
Abstract
Objectives:
Body dysmorphic disorder is commonly considered a contraindication for major cosmetic surgery, but whether body dysmorphic disorder relates to poorer outcomes from minor cosmetic treatment remains unknown. This study aimed to explore the prevalence of body dysmorphic disorder in clients seeking non-surgical cosmetic procedures and to examine whether body dysmorphic disorder clients are vulnerable in minor cosmetic settings. Vulnerability was explored in terms of psychological distress, unrealistic expectations and motivations for treatment outcome, and reduced satisfaction with past cosmetic procedures.
Method:
A cross-sectional online survey was completed by 154 women seeking minor cosmetic procedures which included the Body Dysmorphic Disorder Questionnaire – Dermatology Version to screen for body dysmorphic disorder, and measures of cosmetic treatment motivation, expectations and satisfaction.
Results:
Roughly 25% of women in the current sample screened positive for a potential body dysmorphic disorder diagnosis. Participants with suspected body dysmorphic disorder demonstrated higher levels of psychological distress and more unrealistic expectations and motivations for cosmetic treatment, such as improving social or romantic relationships. However, body dysmorphic disorder participants reported similar levels of satisfaction with past minor cosmetic treatments to the non–body dysmorphic disorder group.
Conclusion:
While the relationship between body dysmorphic disorder and treatment outcome warrants further investigation in prospective research tracking satisfaction and adverse reactions over time, this preliminary evidence suggests clients with suspected body dysmorphic disorder display several vulnerabilities in non-surgical cosmetic settings. Given the rapidly increasing accessibility of minor cosmetic procedures, further research is needed to determine their safety for clients with body dysmorphic disorder. Detection of body dysmorphic disorder in non-surgical cosmetic settings could facilitate earlier psychological intervention, promoting superior long-term outcomes.
Keywords
Introduction
While many individuals report improvements in body image and self-esteem following cosmetic procedures (Honigman et al., 2004; von Soest et al., 2011), it has long been recognised that individuals with body dysmorphic disorder (BDD), a psychiatric condition involving preoccupation with a minimal or non-existent flaw in physical appearance, do not usually improve following cosmetic surgery (Bowyer et al., 2016; von Soest et al., 2011). Instead, research has demonstrated that BDD symptoms may worsen following cosmetic treatment, with reports of increasing appearance preoccupation, concerns shifting to a different physical feature or increased hopelessness and suicidality if efforts to improve their body image are unsuccessful (Phillips et al., 2005; Picavet et al., 2013; Tignol et al., 2007). Despite these findings, approximately 76% of those with BDD undergo major or minor cosmetic procedures to correct perceived physical flaws (Crerand et al., 2010). In turn, BDD patients make up a disproportionate number of individuals seeking cosmetic treatment, with BDD prevalence in cosmetic populations between 5% and 25% (Bowyer et al., 2016; Veale et al., 2016), in contrast to a prevalence of 0.7–2.4% in the general population (Buhlmann et al., 2010). The high rates of cosmetic surgery seeking in BDD sufferers has often been explained by poor or absent insight, with around two-thirds of individuals with BDD holding a strong conviction that they look deformed or flawed (Phillips et al., 2012; Toh et al., 2017). As such, those with BDD may seek cosmetic surgery as the solution to a physical problem, rather than looking to evidence-based psychological treatments to address their body image dissatisfaction.
Previous research in cosmetic surgery settings has identified that BDD often co-occurs with other treatment contraindications. Clients with BDD are often younger, more anxious and depressed, and more preoccupied with their appearance than non-BDD counterparts in cosmetic settings (Dey et al., 2015). Furthermore, they tend to have more extensive histories of seeking cosmetic procedures, hold higher expectations, describe externally driven motivations for treatment (e.g. improving relationships or social life) and report lower satisfaction with the results of previous treatments (Brunton et al., 2014; Conrado et al., 2010; Honigman et al., 2004). As such, many have concluded that pre-treatment screening for BDD is necessary, and clients with suspected BDD should be referred for further psychosocial assessment (e.g. Bowyer et al., 2016; Brunton et al., 2014; Dufresne et al., 2001; Honigman et al., 2011). However, the majority of previous studies have been conducted in major cosmetic surgery or dermatology clinics that provide both surgical and non-surgical treatments, with significantly less evidence available regarding the characteristics of clients seeking minor cosmetic procedures alone (Bowyer et al., 2016; Brunton et al., 2014).
Minor cosmetic procedures do not involve cutting beneath the skin, but may involve piercing the skin (Medical Board of Australia, 2016). They include anti-wrinkle injections, dermal fillers, laser skin treatments and chemical peels, among others. Of 17.5 million cosmetic procedures performed in America in 2017, 91% were cosmetic injectables (International Society of Aesthetic Plastic Surgery, 2018). Similarly, Australians spent over $350 million on anti-wrinkle injections in 2017 (International Society of Aesthetic Plastic Surgery, 2018). Compared to major cosmetic surgeries, minimally invasive treatments are considered lower risk, are less expensive and are more accessible (in that they can often be attained on the day they are sought, without extensive consultation or cooling-off periods), making them an appealing choice for consumers (Walker et al., 2017). The growing popularity of minor cosmetic treatments suggests a simultaneous rise in individuals with BDD who may be seeking out these procedures. However, few studies have determined whether minor procedures are considered harmful for individuals with BDD and if pre-treatment screening should be recommended in settings that only provide non-surgical treatments.
While cosmetic surgeries are exclusively carried out by medical practitioners bound by strict ethical codes (Medical Board of Australia, 2016), minor procedures are delivered by a wide range of professionals including beauty therapists, dermal scientists and nurses, with regulations on who can provide these treatments differing between Australian states (Leow, 2017). Despite the lack of consistent regulation, non-surgical cosmetic clinics are a burgeoning market, with these clinics appearing within many shopping centres across Australia, increasing their reach. The primary staff members at these clinics are nurses or beauty therapists, with remote or occasional on-site consultation with medical physicians (e.g. Australian Skin Clinics, 2015). While this does not necessarily compromise the quality of care (Freedman and Earley, 2000; Leow, 2017), existing ethical guidelines, which emphasise the need to ensure the psychosocial suitability of cosmetic clients (Medical Board of Australia, 2016), do not apply to non-medical professionals delivering cosmetic treatment in Australia.
As such, the potential for harm may be higher for minor treatment, despite beliefs that these are low-risk procedures with short recovery periods. Thus, this study employed an online survey design to explore whether BDD should be considered a risk factor for minor cosmetic treatment, by examining the prevalence of BDD and its co-occurrence with other documented predictors of poor cosmetic treatment outcome. Participants were recruited from metropolitan clinics in Melbourne, Australia, who provide only non-surgical cosmetic procedures. To identify whether BDD should be considered a risk factor for minor cosmetic procedures, we explored (a) the prevalence of BDD within the sample using an adapted version of the Body Dysmorphic Disorder Questionnaire – Dermatology Version (BDDQ-DV), which is a brief screening measure that has been validated for use in cosmetic settings; (b) additional aspects of appearance dissatisfaction (i.e. the time spent per day thinking about appearance, areas of appearance concern and duration of concerns) to further characterise individuals who screen positive on the BDDQ-DV; (c) psychological distress to identify whether clients with suspected BDD may be more emotionally vulnerable and therefore susceptible to negative outcomes from cosmetic treatment; (d) motivations and expectations for treatment, to determine if BDD participants are more likely to hold motives that are considered unrealistic or externally driven; and finally (e) satisfaction with previous minor cosmetic treatments, to identify whether clients with suspected BDD tend to be more dissatisfied with the outcomes and process of non-surgical cosmetic procedures.
Material and methods
Design and measures
Ethical approval was obtained from the Swinburne University Human Research Ethics Committee, in accordance with the Declaration of Helsinki. The study involved a cross-sectional online survey of participants who had previously obtained or were considering a minor cosmetic procedure. Participants were recruited via email from a database of past and prospective clients at non-surgical cosmetic clinics in Melbourne, Australia. To confer eligibility, participants were required to be over 18 years of age and speak sufficient English. All data provided were anonymous and participants gave informed consent prior to beginning the survey which was administered on the Qualtrics platform and took approximately 15 minutes to complete. Participants provided demographic information, a history of previous cosmetic procedures undertaken, and completed the measures described below.
Presence of BDD
To assess whether BDD was present, a modified version of the BDDQ-DV (Dufresne et al., 2001) was used. The BDDQ-DV is a brief screening tool which includes a series of yes/no and free-response questions probing preoccupation with appearance, distress, interference with functioning and avoidance in relation to appearance. The BDDQ-DV is one of the most widely used BDD screening tools in cosmetic treatment studies (Higgins and Wysong, 2018; Picavet et al., 2011), demonstrating 100% sensitivity and 94.7% specificity in detecting BDD in cosmetic and dermatological settings (Dufresne et al., 2001). This study utilised a modified version of the BDDQ-DV which involved adapting yes/no questions from the original version to five scaling questions, rated on 5-point Likert-type scales (to address research questions not explored within the current paper). A similar adaptation of the BDDQ-DV has been used in previous work, reporting that the scale retains its reliability and validity when scored with Likert-type responses (Lekakis et al., 2016). Likewise, the adapted BDDQ-DV scale in this study demonstrated high internal consistency (α = 0.89). To facilitate comparison with previous work, the original BDDQ-DV scoring guidelines were followed. Thus, to screen positive for a potential diagnosis of BDD, participants were required to endorse preoccupation with appearance (scoring ⩾ 3 out of 5; at least moderate worry about appearance) and either distress or interference with work, social or role functioning due to appearance (scoring ⩾ 3 out of 5; indicating at least moderate interference; Dufresne et al., 2001; Lekakis et al., 2016). While the BDDQ-DV provides a useful preliminary screen for BDD, diagnosis should be supported by a clinical interview.
To further characterise individuals in the BDD group, participants were asked additional questions regarding the amount of time spent per day thinking about appearance, the duration of appearance concerns and the location and number of areas of appearance concern.
Psychological distress
Psychological distress was measured using the Depression Anxiety and Stress Scale – 21-item version (DASS-21; Lovibond and Lovibond, 1995) which yields subscale scores for anxiety, depression and stress over the past week. Scores on the DASS-21 are doubled, to facilitate interpretation in line with the original DASS scoring guidelines (Lovibond and Lovibond, 1995). Items are rated on a 4-point scale from 0 (never) to 3 (almost always) and summed, with higher scores indicating greater psychological distress.
Treatment motivation
Participants selected their motivations for cosmetic treatment from a checklist of 12 common motivations developed by the researchers in an unpublished pilot study. The list including motivations rated by the researchers as intrinsic (e.g. to feel more confident about myself) or extrinsic (e.g. relationship reasons such as finding a new partner), as previous research has identified that clients who report extrinsic motivations are more likely to be dissatisfied with cosmetic treatment outcomes (Maisel et al., 2018; Sobanko et al., 2015). Participants were also asked whether they were encouraged by another person directly (i.e. explicitly told or recommended) or indirectly (i.e. inferred from another person’s actions or behaviour towards them) to seek cosmetic treatment.
Treatment expectations
Treatment expectations were assessed using the Aesthetic Procedure Expectations Scale (ASPECT; Pikoos et al., 2020) which includes 19 items assessing unrealistic expectations for physical and psychosocial change following a cosmetic procedure. Questions relate to two subscales: intrinsic expectations (8 items; for example, ‘my confidence will improve’) and extrinsic expectations (11 items; for example, ‘romantic partners will be more attracted to me’). Each item is rated on a 4-point scale (strongly disagree to strongly agree). Scores are totalled, with higher scores indicating more unrealistic treatment expectations.
Cosmetic treatment satisfaction
If relevant, participants were asked about their satisfaction with their most recent minor cosmetic procedure. Satisfaction measures included three scales from the FACE-Q Aesthetics battery (Klassen et al., 2015) probing satisfaction with decision to seek treatment (5 items), satisfaction with outcome of treatment (5 items) and satisfaction with the informed consent process (8 items) each rated on a 5-point scale from very dissatisfied to very satisfied. Higher scores indicated greater satisfaction with treatment. Participants were also asked to rate their satisfaction with the visible change in their appearance following their most recent minor cosmetic procedure on a single item ranging from −5 (very negative change) to +5 (very positive change).
Statistical analysis
Data were analysed using SPSS IBM Statistical Package for Social Sciences (SPSS) v26. Participants were categorised into two groups reflecting ‘possible BDD’ or ‘unlikely BDD’ based on the BDDQ-DV scoring criteria (outlined in the ‘Material and methods’ section). To determine (a) BDD prevalence, the number of individuals in the suspected BDD group was calculated as a proportion of the overall sample.
A series of Mann–Whitney U analyses (continuous variables; due to non-normality in the data) and chi-square tests (categorical variables) were used to compare variables of interest and demographic factors between the suspected BDD group and non-BDD group. To address the research aims, groups were compared on (b) aspects of appearance dissatisfaction including the duration, location and number of appearance concerns; (c) psychological distress on DASS-21 scales; (d) treatment expectations; and (e) satisfaction with past cosmetic procedures. A Bonferroni correction was applied to account for multiple comparisons (p < 0.001).
To determine whether BDD participants displayed more extrinsic motivations for cosmetic treatment (in line with d), a binary logistic regression was performed with the 12 treatment motivations as predictors and BDD group as the outcome variable. Significant predictors were examined to determine whether they were classed as ‘intrinsic’ or ‘extrinsic’ motivators.
Results
The survey was accessed by 216 individuals and completed by 161 respondents with less than 10% missing data (74.5% completion rate; 154 women, 7 men). While the low proportion of men is largely reflective of a typical cosmetic sample (American Society of Plastic Surgeons, 2017), they were excluded from subsequent analyses due to insufficient power to conduct gender-based analyses. As such, participants included in the final sample were 154 women (mean age = 44.97 years, SD = 11.56 years).
Prevalence of BDD and sample characteristics
Of the 154 women included in analyses, 38 (24.7%) screened positive for suspected BDD. Non-BDD and possible BDD groups were subsequently compared on demographic variables and cosmetic treatment history, reflected in Table 1.
Group-based comparisons of demographic variables and cosmetic treatment history for individuals with and without suspected body dysmorphic disorder (BDD).
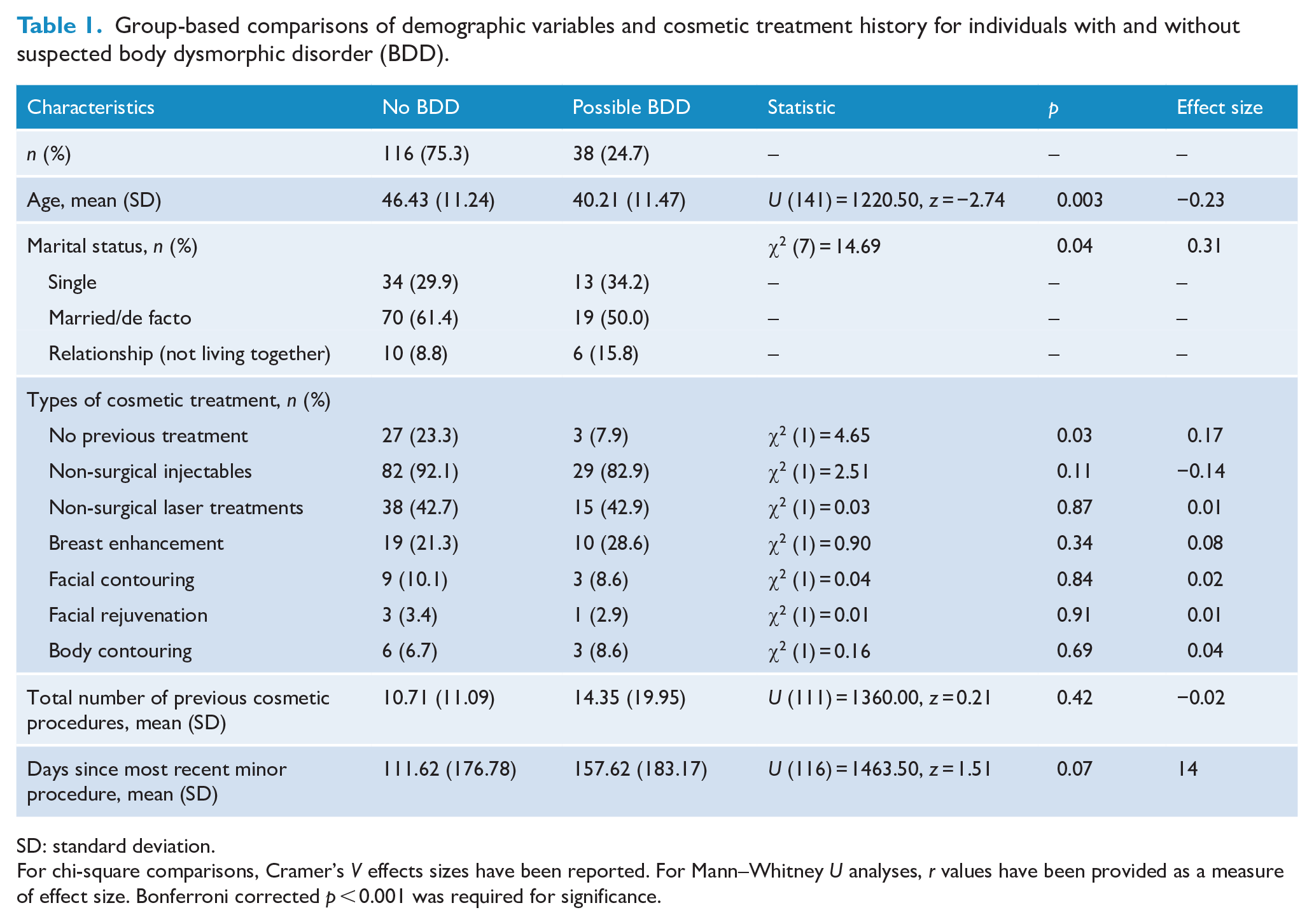
SD: standard deviation.
For chi-square comparisons, Cramer’s V effects sizes have been reported. For Mann–Whitney U analyses, r values have been provided as a measure of effect size. Bonferroni corrected p < 0.001 was required for significance.
There were no demographic differences between groups, nor did they differ on the number or types of previous cosmetic procedures undertaken. The most common procedures across both groups were non-surgical injectables, followed by non-surgical laser treatments. Major procedures were less common (52 participants; 29.1% of overall sample) and were led by breast augmentation surgery, followed by facial contouring, body contouring and facial rejuvenation surgeries.
Appearance dissatisfaction
Comparisons between the suspected BDD and non-BDD groups on appearance dissatisfaction variables (time thinking about appearance, number of appearance concerns and duration of appearance concerns) are presented in Table 2.
Group-based comparisons in appearance dissatisfaction and psychological distress between possible BDD and non-BDD group.
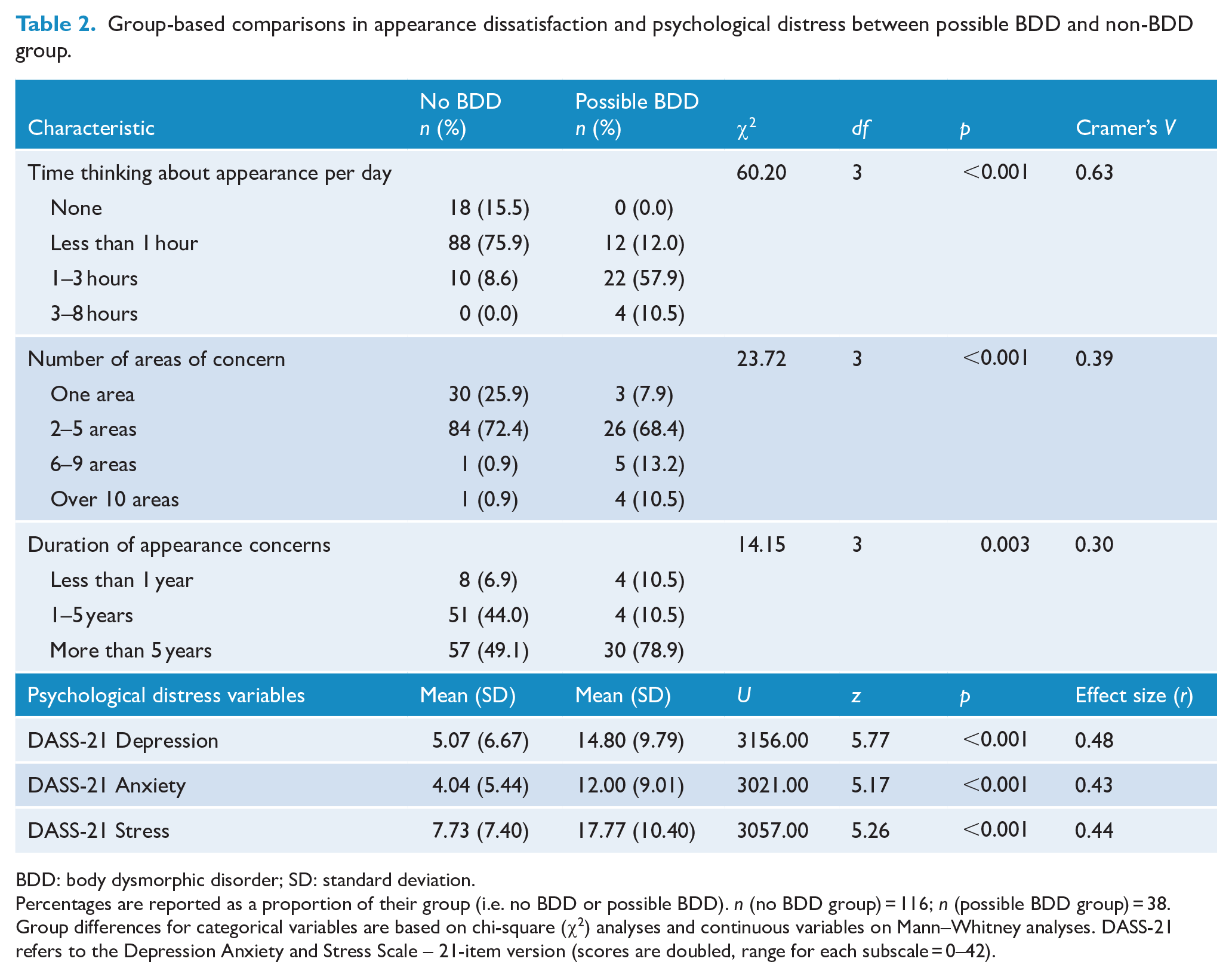
BDD: body dysmorphic disorder; SD: standard deviation.
Percentages are reported as a proportion of their group (i.e. no BDD or possible BDD). n (no BDD group) = 116; n (possible BDD group) = 38. Group differences for categorical variables are based on chi-square (χ2) analyses and continuous variables on Mann–Whitney analyses. DASS-21 refers to the Depression Anxiety and Stress Scale – 21-item version (scores are doubled, range for each subscale = 0–42).
The suspected BDD group spent significantly more time thinking about their appearance per day (i.e. only 9% of the non-BDD group reported thinking about their appearance for more than 1 hour per day, compared to 68% of the BDD group). Furthermore, BDD participants were more likely to report concern with multiple areas of appearance, rather than localised concern. The areas of concern reported by members of the BDD and non-BDD groups are presented in Figure 1. Unsurprisingly, most participants across both groups reported concern with their skin, given this is often the target of non-surgical cosmetic procedures. However, individuals in the BDD group were more likely to be concerned by their nose and weight or shape than non-BDD participants. Both groups reported similar levels of concern regarding other areas of appearance.
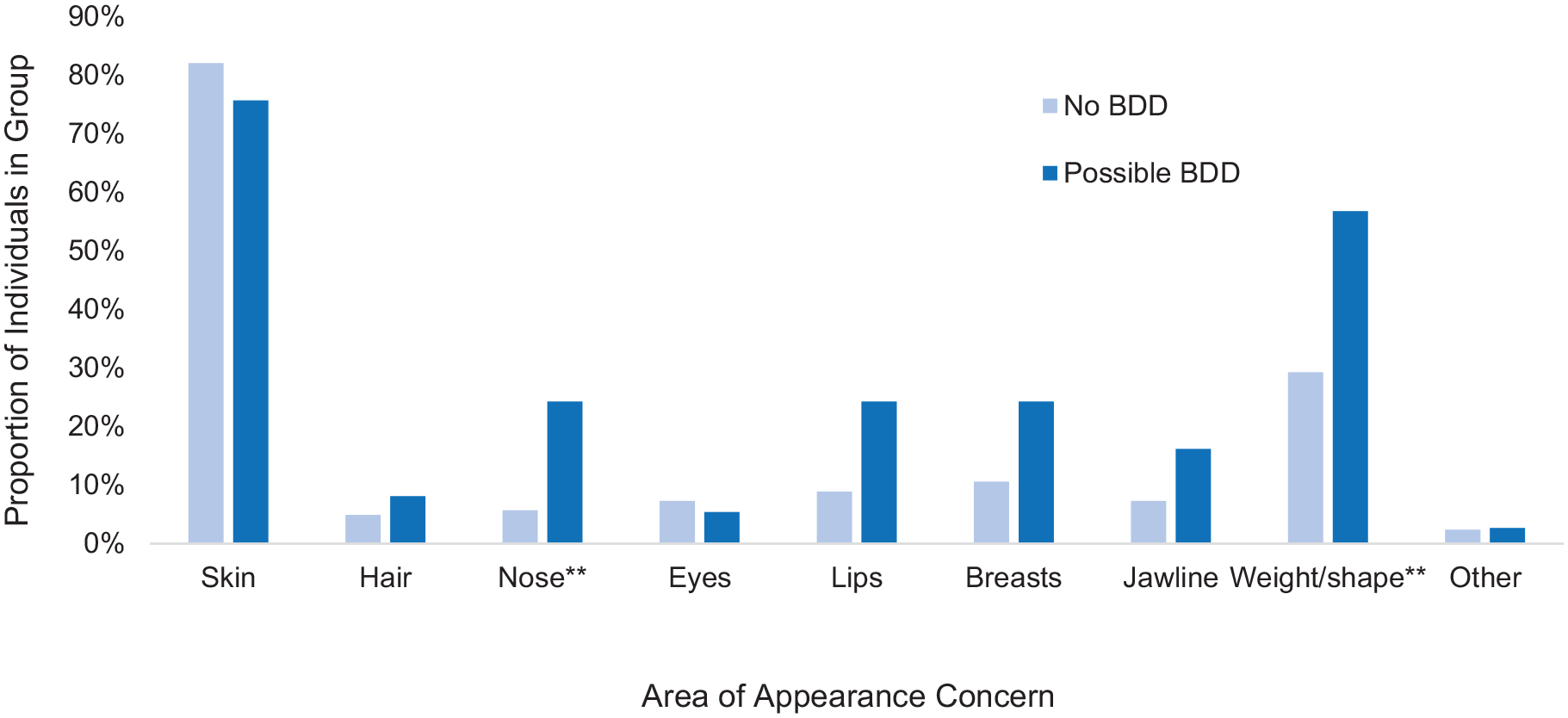
Differences in areas of appearance concerns between possible BDD and non-BDD participants.
Psychological distress
In terms of broader psychological distress, individuals with suspected BDD scored significantly higher than the non-BDD group across all DASS-21 depression, anxiety and stress subscales with medium effect sizes (Table 2).
Cosmetic treatment motivations and expectations
Figure 2 reflects the proportion of individuals in the BDD and non-BDD groups endorsing each treatment motivation. Binary logistic regression revealed that participants who wanted to correct an aspect of their appearance that they saw as problematic despite disagreement from family or friends, or for relationship reasons were more likely to have BDD (see Table 3). One individual with suspected BDD reported boosting their social media profile as a motivation for treatment; however, case numbers were too low to examine statistically. There were no other significant differences in motivations reported between groups.
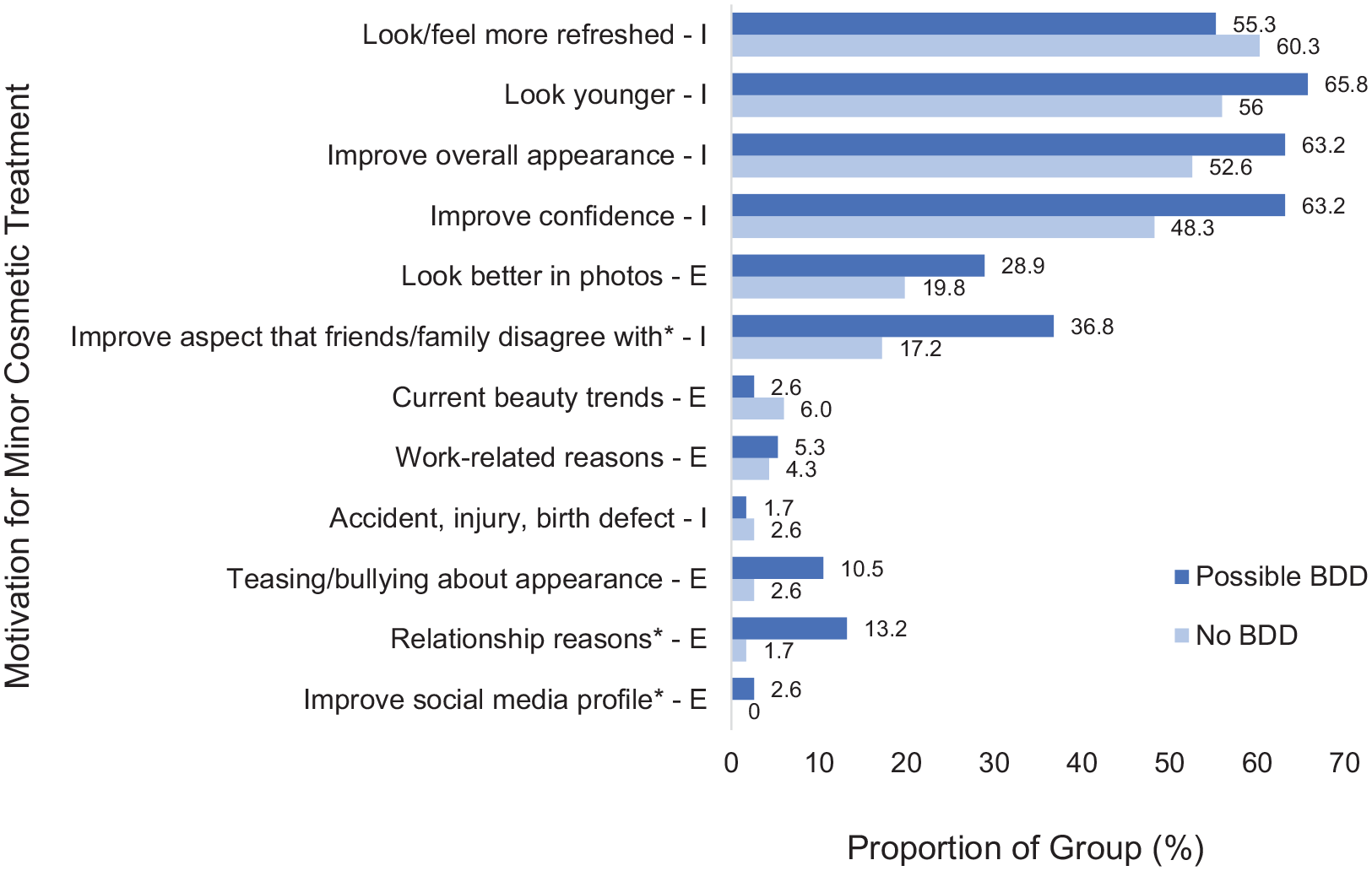
Motivations for seeking cosmetic treatment in participants with and without suspected BDD. Data labels represent the percentage of individuals within their group (n (possible BDD) = 38; n (non-BDD) = 116) who endorsed each motivation. Motivations which were rated as intrinsic by the researchers have been marked with an I; extrinsic motivations have been marked with an E. *Motivations which were significant predictors of BDD group in binary logistic regression analysis (p < 0.05).
Motivations predicting potential presence of BDD: results of binary logistic regression.
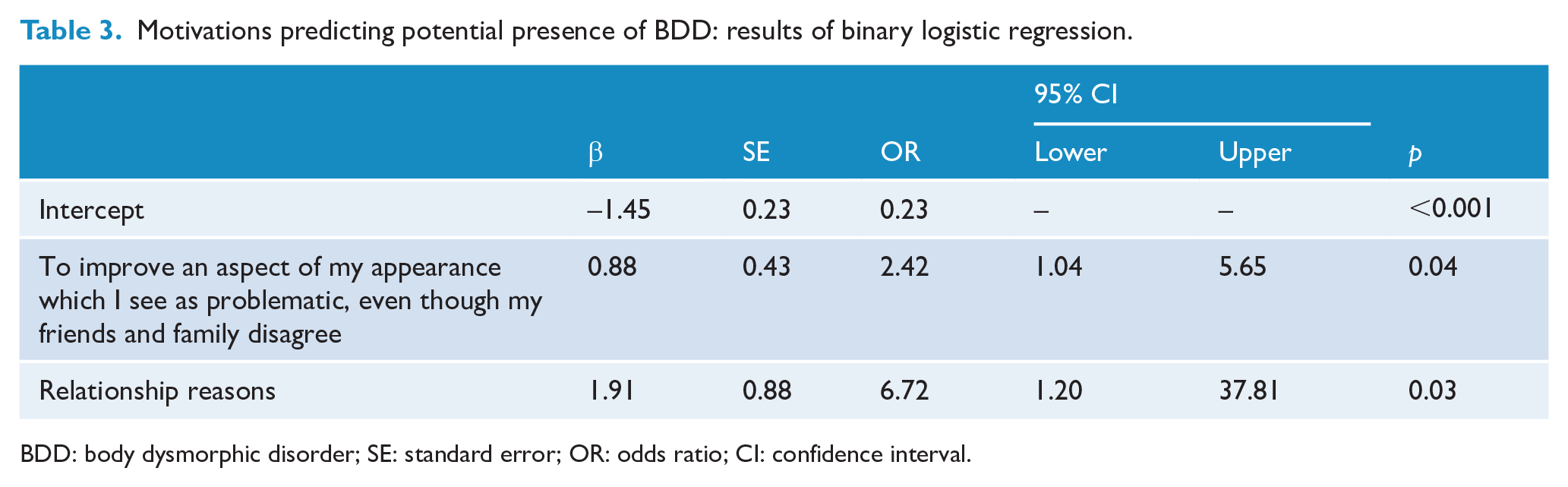
BDD: body dysmorphic disorder; SE: standard error; OR: odds ratio; CI: confidence interval.
To further examine if BDD participants were extrinsically motivated, participants were asked whether they were encouraged by someone else to seek cosmetic treatment. Of the non-BDD group, 6% reported being directly encouraged by another person to seek cosmetic treatment, compared to 29% of BDD participants, χ2 (1) = 14.38, p < 0.001, V = 0.31. Participants with suspected BDD were also significantly more likely to report being indirectly encouraged by another person to seek cosmetic treatment (18%) compared to the non-BDD group, 8%; χ2 (1) = 3.42, p = 0.03, V = 0.15.
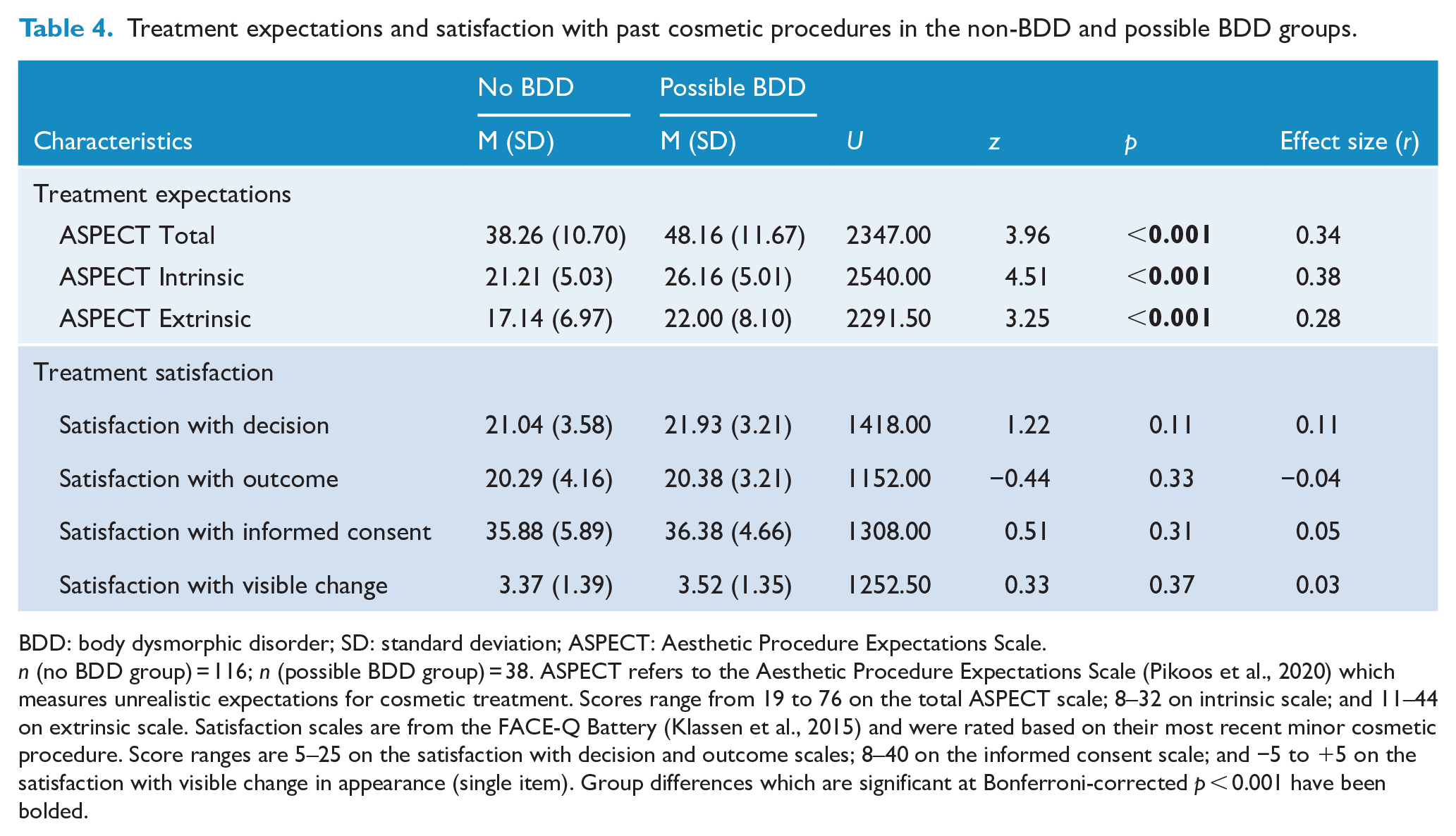
In terms of treatment expectations, ASPECT scores (total score, intrinsic and extrinsic expectations subscales) have been presented in Table 3 for the suspected BDD and non-BDD groups. Individuals with suspected BDD reported significantly higher and more unrealistic expectations for cosmetic treatment across all three ASPECT scales.
Cosmetic treatment satisfaction
All participants reported high mean levels of satisfaction with their decision to seek minor cosmetic treatment, the outcome of their most recent minor cosmetic procedure and the informed consent process (Table 4). Participants on average also considered the visible change in their appearance to be moderately positive following their most recent minor cosmetic procedure. There were no differences between suspected BDD and non-BDD groups on any of the satisfaction variables. To examine whether the lack of significant differences in satisfaction was due to varying time frames since the participants’ last cosmetic procedure, the satisfaction variables were correlated with the number of days since their most recent cosmetic treatment. There was no relationship between time since procedure and any of the satisfaction variables (Spearman’s correlations indicating p > 0.05).
Treatment expectations and satisfaction with past cosmetic procedures in the non-BDD and possible BDD groups.
BDD: body dysmorphic disorder; SD: standard deviation; ASPECT: Aesthetic Procedure Expectations Scale.
n (no BDD group) = 116; n (possible BDD group) = 38. ASPECT refers to the Aesthetic Procedure Expectations Scale (Pikoos et al., 2020) which measures unrealistic expectations for cosmetic treatment. Scores range from 19 to 76 on the total ASPECT scale; 8–32 on intrinsic scale; and 11–44 on extrinsic scale. Satisfaction scales are from the FACE-Q Battery (Klassen et al., 2015) and were rated based on their most recent minor cosmetic procedure. Score ranges are 5–25 on the satisfaction with decision and outcome scales; 8–40 on the informed consent scale; and −5 to +5 on the satisfaction with visible change in appearance (single item). Group differences which are significant at Bonferroni-corrected p < 0.001 have been bolded.
Discussion
Despite extensive research on the prevalence and characteristics of clients with BDD in major cosmetic surgeries, this is one of the first studies to report on BDD prevalence in a purely non-surgical cosmetic setting. This is important, given that psychological risks might be higher for non-surgical procedures due to widespread access and lack of regulation in comparison to major cosmetic interventions. Current results reveal that a quarter of female participants seeking non-surgical cosmetic treatments could meet criteria for BDD, a prevalence rate around 10 times higher than the general population (Buhlmann et al., 2010) and considerably higher than estimates in major cosmetic surgery settings (estimated at 13.2% according to a recent systematic review; Veale et al., 2016). The majority of participants who screened positive for BDD also reported thinking about their appearance in excess of an hour a day, concern with multiple areas of appearance (rather than one localised concern) and a longer duration of appearance concern, with most extending beyond 5 years. In contrast, most non-BDD participants spent less than an hour per day thinking about their appearance, were concerned with fewer areas and mostly for less than 5 years. Both BDD and non-BDD participants reported similar areas of appearance concern, except for concerns with their nose, weight or shape which were more common in BDD participants. This suggests that cosmetic practitioners may need to be more cognisant of potential BDD when clients request procedures focused on the nose or altering their weight or shape (e.g. body contouring); however, appearance concerns were not limited to these areas. Furthermore, as expected, participants screening positive for BDD were significantly more depressed, anxious and stressed than those without BDD. Thus, the current results support the notion that individuals who might present with BDD in non-surgical cosmetic clinics are often experiencing significant appearance-related and general distress and may therefore be more vulnerable than other clients.
The hypothesis regarding a tendency towards extrinsic cosmetic treatment motivations in BDD clients received mixed support. Overall, motivations did not differ greatly between possible BDD and non-BDD groups, with most participants seeking cosmetic treatment to boost their confidence, enhance overall appearance or to feel more refreshed (i.e. intrinsic motivations). However, participants with suspected BDD were more likely to report wanting a treatment despite disagreement from their peers, or for relationship-related reasons, indicating higher endorsement of extrinsic motives than the non-BDD group. Similarly, a higher proportion of suspected BDD participants reported feeling encouraged by someone else (either directly or indirectly) to seek cosmetic treatment, compared to non-BDD participants. This finding warrants further investigation to determine whether it reflects the relationships that BDD clients have (i.e. perhaps with a higher degree of criticism or appearance-based feedback) or if it indicates an interpretive bias, where individuals with BDD may perceive negative appearance-based feedback from neutral comments or facial expressions from others (Beilharz et al., 2017; Fang and Wilhelm, 2015). Regardless, feeling encouraged by others to seek treatment reflects an extrinsic motive which may predispose individuals to dissatisfaction with cosmetic treatment outcomes, given social relationships rarely change following a procedure (Honigman et al., 2004; Milothridis et al., 2016). Furthermore, participants in the BDD group reported higher and more unrealistic expectations for the outcome of their next cosmetic procedure across both intrinsic and extrinsic domains, supporting original predictions. Taken together, these findings suggest that even within minor cosmetic treatment settings, clients with BDD may be hoping for broader psychological and social changes beyond those that are realistically achievable from cosmetic procedures.
This study did not reveal any differences in treatment satisfaction between BDD and non-BDD groups. The BDD group were equally satisfied with their decision to seek minor cosmetic treatment, the outcome of treatment, the visible change in appearance and the informed consent process. This was contrary to expectations, given previous research has suggested that clients with BDD are less satisfied with cosmetic surgery outcomes (e.g. Crerand and Sarwer, 2010; Higgins and Wysong, 2018; Picavet et al., 2013). The current findings may indicate that BDD does not impact satisfaction with minor cosmetic procedures as significantly as major surgeries. This could relate to the perception that minor cosmetic treatments produce more subtle results, are generally cheaper than cosmetic surgery and have reduced physical risks (Clarke et al., 2007), creating less opportunity for dissatisfaction. Similarly, there have been preliminary accounts which suggest that the status of BDD as a contraindication for cosmetic treatment may vary with treatment type and the severity of BDD symptoms (Bowyer et al., 2016; Felix et al., 2014). This study may provide further weight to this argument, as suspected BDD participants reported high satisfaction ratings across multiple domains of the treatment experience, in contrast to the use of single-item measures in previous studies (Felix et al., 2014; Veale et al., 2014).
However, participants in this study were not asked whether body image, self-esteem or preoccupation with appearance changed following their last cosmetic treatment. While some previous studies revealed similar subjective satisfaction ratings between BDD and non-BDD groups, few have demonstrated reduction in BDD symptoms or recovery from diagnosis at follow-up (Bowyer et al., 2016). Improvement in BDD symptoms could be an important determinant of treatment success, given BDD patients often seek cosmetic remedies instead of evidence-based psychological support (Phillipou et al., 2016). As such, change in BDD symptoms should be explored in future studies to determine with greater confidence whether minor cosmetic treatments are beneficial or harmful for clients with BDD. Irrespective, cognitive-behavioural models of BDD posit that cosmetic treatment seeking (surgical or non-surgical) is a safety behaviour which may promote short-term relief from anxiety or appearance concern, but perpetuate an unhealthy or excessive focus on appearance (Veale, 2004; Wilhelm et al., 2013). Thus, even if clients with BDD self-report positive cosmetic results, they may experience negative psychological effects in the longer term.
In addition, emerging evidence has revealed the potentially addictive nature of minor cosmetic treatments, due to their activation of neurobiological reward pathways by boosting self-esteem and confidence (Shah et al., 2021), and their short-lived effects prompting the desire for further treatment. Individuals with BDD may be particularly susceptible to an addiction to cosmetic procedures, as they often display impulsivity, compulsivity and the presence of other addictive behaviours, such as substance or alcohol abuse (Grant et al., 2019; Shah et al., 2021). As such, subjective dissatisfaction with past procedures may not be a valid indicator of poor cosmetic treatment outcome, as clients may subjectively report treatment satisfaction despite the occurrence of other adverse effects. Furthermore, this study included a sample of clients actively seeking or considering minor cosmetic procedures (rather than a psychiatric sample of individuals with BDD), thus they may be more likely to hold positive beliefs about the benefits of cosmetic procedures (Honigman et al., 2004; Veale, 2000). These factors could contribute to the lack of significant differences in satisfaction between BDD and non-BDD participants in this study.
While the current findings provide preliminary evidence regarding the heightened vulnerability of non-surgical cosmetic clients who screen positive for BDD, there are some limitations worth noting. The high BDD prevalence in the sample may be elevated as a clinical interview was not used to confirm diagnosis. Previous research utilising the BDDQ-DV to screen for BDD without a clinical interview or defect rating scale has identified similar prevalence estimates to this study, ranging from 12.1% to 32% of their samples screening positive for BDD (Calderón et al., 2009; Hsu et al., 2009; Spataro et al., 2020). With the addition of a clinical interview and/or a defect rating scale to confirm minimal deformity, BDD prevalence estimates reduce to 2.9% to 15.2% in cosmetic dermatology settings (Veale et al., 2016). Thus, the use of the BDDQ-DV alone may have resulted in an inflated estimate of BDD prevalence. However, this reflects how screening is likely to work in a cosmetic setting where practitioners without mental health training may need to refer clients for psychosocial assessment to confirm a suspected diagnosis. Furthermore, the use of defect rating scales to confirm minimal deformity in BDD participants has been contested, given the poor inter-rater reliability observed between mental health and cosmetic practitioners (with the latter more likely to detect subtle aesthetic imperfections; Picavet et al., 2011; Sarwer, 2019). As many of the clients presenting for non-surgical cosmetic treatments may wish to enhance the appearance of normal facial features rather than correct deformities, defect rating scales may not display high specificity for BDD in cosmetic settings (Sarwer, 2019). As such, it has been proposed that the clearest indicators of BDD among cosmetic clients include the presence of significant preoccupation with appearance, substantial appearance-related distress and/or interference with functioning (Crerand et al., 2006), as measured in this study.
Furthermore, the current retrospective design may affect findings regarding treatment satisfaction, given participants rated psychological functioning at the time of the survey, while time since their last cosmetic treatment may have varied (however, time was not associated with any of the treatment satisfaction variables). As such, future studies could track participants prospectively from the time of assessment to post-treatment, measuring satisfaction and BDD symptomatology at specific time points to facilitate a more comprehensive analysis of treatment outcome. This study also focused purely on women seeking minor cosmetic procedures, due to the low number of male respondents. However, non-surgical procedures are increasingly popular among men (American Society of Plastic Surgeons, 2017), warranting greater focus on men in future studies. Finally, the present research provided preliminary evidence regarding BDD prevalence and associated features occurring in clients undertaking minor cosmetic treatments collectively, but future studies may consider whether these factors (e.g. underlying psychopathology, expectations, satisfaction) differ based on the type of minor cosmetic treatment undertaken. This may assist in developing a more nuanced decision-making process regarding BDD as a contraindication for minor treatment.
Conclusion
The current results revealed that the prevalence of suspected BDD in non-surgical cosmetic settings was significantly higher than estimates in the general public and major cosmetic surgery practices. Furthermore, participants screening positive on the BDDQ-DV were considerably more vulnerable, as they displayed high levels of depression, anxiety and stress, as well as a greater likelihood of reporting extrinsic motivations and unrealistic expectations for cosmetic treatment than the non-BDD group. Each of these are known risk factors for reduced cosmetic treatment outcome, suggesting that BDD is a possible contraindication for non-surgical procedures (Brunton et al., 2014; Conrado et al., 2010; Dey et al., 2015; Maisel et al., 2018). However, suspected BDD participants did not identify reduced satisfaction with minor treatment results when measured retrospectively, indicating the need for future prospective research to clarify whether BDD predicts poorer outcomes from non-surgical procedures. Nevertheless, individuals in the BDD group continued to report heightened and unrealistic expectations for future cosmetic treatments. This emphasises the need for cosmetic practitioners to implement thorough informed consent processes to manage unrealistic expectations for both physical and psychosocial changes following surgical and non-surgical procedures (Pikoos et al., 2020). While future research is needed to determine whether BDD relates to a broader array of treatment outcomes, this study suggests that non-surgical cosmetic practitioners should take caution with this vulnerable client group. The early detection of BDD within both minor and major cosmetic settings may prevent adverse cosmetic outcomes and prompt referral for psychological interventions for BDD patients. In turn, this may reduce the long delays that generally occur between the onset of BDD symptoms and accessing evidence-based treatment, promoting more positive outcomes for this vulnerable group.
Footnotes
Acknowledgements
The authors gratefully acknowledge the valuable contributions of the participants who dedicated their time to this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was sponsored by the Australian Government Research Training Program Stipend, the Cosmetic Professional Development Institute of Australia, Australian Postgraduate Research Intern and Professor Susan Rossell’s Senior National Health and Medical Research Council (NHMRC) Fellowship (GNT1154651). The contents of this article are the views of the authors and do not represent the opinions of the funding bodies.