
Abstract
Objective:
Few population-based studies have been used to investigate secular trends in psychotropic medication use. Therefore, the aim of this study was to examine psychotropic medication use over time using data from the Geelong Osteoporosis Study, an on-going, population-based, cohort study of Australian women.
Methods:
Of the 1494 women recruited at Time 1 (1993–1997), self-reported medication use from Time 2 (2004–2008) and/or Time 3 (2011–2014) was available for 889 women. Prevalence of antidepressant/antipsychotic/anxiolytic/sedative/anticonvulsant use by age and cohort strata was calculated using bootstrapping methods. Simultaneous age-cohort patterns were evaluated using logistic regression techniques.
Results:
The prevalence of any psychotropic medication use increased from 8.0% (95% confidence interval = [6.3, 9.8]) at Time 1 to 26.0% (95% confidence interval = [22.4, 29.4]) at Time 3, translating to a 4.3-fold increase in the likelihood of psychotropic medication use over the study period (odds ratio = 4.3, 95% confidence interval = [3.2, 5.8], p < 0.001). This increase was driven by the use of antidepressants (odds ratio = 6.4, 95% confidence interval = [4.2, 9.5], p < 0.001) and anticonvulsants (odds ratio = 4.4, 95% confidence interval = [1.8, 11.1]) and modest increases in the use of anxiolytic agents (odds ratio = 1.9, 95% confidence interval = [1.1, 3.1]) and sedatives (odds ratio = 1.7, 95% confidence interval = [1.6, 1.9]). The prevalence of any psychotropic medication use increased with increasing age (40–59.9 years: odds ratio = 1.9, 95% confidence interval = [1.5, 2.6]; 60–79.9 years: odds ratio = 2.6, 95% confidence interval = [1.9, 3.5], compared to the 20- to 39.9-year group). Use of selective serotonin reuptake inhibitors increased dramatically over the study period (odds ratio = 15.3, 95% confidence interval = [7.0, 33.4]).
Conclusion:
Use of psychotropic medication has increased substantially over the past two decades, especially among older women. Further investigations into the correlates and outcomes of the increased use of psychotropic medications are warranted.
Introduction
Mood and anxiety disorders are highly prevalent, with recent studies reporting that up to one in three Australian women suffer from a mood or anxiety disorder in their lifetime (Williams et al., 2010). A focus on developing mental health policies and programmes at the Australian government level has seen the introduction of initiatives such as beyondblue and Better Outcomes in Mental Health Care, which aim to improve community awareness, reduce stigma surrounding mental illness, improve patient access to mental health care and provide education and training for general practitioners. Coinciding with the potentially increasing prevalence and increased government-level focus on mental health is the introduction of new psychotropic medications to the Australian Pharmaceutical Benefits Scheme (PBS). Notwithstanding these initiatives, prevalence rates are either stable or rising, raising important public health questions (Jorm, 2014; Jorm and Reavley, 2012).
Seemingly concordant with these developments in Australia, McManus et al. (2000) reported a marked increase in the use of antidepressants in the 1990s using prescription dispensing data. More recently, using data from the Drug Utilisation Sub-Committee of the Australian Department of Health and Ageing, Stephenson et al. (2013) reported a 58% increase in the dispensing of psychotropic drugs between 2000 and 2011. This increase was propelled by the 95.3% increase in antidepressant use, with selective serotonin reuptake inhibitor (SSRI) use alone doubling between 2000 and 2011. This is supported by PBS data showing a 41% increase in antidepressant use between 2002 and 2007 (Hollingworth et al., 2010a).
Similar secular trends have been reported worldwide using prescriptions data, with marked increases in psychotropic medication dispensed in England (Ilyas and Moncrieff, 2012) and, in particular, increased dispensing of antidepressants shown in the United States (Chen et al., 2008), Canada (Smith et al., 2008) and New Zealand (Exeter et al., 2009). The number of prescriptions for antipsychotics also appear to be on the rise (Alexander et al., 2011; Hollingworth et al., 2010b; Ilyas and Moncrieff, 2012; Stephenson et al., 2013; Verdoux et al., 2010), although not all studies report a change (Paulose-Ram et al., 2007). In contrast, sedative and anxiolytic use appears to be relatively stable (Ilyas and Moncrieff, 2012; Paulose-Ram et al., 2007; Stephenson et al., 2013), although not all studies agree (Hollingworth and Siskind, 2010; Islam et al., 2014); Hollingworth et al. describe a decrease in the total number of prescriptions for benzodiazepines by one-quarter over a 20-year period.
To date, studies have reported prescription data using pharmacy sales, prescription databases or general practice data to investigate trends in psychotropic medication use. Few studies have utilised population-based samples to observe psychotropic medication use over time, with those who have, only able to describe differences between estimates based on cross-sectional analyses of different individuals. In the United States, Paulose-Ram et al. (2007) utilised two waves of the National Health and Nutrition Examination Surveys (NHANES) to report a threefold increase in antidepressant use between 1988–1994 and 1999–2002; Motjabi and colleagues (Mojtabai, 2008) reported a fourfold increase in antidepressant treatment using the US National Comorbidity Survey (1990–1992) and its replication (2001–2003); and Zuvekas (2005) and Olfson and Marcus (2009) reported rapid increases in antidepressant treatment using the Medical Expenditure Panel Surveys (MEPS). Han et al. (2016) also reported an increase in psychotropic medication use without co-occurring inpatient or outpatient treatment between 2008 and 2013.
In order to control for changing demographic profiles within cohorts, it is useful to examine a stable cohort over time. To our knowledge, this is the first study to interrogate longitudinal data using the same population over more than a decade. Using data from the Geelong Osteoporosis Study (GOS), a population-based, prospective cohort study of women residing in South Eastern Australia, we aim to examine secular trends and age-related differences in the prevalence of psychotropic medication use over time using a longitudinal model that accounts for simultaneous age-cohort affects.
Methods
Participants
This study utilised data collected from women participating in the GOS, an age-stratified, population-based sample of women residing in the Barwon Statistical Division located in South Eastern Australia. A comprehensive description of GOS, including details pertaining to recruitment, attrition and data collected at each follow-up phase, has been published elsewhere (Pasco et al., 2012). Briefly, women were randomly selected from the Australian Electoral Commission (AEC) rolls for the Barwon Statistical Division between 1993 and 1997 and followed at regular intervals for over 15 years.
This study explores trends in medication use using data collected at three time points. Of the 1494 women who completed a baseline GOS appointment (Time 1, 1993–1997), medication data from the 10-year (Time 2, 2004–2008) and/or 15-year follow-up (Time 3, 2011–2014) were available for 889 women (59.5% original cohort) aged between 20 and 80 years. This study was approved by the Barwon Health Human Research and Ethics Committee, and written informed consent was obtained from all participants.
Medication use
Trained research personnel documented medication use by questionnaire during the study interviews. Participants were required to list all current medications, including prescription medications, vitamins, minerals, herbs and digestive aids. To ensure accurate recording of data, participants were encouraged to bring medication containers, scripts or lists. Medications were coded according to the classification system of MIMS pharmaceutical database (MIMS Australia Pty Ltd, 2015). The psychotropic medications of interest included sedatives; hypnotics (benzodiazepines used in insomnia, imidazopyridine hypnotic agents, cyclopyrrolone hypnotic agents, ethanolamine antihistamines and melatonin receptor agonists); antianxiety agents (benzodiazepines used in anxiety treatment); antipsychotic agents (atypical antipsychotics, benzamide neuroleptics, benzamide antipsychotics, indole derivative antipsychotics, carboxamide antiepileptics, phenothiazine antipsychotics, thioxanthene neuroleptics, butyrophenone neuroleptic); antidepressants (serotonin noradrenaline reuptake inhibitors [SNRIs], SSRIs, tricyclic antidepressants [TCAs], monoamine oxidase inhibitors, noradrenergic and specific serotonergic antidepressants and reversible inhibitors of monoamine oxidase A); and anticonvulsants (substituted asymmetric triazine antiepileptics, antiepileptics, monosaccharide antiepileptic and carboxamide antiepileptics). Antidepressants were sub-classified into (1) SNRIs – desvenlafaxine, duloxetine, venlafaxine; (2) SSRIs – citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline; (3) TCAs – amitriptyline, clomipramine, dothiepin, doxepin, imipramine, nortriptyline, trimipramine; and (4) ‘other’ – nianserin, mirtazapine, moclobemide, phenelzine, tranylcypromine, reboxetine.
Statistical analyses
Prevalence of psychotropic medication use (antidepressants, antipsychotics, anxiolytics, sedatives or anticonvulsants) for the study population was reported, and 95% confidence intervals (CI) were calculated using bootstrapping methods. Chi-square test was used for bivariate comparison of medication use. Age (time-varying age groups: 20–39.9, 40–59.9, 60–79.9 years) and longitudinal cohort effects (Time 1, Time 2, and Time 3) were evaluated using logistic regression techniques that account for within-individual participants’ autocorrelation. Odds ratio (OR) and 95% CI were reported. Statistical analyses were performed using SPSS Statistics for Windows (version 22; IBM Corp, Armonk, NY).
Results
Baseline characteristics of the study sample can be seen in Table 1. Over the course of the study, 258 of the 889 (29%, 95% CI = [26.1, 32.1]) women used at least one psychotropic medication at one or more time points across the study period. Among psychotropic medication users, the proportion of women who used medications from multiple psychotropic medication categories remained stable across the study period – Time 1: 22.5% (16/71, 95% CI = [13.5, 34.0]), Time 2: 23.6% (38/161, 95% CI = [17.3, 30.9]) and Time 3: 17.7% [31/175, 95% CI = [12.3, 24.2]), p = 0.39.
Baseline characteristics of participants.
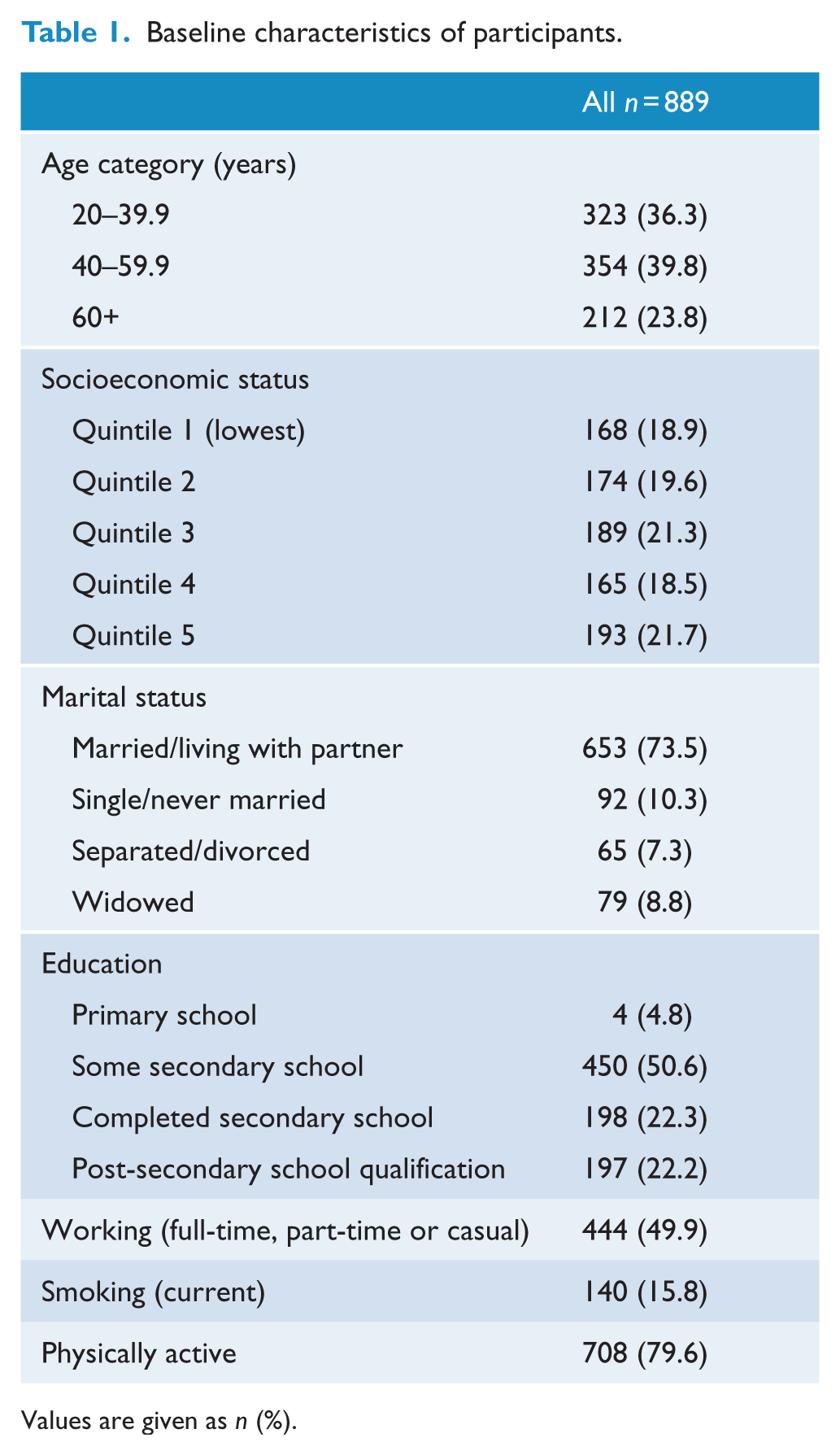
Values are given as n (%).
Unadjusted cohort trend: pattern of psychotropic use over time
The prevalence of any psychotropic medication use increased from 8.0% (95% CI = [6.3, 9.8]) at Time 1 to 18.8% (95% CI = 16.2, 21.4) at Time 2 and 26.0% (95% CI = [22.4, 29.4]) at Time 3, translating to a 4.3-fold increase in the likelihood of psychotropic medication use over the study period (p < 0.001, Table 2). This increase was driven by a marked increase in antidepressant (OR = 6.4, 95% CI = [4.2, 9.5], p < 0.001) and anticonvulsant use (OR = 4.4, 95% CI = [1.8, 11.1], p = 0.001) and a modest increase in anxiolytic (OR = 1.9, 95% CI = [1.1, 3.1], p = 0.02) and sedative use (OR = 1.7, 95% CI = [1.6, 1.9], p < 0.001) between Time 1 and Time 3. No changes were seen in antipsychotic use across the study period – Time 1: 0.8% (95% CI = [0.2, 1.3]), Time 2: 1.1% (95% CI = [0.5, 1.8]) and Time 3: 1.3% (95% CI = [0.6, 2.2]), p > 0.05. Figure 1 demonstrates the increase in antidepressant use compared to the other psychotropic medication categories across the study period.
Longitudinal age-cohort models for each of the medication categories according to age and time point.
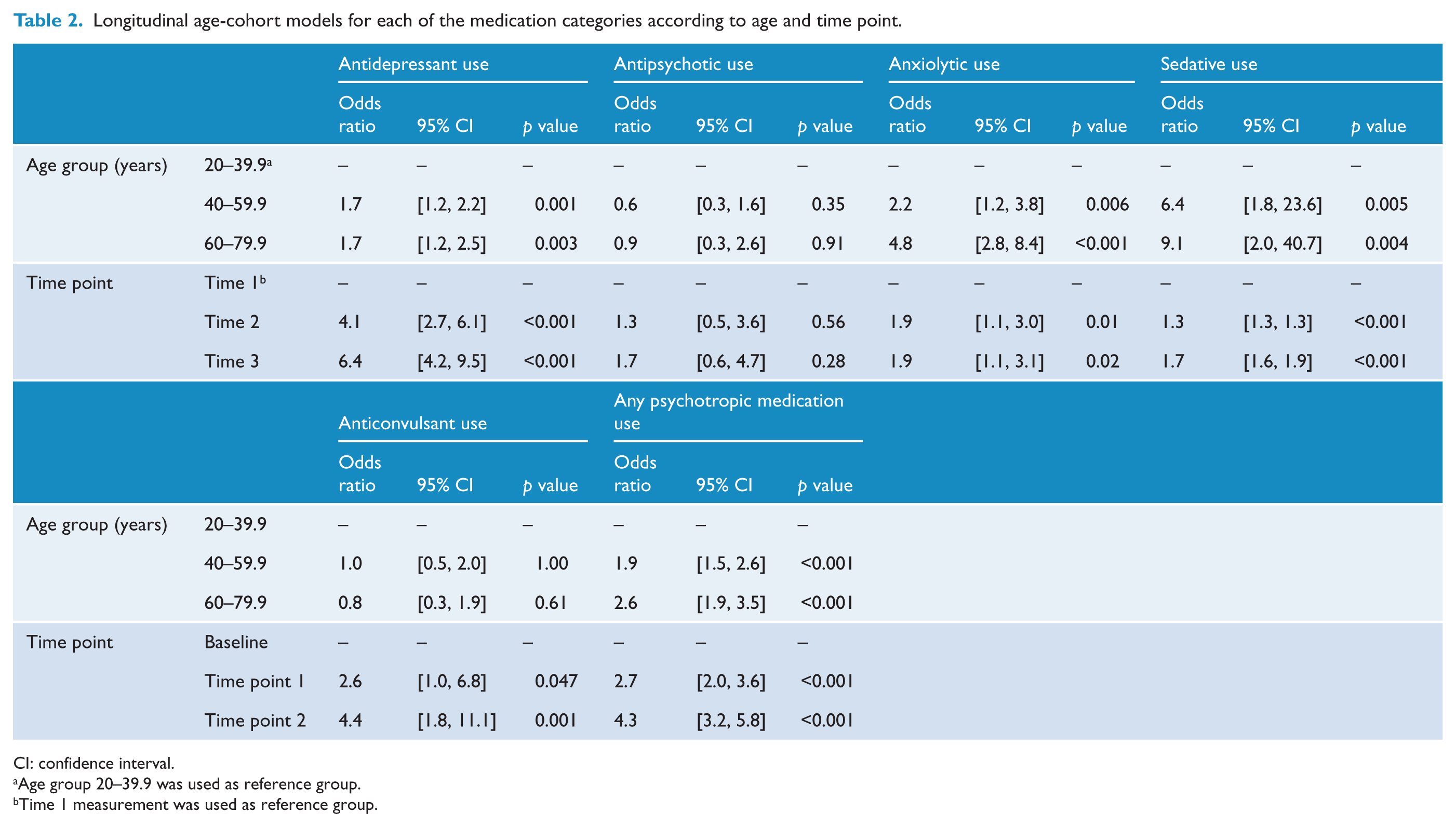
CI: confidence interval.
Age group 20–39.9 was used as reference group.
Time 1 measurement was used as reference group.
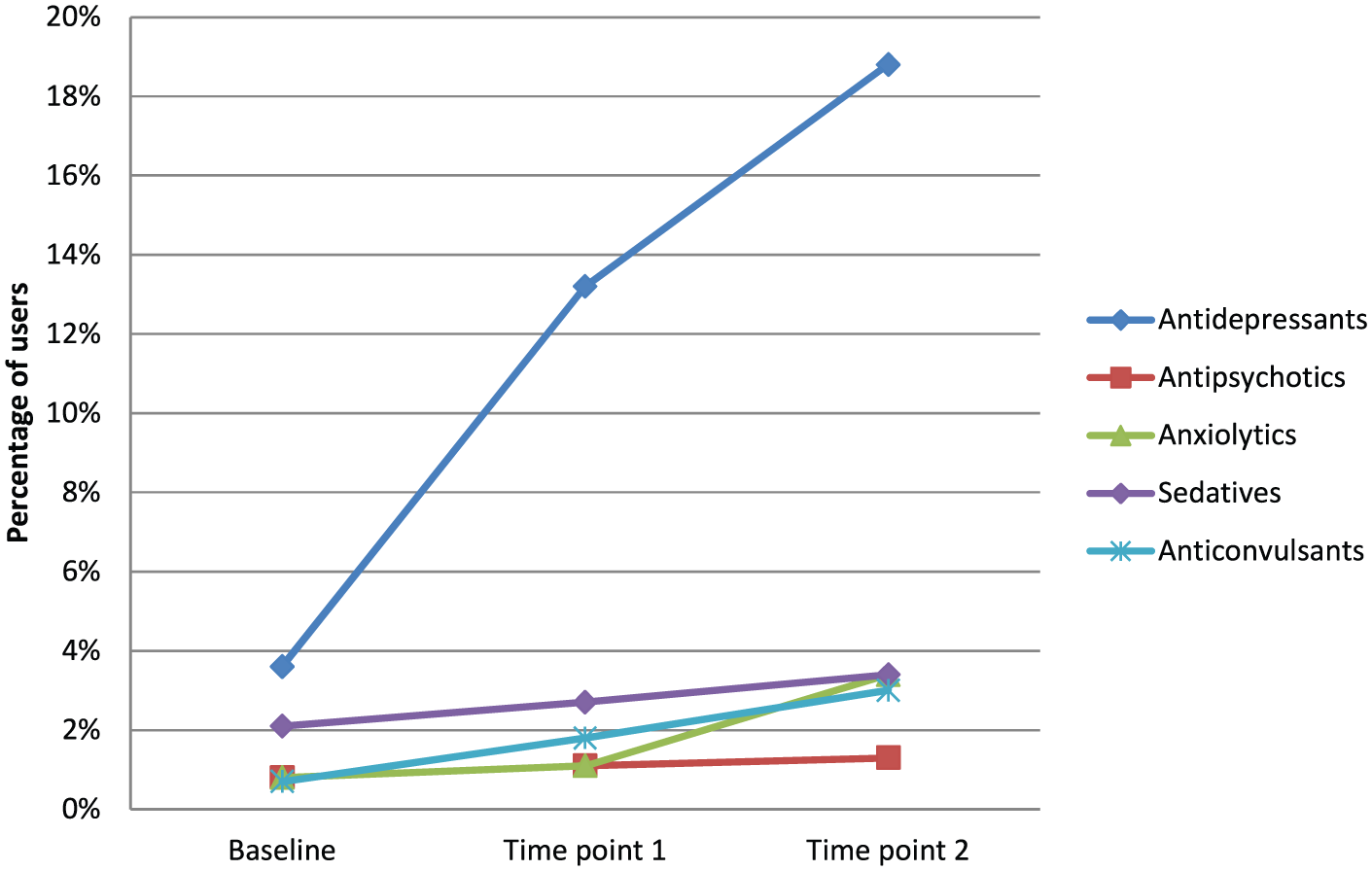
Prevalence of use of the five psychotropic medication categories at each time point.
Unadjusted age effect: pattern of psychotropic use by age
The prevalence of any psychotropic medication use increased with advancing age (Table 2). This pattern was also seen for anxiolytic use and sedative use. With regard to antidepressant use, there was a 1.7-fold increase in usage for both the 40- to 59.9-year and 60- to 79.9-year age groups, compared to the 20- to 39.9-year age group. There were no age effects seen for anticonvulsant or antipsychotic use (see Figure 2).
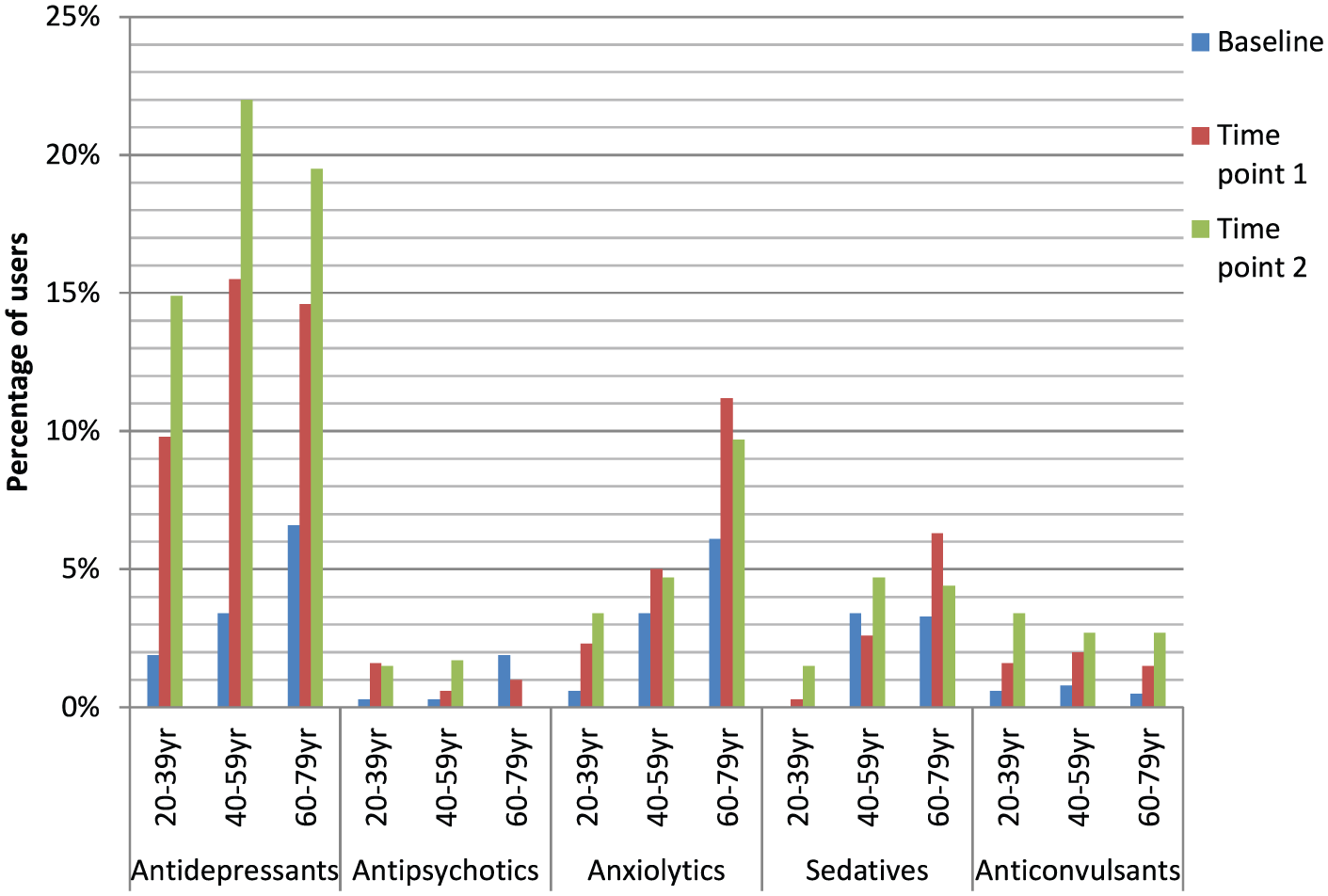
Prevalence of use of the five psychotropic medication categories at each time point, displayed in age categories.
Regarding subcategories of antidepressants, TCAs were the most commonly used antidepressant at Time 1 ([23/33] 69.7%), whereas SSRIs were the most commonly used antidepressant at Time 2 ([55/113] 48.7%] and Time 3 ([74/127] 58.3%] (see Figure 3). The greatest increase was seen for the use of SSRIs, which increased 8-fold by Time 2 (OR = 8.7, 95% CI = [3.9, 19.1], p < 0.001; Table 3) and 15-fold at Time 3 (OR = 15.3, 95% CI = [7.0, 33.4], p < 0.001); this was accompanied by a 1.8-fold increase in TCA use between Time 1 and Time 3 (OR = 1.8, 95% CI = [1.0, 3.2], p = 0.03). Use of other antidepressants increased threefold at Time 2 (OR = 3.4, 95% CI = [1.1, 10.5], p = 0.048), but this change was not sustained at Time 3. There were no SNRI users at Time 1; no cohort effects were seen for SNRI use between Time 2 and Time 3. The older age group was more likely to use TCAs compared to those aged below 40 years (OR = 2.9, 95% CI = [1.6, 5.2], p < 0.001); there were no other significant age effects.
Longitudinal age-cohort models for the antidepressant categories according to age and time point.
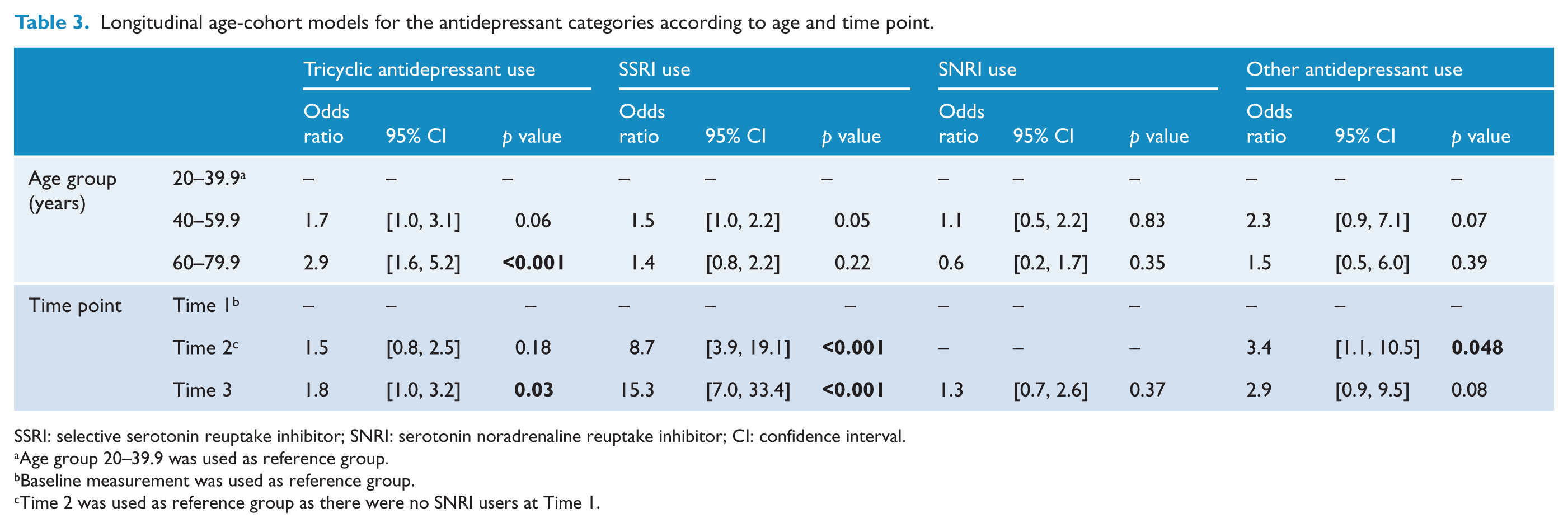
SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin noradrenaline reuptake inhibitor; CI: confidence interval.
Age group 20–39.9 was used as reference group.
Baseline measurement was used as reference group.
Time 2 was used as reference group as there were no SNRI users at Time 1.
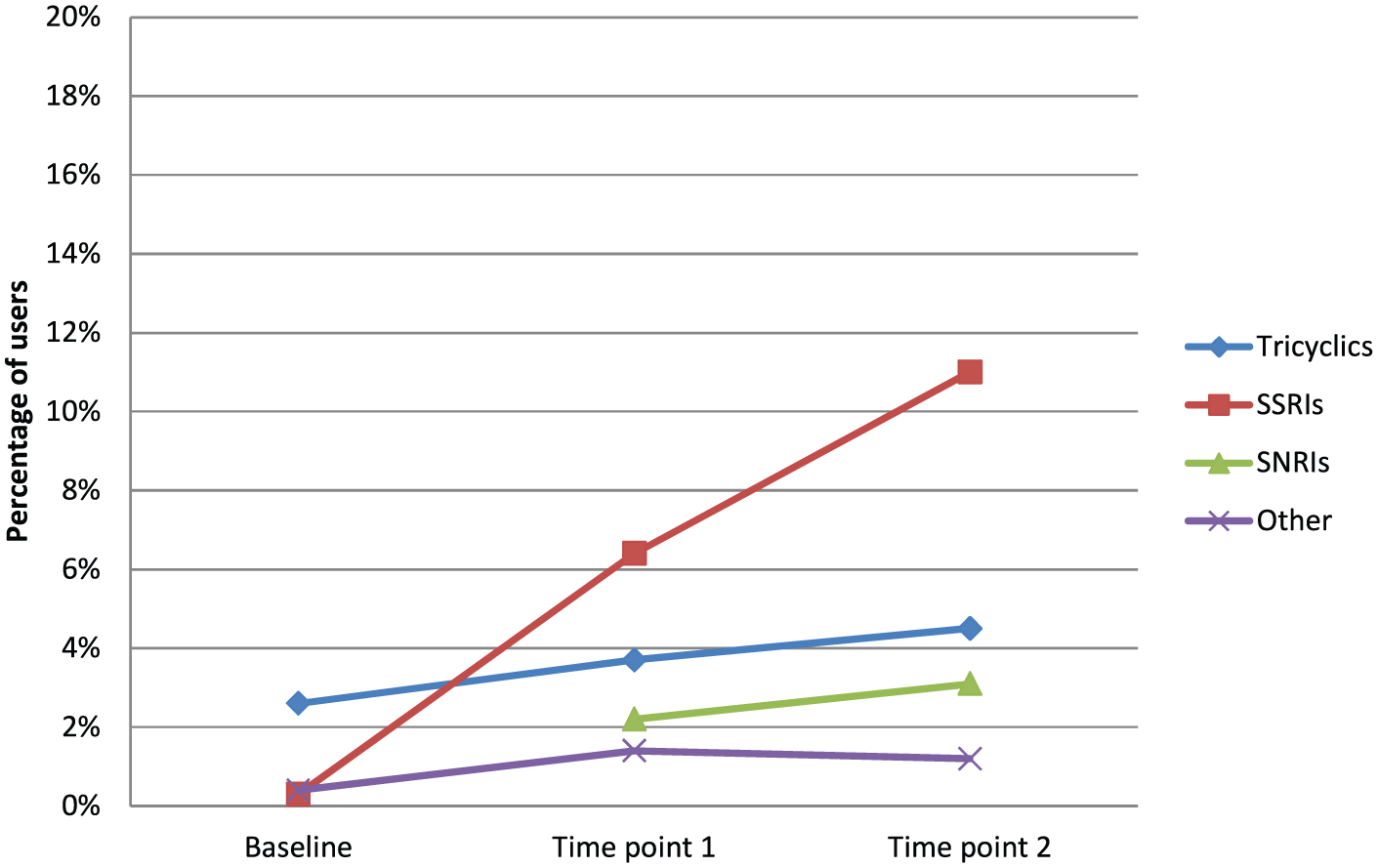
Prevalence of use of four antidepressant medication categories at each time point.
Discussion
Driven by reports of a substantial global increase in antidepressant and anticonvulsant use, we report that the prevalence of psychotropic medication use has increased fourfold in this prospective cohort over the past two decades. The results of this study support previous literature using prescription and physician databases (Hollingworth et al., 2010a; Ilyas and Moncrieff, 2012; McManus et al., 2000; Stephenson et al., 2013) and US nationally representative surveys (Han et al., 2016; Mojtabai, 2008; Paulose-Ram et al., 2007; Olfson and Marcus, 2009; Zuvekas, 2005). To our knowledge, this is the first study to investigate secular trends in psychotropic medication use in a population-based sample followed for almost 20 years.
Our results are concordant with those described by Paulose-Ram et al. (2007) who utilised two of the US NHANES to describe secular trends in psychotropic medication use. In both NHANES studies and this study, the use of any psychotropic medication was highest among those aged 60+ years, compared to those below 40 years. Olfson and Marcus (2009) also reported highest psychotropic medication use among those aged 50+ years, and Han et al. (2016) reported highest use in the Baby Boomers group. These age trends have also been shown in antidepressant use (Exeter et al., 2009; Hollingworth et al., 2010a); however, this study showed a consistent 1.7-fold increase in the odds of antidepressants use for both the 40–59 and 60+ year age groups, compared to the younger group.
Akin to other studies, we found SSRIs were the most commonly used antidepressant during the 20th century, with increasing prevalence of users over time (Chen et al., 2008; Exeter et al., 2009; Smith et al., 2008; Stephenson et al., 2013). Interestingly, we found tricyclic use modestly increased over time in this study, whereas others have reported a corresponding decrease in tricyclic use with the increasing SSRI use (Chen et al., 2008; Exeter et al., 2009; Stephenson et al., 2013; Zuvekas, 2005). This study also confirmed findings of increased TCA use with increasing age reported by Exeter et al. (2009); we found that those aged over 60s are three times more likely to use tricyclics than their younger counterparts. Although not examined in this study, we speculate that the length of use of tricyclics may be a factor for those aged over 60, with individuals hesitant to switch medications once proven efficacious.
In contrast to other studies (Verdoux et al., 2010), the prevalence of antipsychotic medication use did not increase across our study period. We suspect this is could be due to the potentially low prevalence of people with psychotic disorders in this cohort, and perhaps due to the nature of the reason for prescription whereby those taking antipsychotics may not be well enough to attend the study centre, the widespread off-label use of these agents for non-psychotic disorders notwithstanding. Atypical antipsychotic medications, in particular, have become more commonly used in the treatment of bipolar disorder, depression, anxiety, attention deficit hyperactivity disorder and dementia (Alexander et al., 2011). Small numbers of antipsychotic users in this sample did not allow for exploration of treatment indication.
The use of medications from multiple psychotropic medication categories remained stable across time in this study. Mojtabai and Olfson (2010) reported an increase in the combination of antidepressants and antipsychotics but no other combination of psychotropic medication categories between 1996–1997 and 2005–2006. Given participants need to be well enough to attend the study centre for each follow-up assessment, the health of this sample may have contributed to the lack of findings in this area.
Major strengths of this study include the population-based design, face-to-face interview protocol and the longitudinal study nature allowing for observation of the same individuals across two decades. Notwithstanding these strengths, the results of this study should be interpreted with the following limitations in mind. First, using self-reported medication data has its advantages and disadvantages; although self-report data can be reliant on memory recall, prescription data do not account for scripts that are dispensed but not ingested or medications prescribed while in hospital as a patient. Second, the medication use profile of GOS participants may have differed from non-participants and those lost to follow-up. As such, the increase in psychotropic medication use may have been under-estimated. Finally, small numbers of medication users in the subcategories (with the exception of antidepressants) prevented further investigations in the patterns of use over time.
The cause of this dramatic increase observed in the use of antidepressants and psychotropic medications over time is likely to be attributed to a combination of a number of factors, including the possible increase in the prevalence and detection of depression, decrease in stigma, increase in community awareness and help-seeking behaviours, and the roll-out of a new range of antidepressants with less side effects and greater range of off-label uses (McManus et al., 2000; Olfson and Marcus, 2009; Paulose-Ram et al., 2007; Stephenson et al., 2013). The stable or rising prevalence of depression in the community suggests that the widespread use of these agents may not be having an impact on reducing the prevalence of mental illness– logical as these agents are used only once a case has manifested. There is evidence of a disconnect between prescription and diagnosis, with community studies showing that many people prescribed these agents are not diagnosed with depression, and many people who meet criteria for depression remain untreated (Olfson et al., 2016). Future research should target whether increased psychotropic medication use worldwide translates into a reduction in the symptomatic burden of mental illness and improvements in quality of life for patients at a community level. The optimal management of mood disorders in the community and judicious use of psychotropic agents remain vexing issues.
Footnotes
Acknowledgements
The authors acknowledge the research personnel and participants of the Geelong Osteoporosis Study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.L.S., M.M. and S.E.Q. have no conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the manuscript. J.A.P. has received grant/research support from NHMRC, BUPA Foundation, Deakin University, Barwon Health, the Western Alliance, the Geelong Community Foundation and Amgen/GlaxoSmithKline/Osteoporosis Australia/Australian and New Zealand Bone and Mineral Society. S.L.B.-O. has received grant/research support from The University of Melbourne, Deakin University and an Alfred Deakin Postdoctoral Research Fellowship; has received speaker fees from Amgen; and is currently supported by an NHMRC Career Development Fellowship (GNT1107510). M.B. has received grant/research Support from the NIH, Cooperative Research Centre, Simons Autism Foundation, Cancer Council of Victoria, Stanley Medical Research Foundation, MBF, NHMRC, beyondblue, Rotary Health, Geelong Medical Research Foundation, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Meat and Livestock Board, Organon, Novartis, Mayne Pharma, Servier and Woolworths; has been a speaker for AstraZeneca, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Janssen Cilag, Lundbeck, Merck, Pfizer, Sanofi-Synthelabo, Servier, Solvay and Wyeth; and served as a consultant to AstraZeneca, Bioadvantex, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Janssen Cilag, Lundbeck Merck and Servier. L.J.W. has received grant/research support from Eli Lilly, Pfizer, The University of Melbourne, Deakin University and the NHMRC and is supported by an NHMRC Career Development Fellowship (GNT1064272).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Geelong Osteoporosis Study is funded by the National Health and Medical Research Council (NHMRC of Australia, projects 299831, 628582, 1009367, 1026265, 1021345, 1104438). The funding body played no part in the design or conduct of the study; collection, management, analysis and interpretation of the data, or preparation, review or approval of the manuscript.