
Abstract
The obstetric care of pregnant women with serious mental illnesses (SMI) such as schizophrenia and bipolar affective disorders is often complex and challenging. There is now a large body of evidence suggesting women with SMI are at increased risk of obstetric complications [1–3] as well as psychiatric adverse events in the antenatal and postnatal periods [4,5]. These women also tend to have inadequate antenatal care, either presenting late to obstetric services [6] or not regularly attending their appointments [7]. Given that obstetric complications are recognized as a risk factor for schizophrenia in the offspring, it has been proposed that special attention needs to be given to this group of pregnant women, as a primary prevention strategy for schizophrenia [8]. To date there has been little research into specific interventions targeting this at risk group. There is some evidence to suggest that comprehensive support, in particular non-drug support, (such as involvement of families and liaison between midwives, public health nurses and psychiatrists) has the potential to ameliorate Positive and Negative Syndrome Scale (PANSS) scores in pregnant women with schizophrenia [9].
In addition to the opportunity for provision of comprehensive, individualized care for these women, antenatal services are ideally placed to screen for common perinatal psychopathology such as depression and anxiety. This appears important, as anxiety and depression during pregnancy are independently linked to adverse foetal development and related outcomes [10,11]. The course of anxiety and depression throughout the pregnancy also appears significant. Lee et al. [12] reported that the prevalence of antenatal anxiety and depression was characterized by a U-shape curve, with both decreasing from the first trimester to the second trimester and then increasing again in the third trimester.
During the antenatal period, universal screening is undertaken by many obstetric services in Australia using the Edinburgh Postnatal Depression Scale (EPDS) [13]. Not withstanding its designation, the EPDS has been validated for use during pregnancy [14] and appears well accepted by patients [15]. It also has satisfactory sensitivity and specificity for detecting an antenatal major depressive disorder (MDD) [16]. There is evidence to suggest that a 4-point change in the total score may indicate clinical significance [17] and furthermore, as the EPDS scale contains an anxiety subscale with three anxiety related items (questions 3–5), it may also be used to screen for anxiety [18]. Despite the considerable research into the screening for perinatal anxiety and depression in the general population, to date there has not been any reported use of the EPDS in women with SMI and little is known about the pattern and course of anxiety and depression in these women during the perinatal period [19]. This appears especially important as anxiety and depression often co-occur and are characteristically more prominent within the clinical picture of women with schizophrenia compared to men [20,21], and that anxiety frequently co-occurs in patients of both genders with bipolar affective disorders [22].
In Western Australia we have established a specialist antenatal clinic for pregnant women with SMI, in particular, those with existing schizophrenia and related psychosis and bipolar affective disorders, type 1 and 2. The clinic, which is a collaboration between psychiatry and obstetric services, utilizes a small, consistent multidisciplinary team to provide comprehensive antenatal care for these at-risk women. The aim of this preliminary study was to use serial EPDS scores to assess anxiety and depressive symptoms in a sample of pregnant women with serious mental illness.
Method
In 2007, we established the Childbirth and Mental Illness (CAMI) Clinic, which is situated at King Edward Memorial Hospital (KEMH), a tertiary maternity hospital in Perth, Western Australia. The clinic has a multidisciplinary team, which comprises a midwife, a general practitioner/obstetrician, a psychiatrist and a social worker, all with sessional capacity, who come together during the running of the weekly outpatient clinic. The small team approach aims to provide continuity and consistency of care to promote trust, and emphasizes a collaborative partnership with the patient, their families and their community mental health providers. In addition to their routine antenatal care, the women are reviewed regularly by the attending psychiatrist, as well as the social worker. Monitoring of foetal growth, nutritional status and metabolic complications are also routine. Planning for the delivery and the postnatal period includes a guided tour of the delivery ward as well as reviewing the patient's support network with referral to community agencies as appropriate.
The tertiary hospital mandates that EPDS screening is completed on all referred pregnant women at booking (first antenatal appointment) and again at 32 weeks gestation. A total of 48 women with SMI attended the CAMI clinic and delivered their babies between December 2007 and November 2009. All these women had a diagnosis of schizophrenia, schizoaffective disorder, or bipolar affective disorder, made by an adult mental health service, a private psychiatrist or a consultant psychiatrist within the Department of Psychological Medicine at KEMH. Women included in this preliminary study were 27 women (n = 27) who completed the EPDS at both booking and 32 weeks gestation. Of these, 11 had schizophrenia or schizoaffective disorder and 16 had bipolar affective disorders. We were able to obtain scores for the anxiety subscale for 24 women. A retrospective review of the patient case notes was also undertaken to determine demographics, gestation at booking, and attendance rate of these 27 women (group 1) and the other 21 who did not complete one or both of their EPDS (group 2) for comparison. The study was approved by the King Edward Memorial Hospital (KEMH) Ethics Committee.
Statistical analyses
Means were compared using independent sample t-tests (for comparison between groups) or paired t-tests (for comparisons of EPDS scores at first appointment to 32 weeks gestation), and categorical data (gravidity, presence of a partner, diagnoses) were compared using Fisher's exact (χ2) test. An alpha level of 0.0056 was used to allow for multiple comparisons (Bonferroni adjustment).
Results
Data for maternal age, gestation at booking, gravidity, diagnosis, antenatal attendance, and partner presence for the two groups of women, those who completed the EPDS at booking and 32 weeks gestation (group 1) and those who completed one or no EPDS during the antenatal care (group 2) are presented in Table 1. Group 1 had 16 primigravidas (59%) and group 2 had 8 primigravidas (38%). In group1, 22 women (81%) confirmed having a partner compared with 13 (62%) in group 2. These differences were not statistically significant.
Characteristics of the women who completed both EPDS assessments (group 1) and those who completed one or no EPDS assessments (group 2) during antenatal care
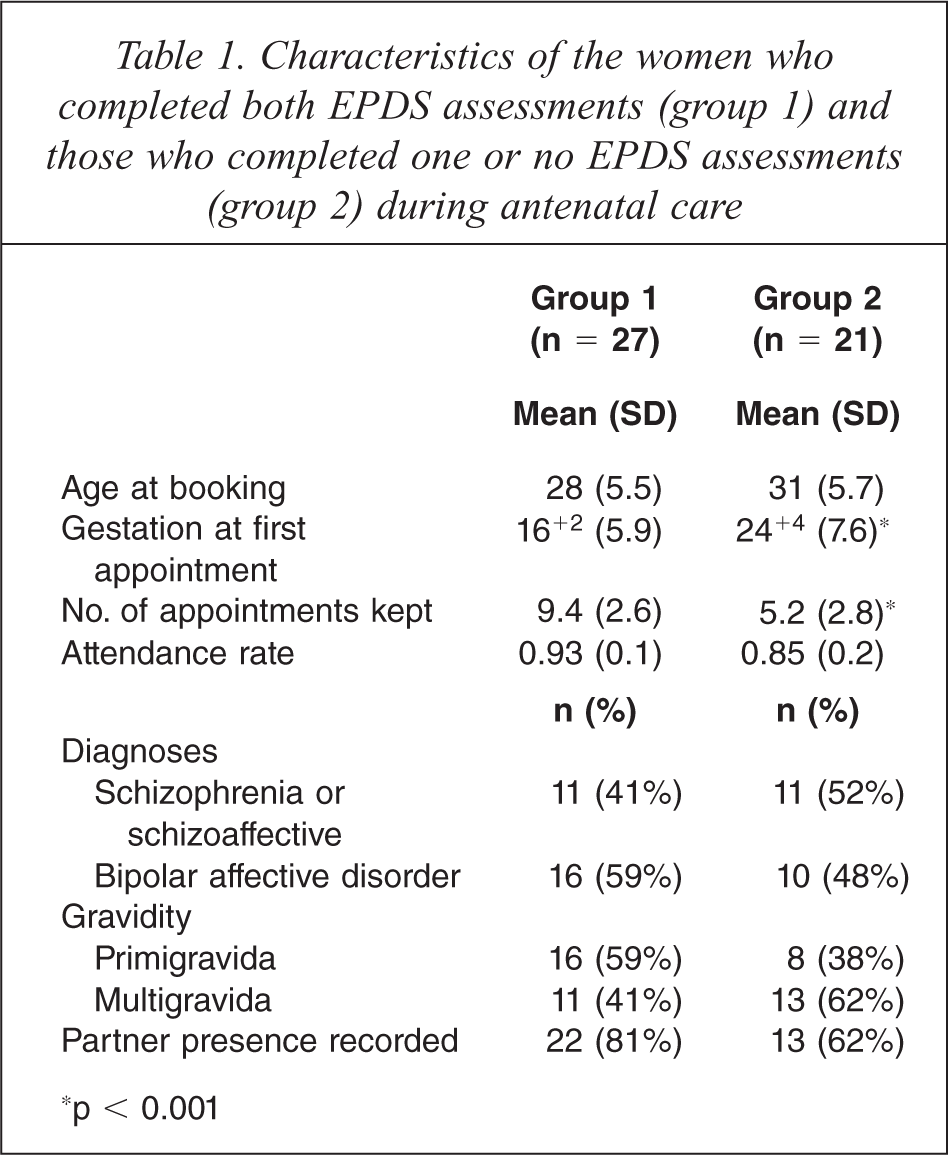
∗p < 0.001
Group 1 women for whom both EPDS scores were available attended the clinic eight weeks earlier in the pregnancy and attended four more appointments on average than group 2 women with one or no EPDS scores. Mean attendance rate to antenatal clinic appointments for all women was 90%.
Total EPDS: For group 1 women (n = 27), mean total EPDS score decreased from 12.2 (SD 7.6) at booking to 8.5 (SD 6.4) at 32 weeks gestation (p = 0.007; Figure 1, upper panel). A comparison of these changes between women with schizophrenia/schizoaffective disorder (n = 11) and bipolar affective disorder (n = 16) revealed no significant difference (p = 0.74; Figure 1, lower panel). Using a total EPDS score of 12 as a cut off (16), nine women who initially scored 12 or above at booking improved to below clinical cut-off by 32 weeks gestation. Individual women's EPDS scores are presented in Figure 2A. Total EPDS scores decreased for 17 women, remained unchanged for four women, and increased for five women (Figure 3A). Using a threshold change of four points (or more) to indicate a reliable change, 13 of the sample improved, ten had no reliable change, and four deteriorated.
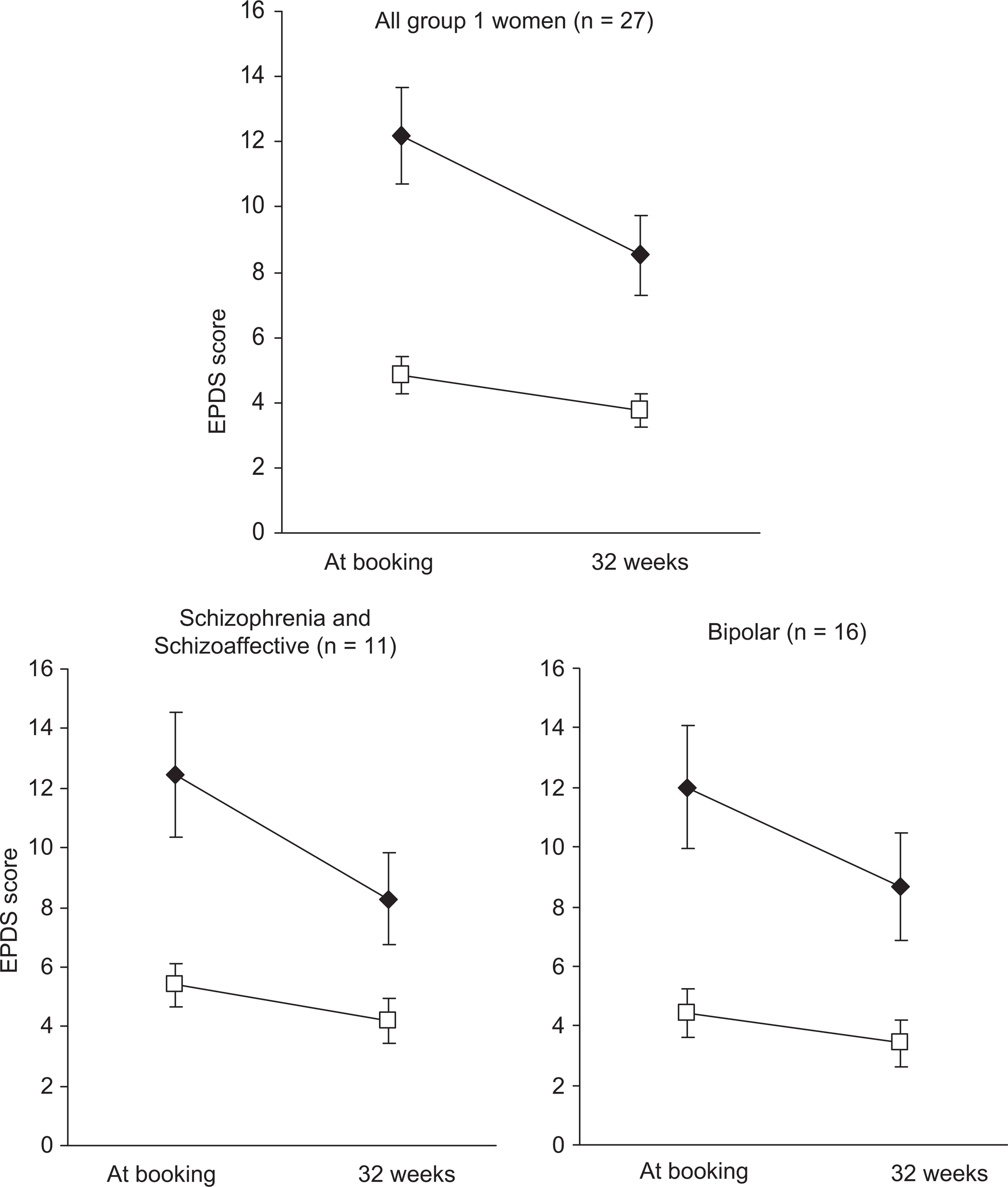
Mean total EPDS (♦) and mean anxiety subscores (□) for all group 1 women (upper panel) and subdivided by diagnosis (lower panel). Error bars are ± 1 standard error of the mean.
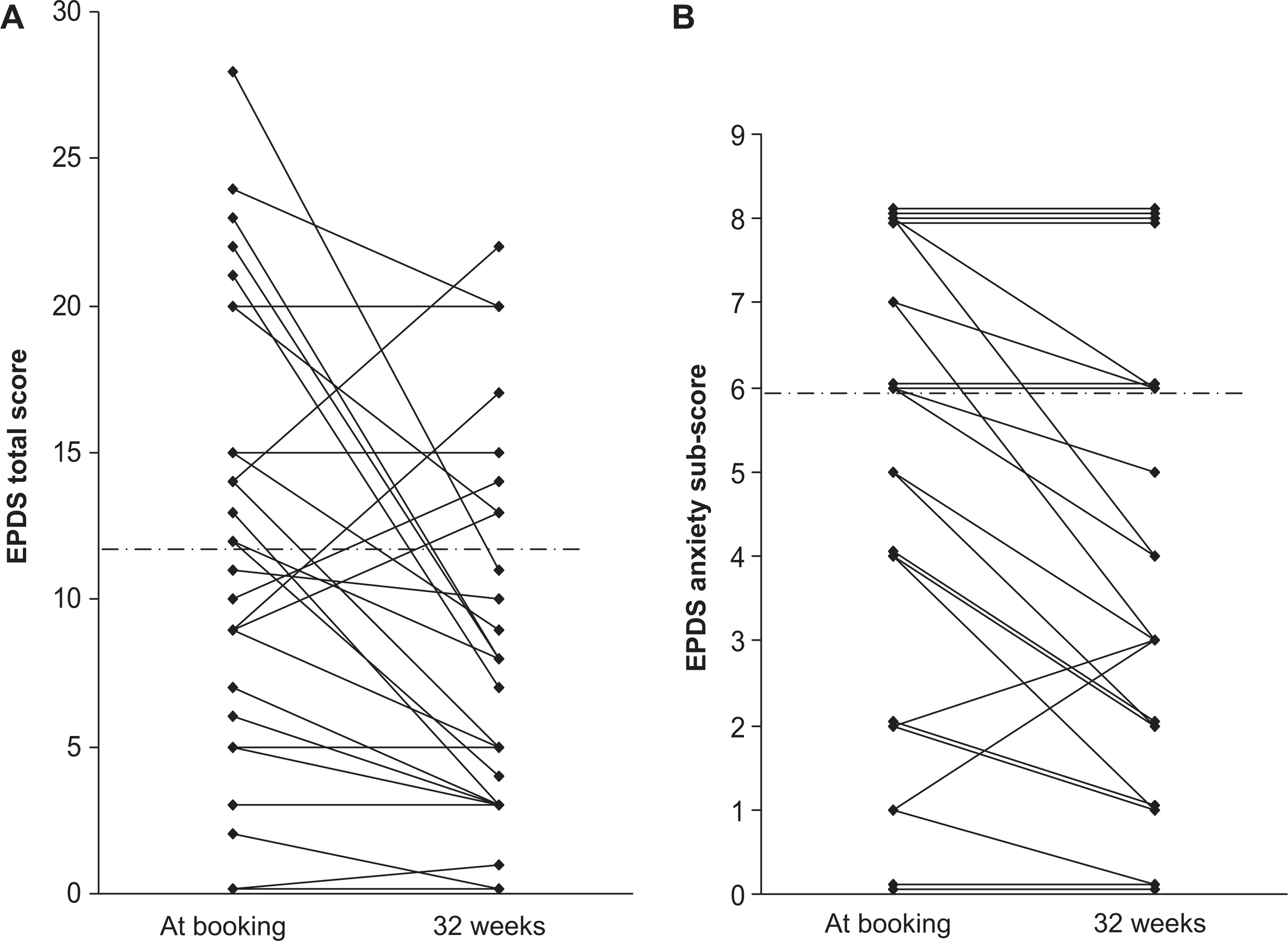
Individual EPDS scores (A) and anxiety subscores (B) at booking and 32 weeks gestation. Overlying points are offset on the y-axis for clarity. The dashed horizontal lines in A and B indicate the cut-off for total EPDS score of 12 and anxiety subscore 6 respectively; scores above these lines indicate likely depression or anxiety.
Anxiety subscores: Anxiety subscores were available on 24 of group 1 women (89%) as the records for three women only indicated their total EPDS score and individual items were not available. Out of a possible nine points, mean anxiety subscores on the EPDS were 4.8 (SD 2.8) at booking and this decreased to 3.8 (SD 2.6) at 32 weeks gestation (p = 0.002, Figure 1, upper panel). A comparison of the changes in anxiety subscores from booking to 32 weeks between women with schizophrenia/schizoaffective disorder and bipolar affective disorder revealed no significant difference (p = 0.76; Figure 1, lower panel). Individual subscores are shown in Figure 2B. Furthermore, 14 women's anxiety subscores decreased from booking to 32 weeks, 8 had no change, and 2 increased (Figure 3B).
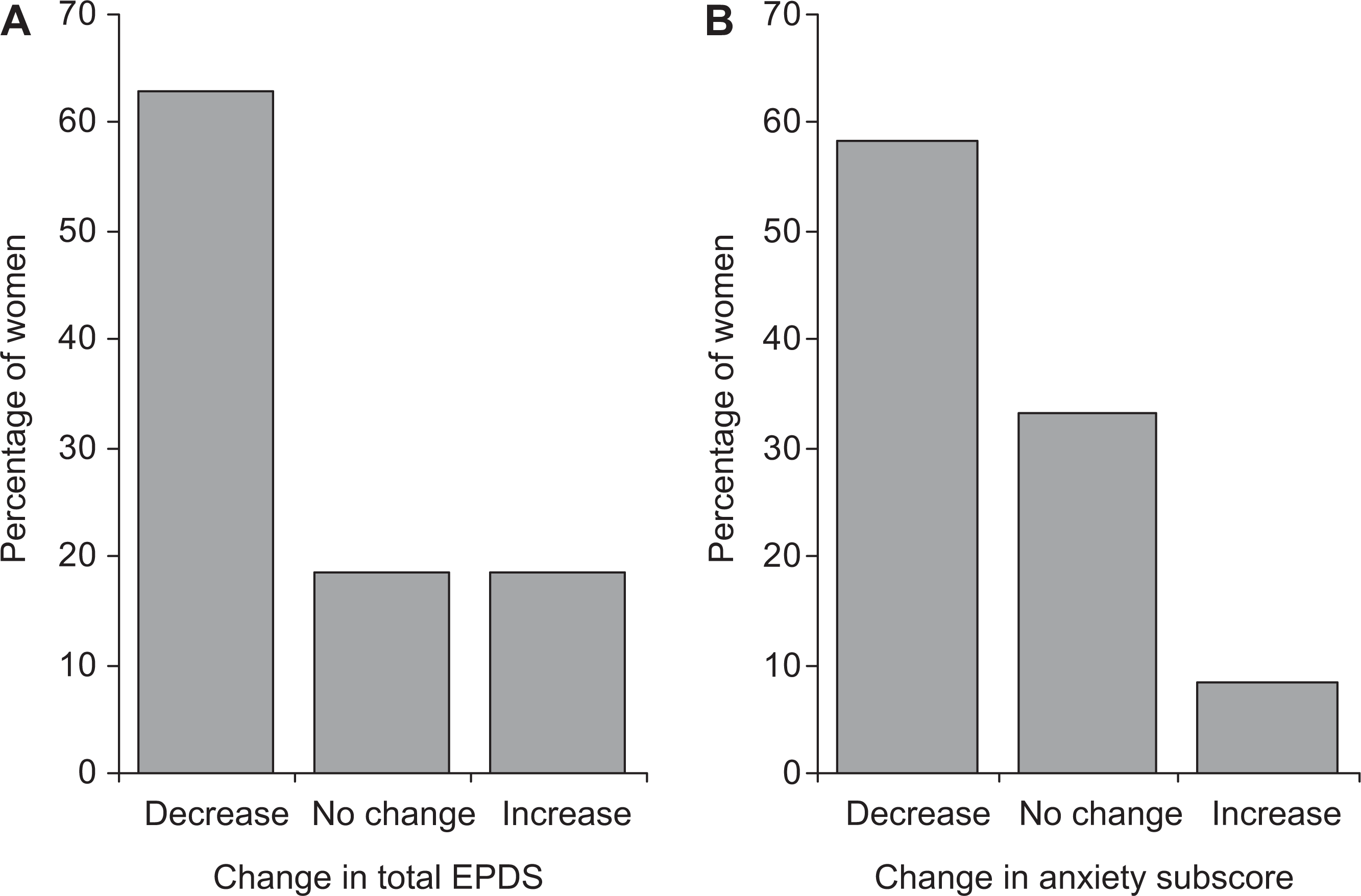
Percentage of women with increase, no change, or decrease in total EPDS scores (A, n = 27), and anxiety subscores (B, n = 24) from first appointment to 32 weeks’ gestation.
Discussion
Our study's primary strength is in using existing universal screening as a marker of progress in a sample of pregnant women with serious mental illness (SMI). The demonstration of a statistically significant 3.7 point drop in the mean EPDS scores between the time of booking and at 32 weeks’ gestation is a finding that requires further investigation. While conclusions regarding the clinical significance of this change in the mean EPDS scores must be interpreted with caution due to a lack of a matched control group, comparisons may be made with some community cohort studies using serial EPDS measurements during the antenatal period. Evans et al.'s [23] large longitudinal study reported higher mean EPDS scores at 32 weeks (6.72) than at 18 weeks (6.62). Van Bussel et al. [24] found higher mean EPDS scores in the first and third trimesters (6.93 and 6.35) compared to the second trimester (6.15) suggesting a U shape distribution for anxiety and depressive symptoms consistent with the findings by Lee et al. [12]. In contrast, Teixeira et al. [25] found a steady modest decline in the mean EPDS scores across the three trimesters (6.55, 6.17 and 5.63 for first, second and third trimesters respectively) in their study. Interestingly in the same study, Teixeira demonstrated a U shape distribution to anxiety symptoms across the three trimesters using a separate anxiety scale.
In comparison to these community samples, our findings are noteworthy on two aspects. Firstly we were able to demonstrate that our cohort had much higher mean EPDS at booking (12.2) than those reported in the population studies, placing them in the high risk category in terms of screening. This also suggests that in the early part of pregnancy, women with SMI may be experiencing significant levels of anxiety and depression. Secondly, the mean EPDS score at booking was above the accepted clinical cut-off of 12 [16], whereas by 32 weeks, it had decreased by 3.7 points, placing it in a lower risk category.
Using the anxiety subscale of the EPDS, as described in Matthey's work [17], we were able to also demonstrate a significant drop in the ‘anxiety scores’ from booking to 32 weeks. This reduction in the anxiety mean scores may be of clinical importance given the impact of anxiety on pregnancy and neonatal outcomes [26].
There is existing literature linking higher rates of obstetric and neonatal complications for women with SMI [2]. Although no results on obstetric complications are available in this study due to small numbers, these risk factors reinforce the importance of these women attending adequate antenatal care. The attendance rate in Group 1 was 93%, and overall was 90%. This attendance rate is comparable to the overall mean attendance rate of our tertiary hospital's antenatal clinics of 84.7% in 2008 (personal communication from A/Manager Business Analysis, KEMH). The mean number of antenatal visits in Group 1 was 9.4 (SD 2.6). This compares favourably with the National Institute for Clinical Excellence (NICE) guideline, which recommends, ‘A schedule of antenatal appointments should be determined by the function of the appointments. For a woman who is nulliparous with an uncomplicated pregnancy, a schedule of ten appointments should be adequate. For a woman who is parous with an uncomplicated pregnancy, a schedule of seven appointments should be adequate’ [27]. The mean number of appointments attended is also important given that Lin et al. found that women with schizophrenia had a significantly lower mean number of prenatal care visits, compared with non-schizophrenia controls [28].
Limitations
Our study has a number of limitations. Although the universal EPDS screening is in place in our institution, only 27 out of 48 women (57%) completed the EPDS at booking and at 32 weeks. Out of 48 women, 21 (43%) women with SMI completed the EPDS only on one occasion or not at all. The non-completion of the EPDS at both screening time points of group 2 women may be partly explained by their comparatively late presentation at first booking. However, once linked in with the clinic, their mean attendance rate was 85% (Table 1) which is comparable to the group 1 women and the general population attending the tertiary hospital. These results may have implications in terms of strategies targeting earlier detection of pregnancy plus priority management of pregnant women with SMI. In addition, our study included patients with a history of schizophrenia, schizoaffective disorders, and bipolar affective disorders. While this grouping is commonly used in clinical practice as ‘psychotic’ or low prevalent disorders, the course of anxiety and depressive symptoms in pregnant women with these individual disorders may be quite varied. Finally much of the research on using the EPDS has been conducted with high prevalent disorders, most notably depression, and therefore its applicability in the psychotic disorders is yet to be determined.
Concluding remarks
Many women approach pregnancy, birth and the postnatal period with significant anxiety and concerns about managing changes during this crucial time. A case could be made that given their complex presentations; women with SMI may have higher levels of anticipatory anxiety than their general cohort. We speculate from our findings that being managed and supported by a small consistent multi-disciplinary team could reduce anxiety and promote attendance at antenatal clinics for these vulnerable women. This preliminary study was unique in its approach of using serial EPDS scores as a marker of progress of pregnant women with SMI. It provides directions for future studies, including validation of the EPDS with measures of psychosis. Furthermore, follow up is recommended into the at-risk postnatal period to determine whether the advantages provided by this specialized approach to care are translated into better outcomes for the woman and her baby.
Footnotes
Acknowledgements
Our thanks to the A/Manager Business Analysis, of King Edward Memorial Hospital, for supplying the overall mean attendance rate of the KEMH general antenatal clinic.