
Abstract
Objective:
Primary care practitioners are well placed to support diagnosis and appropriate treatment of eating disorders as they are often the first point of contact with the health care system. However, little is known about management of eating disorders in primary care. We aimed to estimate the prevalence of management of eating disorders in primary care and identify how these disorders are managed.
Methods:
This study used data from the Bettering the Evaluation of Care of Health programme, which annually surveys 1000 randomly sampled general practitioners in Australia who each record details of 100 successive patient encounters. In total, data were utilised from 1,568,100 primary care encounters between 2000/2001 and 2015/2016.
Results:
Eating disorders were managed in less than 1% of primary care encounters between 2000/2001 and 2015/2016. When extrapolated to the Australian population, up to 0.32% of the population were managed in primary care for a primary or probable eating disorder. In the majority of encounters where an eating disorder was managed (58.5%), the encounter was initiated for reasons other than the eating disorder itself. Of a group of patients identified with a clinically significant low body mass index (N = 5917), a small number (n = 118) had either no other diagnosis or a related condition that may be indicative of an eating disorder. In encounters where an eating disorder was managed, referrals to a mental health specialist/service, medical specialist and nutritionist/dietician were provided in 20%, 8% and 6% of encounters, respectively. Mental health treatment plans, which provide subsidised access to mental health services, were ascribed in approximately 7.7% of encounters where an eating disorder was managed.
Conclusion:
Primary care provides an opportunity to improve detection and management of eating disorders, particularly when patients present for ‘other’ issues or with unexplained low body mass index and one or more symptoms related to an eating disorder.
Eating disorders are estimated to affect up to 15% of the Australian population (Hay et al., 2015, 2017). Onset of these disorders typically occurs between 12 and 21 years of age (Hudson et al., 2007; Swanson et al., 2011; Volpe et al., 2016), and females are estimated to be 4.2 times more likely to develop an eating disorder than males (Qian et al., 2013). Eating disorders are related to a wide range of medical complications in the gastrointestinal, cardiovascular, neurological and skeletal system (Mitchell and Crow, 2006; Westmoreland et al., 2016). In addition, they have high mortality and suicide rates (Chesney et al., 2014; Smink et al., 2012) with anorexia nervosa having one of the highest mortality rates of any psychiatric illness (Arcelus et al., 2011; Chesney et al., 2014). The psychological impact of eating disorders is also considerable with approximately 70% of those affected having at least one additional mental health diagnosis (Keski-Rahkonen and Mustelin, 2016; Ulfvebrand et al., 2015) often co-occurring anxiety and mood disorders (Hach et al., 2005; Keski-Rahkonen and Mustelin, 2016; Ulfvebrand et al., 2015).
Despite the associated morbidity and mortality experienced by people with an eating disorder, a systematic review of 14 studies found only one in four people (23.2%) accessed treatment for the disorder, where treatment included access to any medical or mental health professional who was qualified to provide treatment for an eating disorder (Hart et al., 2011). Importantly, while many individuals do not seek treatment for the eating disorder per se, studies show that they may have relatively higher rates of health service utilisation than their healthy counterparts (Ogg et al., 1997; Striegel-Moore et al., 2008; Swanson et al., 2011). In particular, higher access rates have been found in primary care, both before and after diagnosis (Mond et al., 2008; Ogg et al., 1997; Striegel-Moore et al., 2008). These findings suggest that primary care may provide an opportunity to identify and manage people with eating disorders; however, there is little contemporary data on rates and reasons for presentation, and course of care.
Primary care practitioners are well placed to support the diagnosis of eating disorders and facilitate access to appropriate treatment as they often are the first point of contact with the health care system and first to diagnose and treat eating disorders (Walsh et al., 2000). There is limited data on the number and incidence of people presenting to primary care and how they are managed. Previous, older studies that assessed rates between the 1990s and early 2000s found relatively stable rates of anorexia nervosa and declines in rates of bulimia nervosa (Currin et al., 2005; Smink et al., 2012; van Son et al., 2006). In a more recent UK study, eating disorders identified by general practitioners (GPs) were estimated to almost double in incidence from 17 to 30 per 100,000 persons between 1993/1994 and 2003/2004 and then levelled off at 22 per 100,000 persons in 2016/2017 (Demmler et al., 2020). More contemporary data exploring current rates and reasons of people with eating disorders presenting to primary care and subsequent referral and management of these patients are required to assess whether this entry point into the healthcare system is being effectively utilised.
The role of the primary care practitioner in managing eating disorders is even more crucial in Australia as they are one of the main gatekeepers for patients to access subsidised mental health care. Since 2006, primary care practitioners in Australia, along with paediatricians and psychiatrists, have been able to complete a Mental Health Treatment Plan (MHTP) that allows patients with a mental health diagnosis to access 6–10 subsidised sessions with a mental health clinician each year (Australian Government Department of Health, 2012). In late 2019, this programme was extended to enable individuals with an eating disorder to access up to 60 rebated sessions (40 psychological, 20 dietetic) (Australian Government Department of Health, 2019). Despite the key role primary care practitioners play in identifying eating disorders and managing and facilitating access to multidisciplinary care for patients with an eating disorder, there is limited data on the uptake and use of MHTPs for this group.
Given the limited contemporary data on rates and management of people with eating disorders presenting to primary care, the aims of this study were to estimate the prevalence and management of people with eating disorders in primary care; to identify their demographic characteristics, examine reasons for attendance, nature of management, referral and/or intervention; and to assess the extent to which MHTPs are utilised in the management of eating disorders.
Methods
Data source
Data from the Bettering the Evaluation of Care of Health (BEACH) programme were used to examine the prevalence and management of eating disorders in primary care. Each year, the BEACH programme surveyed an ever-changing sample of 1000 randomly sampled primary care providers, known as GPs in Australia, who each recorded details of 100 successive patient encounters (Britt et al., 2016). The survey captures information on a range of patient demographic characteristics, patient reason(s) for the encounter, up to four problems/diagnoses (i.e. new and existing) managed during the encounter and information on the intervention undertaken for problems/diagnoses (e.g. patient referral, medication). Diagnoses are coded using the International Classification of Primary Care Version 2 PLUS (ICPC-2 PLUS) (Britt, 1997) and then automatically classified to ICPC-2 (World Organization of National Colleges Academies & Academic Associations of General Practitioners/Family Physicians, 2005).
Study participants
Two study groups were identified from the BEACH data. The first study group included all GP encounters with patients that occurred between April 2000 and March 2016. The second study group was a subset of the first and included the 40% of GP encounters where they were asked to record patient weight and height.
Study outcome
The study outcome of interest was when a GP recorded that they had managed an eating disorder, either new or existing, during the GP encounter. A number of ICPC-2 PLUS codes were identified and used to classify ‘Primary’ and ‘Probable’ eating disorders. Primary eating disorders included the following: Anorexia nervosa (P86002); Bulimia (P86003); Disorder, eating, behavioural (P86004); Disorder, eating, child, psych (P11001); and Pica, child (P11004). Probable eating disorders ICPC2-PLUS codes included the following: Problem eating, behavioural (P86005); Binge eating (T02008); Disorder eating, adult (T05006); Problem eating, child psychological (P11003); Problem feeding, child psychological (P11002); and Disorder eating, child (T04011). Medicare item numbers associated with MHTPs and GP provision of focused psychological strategies were also assessed and included.
Consultation with a panel of specialist clinicians with expertise in the management of people with eating disorders, including GPs and psychologists, was undertaken to examine whether additional criteria could be used to identify possible eating disorder cases not managed at the encounter. Criteria identified by the panel informed the second study group and included a body mass index (BMI) of less than 17.5 kg/m2, consistent with the International Classification of Diseases version 10 (ICD-10) definition for anorexia nervosa (World Health Organization, 1992) and at least one additional diagnosis or problem that may be associated with the presence of an eating disorder (Supplementary Table 1 for a list of ICPC2-PLUS diagnosis/problem codes identified by expert group as relevant to a possible eating disorder).
Additional variables
Information was also available on a range of patient and GP sociodemographic characteristics. Patient information utilised in this study included patient age, sex (i.e. male, female), English or non-English speaking background and whether the patient was a Health Concession Care Card holder. Patient residential postcode was used to derive state of residence and geographical location (i.e. major city, regional or remote) using the Australian Statistical Geography Standard classification and socioeconomic status using Australian Bureau of Statistics Index of Relative Socio-Economic Advantage and Disadvantage (IRSAD) (Australian Bureau of Statistics, 2012a, 2013). The IRSAD is a score assigned to each postcode, and categorised into deciles with lower deciles reflecting areas of ‘relatively greater disadvantage and a lack of advantage’, while higher deciles reflected a ‘relative lack of disadvantage and greater advantage in general’ (Australian Bureau of Statistics, 2013). For analysis, IRSAD deciles were aggregated to form quintiles. GP characteristics included age, sex, practice location (major city, regional, remote), number of years practicing, country of graduation and whether the GP was a fellow of the Royal Australian College of General Practitioners.
Data analysis
The number and rate of management of primary and probable eating disorders reported by the GP during an encounter was calculated for the overall study group. Where an eating disorder was recorded, rates of referral and activity (i.e. procedures, other treatment and counselling) were calculated for each study group. Rates of management of primary and probable eating disorders were extrapolated to the Australian population using total population figures and information on the proportion of people who had seen a GP in Australia in any given year (Australian Bureau of Statistics, 2012b, 2019). Details of method used to extrapolate management rates to the Australian population are provided in Supplementary Table 2.
Referrals were aggregated into four categories including (1) mental health professionals/services, (2) dietician/nutritionist, (3) other medical specialist/services and (4) community/allied health/other. Mental health professionals/services identified in the data and included in this category were counsellor, mental health team, psychologist, psychiatrist, psych clinic and hospital psychiatrist. Details of practitioners/services in each category are provided in Supplementary Table 3. Information on the provision of MHTPs are recorded as part of the activities related to each diagnosis managed in the primary care encounter and are also recorded in a separate item which captures Medicare items related to the encounter. For the second study group, consisting of adults aged 18 and over with a BMI of 17.5 kg/m2 or less, the frequency of those with and without a recorded eating disorder–related problem or diagnosis were quantified and for those without, the presenting diagnoses were aggregated by ICPC2-PLUS component codes representing diagnosis, symptoms or management: (1) infections; (2) neoplasms; (3) injuries; (4) congenital anomalies; (5) other diagnoses; (6) symptoms/complaints; or (7) process codes (diagnostic/screening/preventive, medication/treatment/procedures, test results, administration, referrals). All analyses were conducted using SAS v9.4 and ethics approval for the study obtained from the Human Research Ethics Committee of the University of Sydney (Reference: 2012/130), and from the Australian Institute of Health and Welfare Ethics Committee (while they were a collaborating centre in 2000-2010).
Results
Between 2000/2001 and 2015/2016, 15,681 GPs recorded 1,568,100 encounters with patients. Overall, GPs reported management of 532 primary and 396 probable eating disorders, in total less than 1% (59.2 per 100,000) (Study Group 1) (Table 1). Anorexia nervosa accounted for almost two-thirds (62.2%) of all primary eating disorders and disordered eating three-quarters of all probable eating disorders (Table 1). Primary and probable eating disorders were newly identified in 16.3% of encounters, pre-existing in 64.0% and was of unknown status in 20.2% of encounters.
Frequency and rate of reported primary and probable eating disorders.
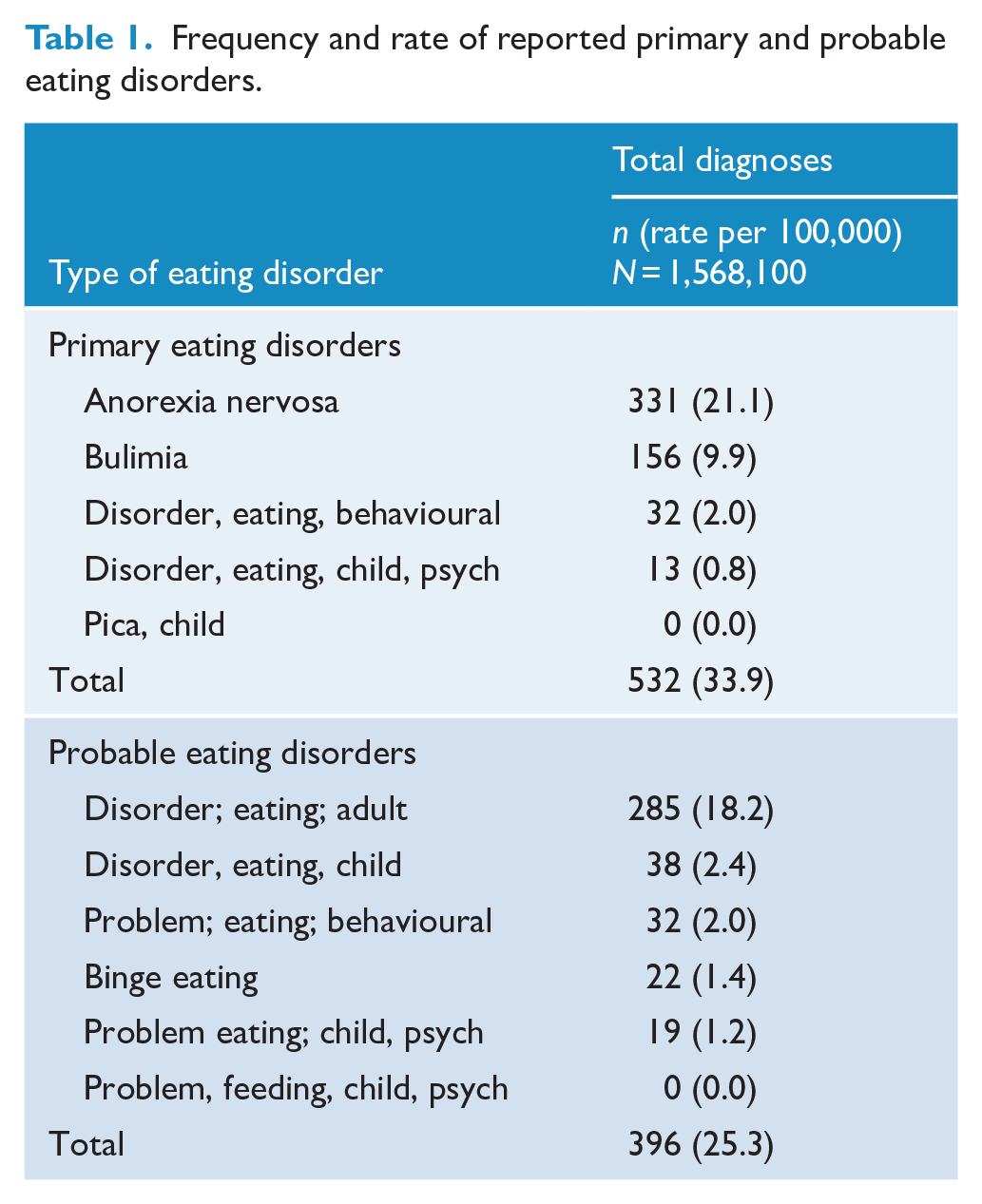
Over the study period, the reported management of both primary and probable eating disorders increased significantly from 23.0 to 43.5 per 100,000 GP encounters (χ2 = 45.1, p < 0.01) and 11.0 to 33.2 per 100,000 GP encounters (χ2 = 86.5, p < 0.01), respectively. When extrapolated to the Australian population, the average annual rate of primary eating disorder management was 180 per 100,000 persons and 140 per 100,000 persons for probable eating disorders. This translates to less than 0.18% and 0.14% of the Australia population managed in primary care each year for a primary or probable eating disorder, respectively.
The demographic characteristics of persons with a primary or probable eating disorder are presented in Table 2. The majority of people reported as having an eating disorder were female (95.7% and 86.4%, respectively), and almost two-thirds were aged between 18 and 44 years and most were from an English-speaking background (97.1% and 93.4%, respectively). For both primary and probable eating disorders, almost two-thirds of persons were from areas of greater advantage and lack of disadvantage and a lower proportion were concession card holders. Management of eating disorders was primarily provided by female GPs (72.7%), those aged between 35 and 49 years (49.0%) with practices located in metropolitan areas (75.6%). Most GPs were qualified with a Fellowship to the Royal Australian College of General Practitioners (FRACGP) (61.9%) and had over 10 years of experience (79%) (Table 3).
Demographic characteristics of people with primary or probable diagnosis of eating disorder.
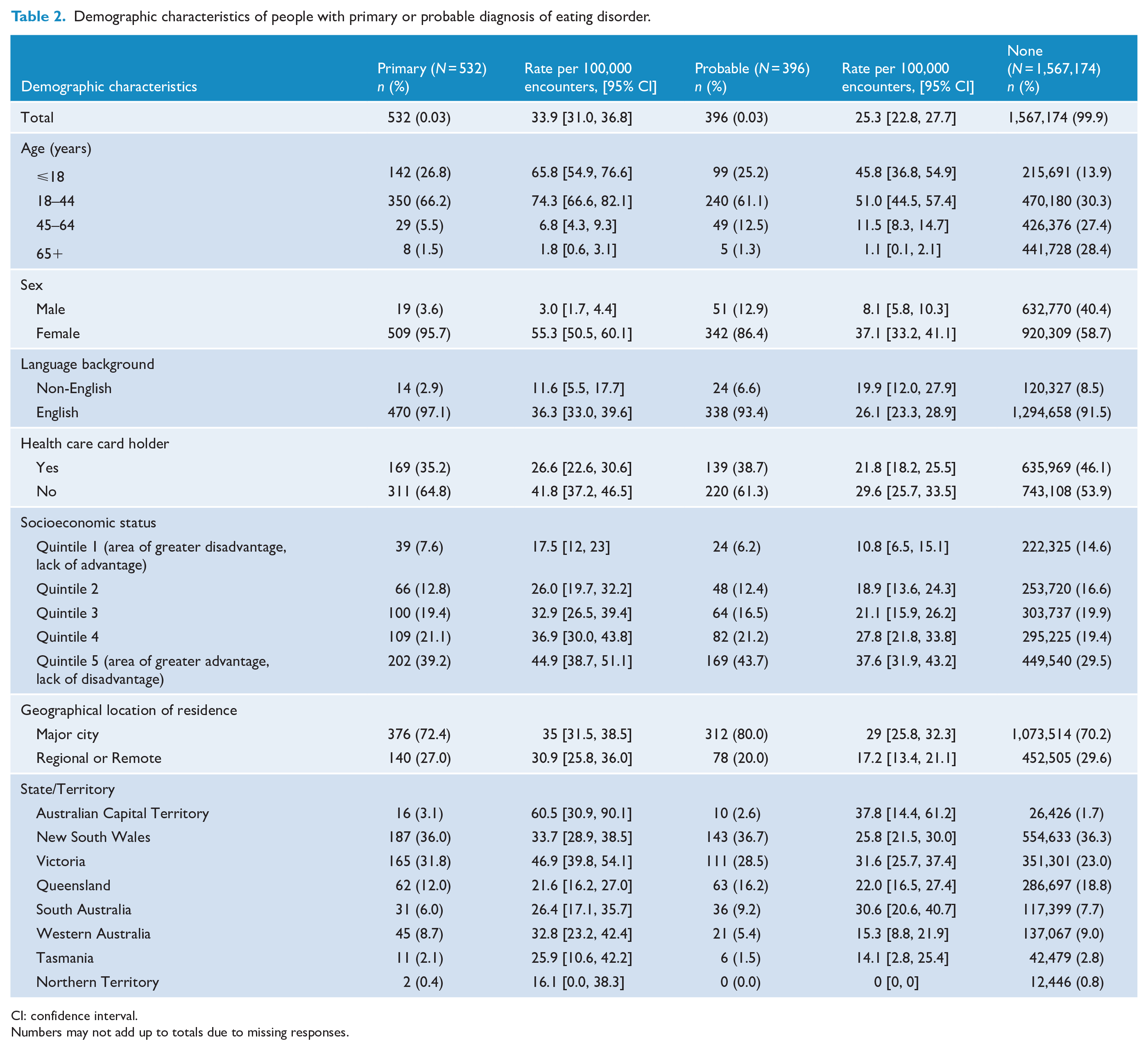
CI: confidence interval.
Numbers may not add up to totals due to missing responses.
GP characteristics of encounters where an eating disorder was reported, primary and probable.
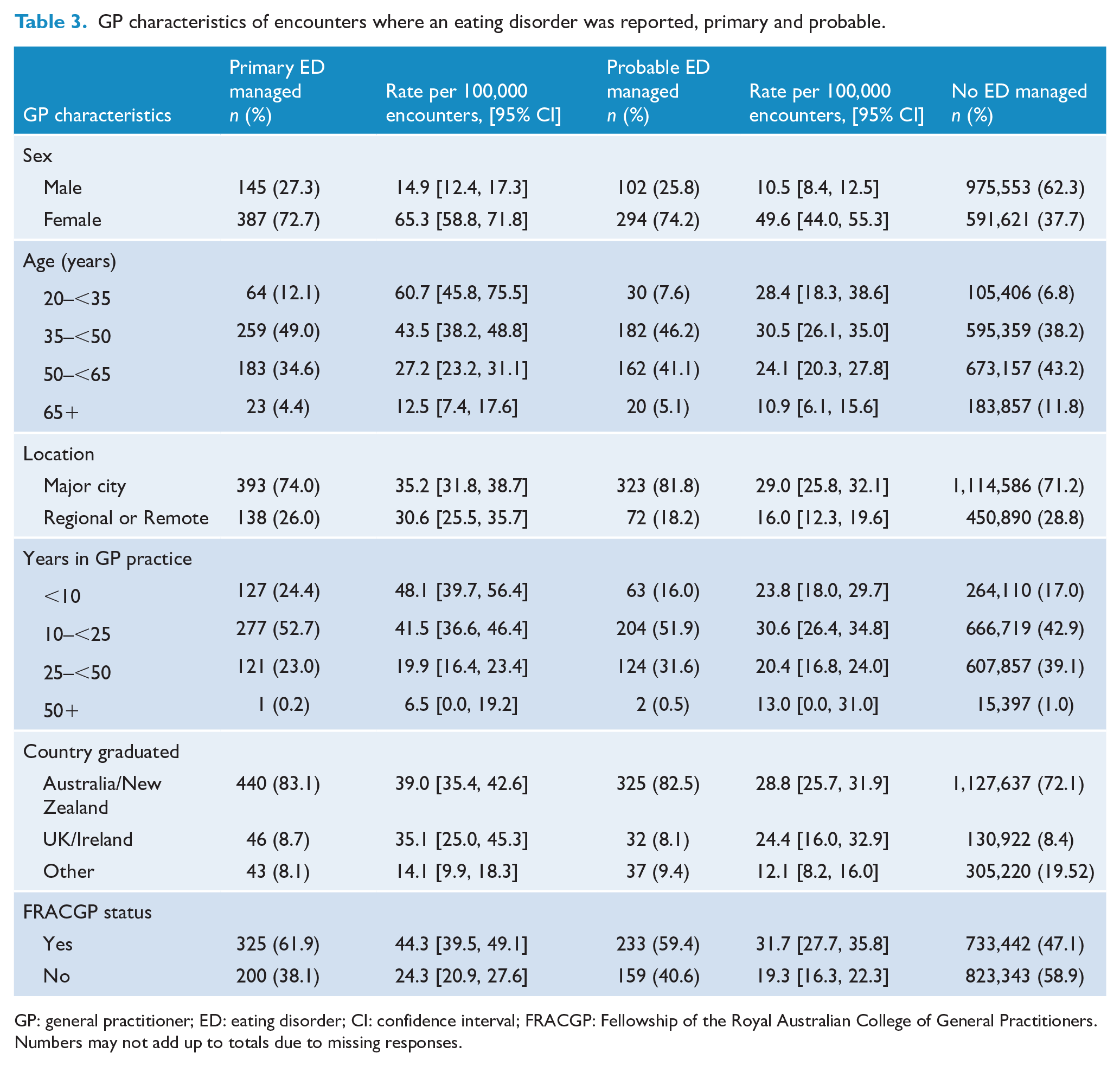
GP: general practitioner; ED: eating disorder; CI: confidence interval; FRACGP: Fellowship of the Royal Australian College of General Practitioners.
Numbers may not add up to totals due to missing responses.
The most common reasons for a patient with a primary or probable eating disorder to initiate a GP encounter are presented in Table 4. Approximately half of the patients attended for one issue. Patients nominated eating disorder diagnoses (i.e. primary or probable) as a reason for the GP encounter in approximately 41.5% of encounters where a primary (n = 222, 41.7%) or probable (n = 163, 41.2%) eating disorder was managed.
Reported reasons for encounter, frequency and type.
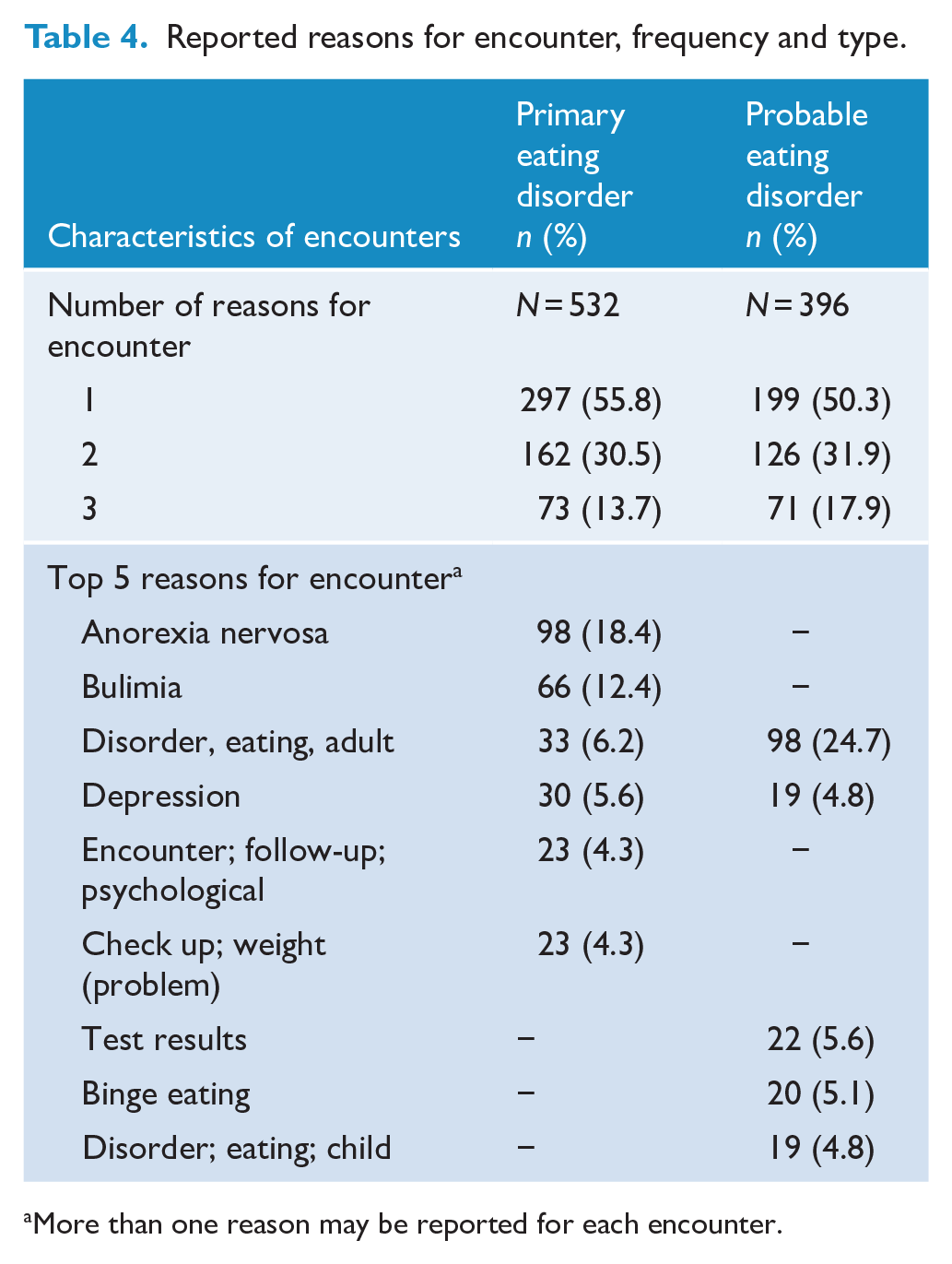
More than one reason may be reported for each encounter.
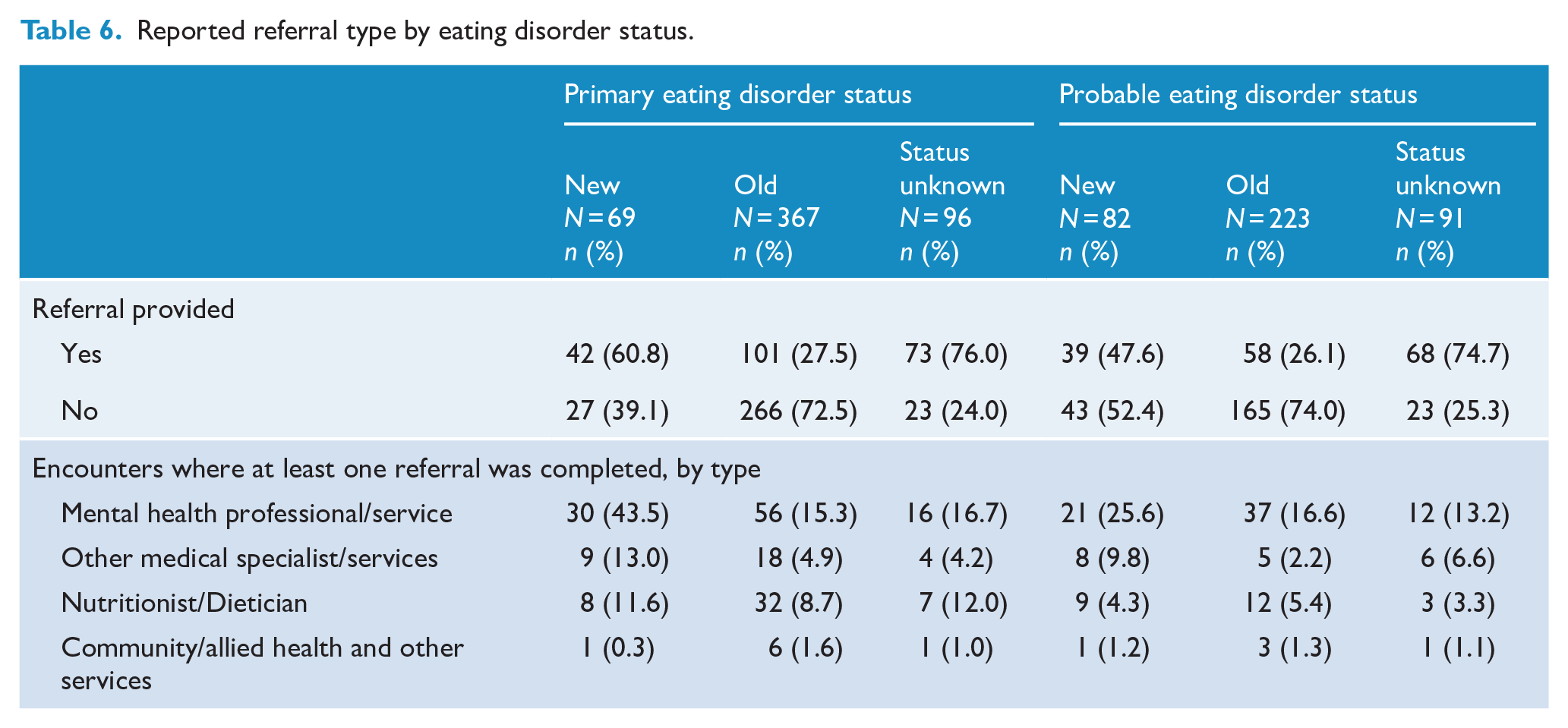
GPs recorded one or more activities in approximately three-quarters of encounters where a primary or probable eating disorder was managed. Therapeutic counselling and listening was the most frequent type of activity reported for both primary (n = 260, 48.9%) and probable eating disorders (n = 157, 39.6%; Table 4). Referrals to other health practitioners recorded in approximately 30% of encounters where an eating disorder was diagnosed (Table 5). In approximately 20% of encounters where a primary or probable eating disorder was managed, a referral to at least one mental health care practitioner/service was reported. A referral to a psychologist was recorded in 12.2% and 14.4% of encounters where a primary or probable eating disorder was managed, respectively. In approximately 5% of encounters, a referral to a nutritionist or dietician was recorded. Referrals for other medical specialists/services were reported in 5.8% and 4.8% of encounters where a primary or probable eating disorder was managed, respectively. Overall, referrals were higher for diagnoses that were new (primary: 60.1%; probable: 47.5%) compared with those existing prior to the GP encounter (primary: 27.0%; probable: 26.0%). The pattern of higher referrals for new diagnoses was found for all types of referrals (Table 6). Between 2006/2007 and 2015/2016, MHTPs were reported to be completed as part of the direct management of an eating disorder in 3.2% (n = 12) and 6.2% (n = 17) of GP encounters where a primary and probable eating disorder was managed, respectively. The provision of services related to MHTPs for any mental health issue for those with a recorded primary or probable eating disorder was as follows: preparation of MHTPs was recorded in 5.9% (n = 22) and 9.9% (n = 29) of encounters respectively; MHTP reviews in 0.5% (n = 2) and 1.0% (n = 3) of encounters, respectively; and GP mental health treatment consultation were recorded in 14.8% (n = 55) and 10.2% (n = 30) of encounters, respectively.
Characteristics of GP activities and reported referrals during encounter for primary and probable eating disorders.
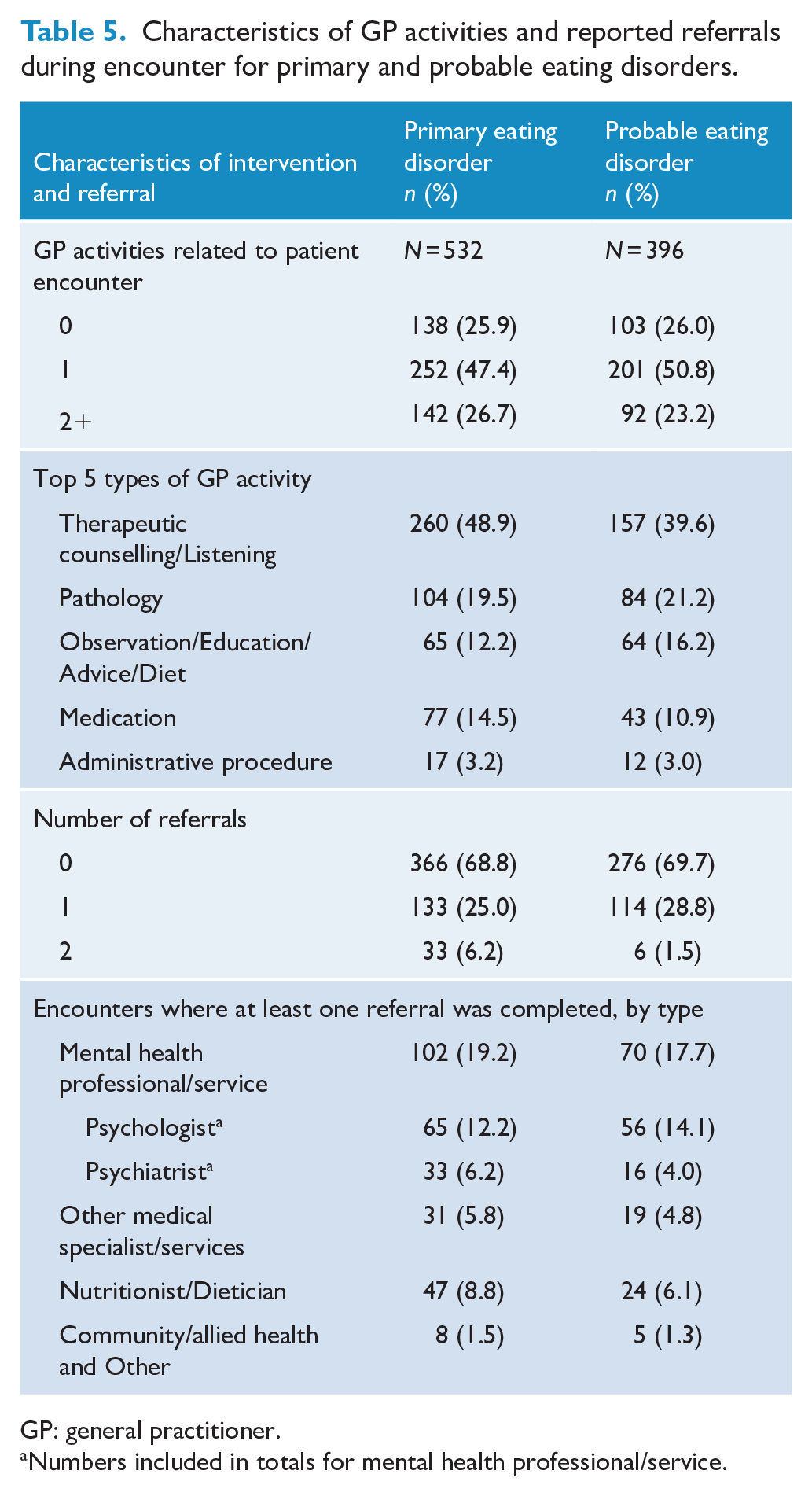
GP: general practitioner.
Numbers included in totals for mental health professional/service.
Reported referral type by eating disorder status.
Study group 2 aimed to detect possible eating disorders. From a total of 574,825 patients aged 18 or over who had weight and height information recorded, 5917 (1.0%) had a BMI ⩽ 17.5 kg/m2. Of these, 6.8% (n = 401) had a diagnosis or problem recorded that may be related to an eating disorder (see Supplementary Table 1). Approximately 70% of this group also had another diagnosis, condition, symptom/complaint or investigation recorded that may explain low BMI (Figure 1), while 29% of this group (n = 118) had no additional diagnosis, condition, symptom/complaint or investigation recorded to explain low BMI. Of those with a BMI ⩽ 17.5 kg/m2 that did not have a diagnosis recorded that may be related to an eating disorder (n = 5516, 93.2%), the majority had one (n = 3207, 58.1%) or two (n = 1549, 28.1%) recorded diagnoses, conditions, symptoms or investigations (Figure 1). See Supplementary Table 4 for disorder classifications for those with BMI ⩽ 17.5, with and without eating disorder–related problems/diagnoses.
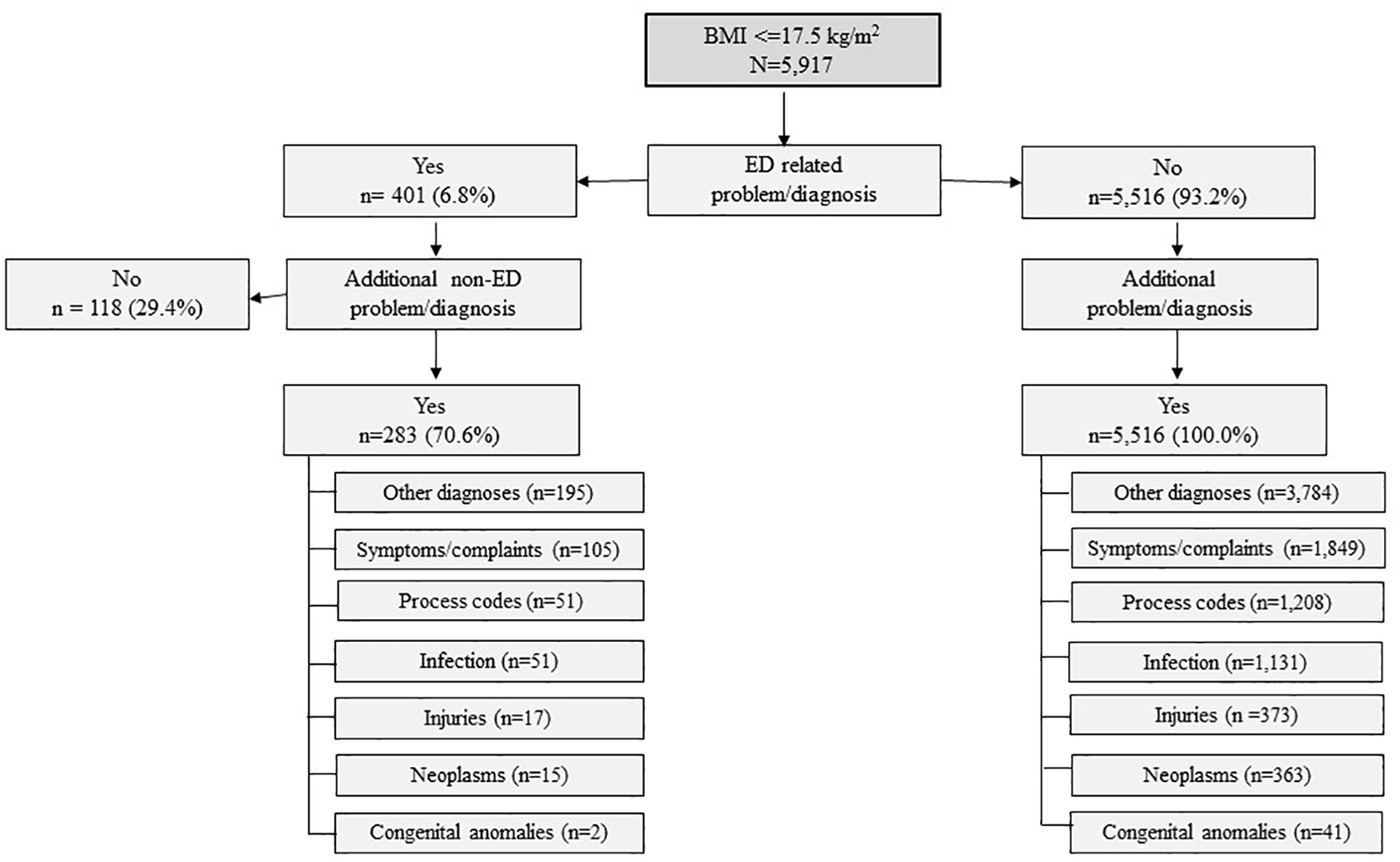
People with a possible eating disorder based on BMI ⩽ 17.5 kg/m2 and reported eating disorder-related diagnosis.a
Discussion
This is the first study to examine the rate of active management of eating disorders in primary care. Overall, eating disorders were reported to be managed in less than 1% of primary care encounters between 2000/2001 and 2015/2016. When extrapolated to the Australian population, we estimated that, each year, up to 0.32% of the population were managed in primary care for a primary or probable eating disorder. While rates of management were low relative to Australian population prevalence estimates, rates of management of primary and probable eating disorder doubled over the study period. Of note, approximately 40% of GP encounters for eating disorders were initiated for the condition, with most people presenting for reasons other than the eating disorder itself. Psychological counselling and listening was the most common form of intervention provided by primary care practitioners, while referrals to specialists and other health care practitioners occurred in approximately one-third of all encounters where an eating disorder was managed. MHTPs that enable access to subsidised mental health care were provided in 7.7% of these encounters. The study also attempted to identify a group of patients with a possible eating disorder based on a clinically significant low BMI (consistent with an ICD-10 diagnosis of anorexia nervosa) alongside an eating disorder–related diagnosis. Of all encounters where low BMI was identified, 6.8% had an eating disorder–related problem or diagnosis managed, and 29.4% had no other diagnoses. In most cases of low BMI, other diagnosis, conditions, symptoms or complaints were identified that may provide a non-eating disorder–related explanation for the symptoms.
This study offers a unique contribution to the literature with no other studies found to have examined the prevalence, and types, of active management of eating disorders in primary care in a nationally representative sample of GPs. Typically, studies in this area have focused on defining approaches to identify and manage eating disorders in primary care (Sim et al., 2010; Williams et al., 2008) or estimate the incidence of eating disorders in primary care (Currin et al., 2005; Demmler et al., 2020; Smink et al., 2016; van Son et al., 2006). Specifically, we found the management rate of anorexia nervosa was 21.1 per 100,000 GP patient encounters and 9.9 per 100,000 for bulimia. These rates were higher when compared to Dutch and UK studies from the 1980s to 1990s (Currin et al., 2005; Smink et al., 2016; van Son et al., 2006), and similar to recent 2016/2017 data from the United Kingdom (Demmler et al., 2020). Overall, our estimated annual rate of less than 0.32% of the population managed in primary care was considerably lower than population prevalence rates of eating disorders in Australia, which have been estimated at approximately 15% (Hay et al., 2015, 2017). This finding of unmet need at the primary care level is consistent with findings by Smink et al. (2012) who, in a review of the literature, found prevalence estimates of eating disorders in primary care to be substantially lower than prevalence estimates of eating disorders in the community (Anorexia nervosa: 160 vs 370 per 1,000,000 persons; Bulimia nervosa: 150 vs 1000 per 100,000 persons). This discrepancy between eating disorder prevalence and attendance to primary care has been attributed to a range of individual and practitioner-level factors. For individuals, this may include a lack of acknowledgement of problematic eating behaviours and an unwillingness to engage with services (Eisenberg et al., 2011; Hart et al., 2011), and for practitioners, limited knowledge of eating disorders and low levels of screening, identification and diagnosis of eating disorders have been identified (Currin et al., 2005; Hach et al., 2005; Hart et al., 2011; Linville et al., 2012; Mitchison et al., 2017).
In this study, females (95.7%) accounted for the vast majority of patients managed in primary care for an eating disorder. While the literature finds that females are typically more likely to develop an eating disorder, males have been found to account for approximately 25% of all eating disorders (Sweeting et al., 2015). The relatively high rates of management of eating disorders in primary care for females may indicate a bias on the part of the GPs towards identifying signs and symptoms of eating disorders in female patients. However, it may be that males with an eating disorder are less likely to present to primary practice. In addition, in this study female GPs were found to manage almost three-quarters of encounters where an eating disorder was managed. In a study of Australian GPs, female GPs were found to be more likely to manage female patients and psychological problems, despite patients with psychological problems presenting equally to male and female GPs (Harrison et al., 2011). Identifying the reasons for relatively low rates of management of eating disorders for males and low management of eating disorders by male GPs has the potential to inform strategies to improve identification of eating disorders in primary care and/or access to appropriate care.
The study also found that the majority of primary care encounters for people with an eating disorder were initiated for reasons not directly related to the disorder. These findings are consistent with previous studies where individuals with eating disorders are found to access a range of health care services and may actually present more often than those without an eating disorder (Ogg et al., 1997; Striegel-Moore et al., 2008; Swanson et al., 2011). For example, Striegel-Moore et al. (2008) found that individuals diagnosed with an eating disorder had significantly higher levels of contact with primary care, mental health services, emergency or urgent care departments and telephone consultations in the year prior to diagnosis. Ogg et al. (1997) found that patients with an eating disorder had significantly more consultations with a GP up to 5 years prior to an eating disorder diagnosis. Specifically, the authors found that 71% of those with an eating disorder had four or more consultations in the 5 years prior to diagnosis, compared with 18% for controls.
Excess weight and weight loss have also been identified as common reasons for accessing treatment (Mond et al., 2007). In a systematic review, Hart et al. (2011) estimated that between 30% and 74% of individuals who sought treatment did so for weight loss. Further reasons for the relatively high rates of access to treatment include high levels of psychological distress and impairment, comorbid mental health disorders and physical illness associated with the eating disorder (Striegel Weissman and Rosselli, 2017; Striegel-Moore et al., 2008).
We also identified a reasonably large group of patients presenting to primary care with a clinically significant low BMI of ⩽17.5 and a smaller group among them with either (1) no other diagnosis recorded in this encounter or (2) with a related condition that may be indicative of an eating disorder. Unexplained low BMI of 17.5 or less is one of the diagnostic criteria for Anorexia Nervosa in the ICD-10 (World Health Organization, 1992) and should provide practitioners with a prompt to further investigate and screen for this disorder (National Institute for Health and Care Excellence, 2017), particularly when no other cause for low weight is identified. It also provides GPs with an opportunity to become involved in, and promote access to, appropriate care. However, for this to occur, the practitioner must have the necessary knowledge and skills to identify symptoms associated with eating disorders, be aware of indicators of eating disorder (e.g. social withdrawal, particularly from situations that involve food) and have knowledge of eating disorder screening tools appropriate for use in primary care, such as the Sick, Control, One, Fat, Food (SCOFF) or Eating Disorder Examination questionnaires (Hach et al., 2005; Mond et al., 2008; Morgan et al., 2000; National Institute for Health and Care Excellence, 2017).
Overall, we found for encounters where an eating disorder was managed, a referral to a mental health specialist or service was provided in 20% of encounters, a referral to a medical specialist or service was provided in 8% of encounters, and a referral to a nutritionist or dietician was provided in 6% of encounters. Almost two-thirds of people with newly identified eating disorders were provided a referral compared with only half of those with a pre-existing eating disorder. While some patients may not be ready or willing to access specialised care, further efforts to increase referrals should be pursued given the complexity of eating disorders, the availability of effective interventions, best practice recommendations endorsing multidisciplinary care and evidence of improved outcomes with shorter illness duration (Berkman et al., 2007; National Institute for Health and Care Excellence, 2017; Vall and Wade, 2016).
MHTPs provide patients with access to government subsidised mental health services in Australia. In our study, GPs recorded the creation of one of these plans as part of their management of eating disorders at ~4.5% of eating disorder encounters, and overall, MHTPs were used in ~7.7% of encounters to manage mental health issues identified in this group. While this latter figure may not be directly related to eating disorder management, it provides an indication of how many people with an eating disorder are accessing care under the MHTP. It is important for this rate to be increased. This is particularly key as primary care practitioners are the gatekeepers to these services, and in the last 12 months the government has issued an enhanced care plan for eating to promote best practice models of intervention (Australian Government Department of Health, 2019). The limited use of these plans suggests that there may be potential barriers in completing these plans. Barriers may involve knowledge gaps in the identification and screening of eating disorders, limited knowledge of appropriate treatment and referral pathways, time constraints and a relatively high administrative burden in completing plans (Johnston et al., 2007; Linville et al., 2012; Reid et al., 2010). These issues have been identified with similar government subsidised diabetes and chronic disease management plans (Oldroyd et al., 2003). While these types of subsidised services are crucial to improving patient access, without the support and use of primary practitioners, they will fail to achieve their goals. Implementation of strategies that support practitioners to utilise these plans is required. This may include education to improve identification of eating disorders (e.g. symptom recognition and use of screeners), streamlining the referral process and reducing the administrative and time burden to prepare an MHTP. Addressing these barriers and monitoring uptake is crucial to the success of the new 2019 government-funded Eating Disorders Management Plan, which provides subsidised access to psychological services and dietetic services (Australian Government Department of Health, 2019). Without GP support, there is likely to be little change in the rate of uptake of the newly implemented Eating Disorders Plan and, as a result, little change in access to appropriate care for people with eating disorders.
A strength of this study is that the BEACH data is based on rolling nationally representative samples of primary practice that change each year. A further strength is that the detailed data contained in the BEACH study allows us to identify the frequency, interventions and management of eating disorders in the primary care setting, and in particular, the extent to which MHTPs have been used. Future, longitudinal surveillance of patients presenting to primary care with indicators and/or diagnoses of eating disorders will inform early intervention, diagnosis and ongoing care. The study also has a number of limitations. The coding of eating disorders in the BEACH study is based on the ICPC-2 PLUS classification system and does not directly align with existing diagnostic classification systems of eating disorders, such as the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) or ICD-10. While this limits our ability to report on certain diagnostic categories of eating disorders (e.g. Binge-Eating Disorder [DSM-5], atypical anorexia nervosa or bulimia nervosa [ICD-10]), and thus our ability to compare results to other studies, it does provide us with a clear picture of the framework within which eating disorders are defined and classified in primary practice. The cross-sectional nature of the data means that while we can examine how an eating disorder is managed at an individual encounter, it can be difficult to ascertain the full extent of care across a patient’s course of treatment. While a patient may not have received a referral or a GP MHTP at the encounter studied, the patient may have received one at a previous encounter or will receive one on a future encounter. A further limitation of this study is that our estimate of the proportion of the population that had an eating disorder managed in primary care is an upper level estimate as it assumes that each person who had an eating disorder managed only had it managed once by a GP in that same year. However, it is likely that a number of patients had their eating disorder managed more than once that year, with the result that our estimate is likely to be slightly higher than the true estimate. Even with this likely overestimate, the proportion of people having eating disorder managed by GPs in any given year was low.
Overall, this study found less than 0.32% of the population were managed in primary care for a primary or probable eating disorder in any one year. However, our findings suggest that primary care provides an opportunity to improve detection and management of eating disorders, particularly when patients present for ‘other’ issues or with unexplained low BMI and one or more symptoms related to an eating disorder. The study also identified, on average, approximately one-third of people with an eating disorder managed at the encounter were referred to other health practitioners, such as mental health professionals and dieticians, who are fundamental to best practice management of eating disorders. Importantly, mental health plans were used to manage eating disorders in less than 8% of encounters. Identifying and removing barriers to the use of such schemes is crucial to the success of the new government scheme which offers an unprecedented opportunity for patients with eating disorders to access subsidised psychological care and dietetic services and, as a consequence, a unique opportunity to reduce the high levels of morbidity and mortality associated with eating disorders.
Supplemental Material
sj-pdf-1-anp-10.1177_0004867421998752 – Supplemental material for Prevalence and management of people with eating disorders presenting to primary care: A national study
Supplemental material, sj-pdf-1-anp-10.1177_0004867421998752 for Prevalence and management of people with eating disorders presenting to primary care: A national study by Lorraine Ivancic, Sarah Maguire, Jane Miskovic-Wheatley, Christopher Harrison and Natasha Nassar in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We would like to thank Lyn Chiem, Melinda Hardy, Jan Orman, Jan Russell and Karen Spielman who formed our panel of specialist clinicians and generously contributed their time and expertise in identifying signs and symptoms of eating disorders.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was funded by a MRFF/NHMRC Million Minds Mission program grant (APP1178922).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.