability for each EA dimension, using the direct scores, was calculated in an intraclass correlation coefficient (ICC) two-way random-effects model with absolute agreement (McGraw and Wong, 1996): maternal sensitivity = 0.91, maternal structuring = 0.88, maternal non-hostility = 0.88, maternal non-intrusiveness = 0.84, child responsiveness = 0.94, and child involvement = 0.94. Disagreements in scoring were minor and were resolved via joint viewing of the interaction and reaching agreement on a new score.
Demographics
Participants were also asked demographic questions, among which maternal age, education and parity were included in the correlation analyses due to past research demonstrating their relevance to EA (Biringen et al., 2014).
Statistical analyses
All statistics were conducted using SPSS version 26 (IBM Corp., 2019) unless otherwise specified. Data were first inspected for missing data, outliers and meeting appropriate assumptions for analyses using general linear models. The resulting sample size was 127 dyads. Missing data for depressive symptoms (44%) at Wave 4 were estimated using an Expectation-Maximisation multiple imputation, using the scores from Waves 1, 2 and 5 as predictors. Assumption of normality was violated; accordingly, non-parametric correlations were calculated. Hypotheses were assessed via two multivariate analysis of covariance (MANCOVA) testing for patterns of significant differences in each of the maternal and child EA qualities between groups. Estimated marginal means (EMM) for each group are presented and adjusted for covariates (maternal age, postpartum depressive symptoms).
Results
Sample characteristics
At recruitment in early pregnancy (less than 20 weeks), the majority of women in the sample were in a relationship (94%) and employed (73%), and over half were multiparous (52%) and tertiary educated (56%). Infant gender in the sample was roughly equal (55% male). Few participants reported changing medication agents between pregnancy and postpartum; however, medication use was significantly higher in the BD group (n = 12). In the BD group, all women reported medication use during pregnancy and postpartum, with half reporting use of two or more psychotropic agents (n = 6). The proportion of BD 1 (n = 7) versus BD 2 (n = 5) disorders in the group was roughly equal. Table 1 displays sociodemographic characteristics according to the disorder group (BD, MDD, control), with accompanying significance tests that confirm dyads did not differ between groups in key sociodemographic characteristics (p > 0.05), apart from mental health characteristics as expected.
Frequencies and scaled means of sociodemographic characteristics, maternal mental health and EA by disorder group, with accompanying significance (N = 127).
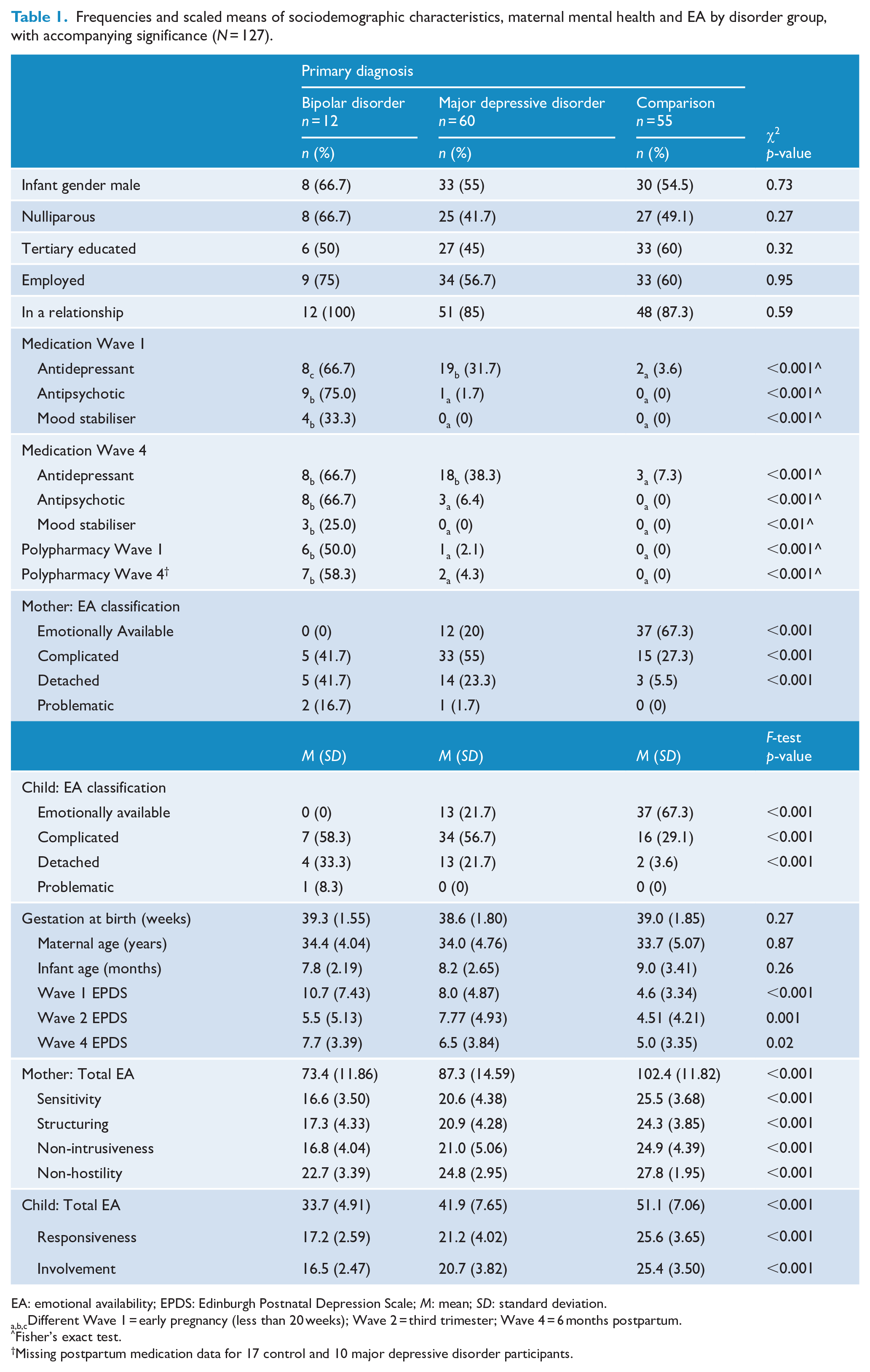
EA: emotional availability; EPDS: Edinburgh Postnatal Depression Scale; M: mean; SD: standard deviation.
a,b,cDifferent Wave 1 = early pregnancy (less than 20 weeks); Wave 2 = third trimester; Wave 4 = 6 months postpartum.
Fisher’s exact test.
Missing postpartum medication data for 17 control and 10 major depressive disorder participants.
EA by disorder group
Table 1 displays scaled means for each of the maternal and child EA dimensions, and accompanying significance of unadjusted F-tests. Compared to the no disorder group, scaled means for each of the six EA dimensions were significantly lower in the BD and MDD groups (p < 0.001). Table 2 presents Spearman’s rho correlations showing medium negative associations between dependent variables (maternal and child EA) and perinatal disorder, depressive symptoms and medication use. Correlations between the sociodemographic variables, and dependent and predictor variables were not significant.
Non-parametric bivariate correlations between EA, mental health and sociodemographics (N = 127).
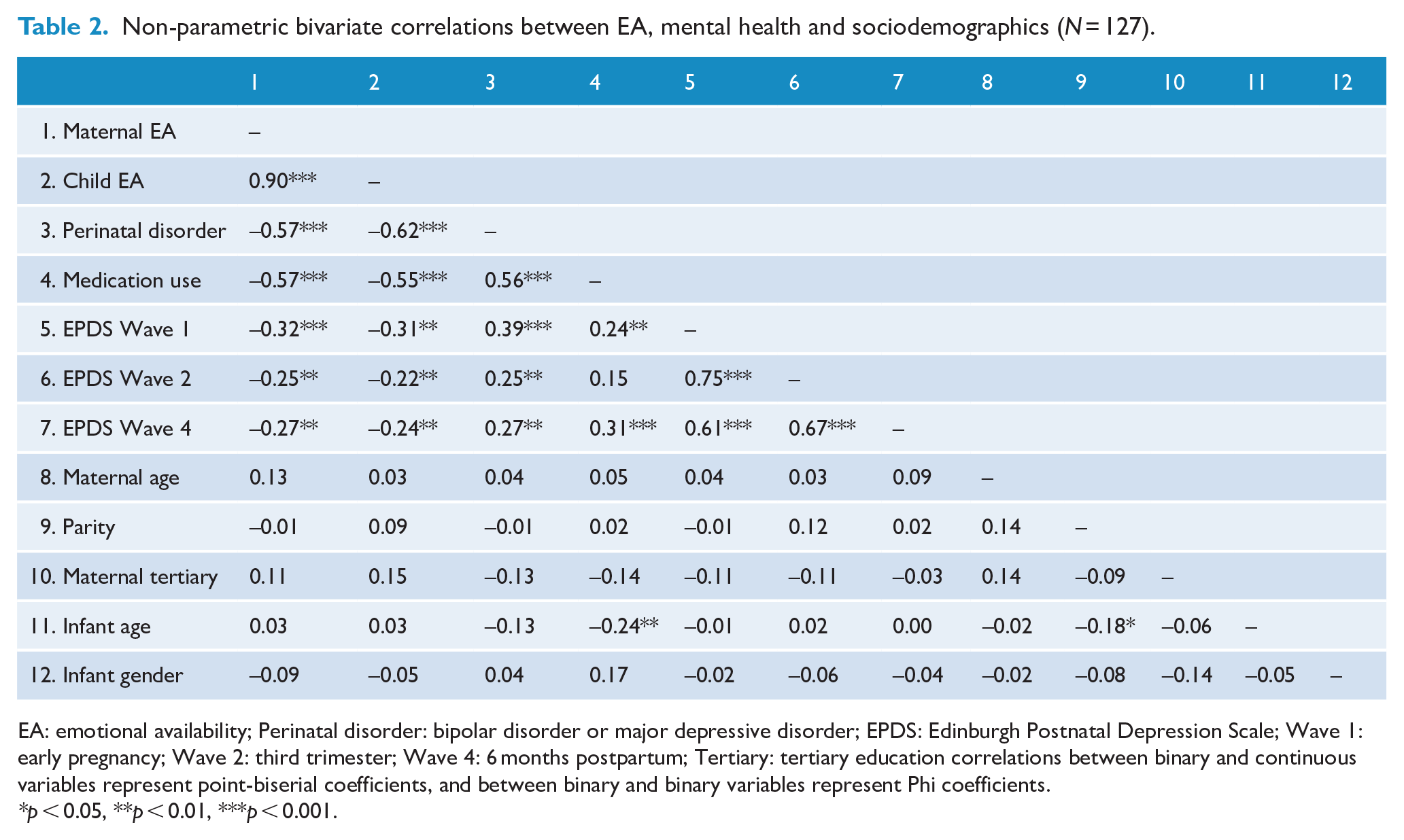
EA: emotional availability; Perinatal disorder: bipolar disorder or major depressive disorder; EPDS: Edinburgh Postnatal Depression Scale; Wave 1: early pregnancy; Wave 2: third trimester; Wave 4: 6 months postpartum; Tertiary: tertiary education correlations between binary and continuous variables represent point-biserial coefficients, and between binary and binary variables represent Phi coefficients.
*p < 0.05, **p < 0.01, ***p < 0.001.
Multivariate models of disorder and EA
For the two MANCOVA models examining the effects of perinatal disorder on combined maternal EA and combined child EA, EMM adjusted for covariates at the sample means are displayed in Figure 1, multivariate F-tests are reported in the text and univariate F-tests are presented in Tables 3 and 4.
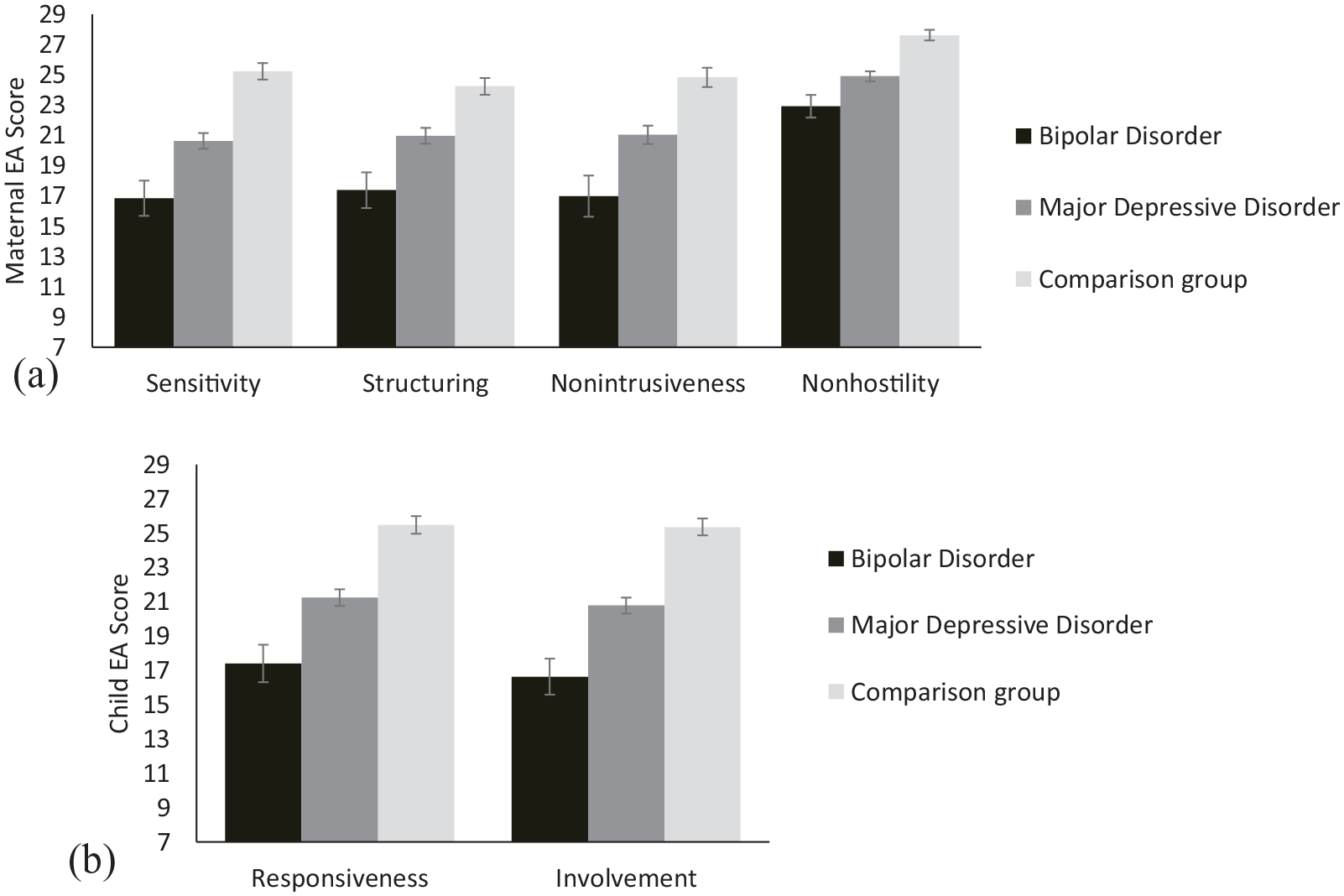
Univariate estimated marginal means (and standard errors as error bars) for disorder groups with (a) maternal EA dimensions and (b) child EA dimensions as outcomes. Estimates are adjusted for covariates.
Univariate F-test results for disorder on each maternal EA dimension.
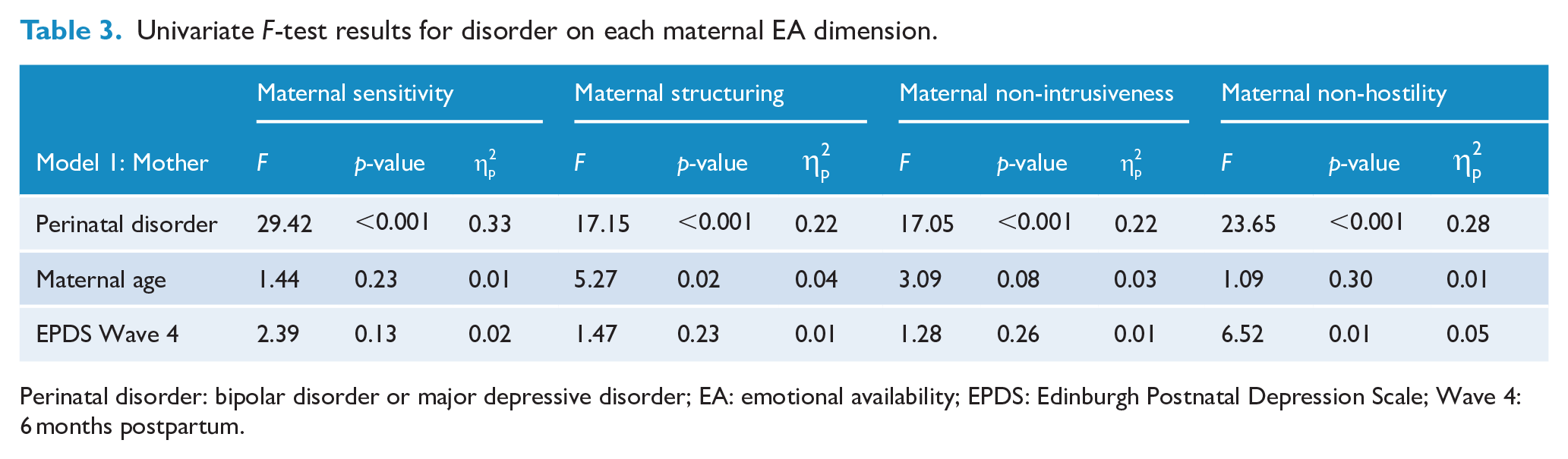
Perinatal disorder: bipolar disorder or major depressive disorder; EA: emotional availability; EPDS: Edinburgh Postnatal Depression Scale; Wave 4: 6 months postpartum.
Univariate F-test results for disorder on each child EA dimension.
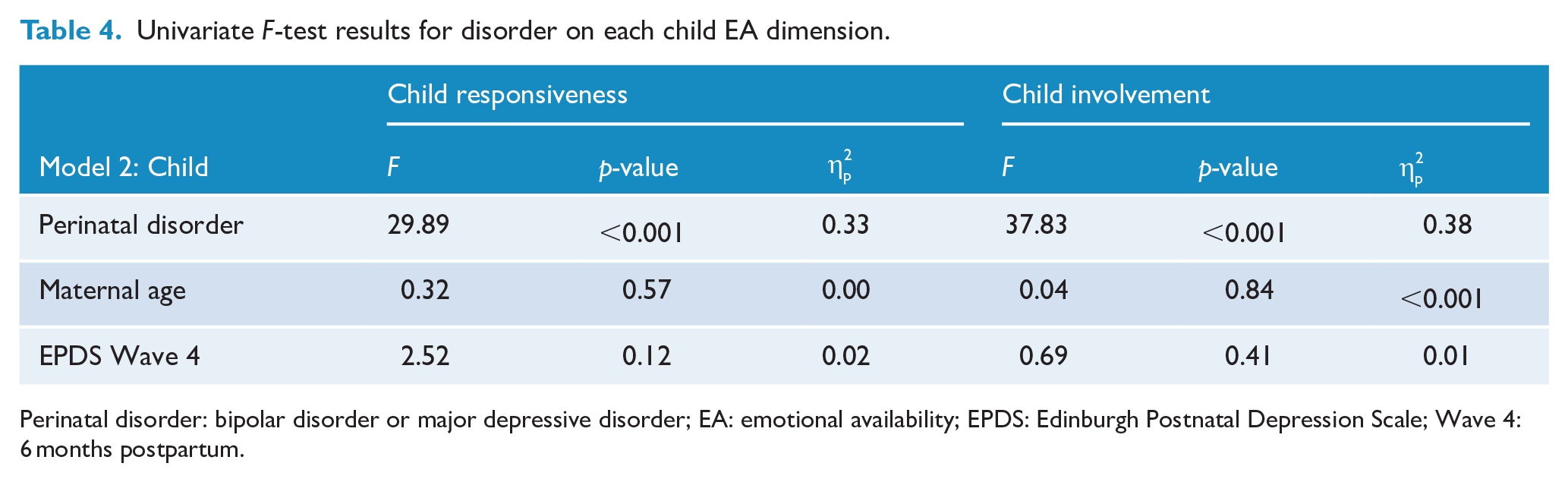
Perinatal disorder: bipolar disorder or major depressive disorder; EA: emotional availability; EPDS: Edinburgh Postnatal Depression Scale; Wave 4: 6 months postpartum.
Model 1 – maternal EA
The first MANCOVA model indicated that after accounting for the effects of maternal age and depressive symptoms, the effect of disorder on maternal EA was significant, F(8, 240) = 6.29, p < 0.001,
Model 2 – child EA
The second MANCOVA model indicated that after accounting for the effects of maternal age and depressive symptoms, the effect of maternal disorder on child EA was significant, F(4, 244) = 14.56, p < 0.001,
Discussion
To our knowledge, this is the first study to investigate the effects of both perinatal BD and perinatal MDD on maternal and infant EA at 6 months postpartum. Our data showed that after adjusting for maternal age and postpartum depressive symptoms, perinatal disorder (BD, MDD, control) accounted for 32.2% of the variance in maternal EA and 36.4% of the variance in child EA. Women with BD and their infants displayed lower EA than women with MDD and their infants, and the control dyads, across all maternal (sensitivity, structuring, non-intrusiveness, non-hostility) and child (responsiveness, involvement) EA qualities (Figure 1).
The magnitude of difference in EA between each group comparison was large (Cohen, 1988), which interpreted as an approximate indicator of clinical significance suggests clinically meaningful differences (Jacobson and Truax, 1991). Among women with a perinatal disorder, both BD (Cohen’s d = 2.43, p < 0.001) and MDD (Cohen’s d = 2.43, p < 0.001) had the greatest effect on maternal sensitivity (Table 3). Comparison of EMM showed that women with disorders differed the most from women without disorders, in their maternal sensitivity scores (Figure 1). For infants, mother’s perinatal disorder had large effects on their EA, accounting for 33% of the variance in their responsiveness towards their mothers (Cohen’s d = 2.67, p < 0.001) and 38% of the variance in their involvement towards her (Cohen’s d = 2.95, p < 0.001). These interaction patterns resemble observations made by Anke et al. (2019, 2020) at 3 and 12 months postpartum, who described mothers with BD in their cohort as having subdued expressions of positive affect and less sensitivity, and their infants as quiet and under-involving, with similar subdued affect as opposed to irritable and easily dysregulated. The EA quality with the least deficits among our cohort was maternal non-hostility, suggesting women in our cohort were not predominantly characterised by negative affect and covertly or overtly hostile language and behaviour. Similarly, across the three domains of maternal behaviour assessed, Anke et al.’s (2019, 2020) cohort showed the least deficits in maternal negative affect and behaviour.
Comparing women with BD to women with MDD in our cohort, women with BD and their infants were rated significantly lower across all six EA qualities. This trend is consistent with that reported by Logsdon et al. (2015) for lower maternal sensitivity and infant reciprocity among their BD compared to unipolar depression group, albeit their findings did not reach significance. Our results also support seminal studies by Radke-Yarrow and colleagues that found offspring of women with BD were more likely to be insecurely attached than offspring of women with unipolar depression (e.g. Radke-Yarrow et al., 1985, 1995; DeMulder and Radke-Yarrow, 1991). Our findings build on these papers by going beyond maternal sensitivity and including additional maternal qualities, such as structuring, intrusiveness and hostility. In our cohort, while women with and without disorders differed the most in terms of their maternal sensitivity (Figure 1(a)), the largest mean difference in EA between women with BD and MDD was the proportionately higher intrusiveness among women with BD (Mdiff = 4.05, p = 0.02). While Anke et al.’s results did indicate that women with BD showed higher intrusiveness than women without disorders, their study did not include a unipolar depression group; thus, this finding cannot be compared. Notably, the observational tool employed by Anke et al., the Parent-Child Early Relational Assessment (PCERA; Clark, 1985), combines intrusiveness, insensitivity and inconsistency into a single maternal subscale; thus, unique effects on each of these maternal qualities are not reported. Accordingly, by examining multiple disorders and interaction qualities independently, our study contributes novel findings to the existing literature.
Consistent with studies in the broader literature mentioned earlier (e.g. Hayes et al., 2013; Ramsauer and Achtergarde, 2018), our findings confirm a negative association between perinatal mental disorder, with onset prior to childbirth, and mother–infant EA. In addition, the lower EA among women with BD and their infants, compared to dyads in the MDD group, supports the notion that the severity and complexity of the disorder are adversely associated with the mother–infant relationship. BD are more severe and complex than major depression. In the broader mother–infant relationship literature, there is evidence for interaction quality being worse in the context of more severe or complex (e.g. chronic, comorbid) psychopathology (Hatzis et al., 2017). Perhaps inconsistency in mood, such as cycling between mania and depression, has greater effects on EA than consistent moods (e.g. consistently depressed). The greatest deficits in interaction quality are characterised by disorganisation, including confusion, inconsistency, or frightening behaviours and affect (Van Ijzendoorn et al., 1999). Researchers have shown maternal disorders and certain personality traits (Hazell Raine et al., 2020; Lorenzini and Fonagy, 2013) particularly those characterised by greater emotional dysregulation, such as borderline personality disorder, to have adverse associations with mother–infant relationship quality, including EA (Kim et al., 2012; Kluczniok et al., 2018; Newman-Morris et al., 2020). Accordingly, the inconsistency in mood that is characteristic of BD could be a potential mechanism underlying the lower EA associated with BD compared to MDD. For example, qualitative research has detailed confusion among toddlers in response to the changes in the mood of a parent with BD (Backer et al., 2017). The degree of inconsistency and mixed features of perinatal BD may be a critical factor that impacts the developing mother–infant relationship. Recommended next steps may be to broaden the focus from categorical disorder classifications to examining the underlying symptom constellations associated with BD 1 and BD 2 in combination with maternal personality traits and how the interaction between BD symptom constellations and maternal personality traits may relate to attachment strategy formation.
Psychotropic medication use adds further complexity and could impact mother–infant interaction quality beyond the disorder itself. While antidepressants are the most common medication prescribed for perinatal depression (Molenaar et al., 2020), mood stabilisers, such as lithium, are most prescribed to treat BD (Wesseloo et al., 2017). Polypharmacy is also common, with half of the women with BD in our cohort reporting use of multiple classes of medication (antidepressant, antipsychotic, mood stabiliser). The impact of psychotropic medication use on pregnancy among women with BD has gained increasing attention (Haskey and Galbally, 2017; Wisner et al., 2019); however, we did not identify any studies that included mother–infant interaction quality as an outcome. The sudden cessation of medication use during pregnancy has been shown to increase the risk of relapse and onset of new episodes among women with BD (Wesseloo et al., 2016); thus, it is plausible that medication is a factor that could also impact EA. Unfortunately, our limited sample size and lack of heterogeneity in our BD group (see Table 1) precluded us from analysing the effects of medication dose and type (pre- and post-pregnancy) on EA. Furthermore, medication use between groups significantly differed, particularly polypharmacy, with no cases of polypharmacy in the control group and less than 5% in the MDD group. High-quality studies with a larger sample of women with BD, medicated and unmedicated, are needed to address the effects of BD and medication use on the mother–infant relationship (Galbally et al., 2018).
Despite these limitations, our study has many strengths. Most studies measure the quality of the mother–infant relationship according to a single construct, typically maternal sensitivity (see Hazell Raine et al., 2020), and employ brief observations, often a few minutes. Our study involved longitudinal prospective assessment over the perinatal period, comparing three groups (MDD, BD, control) on multiple, repeated measures of maternal mental health and observations that exceeded the 20-minute minimum recommended length for EAS observation (Biringen et al., 2008). For researchers with the means to collect larger datasets of women with BD and MDD, further analyses of whether EA differs according to features of the disorder and medication use during and after pregnancy are encouraged.
Conclusion
Howard and Khalifeh’s (2020) recent review of perinatal mental health research highlighted the gaps that remain regarding our understanding of the full range of perinatal disorders and which of these women are in particular need of parenting support. Research concerning the mother–infant relationship among women with perinatal BD is disproportionately scarce (Rusner et al., 2016; Stein et al., 2014). Our study contributes novel findings to the BD literature regarding maternal and infant EA at 6 months postpartum. Further research involving women with perinatal BD and MDD is needed to corroborate our significant findings.
Footnotes
Acknowledgements
The authors would like to thank those who have supported the development of SMPEWS, including Marinus van Ijzendoorn and Michael Permezel, and Marian Bakermans-Kranenburg, Peter Fonagy and Robert Emde for their advice on the design of the postpartum interactional assessment. In addition, we thank our fellow SMPEWS investigators – Donna Kristianopulos and Janine Spencer. The authors thank study coordinator Kylie Marston for her contribution to SMPEWS. We are also sincerely grateful to the study participants who have contributed a substantial amount of time to participate in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported through the 2017–2018 Research Award from the Spinnaker Health Research Foundation.