
Abstract
Eating disorders have been described as culture-bound syndromes associated with Western or Caucasian societies [1–3] and thought to be rare in Asian and non-Western societies [4, 5], although there iswritten evidence in Western societies of anorexia [6] and bulimia [7] far back in the Medieval period.
However, current research and documents from Asia challenge this culture-bound notion. Research in Asian countries demonstrates that eating disorders do occur in Asian settings. Most articles are from Japan, which has records of anorexia in the twelfth century [8]. Anorexia nervosa and bulimia nervosa are nowconsidered common psychiatric disorders in Japan [8, 9].
Hong Kong is the second most advanced country in Asia in terms of eating disorders research. Most studies have been done by Lee et al. [10–14]. In contrast toWestern research findings, they noticed that bulimia nervosa was rarer than anorexia nervosa in Hong Kong [12].
Thailand has rapidly changed from an agricultural to an industrial society, especially from 1978 to 1988, as shown by the ratio of export goods [15]. In the same period, globalization has brought a culture of thinness from the west, which rapidly spread to Thai adolescents through the daily media [16], with female ideal body image reported to change from being plump to being thin [17].
The changing lifestyles in Thailand may also contribute to the greater emergence of eating disorders, with obesity reported to be a premorbid condition of anorexia nervosa and bulimia nervosa [18]. Importantly, Thai diet has changed from low fat, with a lot of fish and vegetables, to more Western fast food [16], and has been linked to higher rates of obesity [19]. The assertion that urban middle class women, who comprised the current study population, are more likely to be affected by eating disorders comes from a study indicating that while Thai obesity is increasing in urban areas, malnutrition is still prevalent in the rural areas [19].
In Thailand, only seven cases of anorexia nervosa have been reported [16,20–23]. There have been few studies on eating disorders in Thailand, but a couple of two-stage design studies of eating disorders have been published in the Thai language [23, 24]. Kaewpornsawan [24] reported 8.96% of 226 female Thai students aged 12–19 years scored above the diagnostic threshold on a Thai version of the 40-item version of the Eating Attitudes Test (EAT-40). Subsequent diagnostic interviews revealed several subjects with partial eating disorder syndromes. Piyavhatkul et al. [23] validated the Thai General Health Questionnaire-28 in 300 adults from the northeast of Thailand. They reported one case each of anorexia nervosa and bulimia nervosa. Unfortunately, details are not available. Although these results are few and incomplete, they demonstrate that eating disorders do occur in Thailand.
Notwithstanding the limited findings, most recent studies show that Asian girls have unhealthier eating attitudes than Caucasian girls [25–27]. Some studies also reported that Asians living in Western societies had more unhealthy attitudes to eating than Asians in their own countries. British Asian (Pakistani) girls had higher scores on the EAT-26 than Pakistani girls in Pakistan [27]. One Australian study reported that female Hong Kong–born students attending an Australian university and classified as culturally traditional had more disordered eating attitudes than their Australian-born counterparts [28]. However, one British study found no significant differences of eating disorder attitudes between British Asians and British Caucasians [29].
This study aims to compare eating disorders among CaucasianAustralian, AsianAustralian and Thai communities and to examine eating attitudes and psychopathology of 18- to 24-year-old females in a community setting. The final aim is to test the internal reliability of the two screening tests of eating disorders in these groups.
Method
The study is a cross-sectional survey study. Participants were female Caucasian Australian, Asian Australian and Thai university students. Their ages ranged from 18 to 24 years. The measurements consisted of the Eating Attitudes Test (EAT-26), the Eating Disorders Inventory–2 (EDI-2) and the Eating Disorders Inventory–Symptom Checklist (EDI-SC).
Participants
The participants were female university students from The University of Western Australia in Perth, Western Australia, and Srinakharinwirot University from downtown Bangkok, Thailand. The chosen universities are similar to each other in terms of location within the major city, and number of students. The total number of participants was 341, comprising 110 Caucasian Australian, 130 Asian Australian and 101 Thai students.
Approval was obtained from the ethics committees of both universities. Students were recruited by advertising in their class. In the Australian University, letters were sent to heads of departments that had a high proportion of Asian students. Two weeks were allowed for a reply. In the Thai University, letters were sent to the dean of the faculty of education and heads of departments. Four weeks were allowed for a reply. Once the Heads of Departments replied, lecturers advertised the poster of the study in classes asking for volunteers. Letters, consent forms and then questionnaires were sent to volunteer students.
Measures
The Eating Attitudes Test (EAT-26) [30, 31] is a screening test that measures attitudes to eating. It is a 26-item measure that generates a total score and has three subscales: Dieting, Bulimia and Food Preoccupation and Oral control. The EAT-26 items have four score values (0–3). Total scores range from 0 to 78, and a score of ≥20 has been taken to define the first stage of screening for susceptible cases of an eating disorder [31].
The Eating Disorders Inventory–2 (EDI-2 items booklet or EDI-2) [31, 32] is a screening test that measures eating disorder psychopathology. The EDI is a potential screening test to detect young persons at risk of developing eating disorders in the early stages [33] It is a self-rating inventory with 91 items and 11 subscales designed for the assessment of attitudinal and behavioural dimensions relevant to anorexia and bulimia nervosa. Other information collected includes the individual's age, height, current body weight and desired body weight. The EDI-2 items have four score values (0–3). Total scores range from 0 to 273. The suggested cut-off score for diagnostic screening purposes is 14 in the subscale Drive for Thinness.
EDI-SC is a self-report checklist that details the symptoms of eating disorders [32]. These details help the diagnosis of susceptible cases of anorexia nervosa, bulimia nervosa and Eating Disorders Not Otherwise Specified, using the DSM-IV criteria [34].
We used Thai versions of EAT-26, EDI-2 and EDI-SC for the Thai students, which were created by the first author with permission from the copyright holders. All instrumentswere checked with a back-translation [35].
Statistical analysis
The data were analysed using SPSS, in particular descriptive analysis, Kruskal–Wallis test, Spearman's rank–order correlations, χ2 and reliability testing. EAT-26 and EDI-2 data were analysed both as continuous total score and subscale variables, using published cut-offs as categorical variables. As most of the data were not normally distributed, the above non-parametric tests were used. A probability level of 0.05 was used to define significance for all statistical tests.
Results
Participation rates
Of the total of 401 questionnaire sets distributed, 341 sets were completed. The participation rates of Caucasian Australian students and Asian Australian students were 110/150 (71%) and 130/150 (83%), respectively, while the Thai participation rate was 101/101 (100%).
Demographic and physical data
Ethnic group classification was by self-description. Three ethnic groups were identified: Caucasian Australians, Asian Australians and Thais. Some students who identified themselves as Europeans or Eurasians were regrouped, Eurasian as Asian and European as Caucasian.
Most of the fathers' occupations were in the higher ranks, using the Australian Standard Classification of Occupations [36]. Thai fathers' occupations for 27.6% Caucasian Australian, 35.2% Asian Australian and 43.5% were in the manager and administrator ranks. Furthermore, 46.8% of the Caucasian Australians, 36.0% of the Asian Australians and 17.5% of the Thais reported that their fathers' occupations were of the professional rank.
There were differences among the religions of these groups. Most of the Caucasian (55.5%) and Asian (44.6%) students were Christian, while most of the Thai (99%) students were Buddhist.
There were significant differences in the mean ranks of age of the three groups (Tables 1 and 2). Body mass index (BMI=weight (in kilograms)/height2 (in metres)) mean ranks were different among the three ethnic groups. The Caucasian group had the highest mean rank of BMI, Asian Australians an intermediate value and the Thai group the lowest (Tables 1 and 2).
Means (M), standard deviation (SD) and 95% confidence interval (CI) for age, BMI, the EAT-26, the EDI-2 and its subscales in Asian Australian, Caucasian Australian and Thai female university students
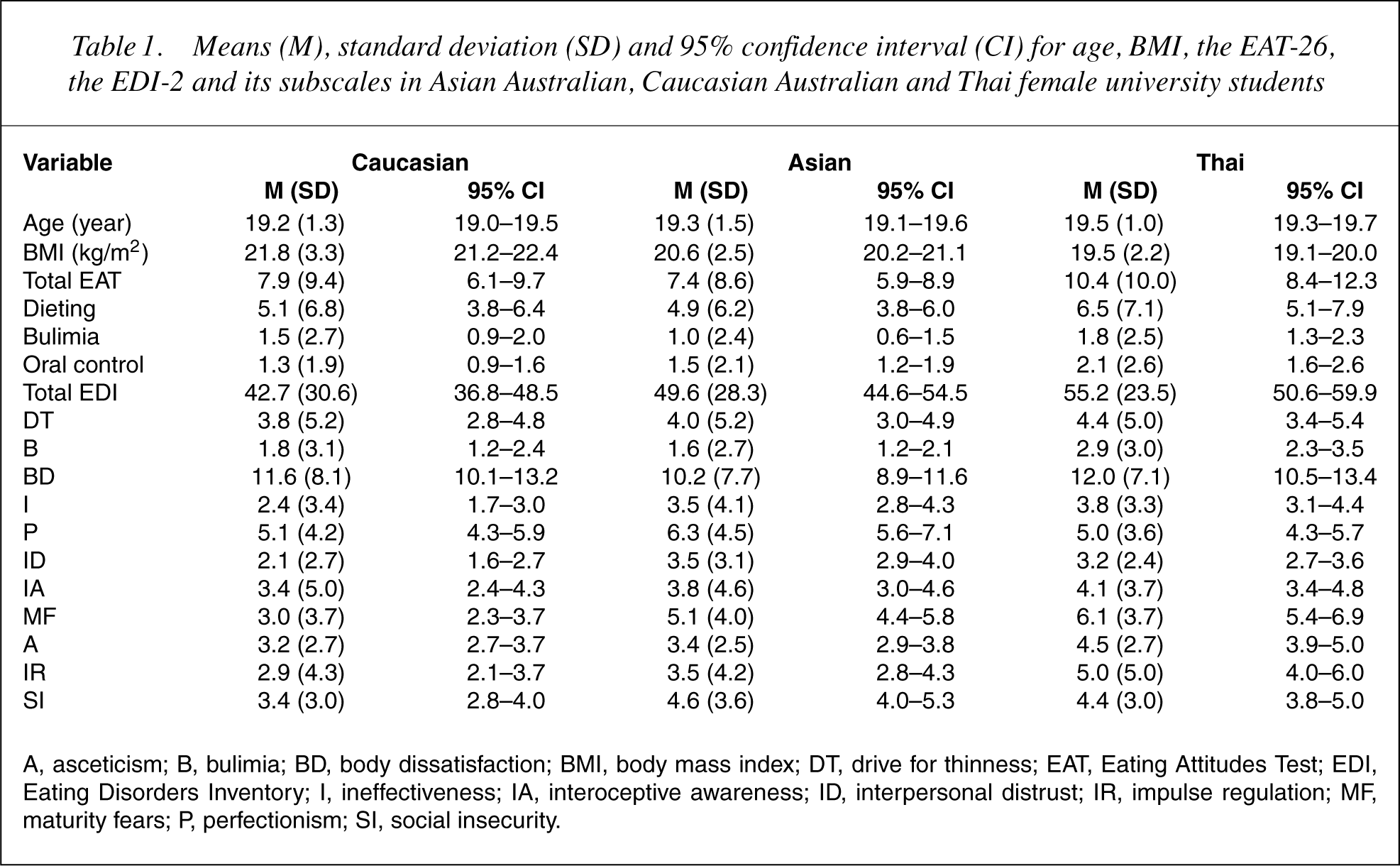
A, asceticism; B, bulimia; BD, body dissatisfaction; BMI, body mass index; DT, drive for thinness; EAT, Eating Attitudes Test; EDI, Eating Disorders Inventory; I, ineffectiveness; IA, interoceptive awareness; ID, interpersonal distrust; IR, impulse regulation; MF, maturity fears; P, perfectionism; SI, social insecurity.
Kruskal–Wallis (K-W) χ2, probability values (of being the same), significant result from K-W test and significant result from Mann–Whitney (M-W) test of the age, BMI, EAT-26, EDI-2 and its subscales for Asian Australian, Caucasian Australian and Thai female university students
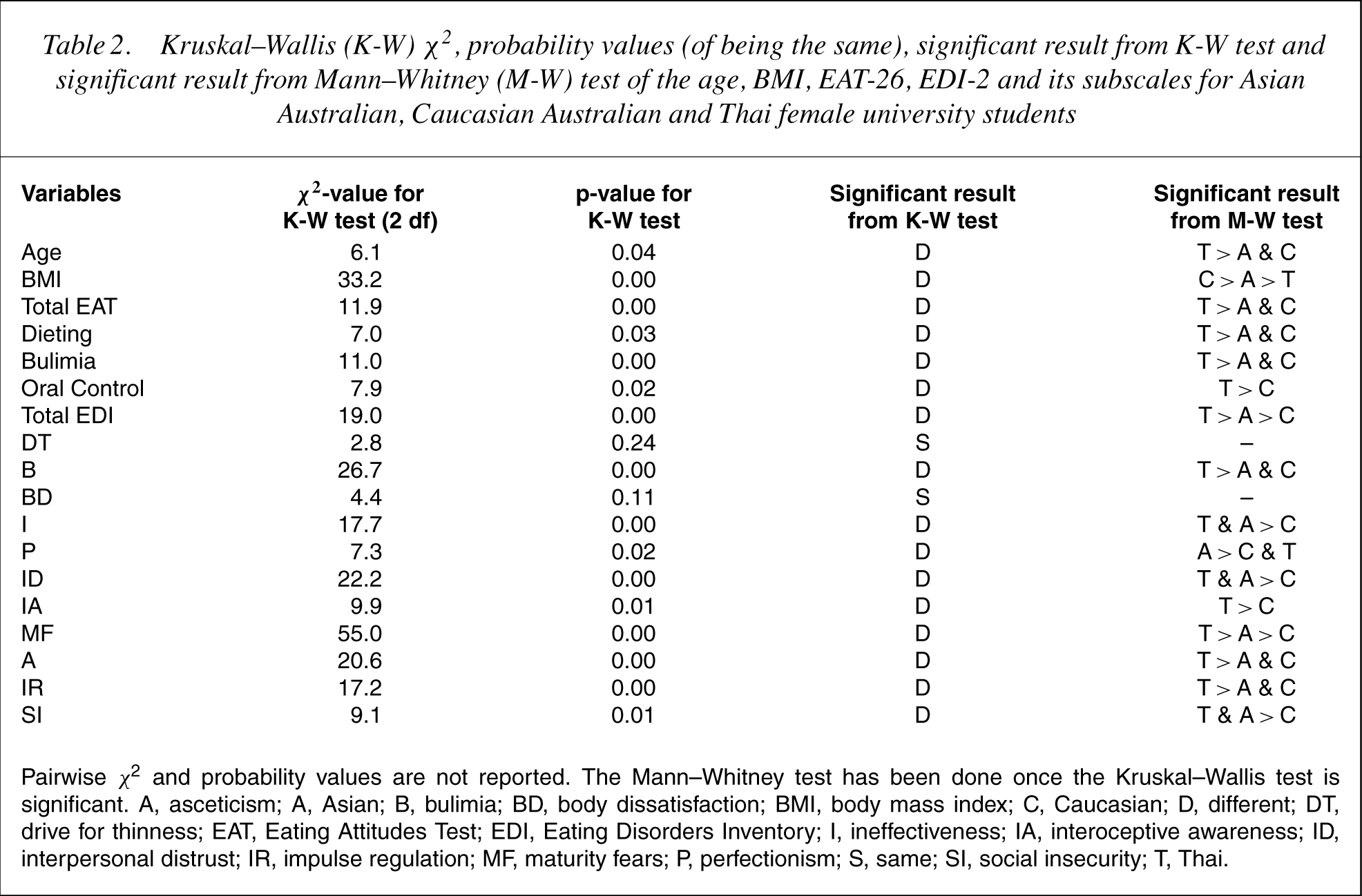
Pairwise χ2 and probability values are not reported. The Mann–Whitney test has been done once the Kruskal–Wallis test is significant. A, asceticism; A, Asian; B, bulimia; BD, body dissatisfaction; BMI, body mass index; C, Caucasian; D, different; DT, drive for thinness; EAT, Eating Attitudes Test; EDI, Eating Disorders Inventory; I, ineffectiveness; IA, interoceptive awareness; ID, interpersonal distrust; IR, impulse regulation; MF, maturity fears; P, perfectionism; S, same; SI, social insecurity; T, Thai.
Comparison of the eating disorder attitudes and psychopathology
Attitudes
Attitudes to eating were found to be different among the three ethnic groups, in that mean rank of total scores for the EAT-26 (Total EAT) and its subscales were significantly higher for the Thai group (Tables 1 and 2).
Psychopathology
Eating disorder psychopathology scores were different among the three ethnic groups (Tables 1 and 2). The Kruskal–Wallis test revealed a significant group difference in the mean rank of total EDI-2 scores (Total EDI), with the Thai group having a higher mean rank than the Asian Australian group, which in turn had a higher mean rank than the Caucasian group.
The Thai group mean ranks were significantly higher than the other two groups' in the Bulimia (B), Maturity Fears (MF), Asceticism (A) and Impulse Regulation (IR) subscales (Tables 1 and 2). The Asian Australian and Thai groups had higher mean ranks than the Caucasian Australian group in the Ineffectiveness (I), Interpersonal Distrust (ID), Maturity Fears (MF) and Social Insecurity (SI) subscales. The Asian group had higher mean rank than the other two groups in Perfectionism (P) subscale.
Reliability testing
The internal consistencies of the three groups were excellent [37], with Cronbach's alphas for the EAT-26 ranging from 0.87 to 0.89 and the EDI-2 ranging from 0.90 to 0.93.
Convergent validity
A significant good-to-excellent correlation existed between subscale Dieting of EAT-26 and subscale Drive for Thinness of EDI-2 (Caucasian r=0.76, Asian r=0.74 and Thai r=0.82). A significant positive moderate relationship also existed between Total EAT and Total EDI for all groups (Caucasian r=0.63, Asian r=0.67, Thai r=0.55).
Relationship between age, BMI and eating disorder attitudes and psychopathology
Age had a fair but significant negative correlation to eating disorder attitudes (r=−0.43 Total EAT) and psychopathology (r= −0.36 Total EDI) only in the Caucasian group. That is, the younger they are, the unhealthier their eating disorder attitudes and psychopathology. BMI had a small but significant positive correlation on eating disorder psychopathology scores as measured by the Total EDI in the Asian Australian (r=0.22) and Thai (r=0.41) groups. The heavier they are, the higher their eating disorder psychopathology scores. Only the Thai group has a significant correlation between BMI and Total EAT (r=0.42).
Susceptible cases
Similar numbers of students in each group were susceptible to eating disorders. Using published cut-off scores of the EAT-26 and the EDI-2 to create categorical variables, 10.0% (11/110) of Caucasian students were identified as susceptible to an eating disorder (4 EAT-26 only; 2 EDI-2 only; 5 both). This percentage was similar to that of Asian Australians at 11.3% (15/130; 2 EAT-26 only; 6 EDI-2 only; 7 both) and the Thai group at 14.9% (15/101; 5 EAT-26 only; 2 EDI-2 only; 8 both). There were no significant differences among the three groups, using χ2 analysis. Checking these cases against their EDI-SC records, showed a total of 7, 6 and 10 cases with symptoms in the Caucasian Australian, Asian Australian and Thai groups, respectively.
Discussion
While many published studies have reported on eating disorders inWestern Caucasian populations, little research has focused on Asian populations [25, 38, 39], with even less comparing eating disorders among Asians and Caucasians. The current research is therefore significant in that it not only compares these two populations but also looks at the role of Western acculturation on Asian populations and eating disorders.
The major study finding was that students in Thailand had higher disordered eating attitudes and eating disorder psychopathology scores than either Asian Australian or Caucasian Australian students. With respect to the Thai and Caucasian Australian students, this finding is similar to that of previous research indicating that female university students in India scored significantly higher than their counterparts in Australia [26].
That the Thai group had the highest scores in susceptibility to developing an eating disorder and eating disorder psychopathology may be partially explained in sociocultural terms, with pressure to be thin more extreme in Thailand than in Australia.
In the current study, the Thai university students came from the urban middle class, a group that would be more exposed and arguably more affected by globalization and introduction of Western advertising. This assertion is consistent with the report that Thai women are not only under the influence of western culture to be thin but also under the influence of traditional Thai culture to be beautiful in order to hold men's attention and maintain their status [40].
It could also be argued that young women in western cultures having been exposed to advertising over a longer period are less affected. This is supported by a study of Sharps and colleagues (2001), which reported that young Thai females in rural Thailand exhibited preferences for figures to be thin because of western influence, and these preferences were greater than those held by their American counterparts [41].
Thai and Caucasian Australians
Study results indicated that the Thai group had unhealthier eating disorder attitudes and psychopathology than the Caucasian group. This is consistent with the finding that there was a difference in eating disorder attitudes between Indians and Caucasians of comparable socioeconomic class in [26]. This suggests that in Thailand, the eating attitudes and psychopathology may be more affected by multifactors including traditional values of beauty [40], western culture of thinness [41] and culture clash [42] due to conditions of rapid economic and sociocultural change.
Thailand is a developing country, which was caught in the dilemma of fast economic growth and then a sudden crash in 1997 [43, 44]. The Asian economic crisis had severe social impact on Thailand and other Asian countries [45], especially on the new middle class, from where most Thai and Asian students come. Socioeconomic insecurity may cause family crisis and individual anxiety, which may enhance social insecurity. Both the Thai and Asian groups had higher scores on Social Insecurity.
Thais and Asian Australians
The Thais and Asian Australians both had significantly higher scores than Caucasian Australians on the eating disorder psychopathology subscales of Ineffectiveness, Interpersonal Distrust, Maturity Fears and Social Insecurity. This finding is similar to that of the study of Lee et al. [14], and might reflect the nature of Asian female students, who have a tendency to have overprotective parents, less encouragement toward independent values and more conflict with their parents due to cultural change compared with the Caucasian students [9, 27, 46].
The differences noted above were not associated with significant differences in the number of susceptible cases. This is similar to a phenomenon noted by Weisz et al. [47], where different cultures seem to have a similar prevalence of symptoms of child behaviour problems, but the measured psychopathology of the symptoms varies with the culture.
Asian Australians and perfectionism
Asian Australians had a higher level of perfectionism than the other two groups. This trait is similar to a finding of high perfectionism in an Asian group as a result of parents' higher expectations, especially academic expectations [48].
The similarities of eating attitudes (EAT-26) of the Asian Australians and Caucasian Australians contrast with a study of Asians and Caucasians in Britain, and Pakistanis in a Pakistan University students [27]. In Mujtaba's study [27], the British Asian group had the highestmean susceptibility to developing an eating disorder, followed by the Pakistani group, while the Caucasian British group had the lowest.
The between-groupBMIdifferences are consistent with other research. Ko and Cohen [49] found their Korean American sample to have higher BMI than their Korean group in Korea. This result is similar to that of a study comparing Pakistanis, British Asians and Whites [27]. There may be other explanations for the BMI differences than eating disorders: there may be genetic differences in ethnic morphology, or differences in diet and nutrition [50–52].
Finally, the proportion of Thai students above the cutoffs in both EAT-26 and EDI-2 is 8/101 (7.9%) is similar to that reported by Kaewpornsawan (8.96%) [24].
Study limitations
There are a number of limitations in this study. First, the measures used in the EAT and EDI were developed for eating disorders in Western societies. Where culture plays an important part in the psychopathology being measured, an instrument developed in one culture may not measure the same thing in another culture. Even though there was a careful translation into Thai and a back-translation check, some questions in this study may have been misunderstood when used to screen for eating disorders in Thailand, or have different meanings to participants in different cultural contexts. Furthermore, cut-off scores for the Thai population have not been validated against a clinical standard. Notwithstanding this limitation, the Thai group in the current study had the highest scores on all three instruments used, indicating consistency. Past research has demonstrated that both the EAT and EDI have suitable psychometric properties for research purposes [53]. This is consistent with the internal consistency of this sample. The convergent validity [54] also showed that the EDI-2 was valid and agreed with EAT-26 in screening eating disorders. Second, the study relied on volunteers and self-report measures. In the current study, the participation rate was highest in the Thai students, lowest in Caucasian students and intermediate in Asian Australian students. This is consistent with the Asian ethnic tendency to comply with perceived authority [55, 56]. While this was not unexpected, the disproportionate participation from each group and selfreport measures may have resulted in some bias.
Future directions
The study indicates that eating disorders are not limited toWestern societies, and thatWestern influences may be associated with the rise of eating-related psychopathology in Asian countries. Future research should investigate the degree of Asian ethnic identity and Western acculturation and eating disorder attitudes and psychopathology. Work on instrument validity, including factor analysis, to examine the item endorsement is required, as are measures of malnutrition and eating disorders clinical diagnoses in Asian and Thai samples.
It is hoped that the findings of this research will alert the Thai medical world to attend to the emergence of eating disorders in Thailand.
Footnotes
Acknowledgements
We are grateful to Tossaporn Prasertsuk for data collection in Thailand and to Dominique Blache and Anh-Van Pham for their advice.