
Abstract
Objectives:
(1) To collect, analyze and synthetize the evidence on muscle dysmorphia diagnosis as defined by Pope et al. and (2) To discuss its appropriate nosology and inclusion as a specific category in psychiatric classificatory systems.
Method:
A systematic search in the MEDLINE, the PsycNET, the LILACS and SciELO databases and in the International Journal of Eating Disorders was conducted looking for articles published between January 1997 and October 2014 and in EMBASE database between January 1997 and August 2013. Only epidemiological and analytical studies were considered for selection. The methodological quality of included studies was assessed according to the Evidence-Based Mental Health and the National Health and Medical Research Council’s guidelines. The support for inclusion of muscle dysmorphia in psychiatric classificatory systems was examined against Blashfield et al.’s criteria.
Results:
Thirty-four articles were considered eligible out of 5136. Most of the studies were cross-sectional and enrolled small, non-clinical samples. The methodological quality of all selected papers was graded at the lowest hierarchical level due to studies’ designs. Forty-one percent of the publications considered the available evidence insufficient to support the inclusion of muscle dysmorphia in any existing category of psychiatric disorders. The current literature does not fulfill Blashfield et al.’s criteria for the inclusion of muscle dysmorphia as a specific entity in psychiatric diagnostic manuals.
Conclusion:
The current evidence does not ensure the validity, clinical utility, nosological classification and inclusion of muscle dysmorphia as a new disorder in classificatory systems of mental disorders.
Muscle dysmorphia (MD) represents a mental and behavioral condition in which the individual perceives himself or herself as insufficiently large and muscular when, in general, the person possesses a bigger muscularity and leanness than average people. Also known as ‘bigorexia’ or ‘reverse anorexia nervosa’, both of them in reference to anorexia nervosa (AN) (Pope et al., 2005), some researchers (Grieve et al., 2009; Leone et al., 2005) and especially professionals of the physical education field observed that an increasing number of people seems to be affected by this syndrome, what they believe to characterize a silent ‘epidemic’. It is very likely that the number of cases is increasing even beyond cultural barriers since MD sufferers have been described in China (Ung et al., 2000), South Africa and Latin America (Behar and Molinari, 2010; Rutsztein et al., 2004; Soler et al., 2013). However, both the validity and clinical utility of this condition as well as its nosological status in the classification of mental disorders remain controversial.
The pathological preoccupation about not being big and strong enough was first described among male bodybuilders who were anabolic-androgenic steroids (AAS) users and was then regarded as a reverse form of AN (Pope et al., 1993). Five years later, Pope et al. (1997) stated that the newly observed syndrome seemed to be more properly related to the phenomenology of body dysmorphic disorder (BDD) than that of an eating disorder (ED) and presented the term ‘muscle dysmorphia’ to identify the condition, which was well-accepted by the clinical and scientific communities in general. In addition, a set of operational criteria to diagnose MD was proposed and remain fairly unchanged ever since (for details, see Pope et al., 1997).
In order to validate MD as a psychiatric nosological entity, a strong body of scientific evidence is required to avoid its reification or ‘pathologizing’ the typical routine of several athletes that, as is known, is characterized by a rigid commitment to a specific and restricted diet and long-hours dedicated to exercise. Such behaviors have the propensity for the individual to give up social activities for the purpose of achieving their athletic goals. On the other hand, the excessive preoccupation about not being strong and large enough in MD, and the characteristic associated behaviors, usually impair the functioning in many areas of life. Once recognized as a valid psychiatric condition, it is expected that further research will improve knowledge on the psychopathology, epidemiology, natural history, clinical course and treatment of MD. After 1997, a significant number of papers—including empirical studies—about this syndrome have been published, which reinforced its importance as a diagnostic category in the clinical and research literature. In addition, several measurement instruments have been developed in order to evaluate MD symptoms as proposed by Pope et al. (1997). The aforementioned scenario led the American Psychiatry Association (APA) to officially recognize MD as a valid disorder with clinical utility and to include it in the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5, APA, 2013) as a subtype of BDD. However, in the International Statistical Classification of Diseases and Related Health Problems—Tenth Revised Edition (ICD-10, World Health Organization, 1992)—it remains unreported.
We performed a systematic review on the construct ‘muscle dysmorphia’ as proposed by Pope et al. (1997) by collecting, analyzing and synthetizing the literature’s evidence that support its inclusion as a distinct diagnostic category. Additionally, we evaluated the psychopathological basis underpinning the recognition of MD as a BDD, as an ED, as an obsessive-compulsive disorder (OCD) or as another psychiatric category regarding its better fit in the nosological classification.
Methods
Database search
In order to identify all available articles about MD, we performed searches in MEDLINE, EMBASE, the Virtual Library in Health (‘Biblioteca Regional em Saúde’ in Portuguese which encompasses LILACS and SciELO databases) and PsycNET electronic databases and a manual search in the International Journal of Eating Disorders. Although an ‘MD-like’ syndrome was first described in 1993 (Pope et al., 1993), the recognition of the construct ‘muscle dysmorphia’ and operational criteria for it were proposed only in 1997 (Pope et al., 1997). Thus, we decided to search for articles published from January 1997 to October 2014 in the above databases, using the following key terms in all fields: MD, bigorexia, reverse anorexia, drive for muscularity, bodybuilding dependence and body image disorder. An exception was made regarding EMBASE where it was only possible to search for articles until August 2013. Finally, the references of all included papers were examined so that additional papers not identified by the searches could be analyzed and potentially selected.
Inclusion criteria
With the aim of collecting the best available evidence on MD, we included in this review only analytical and prevalence studies in which participants were diagnosed using the diagnostic criteria proposed by Pope et al. (1997) or at least a partial version of it. Only articles written in English, Spanish, French, Portuguese or Italian were selected.
Exclusion criteria
Theoretical papers, studies with a qualitative design, research that aimed at validating a particular questionnaire and those which enrolled MD participants identified by other criteria than Pope et al. (1997) or that did not specify the criteria used to diagnose MD were excluded.
Selection process
The titles and abstracts of articles identified by searches were evaluated by the first reviewer (C.A.S.F.), who excluded studies which failed to meet inclusion criteria for paper selection; thereafter, those which met criteria were read by the first reviewer and a co-reviewer (P.P.T.), and decisions for the inclusion or exclusion of the selected studies were made separately. In case of disagreement or doubt, a third and experienced investigator (S.C.S.) in systematic reviews was consulted and a decision based on consensus was made. None of the revisers were blind to the articles’ authors, institutions or journals.
During the analysis of selected articles, the principal reviewer contacted the first authors of the papers by email whenever necessary in order to clarify aspects regarding the study’s methodology or published results, and, above all, to clarify aspects related to the criteria used to identify the participants with MD.
Assessment of the methodological quality
The methodological evaluation of included articles was based on specific guidelines to each study design. Prevalence studies were expected to be assessed according to the Evidenced-Based Mental Health (EBMH)’s guidelines (Boyle, 1998) where: papers that fulfilled all criteria would be rated as ‘A’ (best evidence level), papers that fulfilled all but the response criterion rated as ‘B’ (regular evidence level) and ‘C’ (lower evidence level) for those in which another criterion besides the response one was not met. Analytical studies were classified along the levels of evidence and grades of recommendations (Stage 2 consultation) provided by the National Health and Mental Research Council (National Health and Medical Research Council [NHMRC], 2008): systematic reviews of level II studies displayed the best grade of evidence (grade I), while cross-sectional and case series studies were ranked within the lowest level of evidence (grade IV).
Evaluation of the evidence that support the inclusion of MD as a specific nosological entity
To examine the adequacy of the inclusion of the diagnostic construct ‘muscle dysmorphia’ in main psychiatric classificatory systems, papers selected were evaluated in accordance with guidelines suggested by Blashfield et al. (1990). In the last 10 years, these parameters have been widely used in several studies with the aim of examining diagnostic constructs (Nieuwoudt et al., 2012; Striegel-Moore and Franko, 2008; Stunkard et al., 2009). When applied to MD, Blashfield et al.’s criteria would need to meet the following:
The literature about MD should be consistent in that a minimum of 50 articles must have been published in the last 10 years, of which at least 25 should be empirical;
There must be a set of diagnostic criteria proposed in the literature defining MD combined with existing measurement procedures specific for this condition such as structured interviews, self-report instruments and rating scales;
The proposed nosological entity should present sufficient reliability properties; that is, there must be at least two empirical studies performed by independent research groups demonstrating adequate inter-clinician levels of agreement for MD, with K values ⩾ 0.70;
The set of the proposed diagnostic criteria must represent a group of symptoms which co-occurs frequently. Blashfield et al. (1990) suggest that to fulfill this aspect, there must exist a minimum of two empirical independent studies showing that in the presence of one of the diagnostic criteria for MD, the participant has a probability ⩾0.50 of fulfilling another criterion out of the proposed set of symptoms and,
In order to ensure that the construct ‘muscle dysmorphia’ is an independent disorder, the proposed syndrome must be properly distinguished from other pre-existing conditions with which it could be mistaken (e.g. BDD, AN, OCD) by at least two independent empirical studies.
A cursory glance at the published literature readily reveals that there are already a substantial number of empirical papers on MD, a reasonable acceptance of a set of diagnostic criteria and specific measurement procedures developed for investigating this syndrome. Since Blashfield et al.’s (1990) first and second criteria have already been met (Nieuwoudt et al., 2012), the aim of this review was to examine whether the existing literature gave support for the last three guidelines.
Results
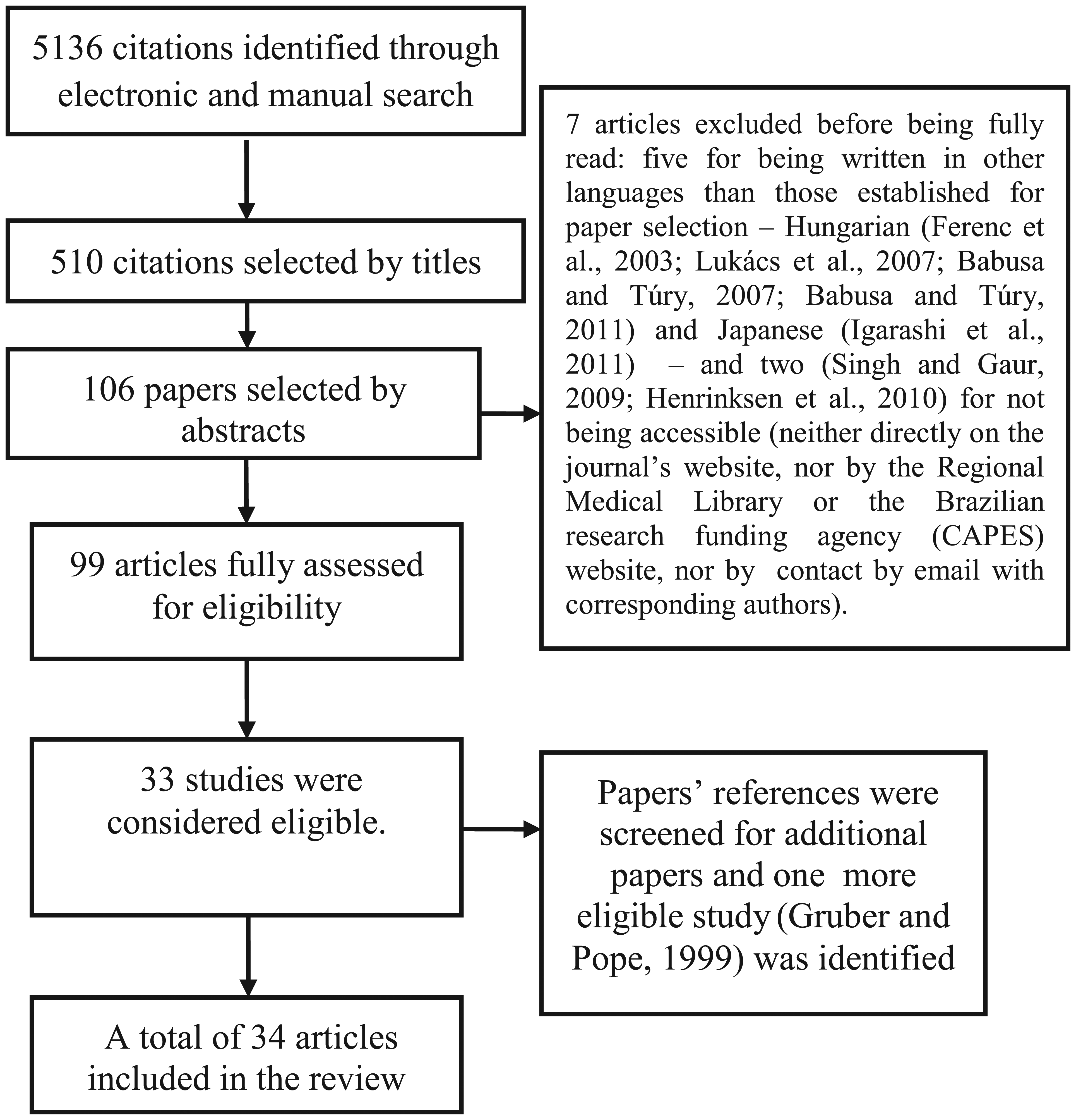
Article selection was performed as displayed in Figure 1, leading to a total of 34 articles included in this review (Table 1). Seven papers were excluded before being fully analyzed: five for being written in other languages than those established for paper selection – Hungarian (Ferenc et al., 2003; Lukács et al., 2007; Babusa and Túry, 2007; Babusa and Túry, 2011) and Japanese (Igarashi et al., 2011) – and two (Singh and Gaur, 2009; Henrinksen et al., 2010) for not being accessible (neither directly on the journal’s website, nor by the Regional Medical Library or the Brazilian research funding agency (CAPES) website, nor by contact by email with corresponding authors). One article (Gruber and Pope. 1999) was selected after included papers’ references were screened for additional eligible studies.
Systematic search.
Description of the included articles.
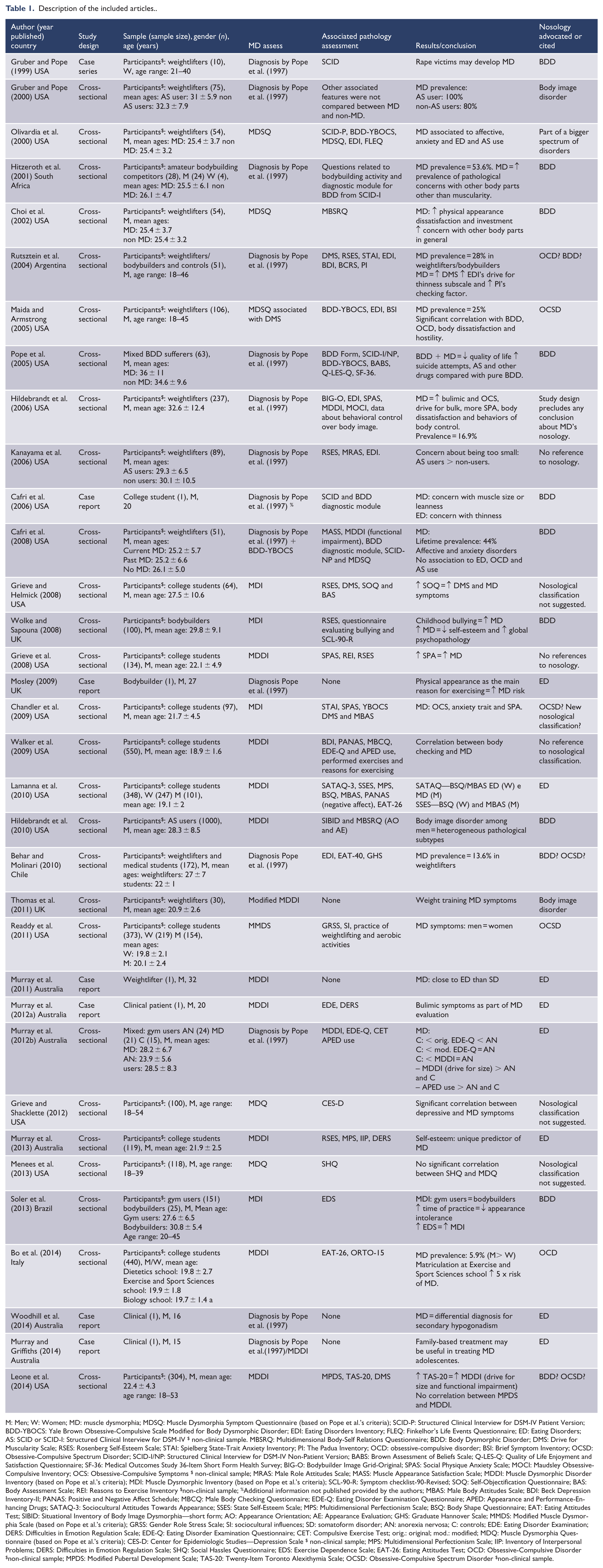
M: Men; W: Women; MD: muscle dysmorphia; MDSQ: Muscle Dysmorphia Symptom Questionnaire (based on Pope et al.’s criteria); SCID-P: Structured Clinical Interview for DSM-IV Patient Version; BDD-YBOCS: Yale Brown Obsessive-Compulsive Scale Modified for Body Dysmorphic Disorder; EDI: Eating Disorders Inventory; FLEQ: Finkelhor’s Life Events Questionnaire; ED: Eating Disorders; AS: SCID or SCID-I: Structured Clinical Interview for DSM-IV $ non-clinical sample. MBSRQ: Multidimensional Body-Self Relations Questionnaire; BDD: Body Dysmorphic Disorder; DMS: Drive for Muscularity Scale; RSES: Rosenberg Self-Esteem Scale; STAI: Spielberg State-Trait Anxiety Inventory; PI: The Padua Inventory; OCD: obsessive-compulsive disorder; BSI: Brief Symptom Inventory; OCSD: Obsessive-Compulsive Spectrum Disorder; SCID-I/NP: Structured Clinical Interview for DSM-IV Non-Patient Version; BABS: Brown Assessment of Beliefs Scale; Q-LES-Q: Quality of Life Enjoyment and Satisfaction Questionnaire; SF-36: Medical Outcomes Study 36-Item Short Form Health Survey; BIG-O: Bodybuilder Image Grid-Original; SPAS: Social Physique Anxiety Scale; MOCI: Maudsley Obsessive-Compulsive Inventory; OCS: Obsessive-Compulsive Symptoms $ non-clinical sample; MRAS: Male Role Attitudes Scale; MASS: Muscle Appearance Satisfaction Scale; MDDI: Muscle Dysmorphic Disorder Inventory (based on Pope et al.’s criteria); MDI: Muscle Dysmorphic Inventory (based on Pope et al.’s criteria); SCL-90-R: Symptom checklist-90-Revised; SOQ: Self-Objectification Questionnaire; BAS: Body Assessment Scale; REI: Reasons to Exercise Inventory $non-clinical sample; %Additional information not published provided by the authors; MBAS: Male Body Attitudes Scale; BDI: Beck Depression Inventory-II; PANAS: Positive and Negative Affect Schedule; MBCQ: Male Body Checking Questionnaire; EDE-Q: Eating Disorder Examination Questionnaire; APED: Appearance and Performance-Enhancing Drugs; SATAQ-3: Sociocultural Attitudes Towards Appearance; SSES: State Self-Esteem Scale; MPS: Multidimensional Perfectionism Scale; BSQ: Body Shape Questionnaire; EAT: Eating Attitudes Test; SIBID: Situational Inventory of Body Image Dysmorphia—short form; AO: Appearance Orientation; AE: Appearance Evaluation; GHS: Graduate Hannover Scale; MMDS: Modified Muscle Dysmorphia Scale (based on Pope et al.’s criteria); GRSS: Gender Role Stress Scale; SI: sociocultural influences; SD: somatoform disorder; AN: anorexia nervosa; C: controls; EDE: Eating Disorder Examination; DERS: Difficulties in Emotion Regulation Scale; EDE-Q: Eating Disorder Examination Questionnaire; CET: Compulsive Exercise Test; orig.: original; mod.: modified; MDQ: Muscle Dysmorphia Questionnaire (based on Pope et al.’s criteria); CES-D: Center for Epidemiologic Studies—Depression Scale $ non-clinical sample; MPS: Multidimensional Perfectionism Scale; IIP: Inventory of Interpersonal Problems; DERS: Difficulties in Emotion Regulation Scale; SHQ: Social Hassles Questionnaire; EDS: Exercise Dependence Scale; EAT-26: Eating Attitudes Test; OCD: Obsessive-Compulsive Disorder $non-clinical sample; MPDS: Modified Pubertal Development Scale; TAS-20: Twenty-Item Toronto Alexithymia Scale; OCSD: Obsessive-Compulsive Spectrum Disorder $non-clinical sample.
Excluded articles
Sixty-six articles were excluded following analysis. The main reason for exclusions was the fact that the analysis of the construct ‘muscle dysmorphia’ as defined by Pope et al. (1997) was not an objective of the investigation nor was discussed in the paper (n = 64). Yet, other papers were rejected for different reasons such as severe methodological shortcomings or being a theoretical paper.
Description of the included articles
Characteristics of the samples
More than half of the studies (20 papers) were conducted in the United States, six in Australia, three in the United Kingdom, one in Argentina, one in Brazil, one in Chile, one in Italy and another in South Africa. Most studies enrolled non-clinical participants (85% of the total), the majority being weightlifters, bodybuilders and male college students; in addition, one of the samples consisted of steroid male users (Hildebrandt et al., 2010). Two articles (6%) comprised mixed samples (clinical and community participants) and three studies (9%) reported a clinical case. Only six papers included female individuals (Bo et al., 2014; Gruber and Pope, 1999, 2000; Hitzeroth et al., 2001; Lamanna et al., 2010; Readdy et al., 2011). The sample size in the studies ranged from one to 1000 individuals, even though not all participants could be diagnosed as sufferers of MD symptoms. However, most of the samples (n = 19) enrolled less than 100 participants.
MD prevalence
Among male weightlifters, the lifetime prevalence of the disorder identified through this review ranged from 13.6% to 44% (Behar and Molinari, 2010; Cafri et al., 2008; Hildebrandt et al., 2006; Maida and Armstrong, 2005; Rutsztein et al., 2004). In addition, the prevalence rates of MD for female weightlifters were 100% among steroid users and 80% among non-users (Gruber and Pope, 2000), 53.6% in a mixed-gender sample of South African amateur bodybuilding competitors (Hitzeroth et al., 2001) and between 22.2% and 28.6% among men with BDD in a retrospective chart review study where two independent reviewers examined the data (Pope et al., 2005). In a mixed-gender group of college students, MD was identified among 5.9% of them, mostly in men (Bo et al., 2014).
Designs and methodological quality
The designs of the selected studies were as follow: 27 cross-sectional articles (79% of the total), six case reports (18% of the total) and one case series (3% of the total). No epidemiological study was found, so the quality of the evidence was assessed only based on the NHMRC guidelines. Consistent with the latter, the data reported by all 34 publications were graded at the lowest level of quality, which is level IV (cross-sectional and case series designs).
Blashfield et al. (1990) guidelines
As to the adequacy of MD’s inclusion in the psychiatric classificatory manuals, this review identified only one article (Pope et al., 2005) related to the third criterion, no study satisfying the fourth guideline and two papers (Murray et al., 2012b; Olivardia et al., 2000) apropos the last one.
The nosological classification of MD
Regarding the nosology of the construct ‘muscle dysmorphia’ as defined by Pope et al. (1997), it is evident in Table 1 that nine out of the 34 selected articles (26% of the total) postulated it as a subtype of BDD, while eight of them (24%) as a variant of ED and three (9%) as part of the obsessive-compulsive spectrum of disorders (OCSD). Notwithstanding, the majority of them (14 articles, representing 41% of the total) did not consider that the available evidence was sufficient to state the inclusion of MD in any of the existing psychiatric nosological categories.
Discussion
This systematic review investigated the validity and clinical utility of the diagnosis MD as proposed by Pope et al. (1997) and found that sufficient evidence was not available to support it as a specific entity in psychiatric classificatory systems where Blashfield et al. (1990) guidelines are applied. In addition, only 26% of the selected articles acknowledged MD as a subtype of BDD, as currently classified in DSM-5, and the majority of studies either did not discuss the nosological status of MD or considered the evidence thus far too weak to include it under any of the existing psychiatric categories.
This review identified that the empirical literature on MD as defined by Pope et al. (1997) concentrated primarily on American studies of small samples comprising male weightlifters and bodybuilders. This has the real possibility of providing somewhat skewed data set pertaining to this construct. Women were noticeably absent in these studies investing MD but as Pope et al. (1997) argue, the reason for this is that mostly affects men. Nevertheless, community data on MD based on epidemiological studies are lacking (Murray et al., 2010) and the proposed criteria may be gender-biased (as also argued for ED), precluding conclusive information relative to gender distribution of this syndrome. In addition, a new body ideal for women is emerging and taking place against the thin ideal: it is characterized by a muscle-toned lean build, although not with a bulky musculature (Gruber, 2007). This emphasis on modest muscularity in the female body may contribute to an increase in MD symptoms among women, stressing the importance of investigating this phenomenon in female samples also. This is supported by Readdy et al. (2011) who identified similar levels of MD symptoms between male and female college students.
The prevalence rates of MD found in our review were somewhat divergent. For example, the lifetime presence of the disorder among male weightlifters ranged from 13.6% to 44% (Behar and Molinari, 2010; Cafri et al., 2008; Hildebrandt et al., 2006; Maida and Armstrong, 2005; Rutsztein et al., 2004). The discrepancy between those prevalence rates may be due to several factors such as the size (small) and type (convenience) of samples. Nevertheless, it is worth noting that most of the MD cases were diagnosed through clinical judgment. Hence, the difference found in prevalence rates may reflect the unreliable way clinicians and researchers are diagnosing MD and the need for a valid set of criteria and reliable measures for identifying this condition among samples comprising different groups (weightlifters, bodybuilders, BDD sufferers, college students, etc.). It is also worth reminding that people who suffer from MD often lack adequate insight on the pathological nature of their preoccupation and related behaviors. Hence, these individuals do not consider themselves as suffering from a mental disorder (Olivardia, 2001), the reason why the reported frequencies may be underestimated (Kanayama and Pope, 2011).
With respect to the application of Blashfield et al. (1990) criteria, only one article fulfilled the third criterion by analyzing the inter-clinician levels of agreement for identifying MD (Pope et al., 2005). In this study, the diagnosis of this syndrome among men with lifetime BDD exhibited an agreement rate of 93.6% between two independent blind investigators, showing adequate reliability coefficient (K = 0.83). As for the fourth criterion, no study in this review investigated the co-occurrence of MD symptoms. Since Blashfield et al. (1990) recommend that there should be at least two independent and empirical studies assessing the aspects of the third and fourth criteria, these two criteria were not met in this review.
However, with regards to the fifth guideline, two independent and empirical papers (Murray et al., 2012b; Olivardia et al., 2000) did try to distinguish men with MD and ED in relation to several variables such as eating and body image pathology, misuse of AAS and lifetime history of anxiety and mood disorders. Olivardia et al. (2000) compared—in a posteriori analysis—male weightlifters with MD and ED college men and found similarities between the two groups in lifetime history of mood and anxiety disorders, body dissatisfaction and Eating Disorder Inventory (EDI) scores. However, the data that supported these findings were not available in the publication. Murray et al. (2012b) compared male patients with MD (n = 21) to males with AN (n = 24) and male controls (n = 15 gym users) with respect to eating symptomatology, body image features, compulsive exercise practice and appearance and performance-enhancing substance use. The authors concluded that, overall, there were more similarities than differences between MD and ED participants, and suggested that MD is a valid nosological entity associated to ED. No other empirical study comparing ‘pure’ MD participants with individuals suffering from BDD, OCD or another psychiatric syndrome was found. Thus, the data of this review cannot support the fulfillment of the Blashfield et al.’s (1990) fifth criterion as existing publications do not provide robust evidence (based on at least 2 empirical studies) of well-established differences between MD and other psychiatric categories. Finally, our conclusions concur with those from Nieuwoudt et al.’s (2012) review, in which Blashfield et al.’s (1990) criteria were also applied to the literature on MD, but different criteria for paper selection, different databases and search terms, as well as a shorter length of time (2001–2011) for identifying publications was used compared with this research. In addition, the present review updates the evidence to 2014.
The inclusion of MD as a subtype of BDD in DSM-5 suggests that its nosological nature has been already defined (APA, 2013). One of the reasons underpinning the classification of MD under BDD category is associated with the fact that the preoccupation with the perceived insufficient muscularity can be understood as part of the vast unobservable or slight flaws in appearance which BDD sufferers are obsessed with. In addition, MD is not gender-exclusive and affects women as well, like BDD (Pope et al., 1997). Moreover, BDD proved to be a stronger predictor of MD symptomatology than OCD or ED symptoms (Maida and Armstrong, 2005).
Some authors (Grieve, 2007; Lamanna et al., 2010; Mosley, 2009; Murray et al., 2010, 2011, 2012a, 2012b; Murray and Griffiths, 2014; Woodhill et al., 2014) claim that MD would be better understood as an ED since both conditions represent specific pathologies related to body image disturbances, abnormal diet and excessive exercise. Such phenomenologies which are widely influenced by sociocultural expected body ideals—thin build for women, bulky build for men—justifying the gender discrepancy between the prevalence rates of both disorders. Also, the inclusion of MD under the ED spectrum could represent the specific male experiences with body image and associated eating pathology (Greenberg and Schoen, 2008). One of the arguments against this point of view is that the eating symptomatology (like excessive attention to diet) seems to be a secondary, less important aspect in MD than the long hours dedicated to weightlifting (Olivardia, 2001). As an example, men with this condition score lower in eating pathology measures in comparison with men with AN (Murray et al., 2012b). Nevertheless, the available ED measurement procedures have their psychometric properties primarily validated in female samples and encompasses items directed to the female experiences, being thus less sensitive among male participants. Moreover, Chung (2001) highlights that it was only recently that behaviors common to AN were conceived as a consequence of a body image misperception, as other motives for food refusal and AN-like syndromes have been reported over time and across cultures (Al-Adawi et al., 2013). Therefore, the reported similarities between ED and MD etiologies should be considered with caution. The author also underlines that the eating and exercise-related symptoms shared between MD and ED are obsessive-compulsive in nature and that the preoccupation regarding one’s own muscularity in MD is not pathological in itself, but the behaviors stemmed from this kind of concern are, as in OCD. Therefore, Chung (2001) argues for the inclusion of MD as part of the OCSD.
So far, it seems that the appropriate nosology of MD remains open to debate. In fact, the current review demonstrated that the majority of authors described the condition as a body image disorder—an unspecified category that covers symptoms regarding diverse psychiatric conditions or depicted it as part of a bigger group of disorders (Gruber and Pope, 2000; Maida and Armstrong, 2005; Olivardia et al., 2000; Readdy et al., 2011; Thomas et al., 2011)—which may include BDD, OCD and ED; others preferred not to state any firm conclusion about the best nosology for MD (Behar and Molinari, 2010; Chandler et al., 2009; Grieve et al., 2008; Grieve and Helmick, 2008; Grieve and Shacklette, 2012; Hildebrandt et al., 2006; Kanayama et al., 2006; Menees et al., 2013; Rutsztein et al., 2004; Walker et al., 2009). The observed uncertainty around MD’s nosological classification may stem from the insufficient body of good or fair evidence about the construct’s validity and clinical utility found in the literature. In addition, little is known about the etiology of MD, especially concerning neurobiological or genetic factors involved. In one study, Grieve et al., (2009) identified potential risk factors for MD as follows: body dissatisfaction, body distortion, ideal body internalization, low self-esteem, participation in sports, perfectionism and negative affect. Therefore, it seems premature to define MD as a specific category within a major class of psychiatric disorders at the current stage of knowledge.
However, MD has been categorized as a subtype of BDD which, in turn, is classified under the category of obsessive-compulsive and related disorders in DSM-5. A more conservative approach to the nosological status of MD would be to include it among disorders in need of further research aiming at improving its validity, akin to the process that the category of binge eating disorder has evolved through. Another suggestion would be to include MD, ED and BDD in a body image disorder category, designed to encompass all conditions characterized by body image disturbances and by the behaviors and mental acts arising out of those concerns and misperceptions.
The current review has some limitations. By restricting our research to articles about MD as defined by Pope et al. (1997), we tried to provide more specific information regarding this construct, considering its general acceptance among researchers and clinicians. Nevertheless, it was not always possible to ascertain that some of the measures used have been based mostly or exclusively on Pope et al.’s (1997) proposed criteria. In addition, Lantz et al. (2001) formulated a psycho-behavioral model to characterize MD, but the application of this model in research was not examined here (papers were excluded) as we were unable to determine how similar it was to Pope et al.’s (1997) criteria. Another shortcoming of this review is that it did not cover electronic databases specific to sports medicine and psychology, and the search carried out in the EMBASE was limited to August 2013, potentially impacting the identification of additional papers. However, this review updates Nieuwoudt et al.’s (2012) work, and broadened the search by enrolling not only North American, but also European and Latin American databases.
In conclusion, despite the considerable number of empirical articles on MD available in the scientific literature as recommended by Blashfield et al.’s (1990) first criterion, the existing data are yet insufficient to cement it as a valid construct. In that sense, research on neurobiology and genetics of MD are crucial in face of the lack of information relative to its etiology. In addition, studies that better delineate at-risk groups for MD, as well as large, prospective studies enrolling more diverse populations (e.g. females, non-weightlifters or athletes) are necessary to enhance the current status of knowledge about the epidemiology and risk factors relative to the syndrome. Developing an understanding of the potential risk factors is absolutely crucial for the successful implementation of interventions (Striegel-Moore and Bulik, 2007) and enabling the identification of such high risk groups for more targeted strategies. Also, there is an urgent need to identify the subgroup of males most at risk for muscularity and thinness-oriented body image disorders. Such recognition would better inform the development of early intervention and prevention programs that are specifically aimed at males (Murray and Touyz, 2012) as it is well known that males are much less likely to seek treatment than their female counterparts (Weltzin et al., 2005). The adoption of such early intervention strategies may have the desired outcome of enabling males to better cope with body-related issues especially those of clinical severity. Such an avenue of research is particularly pertinent with the emerging evidence that eating disorders are on the rise, particularly among younger males (Madden et al., 2009). Because of these factors, there is now a compelling need to develop a better understanding ‘of the complex nature of the divergence of body image psychopathology among males’ (Murray and Touyz, 2012). Such insights may inform the development of more innovative strategies that could be better targeted to the patient’s specific needs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ST has received an honorarium from Shire Pharmaceuticals. AC is chair of the Feeding and Eating Disorders Workgroup for the Mental and Behavioral Disorders Chapter of the World Health Organization (WHO) International Classification of Diseases and Related Health Problems, 11th edition (ICD-11), but the statements here do not represent this Workgroup or WHO positions. The remaining authors declare that they have no conflict of interest in the research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.