
Abstract
Objective:
Several countries have developed Clinical Practice Guidelines regarding treatment of perinatal depressive symptoms and perinatal use of antidepressant. We aimed to compare guidelines to guide clinicians in best clinical practice.
Methods:
An extensive search in guideline databases, MEDLINE and PsycINFO was performed. When no guidelines were (publicly) available online, we contacted psychiatric-, obstetric-, perinatal- and mood disorder societies of all first world countries and the five largest second world countries. Only Clinical Practice Guidelines adhering to quality criteria of the Appraisal of Guidelines for Research and Evaluation instrument and including a systematic review of evidence were included. Data extraction focussed on recommendations regarding continuation or withdrawal of antidepressants and preferred treatment in newly depressed patients.
Results:
Our initial search resulted in 1094 articles. After first screening, 40 full-text articles were screened. Of these, 24 were excluded for not being an official Clinical Practice Guidelines. In total, 16 Clinical Practice Guidelines were included originating from 12 countries. Eight guidelines were perinatal specific and eight were general guidelines.
Conclusion:
During pregnancy, four guidelines advise to continue antidepressants, while there is a lack of evidence supporting this recommendation. Five guidelines do not specifically advise or discourage continuation. For new episodes, guidelines agree on psychotherapy (especially cognitive behavioural therapy) as initial treatment for mild to moderate depression and antidepressants for severe depression, with a preference for sertraline. Paroxetine is not preferred treatment for new episodes but switching antidepressants for ongoing treatment is discouraged (three guidelines). If mothers use antidepressants, observation of the neonate is generally recommended and breastfeeding encouraged.
Introduction
Depression is a common mental disorder and the leading cause of disability worldwide (World Health Organization, 2017). In high-income countries, up to 15% of people experience at least one major depressive episode in their life (Kessler and Bromet, 2013; Kruijshaar et al., 2005). Women in the Western world are affected twice as often as men (Piccinelli and Wilkinson, 2000). Perinatal depression (considered here as depression arising in the period from conception to the end of the first postnatal year) affects up to 15% of women; a recent meta-analysis showed a pooled prevalence of 11.9% of all pregnancies, without significant differences between prevalence estimates for the prenatal and postnatal periods (Woody et al., 2017).
Several management options are available for depressive disorders (Malhi et al., 2015). Most patients, 65–80%, will be treated by a general practitioner (Alonso et al., 2004; Bijl and Ravelli, 2000; Bushnell et al., 2006; Kovess-Masfety et al., 2007; Verhaak et al., 2009, 2012; Wang et al., 2000), who are instructed to use a stepped care management approach (Van Weel-Baumgarten et al., 2012). Especially in mild to moderate depression, these approaches recommend psychotherapy as first-line treatment, before starting antidepressants. However, in current practice, around 70% of cases are primarily treated with antidepressants (Bushnell et al., 2006; Olfson et al., 2016; Sleath et al., 2001; Verhaak et al., 2012). Subsequently, many patients continue to take medication for a longer period; for example, over 60% of Americans continue medication for 2 years or more and 14% continues medication for 10 years or more (Pratt et al., 2011). Women in their reproductive ages are three times as likely to use antidepressants compared to men (Pratt et al., 2011). In case of a pregnancy, decisions regarding the use of antidepressants are complex.
Although antidepressants are generally considered safe to use during pregnancy, this remains controversial (Simoncelli et al., 2010). Antidepressant use has been associated with an increased risk for cardiovascular malformations (Grigoriadis et al., 2013a), persistent pulmonary hypertension of the neonate (Kieler et al., 2012), poor neonatal adaptation (Grigoriadis et al., 2013b), preterm delivery, lower birth weight (Ross et al., 2013) and psychiatric disorders in offspring (Liu et al., 2017).
Untreated perinatal depression is not risk free either. Children of women who suffered from depression during pregnancy have an increased risk of premature delivery, low birth weight, gestational hypertension (Grigoriadis et al., 2013c; Grote et al., 2010) and perinatal death (Howard et al., 2007). Perinatal depression can also lead to behavioural, emotional, cognitive and motor problems in early childhood (Field, 2011; Talge et al., 2007). Postnatal depression may influence the mother–infant relationship, which can lead to poor infant development and outcomes (Goodman et al., 2011; Tronick and Reck, 2009). Together, decisions regarding the prevention and treatment of perinatal depression (including the use of antidepressants) are complex.
To facilitate this decision-making, several countries have developed ‘Clinical Practice Guidelines’ (CPGs), to guide clinicians in choosing the most efficacious and least harmful intervention. According to the Institute of Medicine, CPGs are based on a systematic review of evidence and include recommendations to optimize patient care (Graham et al., 2011). The objective of this study was to review the content of the internationally available guidelines on the treatment of perinatal depression and the perinatal use of antidepressants.
Methods
Identification of guidelines
We initially performed an extensive search in databases for CPGs using the terms ‘pregnancy’, ‘mood disorders’, ‘depression’ and/or ‘antidepressants’. The following databases were searched: National Guideline Clearinghouse (US AHRQ), National Institute for Health and Care Excellence (UK): Evidence Services, Canadian Medical Association Infobase: CPG, Guidelines, National Health and Medical Research Council (NHMRC) (Australia): CPGs and the Guidelines International Network (G-I-N). Second, we searched MEDLINE (accessed via PubMed) using a combination of free text terms (antidepressant, pregnancy, antenatal period, depression, prenatal period, mental health), limiting the results with a filter to retrieve guidelines only. Third, we searched PsycINFO using a combination of title keywords (depression OR mental health OR mood disorder AND guideline), since PsycINFO does not have a search limit for guidelines and would otherwise retrieve too many hits.
Consecutively, we identified all professional societies of obstetricians and gynaecologists and all professional societies of psychiatrists for countries for which we did not yet retrieve a guideline. For feasibility reasons, we limited our search to societies of first world countries and the largest second and third world countries. First world refers to ‘so called developed, capitalist, industrial countries, roughly, a bloc of countries aligned with the United States after World War II, with more or less common political and economic interests’ (source: nationsonline.org). These include 25 countries: the United States, Canada, Australia, New Zealand, Japan, Korea, the United Kingdom, France, Germany, Belgium, the Netherlands, Spain, Italy, Portugal, Turkey, Greece, Luxembourg, Israel, Austria, Switzerland, Ireland, Sweden, Norway, Iceland and Denmark. In addition, we searched for guidelines in large second and third world countries including Brazil, China, India, Mexico and South Africa. When no guidelines were (publicly) available online, we contacted perinatal and mood disorder societies and send two reminders to non-responders.
Finally, we sent out an email to the members of the Marcé society (an international society for perinatal health) and to our international contacts asking for information on missing guidelines, independent on country of origin.
Selection of guidelines
Only CPGs, defined as statements that include recommendations, intended to optimize patient care, that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options, were selected. These should adhere to the quality criteria of the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument (www.agreetrust.org). To avoid documents not meeting these quality criteria, consensus statements and guidance papers were excluded from this review. There were no limits for publication date or language. CPGs that did not comment on the perinatal management of mood disorders and/or on the perinatal use of antidepressants were excluded. Only the latest or more complete version of a guideline was selected when several versions of the same guideline were available.
Data extraction
Data extraction focussed on recommendations before, during and after pregnancy. Recommendations were investigated both for newly arising symptoms of depression and for pre-existent antidepressant use. We included recommendations regarding management of pre-existent antidepressant use, preferred treatment in newly depressed patients and breastfeeding with antidepressants. Recommendations were scored as follows: (blank) no mention of the measure in the guideline, (0) measure mentioned in the guideline but without a clear direction of the recommendation (no positive or negative advice), (+) measure advised by guideline or (–) measure discouraged by guideline.
Results
Our guideline database search strategy produced a set of 1000 articles. Our PubMed search added another 22 articles and our PsycINFO search 72. Of these 1094 articles, 1062 were excluded after screening on title and abstract (Figure 1). Our search strategy through the professional societies, the Marcé Society and international contacts resulted in an additional eight articles. After thorough assessment, 24 articles were excluded for not being an official CPG. This resulted in a total of 16 guidelines originating from 12 countries (ACOG Committee on Practice Bulletins-Obstetrics, 2008; American Psychiatric Association, 2010; Austin et al., 2017; BC Reproductive Mental Health Program, 2014; Dansk Psykiatrisk Selskab, et al., 2014; DGPPN et al., 2015; Li and Ma, 2015; MacQueen et al., 2016; Malhi et al., 2015; Management of Major Depressive Disorder Working Group, 2016; Ministry of Health, 2012; Ministry of Health, Social Services and Equality, 2014; National Collaborating Centre for Mental Health, 2014; Nederlandse Vereniging voor Obstetrie en Gynaecologie, 2012; Nordeng and Jettestad, 2015; Scottish Intercollegiate Guidelines Network (SIGN), 2012). In addition, we received information on the absence of a national guideline from the following countries: Austria, Belgium, France, Israel, Luxembourg, Mexico, Portugal, South Africa, Sweden, Switzerland and Turkey. Guidelines from India and Israel are in progress.
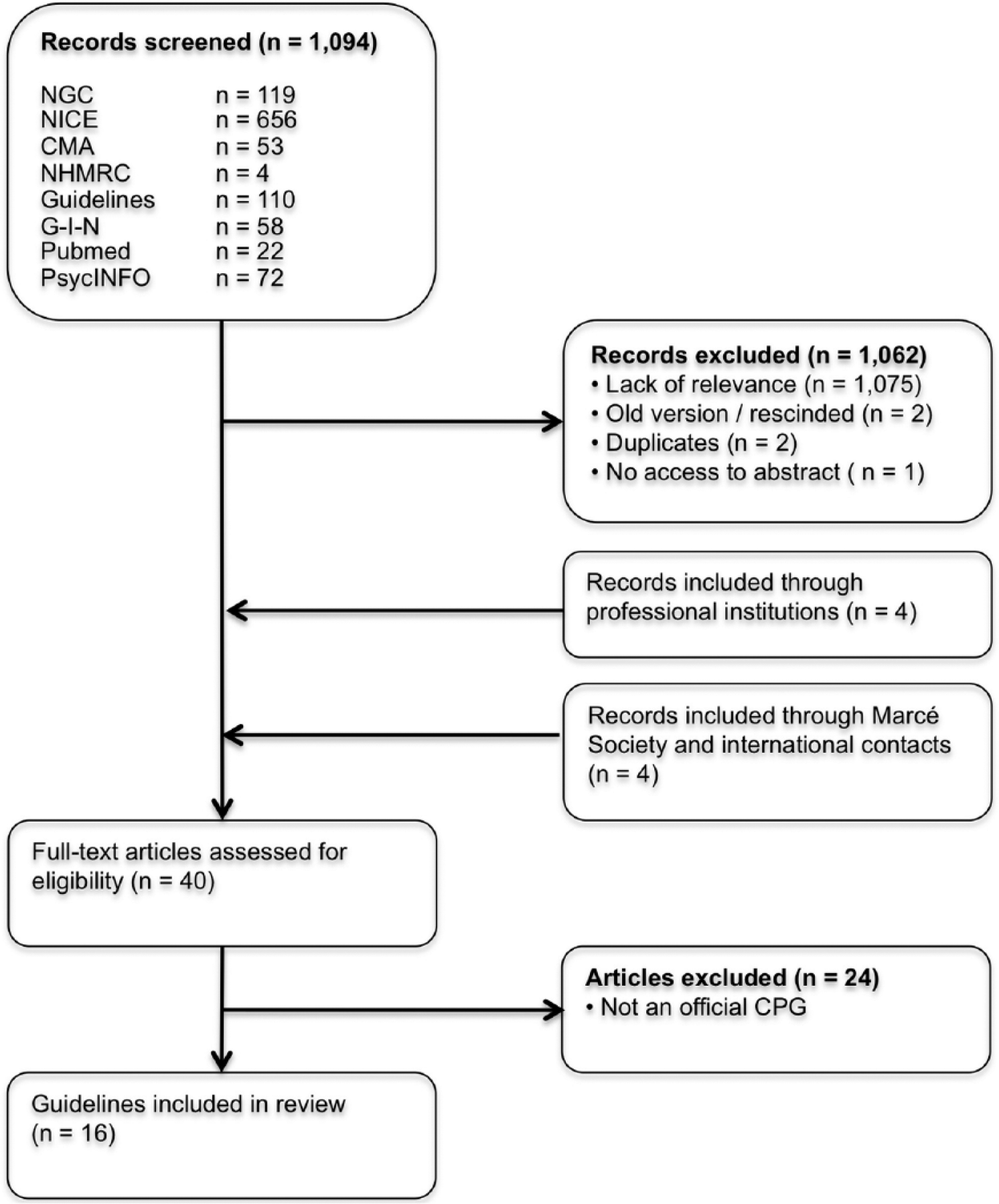
Flowchart of the article selection process.
Table 1 shows the specifics and recommendations of these guidelines. Eight guidelines were exclusively on perinatal management; the remaining guidelines were general guidelines on treatment of depression but included a section on perinatal recommendations.
Summary of guideline recommendations pre-, during and post-pregnancy and perinatal medication recommendations.
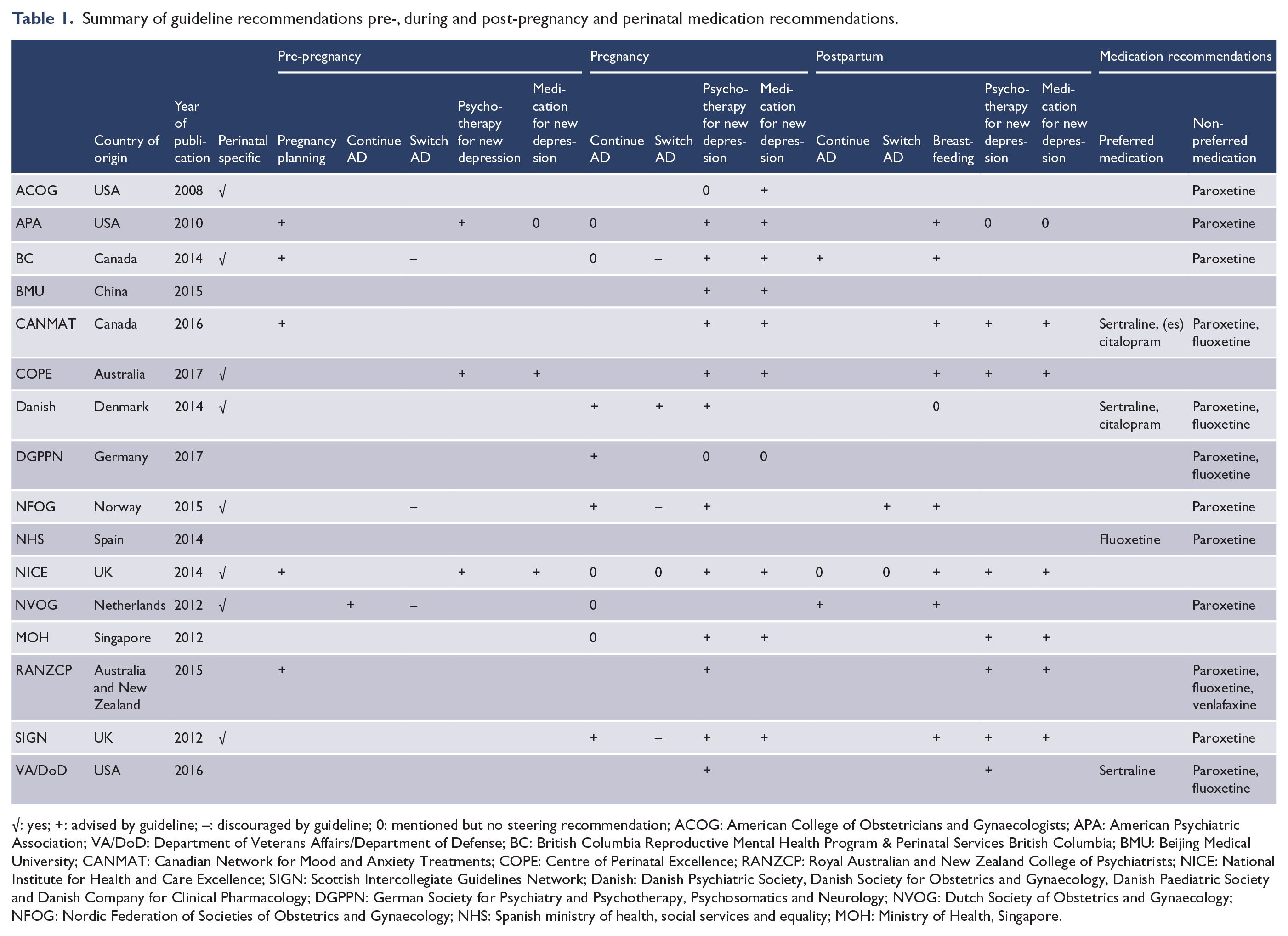
√: yes; +: advised by guideline; –: discouraged by guideline; 0: mentioned but no steering recommendation; ACOG: American College of Obstetricians and Gynaecologists; APA: American Psychiatric Association; VA/DoD: Department of Veterans Affairs/Department of Defense; BC: British Columbia Reproductive Mental Health Program & Perinatal Services British Columbia; BMU: Beijing Medical University; CANMAT: Canadian Network for Mood and Anxiety Treatments; COPE: Centre of Perinatal Excellence; RANZCP: Royal Australian and New Zealand College of Psychiatrists; NICE: National Institute for Health and Care Excellence; SIGN: Scottish Intercollegiate Guidelines Network; Danish: Danish Psychiatric Society, Danish Society for Obstetrics and Gynaecology, Danish Paediatric Society and Danish Company for Clinical Pharmacology; DGPPN: German Society for Psychiatry and Psychotherapy, Psychosomatics and Neurology; NVOG: Dutch Society of Obstetrics and Gynaecology; NFOG: Nordic Federation of Societies of Obstetrics and Gynaecology; NHS: Spanish ministry of health, social services and equality; MOH: Ministry of Health, Singapore.
Pre-pregnancy
Three guidelines discourage switching antidepressants. The Dutch Society of Obstetrics and Gynaecology (NVOG; the Netherlands) advises to continue antidepressants if the patient is psychiatrically stable.
With regard to initial therapy for new depressive symptomatology, the American Psychiatric Association (APA; USA), Centre of Perinatal Excellence (COPE; Australia) and National Institute for Health and Care Excellence (NICE; UK) guidelines give detailed recommendations. All three advise psychotherapy as initial treatment. In more severe cases of depression, the COPE and NICE guidelines advise antidepressants as initial therapy.
Pregnancy
During pregnancy, four guidelines advise to continue antidepressants. Five other guidelines mention the possibility of continuation but do not specifically advise or discourage continuation. Three guidelines discourage switching antidepressants during pregnancy. In contrast, the Danish guideline promotes switching when unfavourable antidepressants (paroxetine and fluoxetine) are used.
Most guidelines agree on psychotherapy as initial treatment for mild to moderate depression and antidepressants as initial therapy for severe depression. Only the American College of Obstetricians and Gynaecologists (ACOG; USA) guideline recommends antidepressants as preferred initial therapy instead of psychotherapy and independent of symptom severity.
There is general consensus that potential harms and benefits of antidepressants during pregnancy should be discussed by the clinician with the patient. This way, patients can make well-informed decisions on preferred treatment.
Management around delivery
Most guidelines recommend a hospital delivery, which is standard in most countries. In the Netherlands and Canada, home births are still common; therefore, these guidelines explicitly mention a hospital delivery with additional observation as preferred option.
Postpartum observation of the neonate is generally recommended but the length of observation is variable (ranging from 12 hours to 3 days). The BC guideline (Canada) recommends more intense monitoring of the neonate, including pulse oximetry for early detection of persistent pulmonary hypertension and on indication neonatal serum levels of antidepressants.
Postpartum
BC (Canada) and NVOG (the Netherlands) specifically recommend continuation of antidepressants to prevent relapse of depressive symptoms. For new episodes, most guidelines agree on psychotherapy as initial treatment for mild to moderate depression and consideration of antidepressants as initial therapy for severe depression. Most guidelines agree on encouraging breastfeeding, independent of the kind of antidepressant medication the patient is taking. The Nordic Federation of Societies of Obstetrics and Gynaecology (NFOG; Norway) advises switching medication when breastfeeding with unfavourable medication. Sertraline is named as favourable medication mainly due to its low level in breast milk and infants serum.
Medication preference
Recommended medication preferences are often not pregnancy stage specific. In general, guidelines agree on avoiding paroxetine during pregnancy, since the use of paroxetine is associated with increased risk of congenital cardiovascular malformations in the newborn (Grigoriadis et al., 2013a). In addition, the ACOG guideline (USA) recommends foetal examination by echocardiography if the foetus is exposed to paroxetine during early pregnancy.
Five guidelines marked fluoxetine as ‘unfavourable’, due to its long half-life and its presence in breast milk. Remarkably, the NHS (Spanish ministry of health, social services and equality; Spain) mentions fluoxetine as preferred medication.
There is general consensus on sertraline as preferred medication by the guidelines mentioning preferences for the postpartum period, mainly due to its favourable profile during lactation (Pinheiro et al., 2015). CANMAT (Canadian) and the Danish guideline also mention citalopram as preferred medication because of its minimized risk during lactation and available data on effectiveness during the postpartum period (Molyneaux et al., 2014).
Discussion
For new depressive episodes, there is general consensus within guidelines for what is considered ‘best clinical practice’. Guidelines recommend, independent of pregnancy stage, to discuss all potential treatment options available and their potential harms and benefits during and after pregnancy. Most guidelines agree that psychotherapy, especially cognitive behavioural therapy (CBT), should be considered as initial treatment for mild to moderate depression, both during pregnancy and the postpartum period. Psychotherapy, such as CBT or interpersonal therapy, has a robust treatment effect for depressive disorder during pregnancy (Van Ravesteyn et al., 2017) and research to other treatment options like bright light therapy is still ongoing (Bais et al., 2016). In more severe cases, antidepressants are preferred treatment options, although, until this date, there are no controlled studies on the effects of psychotropic medication for antepartum mental disorders (Van Ravesteyn et al., 2017); the consequence of ethical constraints of conducting clinical trials with pregnant participants. Paroxetine is not a first-choice treatment option, considering its possible increased risk for congenital heart malformations. Preferred medications during the perinatal period include sertraline and citalopram. Breastfeeding is encouraged with sertraline as preferred medication.
More complicated is the management of pre-pregnancy use of antidepressants and continuation during pregnancy. Unfortunately, evidence on the risks and benefits of tapering antidepressants during pregnancy is limited. One naturalistic study (n = 201) of women with long-standing depression (mean duration of illness 15.4 years) showed a significant increased risk of relapse in pregnant women who discontinued their medication, compared to those continuing medication (44 [68%] vs 21 [26%]) (Cohen et al., 2006), while another naturalistic study (n = 778) showed no clear difference in relapse rates of depression (16% in total) between women continuing and discontinuing antidepressants (Yonkers et al., 2011). Randomized controlled trials (RCTs) are currently lacking with only one RCT in progress (Molenaar et al., 2016). Four guidelines advise continuation of antidepressants during pregnancy, which is remarkable given the scarce evidence. Unfortunately, none of the guidelines discusses treatment options for patients with current depressive symptomatology despite antidepressant use.
Most guidelines acknowledge the importance of personalized medicine. For suitable decision-making, the following should be taken into consideration: psychiatric history and indication for antidepressant medication, current psychiatric symptoms, previous attempts of tapering medication, availability of alternative treatment options such as preventive psychotherapy and the presence of a social support network. Moreover, clinical algorithms need to be developed to improve decision-making. Currently, a pilot study is being executed to investigate if a patient decision aid (PDA) tool can reduce decision-making difficulty and lead to better treatment outcomes in pregnant women with antidepressant use (Vigod et al., 2016).
Overall, the guidelines have good quality (Santos et al., 2012), but most CPGs were not specifically developed for pregnant women and contained limited information on the measures of implementation and audit of the proposed measures. In our review, only eight guidelines were perinatal specific. Moreover, as pointed out by Santos et al. (2012), guidelines do not disclose recommendations on emerging clinical questions and on new available evidence.
For this review, we did not include Clinical Consensus Statements (CSSs) because they were not developed in accordance with CPGs. CSSs reflect the expert views of a panel of individuals who are well versed on the topic of interest while carefully examining and discussing the scientific data available. These consensus statements might give different recommendations than stated in the CPGs. For example, an Austrian CSS suggests tapering of antidepressants 2 weeks before the due date to reduce neonatal adaptation problems (Kasper et al., 2012). None of the CPGs mention this option, possibly because of available evidence suggesting reduction of exposure to selective serotonin reuptake inhibitors (SSRIs) at the end of pregnancy has no significant effect on improving neonatal health (Warburton et al., 2010). In clinical practice, CSSs and other guiding documents are frequently used instead of the formal guidelines and might contain a higher level of detail.
In summary, this overview of information might be helpful for the development of new CPGs. Clearly, there is a need for up-to-date and perinatal-specific CPGs and CSSs to help clinicians and patients in decision-making. It is challenging to develop these CPGs because evidence-based medicine, personalized medicine and legal liabilities need to be balanced.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.