
Abstract
Background:
Nascent evidence indicates that the mental health of parents and children has markedly declined during the COVID-19 pandemic. Considering disruptions to traditional face-to-face mental health services resultant from stay-at-home orders, the potential value of digital mental health interventions has become extremely apparent. Despite this, uptake of digital interventions remains poor, indicating that a better understanding is needed of factors that determine a willingness to use digital platforms.
Method:
The present multi-wave, longitudinal study of 2365 Australian parents explored between-person and within-person predictors of intentions to use digital interventions during the pandemic.
Results:
More than one-third of parents reported likely use of a self-guided and therapist-guided digital intervention, with the most endorsed reason for use being to support their child’s mental health. Between-person baseline predictors of higher intention ratings were parent’s prior mental illness, not living with a partner and recent environmental stressors. Within-person predictors of higher intention ratings were endorsement of mindful parenting strategies, child access to the Internet, better perceived management of child’s education, lower social support and financial hardship.
Conclusion:
Findings demonstrate that willingness to engage in digital interventions fluctuates in response to changing circumstances. Identifying novel ways to increase acceptance and uptake of digital interventions based on modifiable predictors established here is needed to realize the full potential of these modes of care in times of need.
Introduction
The outbreak of the coronavirus disease 2019 (COVID-19) has had a significant impact on Australian families. Most areas of the country have experienced mandated stay-at-home policies to curb the spread of infection, resulting in multiple stressors (Fischer et al., 2020). As the mental health and wellbeing of Australian parents and children have worsened during the pandemic (Newby et al., 2020; Westrupp et al., 2021), ensuring that adequate support is available both during and after COVID-19 is critical.
The potential value of digital mental health interventions has become increasingly apparent during COVID-19 (Gunasekeran et al., 2021; Torous et al., 2020). Empirically supported digital interventions can be scaled up to reach a large number of families, especially those for whom face-to-face treatment approaches are not an option for reasons related to cost, geographical constraints, privacy and health concerns (Andersson, 2016; Andersson et al., 2019). Proponents of digital health also emphasize their flexible content delivery, with some programmes offering guided support while others capitalizing on artificial intelligence features that offer tailored feedback and strategies (Linardon et al., 2019; Torous et al., 2021). Since most Australians own or have access to a smartphone or the Internet (Deloitte Access Economics, 2019), digital interventions may be a suitable mode of support to help address the wellbeing of Australian families psychologically impacted by COVID-19.
Despite the advantages of digital interventions, their uptake is limited. Uptake rates may be as low as 40% in some community and clinical populations (Linardon and Fuller-Tyszkiewicz, 2020; Torous et al., 2018). Furthermore, current digital interventions are still under-servicing key groups, such as fathers, non-urban parents and parents from a low socioeconomic background (Westrupp et al., 2020b). While uptake barriers related to low usability ratings and data security concerns have been noted (Jake-Schoffman et al., 2017; Torous et al., 2018), lower acceptance of digital interventions is one of the more important barriers limiting their uptake (Apolinário-Hagen et al., 2017a).
According to the Unified Theory of Acceptance and Use of Technology (Venkatesh et al., 2016), acceptance is defined as the behavioural intent to use a technology, with intent being the most proximal predictor for actual technology use. Understanding Australian parents’ digital health intentions and associated predictors during COVID-19 may shed light on those most likely to use a digital intervention during a crisis. This information may be needed for informing effective models of dissemination and targeted promotion aimed at increasing the use of digital interventions. Existing research investigating predictors of digital intervention intent has been limited to cross-sectional designs (De Veer et al., 2015; Handley et al., 2015; Linardon et al., 2020b; Sweeney et al., 2015), and little is known about intentions of engaging in a digital mental health intervention among parents, both for themselves or for their children.
Andersen’s model of Health Services Utilization (Andersen, 1995) is a helpful framework to guide understanding of digital intervention intent. This model describes healthcare access as a determinant of factors pertaining to the individual and society. Factors are conceptualized into three broad categories: predisposing (e.g. race, sex, age, poverty level), enabling (i.e. resources that provide or facilitate access to care, such as social support, good health literacy, insurance etc.) and need (i.e. perceived demands for care that can determine the type of care one seeks, including mental health symptom severity, individual experiences, etc.; Andersen, 1995).
Using Anderson’s model as a framework, there may be several plausible predictors of digital health intentions in Australian parents. With respect to predisposing factors, younger people (Bigne et al., 2005; Stallard et al., 2010), particularly women with a higher education (Li et al., 1999; Lynch et al., 2018), have been shown to be more likely to adopt technological innovations and may be more likely to seek help due to less stigma associated with mental health help-seeking. The well-cited treatment barriers faced in racially diverse populations (e.g. Planey et al., 2019) could also indicate that certain racial minority groups might be more receptive to digital interventions given their scalability, cost-effectiveness and flexibility. With respect to enabling factors, sustained social support may predict lower intentions on the basis that a strong support network may be sufficient to effectively manage pandemic-related stressors (Khoury et al., 2021; Yu et al., 2020). Alternatively, social support may predict higher intentions via normalizing or encouraging help-seeking patterns (Jung et al., 2017). For need factors, severity of or changes in a range of different mental health problems from both the parent (e.g. depression, anxiety, stress, drinking behaviour) and child’s perspective (e.g. depression, anxiety, defiance, irritability, general health) may signify higher need to consider digital health interventions in times where face-to-face services have been severely limited. Furthermore, the flexibility of digital interventions is likely to make it attractive to populations with busy schedules, such as parents juggling paid work with caregiving responsibilities and parents with multiple children. Finally, the minimal cost of digital health may also be palatable to parents who have been financially impacted by the pandemic, signifying another ‘needs’ factor.
The present study used intensive, multi-wave longitudinal data collected from Australian parents during the COVID-19 pandemic to investigate potential predisposing, enabling and need predictors of parental intentions to use digital interventions, both for themselves and for their children. Given the limited research investigating predictors of digital health intentions, this study will explore the predictive ability of a range of within- and between-person predictors that broadly aligns with Andersen’s model of Health Services Utilization framework. Our goal of this exploratory work is to inform future confirmatory studies in this area.
Method
Design and recruitment
This study used nine waves of data from the COVID-19 Pandemic Adjustment Survey (CPAS) (Westrupp et al., 2020b), a longitudinal study of 2365 Australian parents of a child 0–18 years aiming to investigate the impact of the COVID-19 crisis on Australian families. Participants comprised an online convenience sample recruited using paid Facebook advertising. Participants completed a 20-minute baseline survey (April 2020) with 10 minute surveys emailed thereafter on fortnightly basis. Strategies to maximize retention including sending text messages (SMS) and phoning participants if they did not participate in three consecutive waves. Participants were eligible to participate if they resided in Australia and were aged ⩾18 years, English speaking and were a current parent of a child aged 0–18 years. The study was approved by the Deakin University Human Ethics Advisory Group (HEAG-H 52_2020).
Participants
As detailed in Table 1, parents in the current sample (n = 2365) were primarily women, living in a major city or inner regional area, had an average age of 38 (SD = 7.1) and a primary school-aged child (just over half were boys). Most parents had at least two children, and roughly 10% were single parents.
Sample characteristics for the COVID-19 pandemic adjustment survey (CPAS) samples.
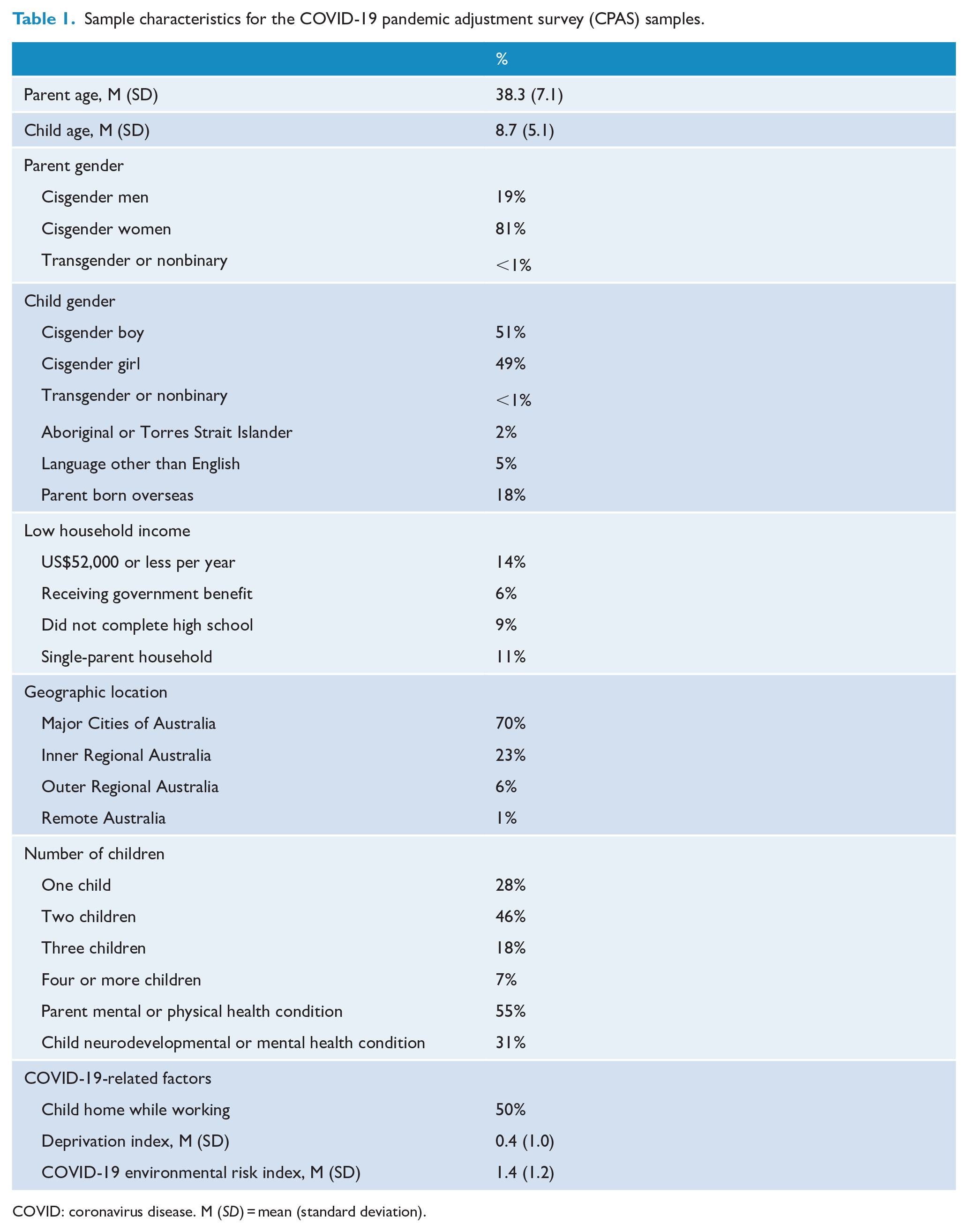
COVID: coronavirus disease. M (SD) = mean (standard deviation).
Most parents in the sample (72%) reported some form of mental health risk for themselves or their children. Seventy-two percent of parents responded in the affirmative for at least one risk factor on the COVID-19 environmental risk index. The COVID-19 environmental risk index was calculated using seven measures. Four items were adapted from the CoRonavIruS Health Impact Survey (CRISIS) to measure (1) participant or family member diagnosis of COVID-19, hospitalization due to COVID-19, self-quarantine due to COVID-19, family member passed away with COVID-19; (2) financial problems directly as a result of COVID-19 (from not at all to extremely); (3) concern with living arrangements due to COVID-19; and (4) food insecurity related to COVID-19. Moreover, participants were also asked whether they had experienced (1) job loss; (6) reduced employment; (7) redeployment to new roles at work. Each of the seven COVID-19 risk factors was converted to a binary variable (0 = no risk; 1 = risk) and summed to form a COVID-19 environmental risk index score. Furthermore, half of the sample reported home-schooling and/or working from home while caring for their child. Baseline characteristics of this sample are broadly consistent with Australian Bureau of Statistics (ABS, 2017); demographic profile of the Australian parent population with respect to number of children per family, parents born overseas, single-parent households and geographic location were reported. The sample was slightly under-representative of families with low income and low education.
Measures
Several instruments were used to collect data on questions of relevance. These include a measure to assess digital intervention willingness at each time-point via three items: ‘The COVID-19 pandemic and the associated measures to increase social distancing have caused many people to feel stressed and worried’. ‘How likely would you be to use an online or smartphone intervention for the following reasons: (1) mental health support for yourself, (2) mental health support for your child and (3) parenting support’. Each item was rated on a 5-point scale from ‘not at all’ to ‘extremely likely’.
Digital intervention preferences were assessed via two items: ‘Should you experience a mental health difficulty in the future, how likely are you to use a (1) Self-guided Internet- or smartphone-app based treatment program? (2) Therapist-assisted Internet-or smartphone app based treatment program?’ Each item was rated on a 5-point scale from ‘extremely likely’ to ‘extremely unlikely’. Participants responded to each of the five items assessing digital intervention willingness and preferences.
Table 2 presents a summary of study measures. Predictors broadly assessed family demographics, individual parent and child factors, COVID-19-related stressors, parent outcomes (i.e. depression, anxiety, stress, emotion regulation, alcohol consumption and smoking), child outcomes (i.e. depression and anxiety) and family functioning (parenting irritability, couple verbal conflict and family).
Within- and between-Person predictors examined.
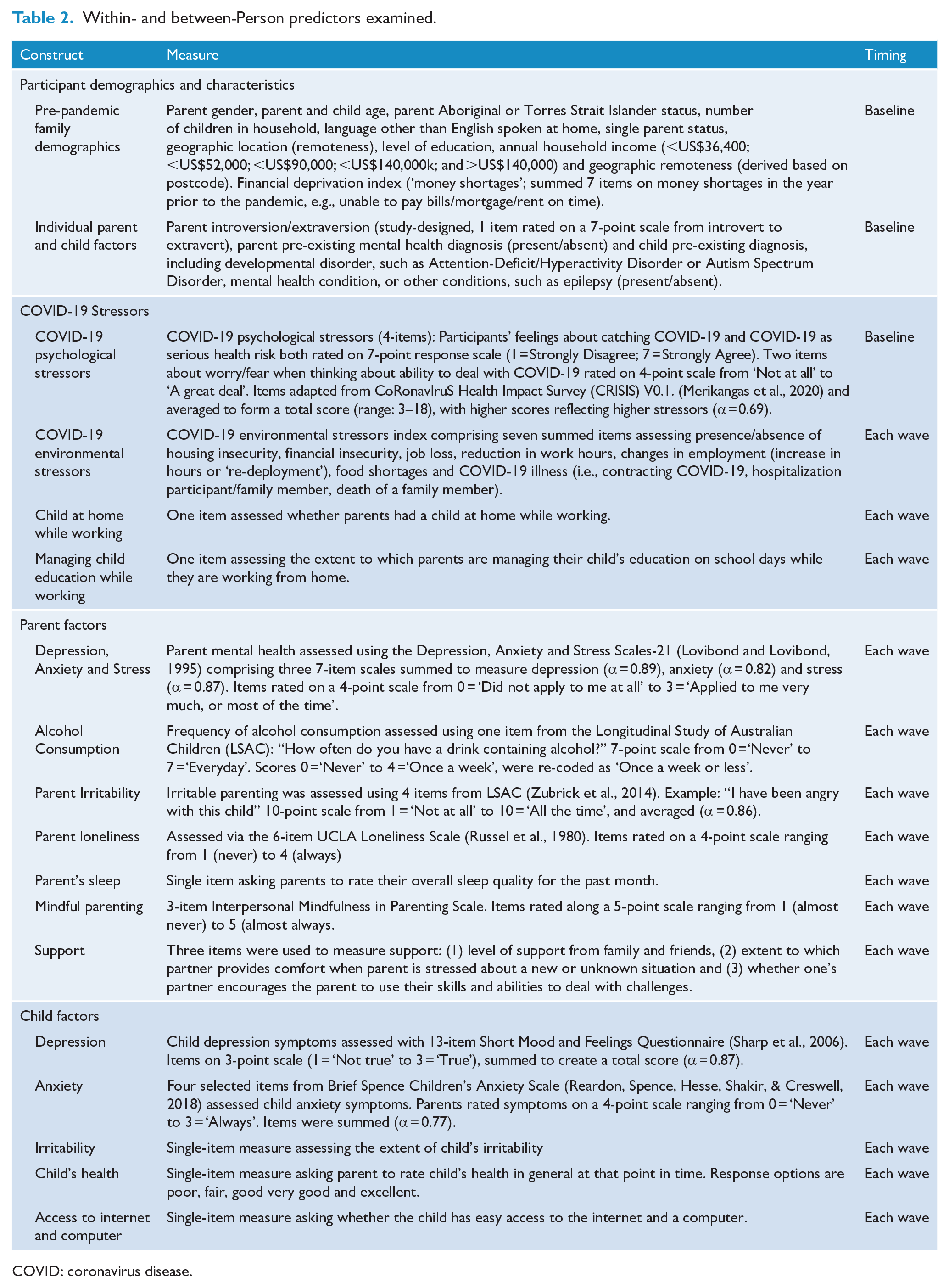
COVID: coronavirus disease.
Data analytic strategy
Analyses were conducted using Mplus Version 8.3. Research questions were tested using multilevel modelling, to control for non-independence in the dataset attributable to the repeated measures design. Each of the five likelihood of app use items were regressed – in separate models – onto between-person predictors measured at baseline and within-person predictors measured at each of the nine waves. These within-person predictors were group-mean centred, whereas between-person predictors were left uncentred. Bayesian estimation was used for modelling, enabling derivation of standardized coefficients for predictors to facilitate comparison across variables and models. Parameter estimates derive from Bayesian posterior distributions and are accompanied with 95% credibility intervals to denote plausible range of values for each predictor.
Variance inflation factor scores were all below 2, suggesting no discernible issues with multicollinearity among predictor variables. Outcomes were modelled as continuous, under the assumption that the underlying distribution for likelihood of digital health treatment uptake followed a normal distribution. Checks of normality of residuals with the Shapiro–Wilk normality test found non-significant results for each outcome (ps ranged from 0.476 to 0.985), suggesting this assumption was adequate for the present data.
Missing data were handled using full information maximum likelihood estimation (FIML). On average, participants in the sample completed four waves of data (SD = 2.65). Sample size for the nine waves was: Wave 1 n = 2365, Wave 2 n = 1302, Wave 3 n = 1103, Wave 4 n = 921, Wave 5 n = 781, Wave 6 n = 820, Wave 7 n = 974, Wave 8 n = 739 and Wave 9 n = 688.
Results
Baseline mental health and digital intervention preferences
At baseline, 23% of parents scored in the moderate to extremely severe range for anxiety, 28% were at least moderate for depressive symptoms and 30% reported scores in at least the moderate category for stress, as assessed by the Depression Anxiety Stress Scales. Furthermore, 9% of children had parent-reported scores within the possible clinical range for depressive symptoms assessed using the Short Moods and Feelings Questionnaire.
Across the nine waves of data collection, the average proportion of preferences for digital interventions were relatively stable across the cohort (see Figure 1). In terms of likelihood of using a digital intervention, 33–38% of participants indicated they were very/extremely likely to use a self-guided digital intervention, whereas 37–41% were very or extremely likely to use a therapist-assisted digital intervention. When asked about the purpose of digital intervention use, 26–31% of participants at each wave indicated they were very or extremely likely to use a digital intervention to support themselves, 36–39% were very/extremely likely to use an digital intervention to support their child and 28–31% were very/extremely likely to use a digital intervention for parenting support. Yet, looking at change within parents over time, level of intent to use digital health services remained stable (across all waves) for less than 20% of the sample. Moreover, within-person correlations among these digital intervention preference variables ranged from 0.25 to 0.55, with strong correlations among the items asking about different reasons for use (self, child, parenting) ranging from 0.52 to 0.55 and the two items asking about likelihood in general (therapist, self-guided) correlating at 0.53. Correlations between these different item types (preference for different reasons vs likelihood in general) ranged from 0.24 to 0.31 (all ps < 0.001). Together, these findings suggest considerable inter- and intra-individual variability in preferences for digital interventions across the COVID-19 crisis in Australia.
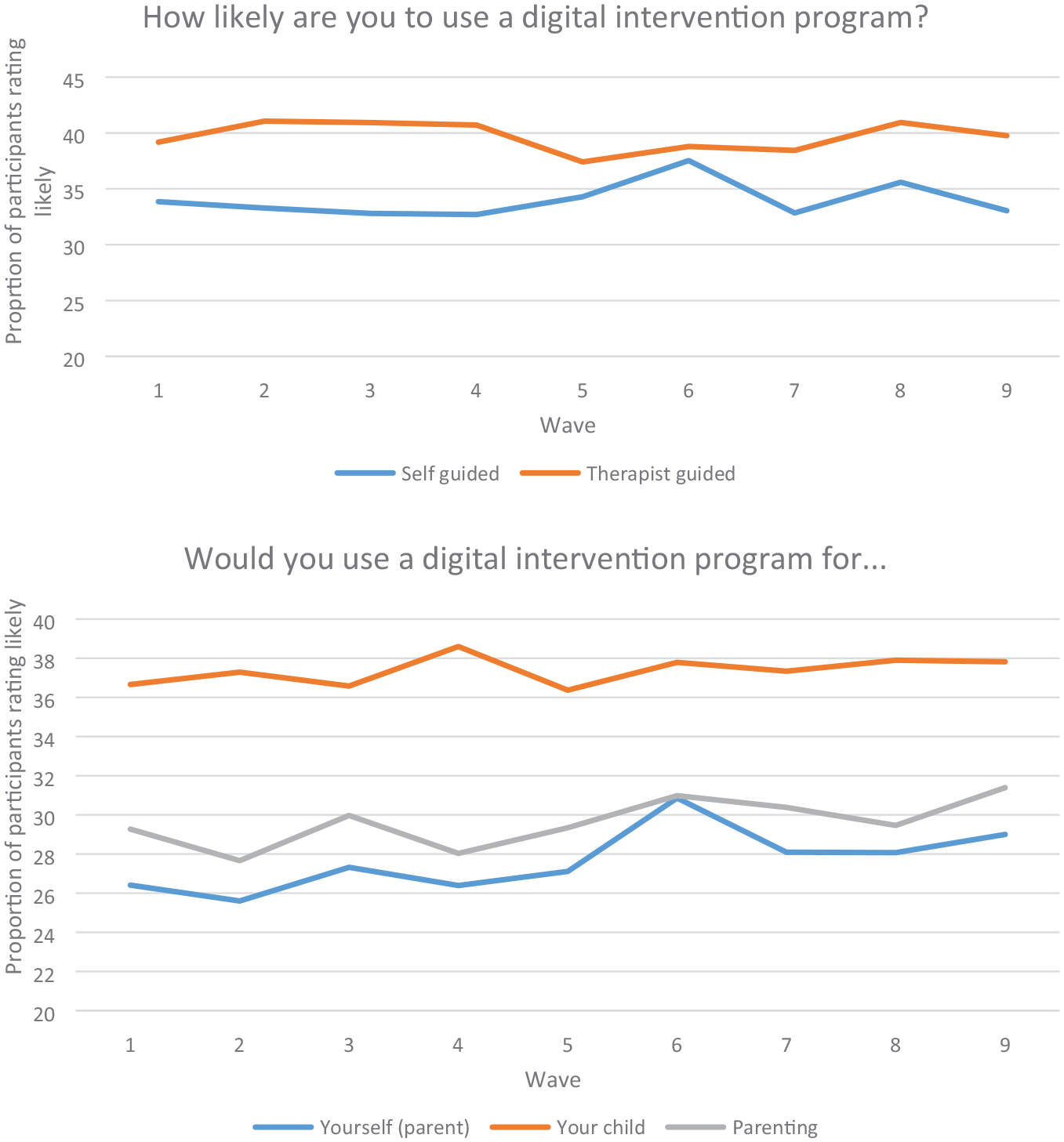
Proportion of participants who likely to use a digital intervention over time.
Main analyses
As shown in Table 3, several between- and within-person predictors were found to predict parents’ ratings of how likely they were to use a digital intervention, whether for their own mental health, that of their child, or for parenting.
Predicting likely use of digital intervention for self (parent), child, or parenting.
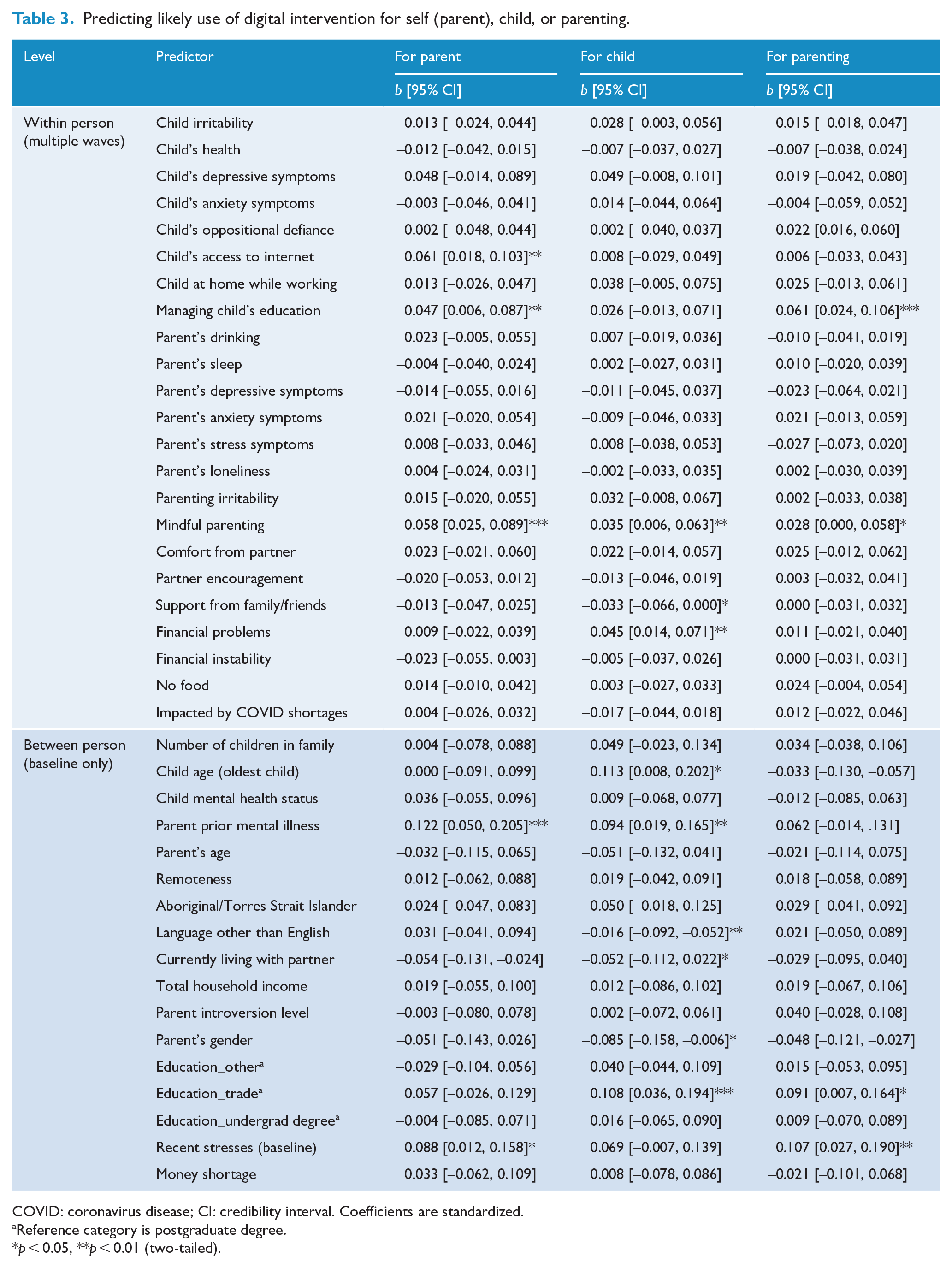
COVID: coronavirus disease; CI: credibility interval. Coefficients are standardized.
Reference category is postgraduate degree.
p < 0.05, **p < 0.01 (two-tailed).
Predictors of reasons for likely use of a digital intervention
Parental mental health
Within-person predictors of parents reporting greater likelihood of using a digital intervention for themselves if (1) they reported greater self-perceived management of child education at home during COVID, (2) they more strongly endorsed mindful parenting and (3) their child had access to the Internet. Between-person predictors of parents reported greater likelihood of using a digital intervention for themselves if (1) the parent had prior history of mental illness and (2) reported higher levels of recent stressors at baseline. In total, the predictors accounted for 11% of within-person variance (p < 0.001) and 14% of the between-person variance (p < 0.001) in likelihood of using a digital intervention for oneself (parent).
Child mental health
Within-person predictors of parents reporting greater likelihood of using a digital intervention for their child were (1) stronger endorsement of mindful parenting, (2) less perceived support from family and friends and (3) elevated financial hardship. Between-person predictors of increased likelihood of using a digital intervention for one’s child included (1) higher age of eldest child, (2) parent’s prior history of mental illness, (3) language other than English spoken at home most of the time, (4) living alone (without a partner), (5) the parent being female and (6) highest level of education being trade certificate, diploma, or apprenticeship (relative to postgraduate degree). Combined, the predictors accounted for 6% of within-person variance (p < 0.001) and 19% of the between-person variance (p < 0.001) in likelihood of using a digital intervention for one’s child.
Parenting support
Within-person predictors for greater likelihood of using a digital intervention for parenting include (1) greater self-perceived management of child education at home and (2) stronger endorsement of mindful parenting. Between-person predictors were (1) higher levels of reported stress at baseline and (2) highest level of education being trade certificate, diploma, or apprenticeship (relative to postgraduate degree). All predictors combined accounted for 7% of within-person variance (p < 0.001) and 13% of the between-person variance (p < 0.001) in likelihood of using a digital intervention for parenting support.
Predictors of mode of use of a digital intervention
Self-guided digital intervention
Table 4 summarizes model results for items asking about likelihood of future use of a self-guided or therapist-assisted digital intervention. Within-person predictors of increased likelihood of using a self-guided programme were (1) poorer child health, (2) greater self-perceived management of child education at home and (3) higher parent irritability. Between-person predictors were (1) living alone (no partner), (2) lower level of introversion and (3) highest level of education being trade certificate, diploma, or apprenticeship (relative to postgraduate degree). In total, the predictors accounted for 5% of within-person variance (p < 0.001) and 12% of the between-person variance (p < 0.001) in likelihood of using a self-guided digital intervention.
Predicting likelihood of using a self-guided or therapist-assisted digital intervention.
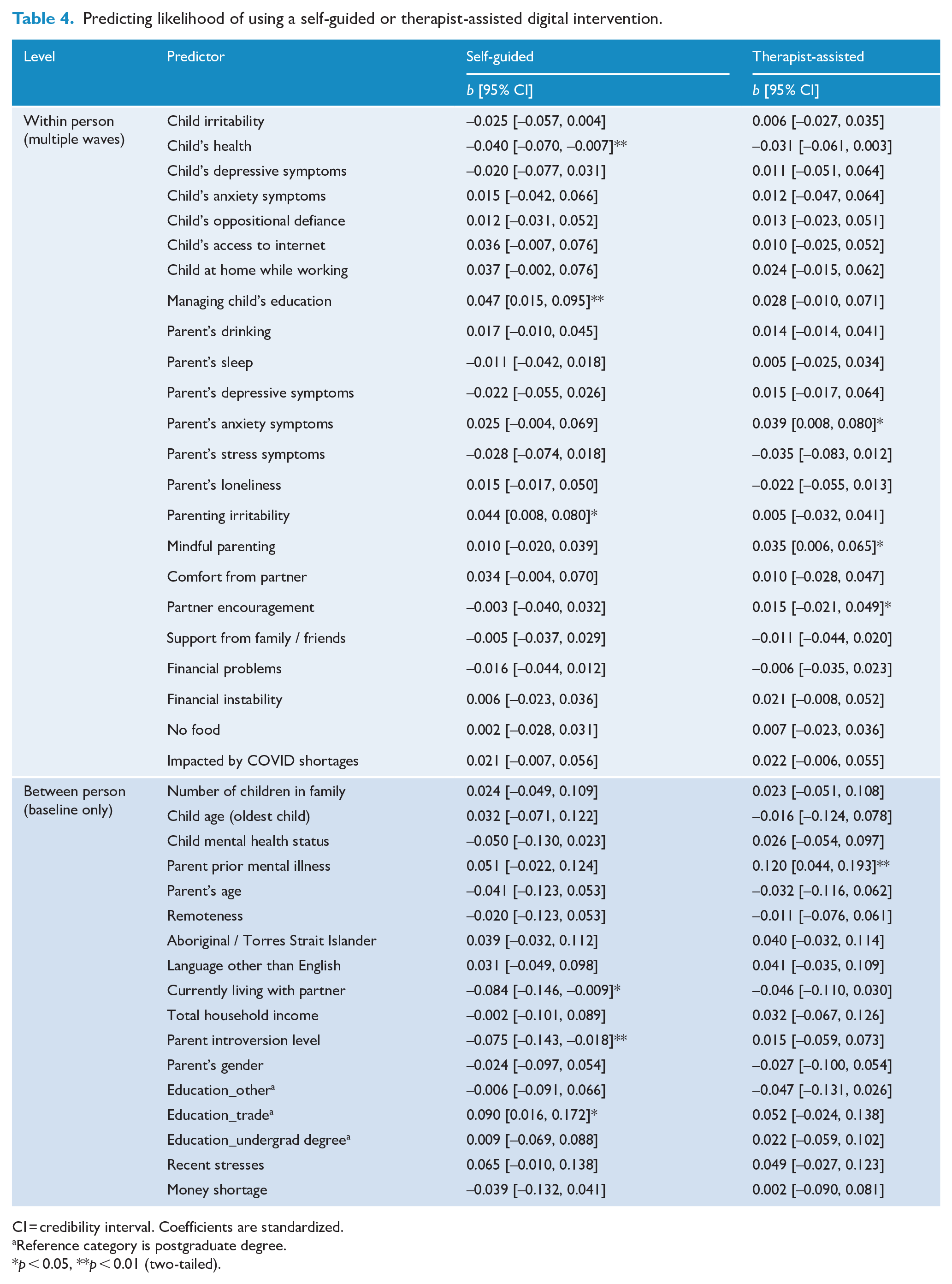
CI = credibility interval. Coefficients are standardized.
Reference category is postgraduate degree.
p < 0.05, **p < 0.01 (two-tailed).
Therapist-guided digital intervention
Within-person predictors of increased likelihood of using a therapist-guided digital programme were (1) higher parent anxiety ratings, (2) more mindful parenting, (3) greater partner encouragement to use their own skills and (4) abilities to deal with challenges. Parent history of mental illness was the only between-person predictor of increased likelihood of using a therapist-guided digital programme. In total, the predictors accounted for 7% of within-person variance (p < 0.001) and 12% of the between-person variance (p < 0.001) in likelihood of using a therapist-assisted digital programme.
Discussion
Summary of key findings
Across the nine waves of data, approximately one-third of the sample indicated that they were very likely to use a digital intervention for the mental health of themselves or their child or for parenting support. While these figures are broadly consistent with digital intervention preference data from prior studies (Apolinário-Hagen et al., 2018; Batterham and Calear, 2017; Linardon et al., 2020a), the present study offered unique insights by exploring shifting preferences over time and in response to changing circumstances. Interestingly, preferences for digital interventions varied within individuals, suggesting that under some circumstances individuals may be more or less likely to adopt a digital programme.
A range of factors were predictive of intentions to use a digital intervention across the multiple domains assessed in this study (parental mental health, child mental health and parenting support). First, parents who reported greater engagement with mindful parenting practices were more likely to report likelihood of digital intervention use for themselves, their child’s health and for parenting. This may reflect willingness for psychological help-seeking based on existing buy-in to psychological principles, such as mindfulness. Prior history of mental illness was also predictive of higher reported likelihood of digital intervention use for child and parent mental health. Interestingly, mindful parenting and prior history of mental illness were both predictive for therapist-guided but not for self-guided intervention options. Given the nature of items used in the present study, it is unclear whether this pattern of findings reflects prior difficulties with self-guided programmes or possible belief that therapists are an essential component for mental health care. Even so, the predictiveness of mental illness history and mindful parenting practice is consistent with the notion that prior experience with psychological treatment helps to break down resistance to help-seeking (e.g. Gulliver et al., 2010).
Findings were more mixed with respect to mental health status as a motivator for intent-to-use digital intervention options. On the one hand, between-person differences at baseline in recent stressors (higher stress increased likelihood of treatment intent) and within-person elevated scores for poorer child health, parent irritability and anxiety symptoms were associated with greater intent for parent, child and/or parenting purposes. By contrast, time-varying measures of the majority of parent and child mental health constructs (anxiety, irritability and oppositional defiance for child; depression and stress for parent and child) did not predict intent ratings. This pattern of findings may reflect parents’ realization of the importance of addressing one’s own mental health concerns in order to provide necessary support for one’s child.
Given recent evidence of COVID-19-related spikes in mental health issues for both parents and children (Westrupp et al., 2020a), null findings for parent mental health variables may also indicate that mental health concerns were already elevated at baseline, in the midst of the first national stay-at-home orders in Australia. Indeed, the proportion of parents who reported moderate to severe levels of psychological distress (anxiety, depression and stress) is higher than established Australian norms with this measure (Crawford et al., 2011).
Although cost associated with treatment is often described as a barrier to help seeking via traditional means (Kazdin, 2017; Kazdin and Blase, 2011; Patel et al., 2018), increasing financial problems were largely unrelated to intention-to-seek digital intervention services. It is possible that the effect of financial situation on treatment seeking is more complex than can be uncovered from our modelling approach. For instance, the predictive value of financial status may be dependent on level of child and parent (mental) health; availability of support from partner, family and friends; and time affordances to utilize geographically located, traditional treatment options. These proposed support and risk factors were similarly inconsistent predictors across models. Future research may consider whether more elaborate predictor combinations enhance prediction of treatment-seeking intent. An alternative explanation might be that parents are aware that digital mental health interventions are of low cost or free, and thus, financial hardship might not be a determining factor on whether one reports an intent to engage with this intervention modality.
Implications/future research directions
Present findings overall highlight that preferences for digital interventions fluctuate in response to one’s changing circumstances. However, history of mental illness and mindful parenting seemed to be a stronger driver of intent ratings than parents’ changing mental health symptoms and levels of social support. Reasons for the reservation from those at greater need to actually use digital intervention options are unclear, but may signal hesitance due to perceived ineffectiveness relative to traditional face-to-face forms of treatment (Linardon et al., 2020a), preference for face-to-face if mental health symptoms are particularly pronounced (Apolinário-Hagen et al., 2018), or fear or lack of awareness of non-traditional forms of treatment (Apolinário-Hagen et al., 2017b). As with prior studies, preferences tended to be higher for therapist-guided than self-guided forms of treatment (Apolinário-Hagen et al., 2018; Linardon et al., 2020b). Negative opinions about digital interventions constitute a barrier for realizing the potential of ‘e-health’ to flexibly and cheaply offer evidence-based therapy at scale (Torous et al., 2015, 2020).
Co-design principles have been proposed as ways to enhance credibility, acceptance and uptake of digital intervention programmes (Torous et al., 2018). Early efforts adopting these recommendations have been promising (e.g. Tighe et al., 2017), yet issues of drop-out and treatment non-adherence remain in these studies (Linardon and Fuller-Tyszkiewicz, 2020). Thus, more work is needed to better understand for whom digital interventions are preferable and likely to yield comparable efficacy to traditional face-to-face therapies. Such information is vital if we are to develop a triaged healthcare system approach that can lighten the burden on face-to-face treatment services without diminishing quality of care (Iorfino et al., 2019; Rowe et al., 2020).
Limitations
Present findings should be interpreted within the context of several study limitations. First, the small number of children and parents identifying as non-binary, trans and queer gender precluded more nuanced explorations of gender identity as a predictor of preferences and intent. Mental health risks and receptiveness to treatment options may differ for these groups (Rees et al., 2020) and thus warrant attention in future research.
Second, the current study’s sample was recruited using both paid and unpaid Facebook advertising. The use of online recruitment may have resulted in a sample with higher digital access and literacy than the broader parent population, which may in turn lead to overestimates of their intention to use digital mental health supports.
Third, many theoretically relevant variables potentially related to digital health preferences and intentions were not assessed due to concerns with balancing richness of data against participant burden and fatigue. For example, prior history of digital intervention use, knowledge levels of key differences between self- and therapist-assisted digital interventions, intentions to seek psychological help more generally (e.g. face-to-face services) and drivers of digital intervention intentions (e.g. performance expectancy, effort expectancy, social influence and facilitating conditions) according to the Unified Theory of Acceptance and Use of Technology (Venkatesh et al., 2016) may have emerged as more influential outcome predictors. Although predictors were selected on the basis of conceptual and pragmatic reasons, their ability to explain <20% variance in intent and preference ratings suggests that future work should seek to explore the predictive value of those other variables outlined above. Relatedly, preference and intent for digital interventions were not assessed prior to the pandemic, suggesting that it is as yet uncertain whether fluctuations in these ratings over time were unique to the COVID-19 pandemic.
Fourth, as with most intensive longitudinal designs, attrition rates were high across the nine waves. Although missing data were accounted for by using FIML, the potential influence of selection and attrition bias should be kept in mind when interpreting the present findings. Although we sought to maximize retention via regular reminder emails and participant remuneration, greater efforts to minimize dropout in these intensive longitudinal designs are needed (Teague et al., 2018).
Conclusion
Overall, present findings show that a significant minority of individuals are receptive to engaging in digital mental health intervention. Such preferences and intent are subject to change over time and may reflect a combination of personal circumstances and entrenched beliefs and prior experience with psychological treatment. In light of evident challenges in delivery of traditional modes of healthcare due to COVID-related restrictions, present findings offer insights into who may be receptive to digital modes of treatment delivery. For instance, targeting promotions aimed at increasing awareness of digital interventions to parents facing financial difficulties or mental health problems might be one avenue towards improving the implementation and uptake of digital interventions. While this exploratory study offers several novel insights, future confirmatory work is needed to establish key drivers of digital intervention preferences and ways to enhance receptiveness to this delivery mode.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This research was conducted according to the Declaration of Helsinki. Ethics approval was granted by Deakin University and all participants provided consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: J.L. (APP1196948) and D.H. (APP 1197488) hold a National Health and Medical Research Council Investigator Grant.