
Abstract
Objective:
Body dysmorphic disorder typically begins in adolescence, yet little is known about the prevalence and correlates of the disorder in this age group. The current study aimed to explore the presenting features of adolescents meeting probable criteria for body dysmorphic disorder in a large community sample, and compare levels of comorbid psychopathology, quality of life and mental health service use between adolescents with probable body dysmorphic disorder and those without.
Method:
Questionnaires were completed at school by 3149 adolescents: 63% male, aged 12–18 years (M = 14.58). These assessed Diagnostic and Statistical Manual of Mental Disorders (4th ed.) body dysmorphic disorder criteria, past mental health service use and symptoms of body dysmorphic disorder, anxiety, depression, obsessive-compulsive disorder and eating disorders. In male participants, additional measures assessed quality of life, muscularity concerns, emotional symptoms, peer problems, conduct problems and hyperactivity.
Results:
The prevalence of probable body dysmorphic disorder was 1.7%; there was no sex difference in prevalence, but older adolescents reported higher prevalence than younger adolescents. Probable body dysmorphic disorder participants reported substantially elevated levels of psychopathology, quality of life impairment and mental health service use compared to non-body dysmorphic disorder participants.
Conclusions:
The prevalence of body dysmorphic disorder in adolescents is similar to adult samples, and probable body dysmorphic disorder is associated with comorbidity, distress and functional impairment in a community sample. Further research is required to better understand the presentation of body dysmorphic disorder in adolescents, and to improve diagnosis and treatment.
Introduction
Body dysmorphic disorder (BDD) involves the preoccupation with perceived flaws or defects in appearance that are not observable or appear minimal to others (American Psychiatric Association [APA], 2013). Few studies have examined BDD in adolescents, despite the fact that mean BDD onset is 16 years (Bjornsson et al., 2013). The clinical presentation of BDD is relatively similar between adults and young people regarding BDD severity, levels of comorbidity and extent of impairment (Albertini and Phillips, 1999; Mataix-Cols et al., 2015; Phillips et al., 2006a). However, adolescents may experience poorer insight and greater suicidality than adults (Phillips et al., 2006a), and adults with BDD onset prior to the age of 18 report higher rates of suicidality and comorbidity than those with adult-onset BDD (Bjornsson et al., 2013). BDD appears to disrupt normal adolescent development by impairing social functioning, initiation of romantic relationships, educational and vocational attainment (Phillips, 2005). As BDD tends to follow a chronic course (Phillips et al., 2013), these difficulties are likely to persist into adult life.
Despite the potential severity of BDD in adolescence, only two studies have explored its prevalence. Mayville et al. (1999) found 2.2% BDD prevalence in 566 US high school students aged 14–19 years. Rief et al. (2006) reported BDD prevalence of 2.3% in 174 Germans aged 14–20 years. Although replication in larger samples is required to increase confidence in these estimates, they are consistent with the adult BDD prevalence of 1.7–3.2% reported across the United States, Germany and Sweden (Brohede et al., 2015; Buhlmann et al., 2010; Koran et al., 2008; Rief et al., 2006; Schieber et al., 2015). Several studies have found a trend towards higher BDD prevalence in females compared to males, but these differences are typically not statistically significant (Buhlmann et al., 2010; Koran et al., 2008; Mayville et al., 1999; Rief et al., 2006), with the exception of Schieber et al. (2015).
Little is known about the correlates of adolescent BDD in community samples. This is potentially problematic, as individuals with BDD often do not access appropriate mental health services (Marques et al., 2011), and BDD is typically not detected in routine clinical settings (Grant et al., 2001; Veale et al., 2015). Caution may therefore be needed when generalising findings from treatment-seeking samples to cases of BDD in the community. One recent study (Mastro et al., 2016) evaluated appearance anxiety, indicative of BDD, in 387 community participants aged 10–13 years. Those at high risk of BDD experienced elevated symptoms of depression and social anxiety, more extreme weight management behaviours, greater rejection sensitivity and poorer social functioning and social competence than those at low risk for BDD. However, it is unclear to what extent the measure used by Mastro et al. (2016) differentiates between BDD and eating disorder symptomatology. This preliminary evidence suggests that BDD symptoms are associated with a range of negative outcomes in adolescents in the community, but further research is clearly needed.
In sum, the available evidence indicates that BDD may have similar prevalence in adolescents and adults, and is associated with considerable distress and impairment in young people. However, knowledge about the presentation and correlates of adolescent BDD is largely restricted to clinical samples. The current study aimed to identify probable cases of BDD (hereafter referred to as pBDD) in a large sample of Australian high school students. We aimed to explore the presenting features of pBDD, including demographic correlates, BDD symptoms endorsed and the body areas of concern. Given that BDD typically begins at 16 years, we hypothesised that the prevalence of pBDD would be higher among participants aged 15–18 years compared to those aged 12–14 years. We also hypothesised that there would be no significant sex difference in pBDD prevalence. Based on patterns of comorbidity found in clinical samples of adolescents with BDD, it was hypothesised that symptoms of anxiety, depression, obsessive-compulsive disorder and eating disorders would be elevated among adolescents with pBDD compared to those without pBDD (referred to as non-BDD). Finally, it was hypothesised that levels of quality of life impairment, muscularity concerns, emotional symptoms, peer problems, conduct problems and hyperactivity – measures that were completed only by male participants – would be higher among males with pBDD when compared with non-BDD males. While past use of mental health services was also assessed, the available evidence did not permit any a priori hypotheses concerning between-group differences in this outcome.
Method
Participants
Participants were recruited from seven high schools in New South Wales, Australia, as part of two separate longitudinal studies of the development of emotional health. The first study examined utilisation of an online treatment programme for anxiety and depression in four Catholic boys’ high schools. The second study examined the development and prevention of anxiety and depression in two independent and one government-run girls’ school. Of 5005 students enrolled at the time of testing, 3149 consented and participated (62.9% response rate). Participants were 63.5% male (n = 2000) and had a mean age of 14.58 years (standard deviation [SD] = 1.37 years, range 12–18 years).
Procedure
Assessment sessions took place during school time, supervised by members of the research team. Questionnaires were completed confidentially using de-identified codes and participants were informed that confidentiality would be broken only if their questionnaire responses indicated serious risk of harm. The research was approved by the Human Research Ethics Committee of Macquarie University, reference 5201300531 and 5201100886, and by each school and their governing body.
All participants consented to involvement in the relevant larger study of emotional health, which included the measures used in the current study. Data presented here are from the initial stages of these larger studies. Parents were provided with written information about the study methods and were asked to discuss participation with their child. Information about the programmes was also provided directly to students, typically in school assemblies or class groups. At boys’ schools, parents were asked to fill in a form to opt out if they did not wish to participate. If parents did not opt out, students provided active consent via an online consent form. At girls’ schools, parents were required to provide written consent to opt in to the research and all students had the opportunity to opt out of testing verbally.
Measures
All participants
The socio-educational advantage of each school was assessed using the Index of Community Socio-Educational Advantage (ICSEA) (Australian Curriculum and Assessment Reporting Authority, 2013). The ICSEA has a mean of 1000 (SD = 100), with higher scores indicating greater socio-educational advantage of the school.
Participants provided demographic information and, if relevant, answered brief questions addressing past assessment or treatment for mental health concerns including the reasons for seeking help, the type of professional consulted, and when services were accessed. They also completed the following measures.
The Body Dysmorphic Disorder Questionnaire–Adolescent Version (BDDQ-A; Phillips, 2005) is a brief screening measure designed to assess Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria for BDD (APA, 1994). Figure 1 displays the content and application of the BDDQ-A. Additional open text items assess the nature of any impairment, and the body areas of concern. The adult BDDQ has good sensitivity (100%) and specificity (89–93%) in psychiatric settings (Grant et al., 2001; Phillips et al., 1995), although sensitivity and specificity information has not yet been established for the BDDQ-A.
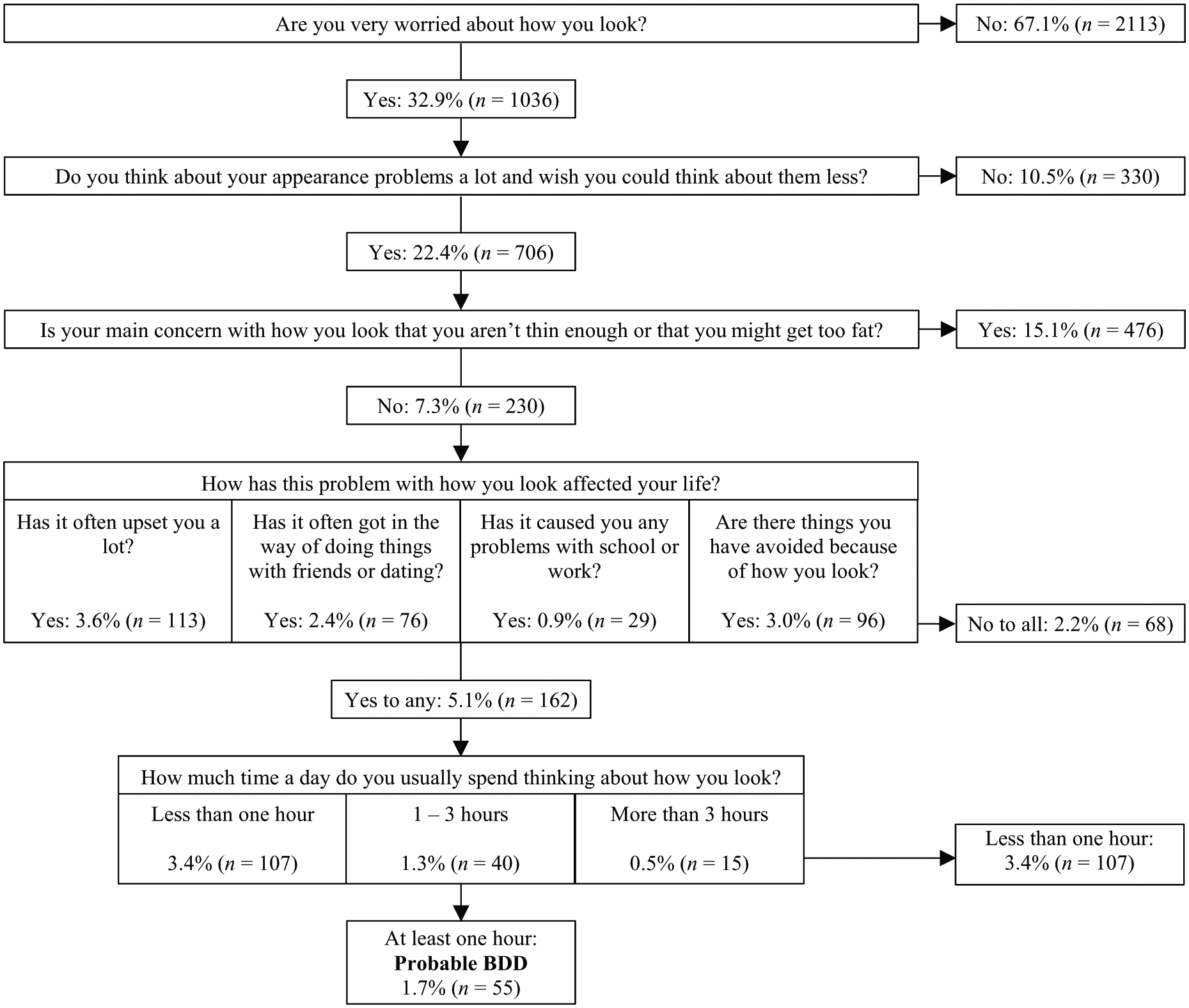
Categorisation of participants using the Body Dysmorphic Disorder Questionnaire–Adolescent Version (n = 3149).
The Body Image Questionnaire, Child and Adolescent Version (BIQ-C; Veale, 2009) examines BDD symptoms such as appearance checking, avoidance and interference. The questionnaire begins with a screening item. If the participant is happy with their appearance and does not want to improve any particular features, they do not answer further items and receive a total score of 0. All other participants rank up to five body areas of concern, then answer 12 items about BDD symptoms with response options ranging from 0 to 8. Psychometric data have not yet been published for the BIQ-C. Cronbach’s alpha for the 12 symptom items was α = 0.88 in the current study.
The Child version of the 26-item Eating Attitudes Test (ChEAT-26; Maloney et al., 1988) measures disordered eating attitudes and behaviours. The least problematic responses (never, rarely, sometimes) are scored 0, with remaining responses scored 1 (often), 2 (very often) or 3 (always). Good internal consistency has been found in previous adolescent populations (Smolak and Levine, 1994). In the current study, internal consistency was α = 0.87. A ChEAT-26 total score of 20 or above indicates a high risk of clinically significant eating disorder pathology in young people (Maloney et al., 1988).
The Spence Children’s Anxiety Scale (SCAS; Spence, 1998) contains 38 items assessing social anxiety, separation anxiety, generalised anxiety, panic/agoraphobia, obsessive-compulsive disorder and physical injury fears, rated from 0 (never) to 3 (always). The scale has strong psychometric properties (Spence et al., 2003). In this study, total scale internal consistency α = 0.93. Age and sex-specific cut-off scores have been developed from Australian community norms that identify the top 16% of anxiety scores (Spence, n.d.).
The Short Mood and Feelings Questionnaire (SMFQ; Angold et al., 1995) measures 13 depressive symptoms from 0 (not true) to 2 (true). The SMFQ correlates well with diagnostic measures of depression and discriminates between depressed and non-depressed individuals, with a total score > 7 suggesting elevated depressive symptoms (Angold et al., 1995). The measure has been found to have strong internal consistency (Rhew et al., 2010), current study α = 0.92.
Male participants only
The Drive for Muscularity Scale (DMS; McCreary and Sasse, 2000) measures muscularity-driven behaviours and body image concerns. The anabolic steroid use item was omitted (McCreary et al., 2004), so the total score is the mean of the remaining 14 items scored from 1 (never) to 6 (always). As muscularity concerns are primarily linked to body image dissatisfaction among males (McCreary, 2007), the DMS was administered to male participants only. The measure has good internal consistency (McCreary et al., 2004), current study α = 0.93.
Two additional measures were administered only at boys’ schools due to differences in the design of the two larger studies. The Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) assesses emotional symptoms, conduct problems, hyperactivity and peer problems using 20 items scored from 0 (not true) to 2 (certainly true). These are summed to create a total difficulties scale; in this study, α = 0.83. Age and sex-specific cut-off scores have been developed from Australian community norms that identify the top 10% of responses (Mellor, 2005).
The Pediatric Quality of Life Enjoyment and Satisfaction Questionnaire (PQ-LES-Q; Endicott et al., 2006) contains 14 items assessing life satisfaction across a range of physical, emotional and social domains. Items are scored from 1 (very poor) to 5 (very good), and the total score is converted to the percentage of the maximum possible score (range 0–100%). The measure shows strong internal consistency and test–retest reliability (Endicott et al., 2006). Internal consistency α = 0.92.
Data analysis
Analyses were conducted using SPSS version 23. Categorical variables were compared between groups using Pearson’s chi-square tests or Fisher’s exact tests, with odds ratios or Cramer’s V. Continuous variables were compared between groups using Independent-Samples t-tests, with Cohen’s d as the measure of effect size.
Results
Demographic characteristics
The demographic characteristics of participants are given in Table 1. Compared to the non-BDD group, pBDD participants were older and more likely to live in ‘other’ household types, such as blended families or families with non-parent primary caregivers. Furthermore, pBDD participants were less likely to report their mothers had an Oceanian cultural background (e.g. Australian, New Zealander, Melanesian or Polynesian), and more likely to report ‘other’ cultural backgrounds (Africa, the Middle East and the Americas). There was no association between the school attended and BDD prevalence; χ2(1, N = 3149) = 3.95, p = 0.684, Cramer’s V = 0.04.
Comparison of demographic characteristics between probable-BDD and non-BDD participants.
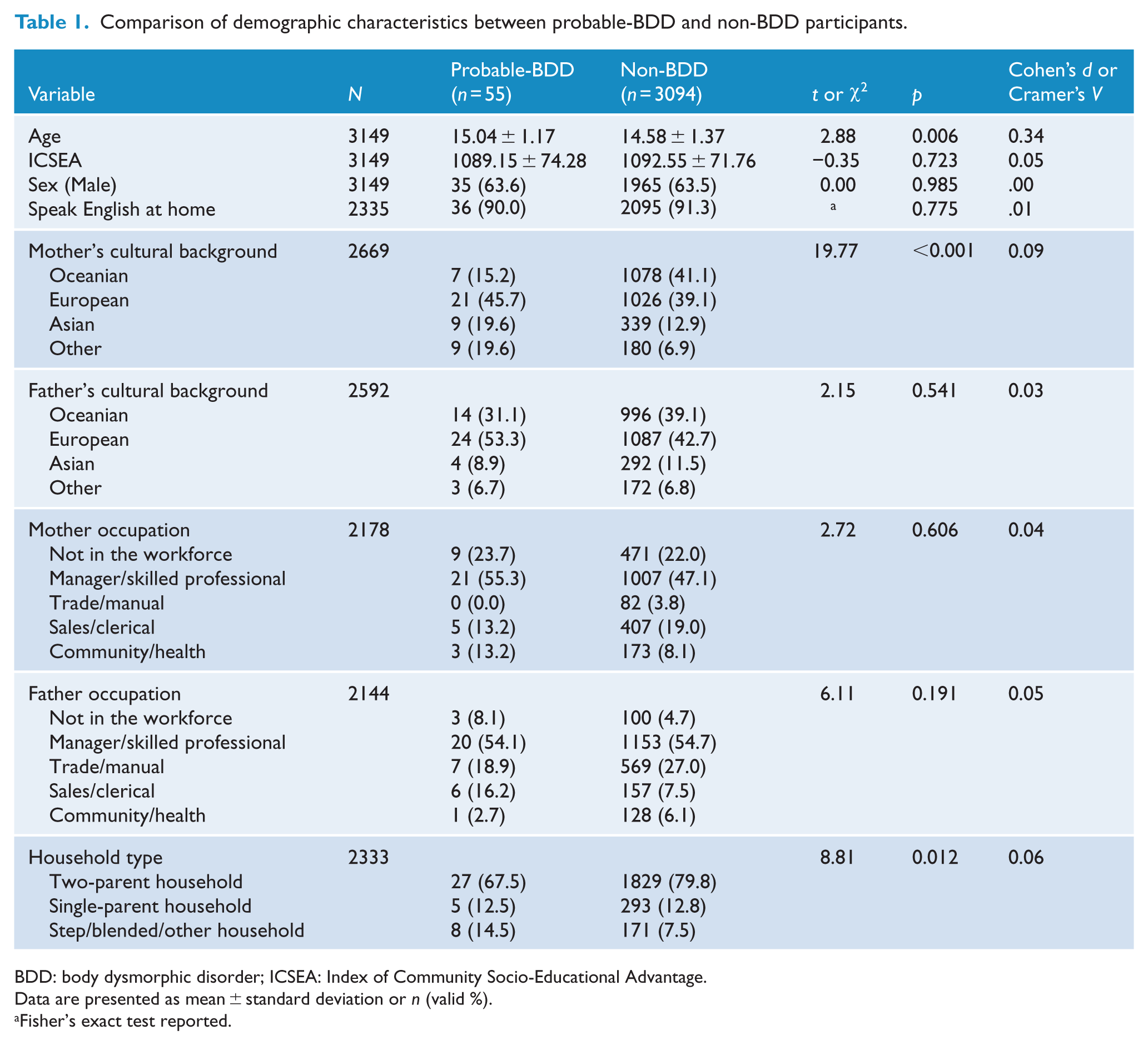
BDD: body dysmorphic disorder; ICSEA: Index of Community Socio-Educational Advantage.
Data are presented as mean ± standard deviation or n (valid %).
Fisher’s exact test reported.
Prevalence and presentation of pBDD
pBDD was identified in 55/3149 participants (1.7%, 95% confidence interval [CI] = [1.4, 2.3]). As predicted, there was no difference in pBDD prevalence between males (35/2000 = 1.8%, 95% CI = [1.3, 2.4]) and females (20/1149 = 1.7%, 95% CI = [1.1, 2.7]), χ2(1, N = 3149) = 0.00, p = 0.985, odds ratio = 1.00 (95% CI = [0.57, 1.73]). The prevalence of pBDD was higher among adolescents aged 15–18 years (39/1637 = 2.4%, 95% CI = [1.8, 3.2]) compared to those aged 12–14 years (16/1512 = 1.1%, 95% CI = [0.7, 1.7]), χ2(1, N = 3149) = 8.03, p = 0.005, odds ratio = 2.28 (95% CI = [1.27, 4.10]).
The 55 pBDD participants most frequently endorsed BDDQ-A items relating to distress (85.5%), followed by avoidance (65.6%), interference with socialising or dating (50.9%) and interference with school or work (21.8%). Most (72.7%) reported thinking about their appearance for 1–3 hours per day, whereas relatively few (27.3%) spent more than 3 hours a day. pBDD participants typically reported multiple body areas of concern (M = 5.3, SD = 2.7, range = 1–13). The most commonly disliked areas were the skin (63.6%), nose (40.0%), hair (34.5%), muscularity (32.7%), stomach (23.6%), weight (21.8%), height (21.8%) and legs (20.0%).
Comparison between pBDD and non-BDD participants
Table 2 presents the comparison of BDD symptoms, comorbid symptom and quality of life between the pBDD and non-BDD groups. Mean symptom scores were significantly higher for pBDD participants than non-BDD participants for all outcome measures. As anticipated, pBDD participants reported significantly higher BIQ-C symptoms of BDD than non-BDD participants. This represented a very large effect size and is consistent with their categorisation using the BDDQ-A. Large effect sizes were also found for group differences in symptoms of depression, social anxiety and generalised anxiety, and in measures administered to males only, for total difficulties, emotional symptoms, peer problems, hyperactivity, drive for muscularity and reduced quality of life. Post hoc analysis of covariance was conducted examining the association between BDD group and symptom scores, controlling for age, sex, mother’s cultural background and household type. The effect of BDD group remained significant in most analyses, with minor reductions in partial eta squared (details available from the first author upon request). However, BDD group was not a significant predictor of scores on the measure of eating disorder symptoms in the analysis of covariance.
Symptom severity and quality of life comparisons between probable-BDD (n = 55) and non-BDD (n = 3094) participants.
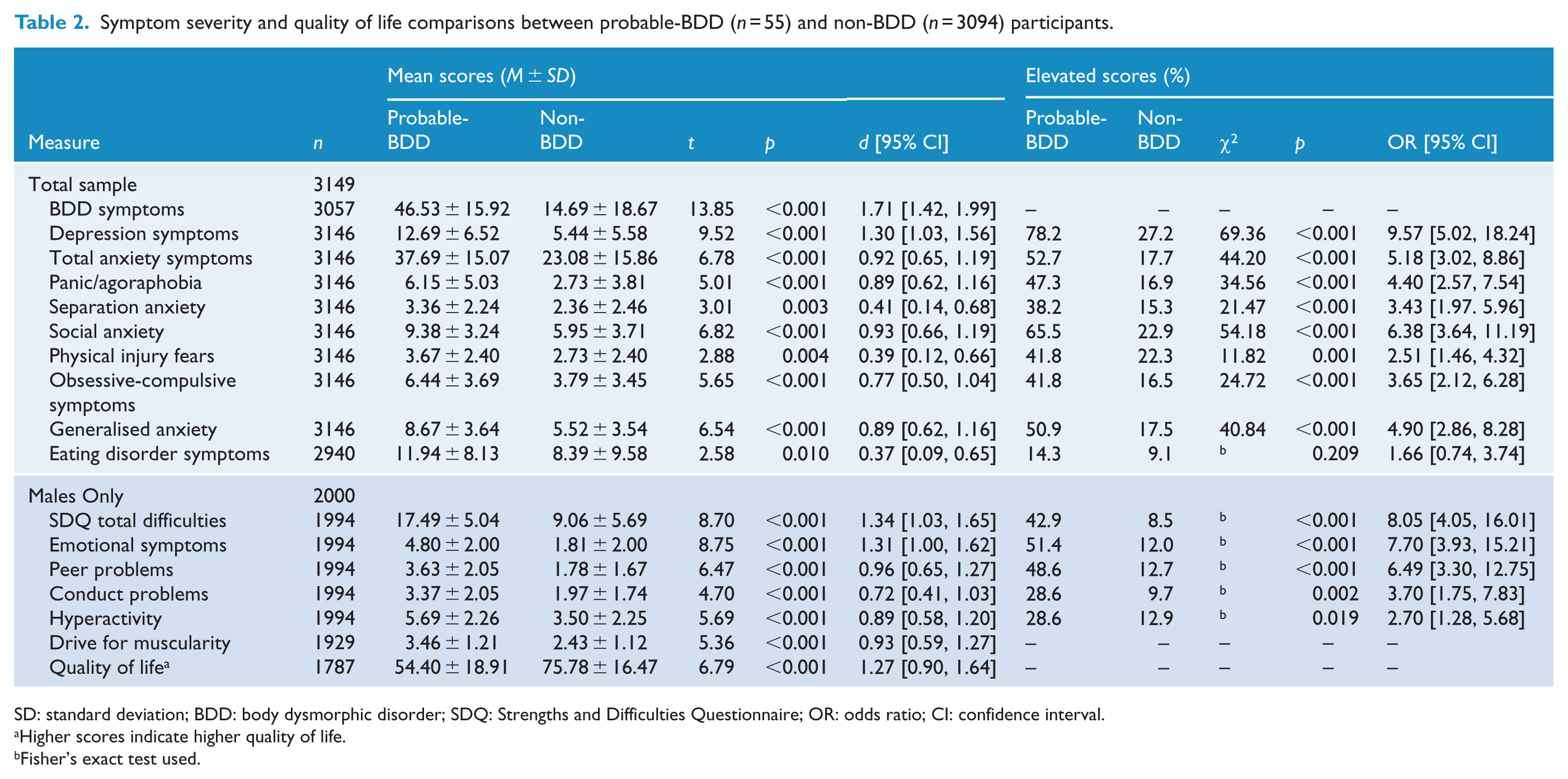
SD: standard deviation; BDD: body dysmorphic disorder; SDQ: Strengths and Difficulties Questionnaire; OR: odds ratio; CI: confidence interval.
Higher scores indicate higher quality of life.
Fisher’s exact test used.
Table 2 also presents the percentage of participants in each group with elevated scores (where measures had published cut-off scores). The pBDD group experienced significantly higher odds of reporting elevated symptoms across all measures with established cut-off scores, again with the exception of the measure of eating disorders. The highest odds ratios were obtained for symptoms of depression and social anxiety and, for male participants, emotional symptoms and peer problems.
Past mental health service use was more common for pBDD (40.9%) than non-BDD participants (15.8%), χ2 (1, N = 2638) = 20.06, p < 0.001, odds ratio 3.69 (95% CI = [2.00, 6.79]). No participants reported BDD or similar concerns among their reasons for accessing services.
Discussion
The current study was the first to examine the prevalence and correlates of pBDD in a large, community-based sample of adolescents. The observed pBDD point prevalence (1.7%) is at the lower end of estimates from previous studies in adolescents and adults (Koran et al., 2008; Mayville et al., 1999; Rief et al., 2006). Older adolescents had higher pBDD prevalence than younger adolescents, consistent with reports of mean BDD onset at 16 years (Bjornsson et al., 2013). No sex difference in pBDD prevalence was observed, consistent with most studies using DSM-IV criteria (Buhlmann et al., 2010; Koran et al., 2008; Rief et al., 2006). Therefore, although symptoms of BDD may be more common among females than males (Buhlmann et al., 2010; Mastro et al., 2016), the prevalence of full criteria BDD appears to be equal between adolescent males and females.
Most demographic characteristics were similar between BDD groups, although pBDD participants were slightly older, and there were some differences in household type and mothers’ cultural background. The number and types of body areas of concern reported by participants in the current study were similar to those observed in clinical adolescent samples (Phillips et al., 2006a), with skin, facial features and hair the most common focus of concern. As predicted, pBDD was associated with markedly elevated symptoms of anxiety, depression, obsessive-compulsive disorder and eating disorders, and differences between pBDD and non-BDD groups on these measures were not accounted for by age, sex, mothers’ cultural background or household type. Additionally, pBDD participants were more likely to report abnormal or elevated levels of most comorbid symptoms. This is consistent with the high rates of these disorders found in clinical samples of youth with BDD (Albertini and Phillips, 1999; Phillips et al., 2006a), and the elevated symptoms of depression and social anxiety in adolescents at high risk of BDD in the community (Mastro et al., 2016). However, the likelihood of reporting high-risk eating disorder scores was not elevated among pBDD participants in the current study, and the association between pBDD and elevated levels of eating disorder symptoms was no longer significant when age, sex, mother’s cultural background and household type were statistically controlled. These findings may be due, in part, to the use of the BDDQ-A, which excludes individuals with primary weight concerns from the pBDD group.
For the measures administered only to males, pBDD was associated with significantly poorer quality of life, and higher levels of muscularity concerns, emotional symptoms, peer problems, hyperactivity and conduct problems. Quality of life impairment in males with pBDD was notable, with scores similar to young people receiving treatment for major depressive disorder (Endicott et al., 2006). Although quality of life does not appear to differ between adult males and females with BDD (Phillips et al., 2006b), it is unclear whether this is the case among adolescents.
Rates of prior contact with mental health services were significantly higher for pBDD than for non-BDD participants, although no participant reported BDD as a reason for accessing these services. This mirrors the adult literature, where individuals with BDD typically receive treatment for comorbid mental health problems rather than BDD per se, even when BDD is the most interfering problem (Grant et al., 2001; Veale et al., 2015). As insight among adolescents with BDD may be particularly poor (Phillips et al., 2006a), mental health professionals should screen for BDD among adolescents with a range of presenting problems, and consider incorporating parent reports when assessing the impact of BDD symptoms.
Limitations
Whereas face-to-face interviews with a structured BDD diagnostic module remain the gold standard for assessment of BDD, epidemiological studies typically demand the use of self-report measures. Hence, the current study identified pBDD. Although the sensitivity and specificity of the BDDQ are strong in adults (Grant et al., 2001; Phillips et al., 1995), this has yet to be established in adolescents. The study began prior to the release of Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) (APA, 2013), and the BDDQ-A was developed using DSM-IV criteria. Automatically excluding participants from a potential BDD diagnosis based on a broad weight concern question is likely to lead to the underestimation of BDD prevalence (Brohede et al., 2015; Koran et al., 2008). As BDD with primary weight concern may be particularly common in female adolescents (Dyl et al., 2006), use of this criterion may have resulted in underestimation of pBDD prevalence among female participants in the current study. Data on the SDQ and PQ-LES-Q were not available for females, thus limiting conclusions about associations between BDD status and scores on these measures to males. Finally, all participating schools were socio-educationally advantaged to some extent, so the generalisability of the findings to less advantaged students is unclear.
Conclusion
This study is the first to have examined pBDD prevalence and correlates in a large community sample of adolescents. The prevalence of pBDD in adolescents is similar to adult samples, and pBDD is associated with substantial distress, impairment in quality of life and comorbidity with other mental health problems. Furthermore, population-based research is needed to elucidate the prevalence and correlates of BDD in young people and thereby inform prevention and early intervention efforts.
Footnotes
Acknowledgements
We would like to thank the students and staff of each school, and Laura Clark (MSc), Keila Brockveld (PhD) and Danielle Einstein (PhD) from the Centre for Emotional Health, Department of Psychology, Macquarie University, Sydney, Australia, for their assistance with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The research was supported by (1) Macquarie University Research Excellence Scholarship awarded to Sophie Schneider; (2) Australian Research Council grants LP130100576, FT120100217; (3) beyondblue National Priority Driven Research funding; and (4) a Sponsored Research Project grant from Macquarie University and one participant school awarded to Jennifer Hudson. These funding sources had no involvement in the study design, data collection, analysis or interpretation and writing of the report. Schools were given a copy of the completed manuscript prior to submission to check that details of school involvement were accurately reported.