
Abstract
Objective:
COVID-19 has led to disruptions to the lives of Australian families through social distancing, school closures, a temporary move to home-based online learning, and effective lockdown. Understanding the effects on child and adolescent mental health is important to inform policies to support communities as they continue to face the pandemic and future crises. This paper sought to report on mental health symptoms in Australian children and adolescents during the initial stages of the pandemic (May to November 2020) and to examine their association with child/family characteristics and exposure to the broad COVID-19 environment.
Methods:
An online baseline survey was completed by 1327 parents and carers of Australian children aged 4 to 17 years. Parents/carers reported on their child’s mental health using five measures, including emotional symptoms, conduct problems, hyperactivity/inattention, anxiety symptoms and depressive symptoms. Child/family characteristics and COVID-related variables were measured.
Results:
Overall, 30.5%, 26.3% and 9.5% of our sample scored in the high to very high range for emotional symptoms, conduct problems and hyperactivity/inattention, respectively. Similarly, 20.2% and 20.4% of our sample scored in the clinical range for anxiety symptoms and depressive symptoms, respectively. A child’s pre-existing mental health diagnosis, neurodevelopmental condition and chronic illness significantly predicted parent-reported child and adolescent mental health symptoms. Parental mental health symptoms, having a close contact with COVID-19 and applying for government financial assistance during COVID-19, were significantly associated with child and adolescent mental health symptoms.
Conclusion:
Our findings show that Australian children and adolescents experienced considerable levels of mental health symptoms during the initial phase of COVID-19. This highlights the need for targeted and effective support for affected youth, particularly for those with pre-existing vulnerabilities.
In Australia, as of 3 June 2021, there had been 30,118 cases and 910 deaths, placing it in the lowest quartile of infection rates and deaths per capita (World Health Organization [WHO], 2021). Australia’s low rate of infection was partly explained by the governments’ use of restrictive measures to reduce the infection rate. These restrictions led to disruptions to Australian families lives through social distancing, school closures and a temporary move to home-based online learning and effective lockdowns. As COVID-19 and the restrictions continued, there was growing concern about the impact on mental health – and youth mental health in particular (Holmes et al., 2020). This was due to the severe disruption to education, affecting young people’s ability to learn and reducing the opportunity for peer interaction. Few studies have determined the impact of pandemic-related disruptions on children and adolescents, which is worrying, given the importance of learning, peer interaction and social connection in these development stages (Orben et al., 2020). Understanding the mental health effects of the COVID-19 pandemic on children and adolescents, in the context of known and pandemic-related risk factors, is crucial to inform policymakers how to support communities as they face the ongoing COVID-19 pandemic and future crises.
Research that does exist has shown that children and young people have experienced high levels of mental health symptoms during the pandemic (Racine et al., 2020). A study in China found that 18.9% of children (grades 2–6) reported elevated anxiety symptoms and 22.6% of children reported elevated depressive symptoms (Xie et al., 2020). A large cohort study (n = 12,500) tracking changes in child and adolescent mental health since early lockdown in the United Kingdom, named Co-SPACE (COVID-19: Supporting Parents, Adolescents and Children during Epidemics) (Waite and Creswell, 2020) found a rise in parent-reported child and adolescent mental health symptoms in the early lockdown period (March–June 2020), with hyperactivity/inattention and conduct problems increasing. Emotional symptoms increased in preadolescents, but slightly decreased for adolescents (Waite et al., 2021). Another non-peer-reviewed study (predominantly United States) found that self-reported depressive symptoms, but not anxiety symptoms, had increased among adolescents over the first 6 months of the pandemic (Barendse et al., 2021). Globally, younger age groups’ mental health has been shown to be disproportionately affected by the pandemic (Santomauro et al., 2021).
In Australia, evidence has shown that adolescent mental health deteriorated early in the pandemic. Self-reported depressive and anxiety symptoms in 13- to 16-year-old Australians increased from before the COVID-19 outbreak to 2 months following government restrictions (Magson et al., 2021; to May 2020). Li et al. (2021) found that 75% of adolescents (aged 12–18 years) reported worsening mental health since the pandemic began (to August 2020), and that these effects were more pronounced among adolescents with a pre-existing anxiety or depression diagnosis. Beyond these studies, estimates of mental health symptoms in children and adolescents – particularly those reported by parents – during the pandemic in Australia are largely unknown and no studies have reported on the magnitude or clinical significance of problems in children and adolescents. Obtaining parent-reported data to detect mental health symptoms in younger children (versus adolescents) is important given the lack of validated self-report measures for children under the age of 8 years, and parent report is considered a more reliable indicator of diagnostic outcomes for preadolescent children (Creswell et al., 2020). Given the severity of restrictions in Australia and the high degree of compliance by Australian citizens (Pfeffer, 2021), as well as a documented increase in help-seeking (Young, 2020), it is likely that Australian child and adolescent mental health may have fared particularly badly.
Pandemic aside, risk factors known to be associated with poor child and adolescent mental health generally include coming from a low-income (Wickham et al., 2017) or single-parent household (Nguyen et al., 2017), identifying as Aboriginal or Torres Strait Islander (Zubrick et al., 2005), having a neurodevelopmental condition (Hansen et al., 2018), having a chronic physical health condition (Pinquart and Shen, 2011a, 2011b) or having a parent with a mental health disorder (Lawrence et al., 2019). Males are more likely to have any mental health disorder across childhood and adolescence compared to females, although during adolescence, females are more likely to experience anxiety or depression than males (Lawrence et al., 2015). Younger children may have faced particular challenges given they are less likely to learn independently while out of school and are more dependent on their parents (who have experienced high levels of stress during the pandemic; Whittle et al., 2020). However, adolescents are likely to have faced challenges given their developmental need for autonomy and social connection, which have been disrupted by restrictions.
In addition to known risk factors, it is important to investigate the relationship between mental health symptoms and risk factors associated with COVID-19, such as exposure to COVID-19, and impacts on parental employment and household finances, given that loss of employment and financial strain are well-documented correlates of youth mental health problems (Bubonya et al., 2017). In Australia, social distancing measures and lockdown resulted in increases in unemployment, causing financial difficulties for many households. Social isolation and loneliness due to restrictions are also likely to be a key factor associated with anxiety and depressive symptoms in children and young people (Loades et al., 2020), and the longer restrictions continued, youth mental health symptoms may have deteriorated further (Raw et al., 2021). The severity and length of restrictions have varied across the states of Australia. Given that stricter government restrictions were negatively associated with adolescents’ mental health symptoms outside of Australia (Barendse et al., 2021), it seems possible that the severity and length of restrictions in Australia would be associated with child and adolescent mental health.
The aim of this study was to assess the impact of the COVID-19 pandemic on child and adolescent mental health during the initial stages of the pandemic in Australia (May–November 2020). We extended the Co-SPACE UK research to an Australian context, and report on the same broad parent-reported measures of mental health symptoms (Strengths and Difficulties Questionnaire, SDQ), as well as outcomes related to child and adolescent anxiety symptoms and depressive symptoms separately, as broad measures may mask differences in outcomes for these symptom domains. The first aim was to report on mental health symptoms in a sample of children and adolescents. The second aim was to examine associations between known risk factors and COVID-19-specific risk factors (e.g. exposure to COVID-19) and child and adolescent mental health symptoms. As a result of the restrictions differences across Australian states, we also examined outcomes for those in Victoria compared to the rest of Australia.
Method
COVID-19 in Australia
In Australia, the number of confirmed COVID-19 cases was over 1000 on 21 March 2020, 10 days after the WHO declared the outbreak a pandemic. On this date, Australian states and territories, with the support of the federal government, began to implement a strategy known as ‘aggressive suppression’ of the virus (Bromfield and McConnell, 2021). Non-essential services, including restaurants and sporting venues, were forced to close; domestic and international borders were closed; schools began to close in most territories and states; and strict limits were placed on social gatherings. Many of these restrictive measures began to ease at the end of April 2020, with schools opening again for a significant majority of children by 27 May 2020. In the subsequent 5 months, there were varying stages of lockdown in different states and territories, including a second lockdown in Victoria (Table 8, Supplementary Materials). Due to these differences, we compared outcomes for those in Victoria to the rest of Australia. The recruitment period ran from 5 May 2020 to 16 November 2020; at the end of this period, there had been over 55 million COVID-19 cases and 1.3 million COVID-related deaths worldwide, with 27,725 cases and 907 COVID-related deaths in Australia.
Study design and participants
Data were collected via two online baseline surveys. Both surveys included the same questionnaires reported on in this paper, as well as additional questions to capture issues specific to the research interests of each research team. Parents 1 (aged 18 years and over) of school-aged children and adolescents (aged 4–17 years) who lived in Australia were eligible to take part. During the second lockdown in Victoria, we targeted parents living in Victoria specifically. A total of 1327 participants were recruited through advertisements on social media (n = 403) or via a panel provider, CINT (n = 924). Participants recruited via CINT were initially screened to determine eligibility and were reimbursed between A$5 and A$6. Participants recruited via social media were given the option of entering a draw to win one of three A$40 vouchers. We report data on 1397 participants who completed the baseline survey between 5 May and 16 November 2020. The self-selecting nature of recruitment means that this is not a nationally representative sample (Table 1 shows participant demographic information and Table 2 shows a comparison with population data).
Sample characteristics, by age group and total sample.
SDQ: Strengths and Difficulties Questionnaire; RCADS25P: Revised Children’s Anxiety and Depression Scale 25.
Statistically significant difference between two independent (age) groups on mental health outcome measures at p < 0.05.
Sample demographics and comparison with population data (parents of children 4–17 years) from the 2016 Australian Census (ABS, 2016).
Data are from the Australian Bureau of Statistics. These data report the characteristics of Australian parents living with a dependent child, defined as children under 15 years old.
Statistically significant differences between the sample and population census data, p < 0.001 using chi-square analysis.
Procedure
Parents provided written informed consent and completed the survey online. If participants had more than one child, they chose one ‘index’ child on which to report. Research ethics approval was obtained from the participating Universities Human Research Ethics Committees (Griffiths University:2020/350; Macquarie University:52020663515639; University of Southern Queensland:H20REA112; University of Queensland:H2OREA112).
Measures
Child and family characteristics
Parents reported on their own and their child’s age, gender, ethnicity, Aboriginal and Torres Strait Islander origin, geographic state, postcode and household income. Parents reported on their relationship status, their relationship to their child, the child’s biological relationship to the parent, their education status, their child’s education type, their employment status before COVID-19 and whether it had changed during COVID-19. Parents were asked whether they had received or applied for government financial assistance before and during COVID-19. They were asked whether their child had a pre-existing and diagnosed neurodevelopmental condition (e.g. autism), mental health disorder (e.g. anxiety) or chronic health condition (e.g. asthma). Parents rated their child’s overall mental health prior to COVID-19 (5-point Likert-type rating, 1 = poor to 5 = excellent).
SDQ – parent-report
The SDQ consists of 25 items, each rated on a 3-point Likert-type scale (0 = not at all; 2 = certainly true), reported on in the last 6 months. The items load on to five subscales, each with five items (subscale score range = 0–10) (Goodman, 1997). We examined the three subscales related to mental health symptoms, namely emotional symptoms, conduct problems and hyperactivity/inattention. The mean was imputed if at least 60% of subscale items were completed. Cronbach’s alpha estimates for the current sample were acceptable (α = 0.83, α = 0.71 and α = 0.69 for emotional symptoms, conduct problems and hyperactivity/inattention, respectively).
Revised Children’s Anxiety and Depression Scale 25 – Parent version (RCADS25P)
The RCADS25P assesses parent-report of youth anxiety and depressive symptoms in children in years 3–12 (aged 8–17 years) 2 (Ebesutani et al., 2016). The scale consists of 25 items, rated on a 4-point Likert-type scale (0 = never; 3 = always). Two subscale scores relating to anxiety symptoms (15 items; score range 0–45) and depressive symptoms (10 items; score range 0–30) are calculated by summing responses. The mean was imputed if there were less than three response items missing. Cronbach’s alpha estimates for this study were high (α = 0.93 and α = 0.92 for the anxiety symptom and depressive symptom subscales, respectively).
Depression Anxiety and Stress Scales (DASS21)
The DASS-21 was used to measure total parental mental health symptoms over the past 2 weeks (Lovibond and Lovibond, 1995). Twenty-one items were scored on a 3-point Likert-type scale (0 = Did not apply to me at all; 3 = Applied to me very much, or most of the time). Items were summed and doubled to yield a total score (maximum score = 126), with lower scores indicating lower levels of symptoms. The DASS-21 has demonstrated satisfactory psychometric properties (Lovibond and Lovibond, 1995) and internal consistency for the current sample was high (α = 0.97).
COVID-19 exposure
Participants were asked, ‘Has your child had COVID-19?’ with four response options (No/Suspected/Yes, diagnosed and recovered/Yes, diagnosed and still ill), which were Dichotomised for analysis (No/Yes, diagnosed). Responses of ‘suspected’ were coded ‘No’. The COVID-19 status of the child’s close contacts was assessed, ‘Has anyone close to your child been diagnosed with COVID-19’ (Yes/No). Parents were also asked, ‘How much is your child asking questions, reading or talking about COVID-19?’ (5-point Likert-type rating, 1 = never; 5 = most of the time).
Self-isolation status
Self-isolation status was assessed using 11 response options, including ‘I am living my life as normal’ to ‘I am self-isolating due to a diagnosis or COVID-19 possible symptoms’ (Table 6, Supplementary Materials). We dichotomised responses, namely ‘0 = I am living life normally/I am not strictly self-isolating’ versus ‘1 = I am strictly self-isolating’ (e.g. not leaving home at all).
Stage of lockdown/days in lockdown
Two variables were created to account for (1) the stage of lockdown at the time of survey completion and (2) days in lockdown prior to survey completion. The stage of lockdown variable measured the severity of restrictions in place at the survey was completed and area postcode, ranging from stage 1 (few to no restrictions) to stage 5 (enforced stay-at-home orders). Stages were created by the study authors based on classification systems in Australia (Table 7, Supplementary Materials). The days in lockdown variable was created by calculating the total number of days participants had been in the highest stage of lockdown (stage 5) starting from 21 March, 2020 to the date of survey completion (M = 74.9 days, SD = 41.1 days, range = 28–157 days; Table 8, Supplementary Materials).
Data analysis
Our first aim was addressed using descriptive analyses. We dichotomised age to create two variables to reflect the typical patterns of child and adolescent mental health and the different education experiences (children = aged 4–11 years; adolescents = aged 12–17 years). We report on five primary outcome variables related to mental health: SDQ emotional symptoms, SDQ conduct problems, SDQ hyperactivity/inattention, RCADS25P anxiety symptoms and RCADS25P depressive symptoms. We used published cut-off scores to determine the proportion of our sample who experienced different category thresholds of symptoms. No cut-off scores were available for children in grades K to year 2 for RCADS25P, so we used the cut-off scores for the lowest grade available (i.e. grade 3).
Our second aim was addressed using raw scores for the five mental health outcome measures. Initial associations between each outcome variable and each independent variable were examined using univariate analyses. If an independent variable was significantly associated with the outcome variable in the univariate analysis, it was included in the multiple linear regression model for that outcome variable. Multiple linear regression was used to investigate relationships between independent variables and each of the outcome measures, controlling for other measures in the model. Thirty independent variables were assessed and grouped: child/family characteristics (22 variables: split into child/parent demographics [13], child clinical/health background [3], family factors/functioning [3], relationship factors [3]) and COVID-19 risk factors (8 variables: split into COVID-19 exposure variables [2]; COVID-19 impact/measures [6]). Independent variables with more than two categories were collapsed into two categories and dummy coded. Models were checked and showed an absence of multicollinearity, outliers and non-normality of residuals. In accordance with Perneger (1998), we report outcomes without adjusting for multiple comparisons.
Finally, as a result of the second lockdown in Victoria, we also compared mental health outcomes and regression results for participants in Victoria who experienced a second lockdown (on or after 8 July, 2020) to participants in the rest of the country to determine whether there were geographic differences in responses. All analyses were conducted in SPSS v27.
Missing data
Data for participants were included in the analyses when a participant had completed one of the primary outcome measures. Overall, <1% of the data were missing with the exception of the variables measuring government financial assistance before or during COVID-19 (n = 39, 2.9%; n = 117, 8.8% missing responses for each variable, respectively). Due to minimal missing data, all analyses were conducted using listwise deletion.
Results
Mental health and clinical characteristics
Overall, 30.5%, 26.3% and 9.5% of our sample scored in the high to very high range for emotional problems, conduct problems and hyperactivity/inattention, respectively. For anxiety and depressive symptoms, 20.2% and 20.4% of our sample, respectively, scored in the clinical range. Mental health estimates were 2 to 3 times higher in children and adolescents with a pre-existing mental health diagnosis (Table 3). Children experienced higher rates of high to very high levels of emotional symptoms, conduct problems and hyperactivity/inattention than adolescents. On anxiety and depressive subscales, clinical levels of anxiety symptoms and depressive symptoms were similar across age groups, with approximately one in five children or adolescents experiencing clinical levels of symptoms. Of those children and adolescents whose mental health was rated as very good or excellent prior to COVID-19, 23.8%, 23.2% and 7.7% scored in the high–very-high range for emotional symptoms, conduct problems and hyperactivity/inattention, respectively, at the time of survey completion. Similarly, 16.4% and 16.0% of children who were rated as having very good or excellent mental health prior to the pandemic scored in the clinical range for anxiety symptoms and depressive symptoms at the time of survey completion, respectively.
Prevalence of symptoms based on parent-report subscales of the SDQ and RCADS25, by age group and total sample.
SDQ: Strengths and Difficulties Questionnaire; RCADS25P: Revised Children’s Anxiety and Depression Scale 25.
Univariate relationships
Univariate outcomes are shown in Tables 10 and 11, Supplementary Materials.
Multiple linear regression
The independent variables accounted for a significant amount of variance in each model (R2 range = 0.24–0.54, p < 0.001; Tables 4 and 5).
Linear regression models for each SDQ subscale outcome.
SDQ: Strengths and Difficulties Questionnaire.
Bold indicates tests significant at p < 0.05.
p < 0.05; **p < 0.01; ***p < 0.001.
Linear regression models for each RCADS25P subscale outcome.
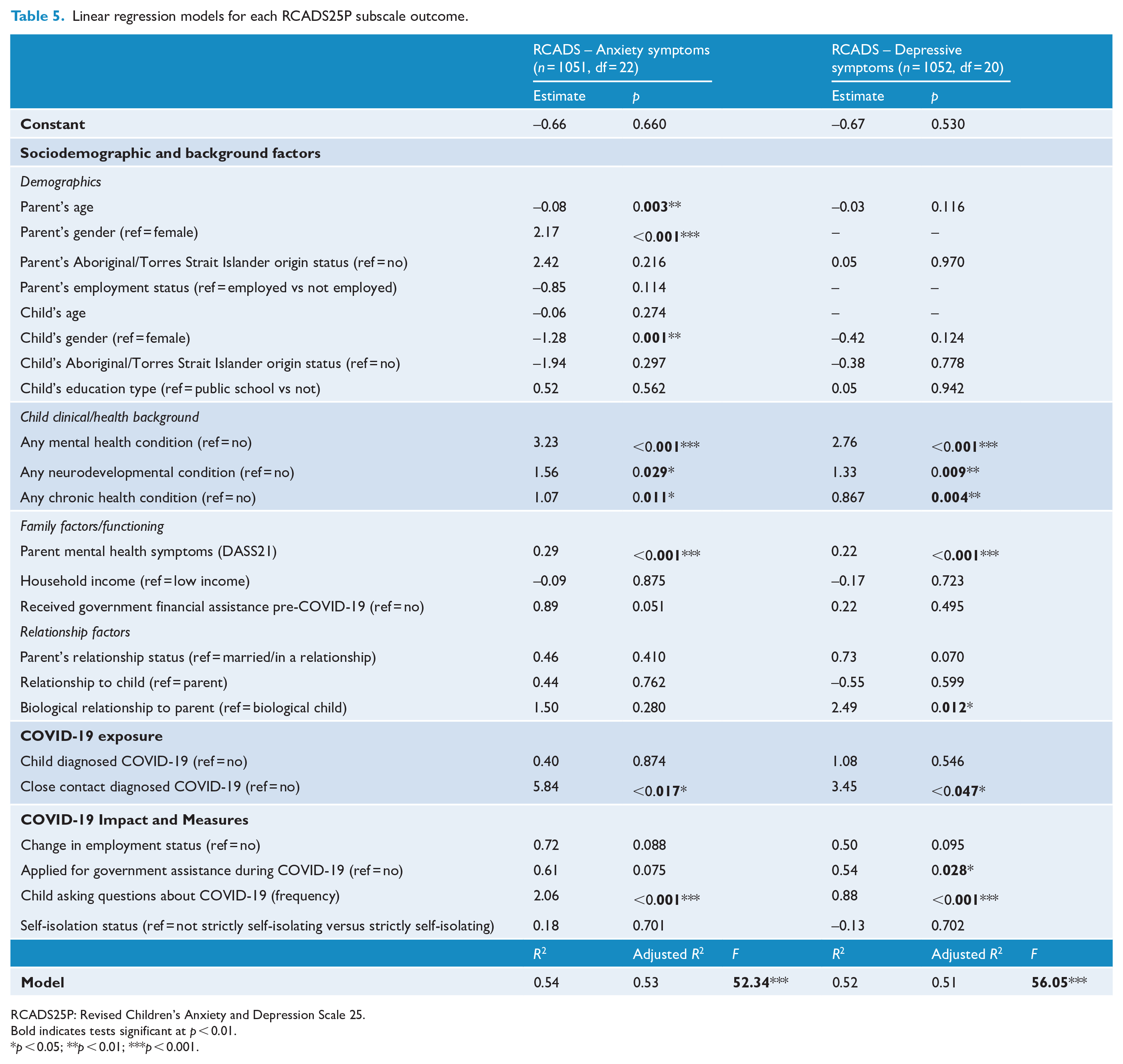
RCADS25P: Revised Children’s Anxiety and Depression Scale 25.
Bold indicates tests significant at p < 0.01.
p < 0.05; **p < 0.01; ***p < 0.001.
Child and family characteristics
Demographics
Parents who were younger and male reported higher levels of conduct problems (ß = −0.13, t = −4.20, p < 0.001 and ß = 0.11, t = 4.01, p < 0.001) and anxiety symptoms (ß = −0.08, t = −2.96, p = 0.003 and ß = 0.11, t = 4.95, p < 0.001) in their child. Younger children were reported to have higher levels of hyperactivity/inattention (ß = −0.14, t = −6.89, p < 0.001) compared to older children. Females were reported to have higher levels of emotional symptoms (ß = −0.08, t = −3.02, p < 0.001) and anxiety symptoms (ß = −0.07, t = −3.28, p < 0.001) compared to males, whereas males were reported to have higher levels of hyperactivity/inattention (ß = 0.65, t = 4.87, p < 0.001).
Child clinical/health background
A child’s pre-existing mental health diagnosis was significantly associated with parent-reported child mental health symptoms across all five outcome measures (ß range = 0.06–0.26, ps < 0.001). A child’s neurodevelopmental condition was significantly associated with parent-reported mental health symptoms for four of the five outcome measures: conduct problems (ß = 0.09, t = 3.09, p = 0.002), hyperactivity/inattention (ß = 0.16, t = 5.03, p < 0.001), anxiety symptoms (ß = 0.05, t = 2.19, p = 0.029) and depressive symptoms (ß = 0.07, t = 2.63, p = 0.009). Children with a chronic illness were reported to have higher levels of anxiety (ß = 0.06, t = 2.54, p = 0.011) and depressive symptoms (ß = 0.07, t = 2.88, p = 0.004).
Family factors/functioning
Parents’ mental health symptoms were significantly associated with parent-reported child and adolescent mental health symptoms across all five outcome measures (ß range = 0.24–0.51, ps < 0.001).
COVID-19 exposure
If a child had a close contact who was diagnosed of having COVID-19, their parents reported the child as having higher levels of anxiety symptoms (ß = 0.10, t = 2.40, p = 0.017) and depressive symptoms (ß = 0.08, t = 5.26, p = 0.047).
COVID-19 impact and restrictions
Application for government financial assistance during COVID-19 was significantly associated with parent-reported emotional symptoms (ß = 0.07, t = 2.54, p = 0.011) and depressive symptoms (ß = 0.05, t = 2.20, p = 0.028). Children asking more frequent questions about COVID-19 had higher levels of emotional symptoms (ß = 0.14, t = 5.20, p < 0.001), anxiety symptoms (ß = 0.19, t = 8.71, p < 0.001) and depressive symptoms (ß = 0.12, t = 5.26, p < 0.001). Days in lockdown was significantly associated with parent-reported child conduct problems (ß = 0.15, t = 1.98, p < 0.048). The greater number of days in lockdown, the higher levels of conduct problems reported.
Comparisons of mental health outcomes in Victoria from the rest of Australia
Given evidence for the association between the severity and length of lockdowns and child and adolescent mental health (Barendse et al., 2021; Raw et al., 2021), we examined mental health outcome among young people located in Victoria on or after 8 July (n = 339)* to the rest of Australia or Victoria before this date (n = 988). We found no significant differences in emotional symptoms, hyperactivity/inattention, anxiety symptoms and depressive symptoms (ps > 0.05). However, conduct problems were reported to be higher in children and adolescents living in Victoria (M = 2.74, SD = 2.36) compared to youth in the rest of Australia (M = 2.17, SD = 2.12), t (1324) = 4.17, p < 0.001. The pattern of regression results for conduct problems for Victorian children and adolescents was the same for participants in the rest of Australia, except that applying for financial assistance during the pandemic was significantly associated with conduct problems (ß = 0.16, t = 2.76, p = 0.006).
Discussion
This study reports parent-reported mental health symptoms in children and adolescents during the initial stages of the COVID-19 pandemic in Australia. Approximately 1 in 3 children and adolescents reportedly experienced high to very high levels of emotional symptoms, 1 in 4 experienced high to very high levels of conduct problems and 1 in 10 experienced high to very high levels of hyperactivity/inattention. One in five children and adolescents reportedly experienced symptoms of anxiety and/or depression indicative of a mental health disorder. We do not have pre-pandemic data so we cannot comment on changes in mental health symptoms because of the pandemic. Nevertheless, these rates are high compared to pre-pandemic levels in a representative pre-pandemic sample of Australian children and adolescents (Laurens et al., 2017; Lawrence et al., 2015; Table 12, Supplementary Materials), although comparisons are highly tentative due to the non-representative sample and symptom measures used in this study. Mean levels of symptoms for the three SDQ subscales were comparable to those reported in UK children and adolescents during a similar phase of the COVID-19 pandemic (Pearcey et al., 2020). Overall, these findings indicate that parent-reported mental health symptoms for children and adolescents were notably high during the initial stages of the pandemic in Australia.
The findings indicated that parent-reported child and adolescent mental health symptoms deteriorated during the pandemic. This result is consistent with a broader trend of worsening mental health symptoms in children and adolescents in Australia even before the pandemic (Brennan et al., 2021; Danchin et al., 2019). Approximately 23% of parents who reported their child as having excellent or very good mental health prior to the pandemic reported high to very high scores for emotional symptoms and conduct problems. Around 16% of parents who reported their child as having excellent or very good mental health prior to the pandemic reported clinical levels of anxiety and depressive symptoms in their child. We acknowledge that obtaining pre-pandemic retrospective estimates of mental health from parents without the use of validated symptoms measures is a limitation of the current research. While our pattern of findings is consistent with other studies that have examined adolescent self-reported symptoms (Li et al., 2021; Magson et al., 2021), we also consider the possibility that parents may not be fully aware of the extent of their child’s symptoms, particularly emotional, anxiety or depressive symptoms (Salbach-Andrae et al., 2009), and thus, our results may be an underestimate of these difficulties. Our reliance on parent-report data for detecting youth mental health symptoms introduces the possibility that parents are less reliable reporters of youth mental health symptoms – particularly for adolescents’ (versus children’s) emotional symptoms (Van Roy et al., 2010). This highlights the importance of a multi-informant approach to obtain a richer and more accurate perspective of children’s mental health symptoms (Gray et al., 2021).
Parents reported higher levels of hyperactivity/inattention in younger children, which supports pre-pandemic data (Lawrence et al., 2015). However, age did not predict greater levels of internalising symptoms. This is surprising – particularly for depressive symptoms–given that a known risk for the onset of these mental health problems is adolescence (Kessler et al., 2005). It may be that increases in family stress, caused by the demands of balancing home learning and work, may have been a particular challenge for parents of younger children. Indeed, younger children would have been more reliant on their parents for educational support and other provision of needs throughout the day. This result is consistent with findings from the United Kingdom that preadolescent children tended to experience greater deterioration in mental health symptoms, including emotional symptoms, whereas adolescents’ emotional symptoms improved over the first month of lockdown (Waite et al., 2021), perhaps due to an ability to better maintain peer relationships via the use of technology (Li et al., 2021).
Children with a pre-existing mental health disorder, neurodevelopmental condition or chronic physical illness had higher levels of parent-reported mental health symptoms compared to those without these difficulties. This finding is consistent with other research (Li et al., 2021; Pellicano et al., 2021) and highlights that expansion of mental health services to support these vulnerable groups of children was necessary. Families who applied for government financial assistance during COVID-19 reported that their child experienced higher levels of emotional symptoms, depressive symptoms and conduct problems (Victoria only). Financial hardship as a result of the restrictions is a risk factor for youth mental health and justifies the use of financial assistance (e.g. Jobseeker) for families affected by the pandemic.
Parent mental health symptoms was associated with child and adolescent mental health symptoms. Parent mental health has deteriorated during the pandemic (Shum et al., 2021; Westrupp et al., 2020) and support to help parents cope may have assisted families. However, we acknowledge the possibility that the association between parent mental health symptoms and child mental health symptoms may be representative of parents providing higher ratings of their child’s symptoms in the context of their own symptoms (Becker-Haimes et al., 2017). Collecting self-reported data would overcome this issue in future research.
Children with a close contact with COVID-19 experienced higher levels of anxiety symptoms and depressive symptoms, suggesting screening children and young people for mental health difficulties following a COVID-19 diagnosis of a close contact may be worthwhile to determine whether additional support is warranted. Children who asked more frequent questions about COVID-19 were reported to have higher levels of emotional symptoms, anxiety symptoms and depressive symptoms. This result is perhaps unsurprising and shows that children who worried more were more likely to ask questions about COVID-19 (or seek reassurance about it). Nevertheless, this finding highlights that parent-reported youth internalising symptoms were, in part, related to the pandemic itself.
In contrast to research outside of Australia (Barendse et al., 2021), neither severity of government restrictions nor self-isolation status were associated with child and adolescent mental health symptoms. However, total number of days in lockdown were significantly associated with conduct problems. This result is consistent with research in the United Kingdom which showed that conduct problems in children and adolescents increased as restrictions continued (Raw et al., 2021). The lack of association between severity and length of government restrictions on child and adolescent mental health symptoms may reflect that the impact of restrictions on known risk factors (e.g. financial hardship) were more relevant for understanding how lockdown impacted child and adolescent mental health than the restrictions themselves.
This study has some limitations. The sample was non-representative and biased towards families with Oceanian backgrounds from metro areas. We did not obtain pre-pandemic data so we cannot comment on changes in mental health symptoms because of the pandemic. We used a measure (RCADS25P) which has not been validated for young children (below 7 years old). Results were similar when we excluded these children; however, future research might benefit from including a measure for anxiety and depressive symptoms developed and validated for younger children (e.g. Preschool Anxiety Scale (PAS); Spence et al., 2001). Finally, we did not assess the presence of mental health disorders using diagnostic classifications. Incorporating diagnostic measures is required to determine the full impact of COVID-19 on mental health in child and adolescent samples.
These findings have important implications. First, expansion of mental health services for children and adolescents during the pandemic – particularly for those with pre-existing vulnerabilities – was important to mitigate the effects on child and adolescent mental health. Youth mental health services were overburdened early on (Young, 2020), and despite a move to the use of telehealth, more could be done to increase efficiencies in the delivery of mental health services, such as the increased use of evidence-based digital interventions (Spence et al., 2011). Second, the need for additional parent mental health support is highlighted, particularly for parents of younger children who struggled with the challenges of balancing children’s home learning and work during lockdowns. The provision and accessibility of parenting interventions which target child behavioural difficulties are recommended in any future lockdowns, given the rise in conduct problems in younger children (Piotrowska et al., 2020). Finally, a focus on the prevention of mental health difficulties and encouraging help-seeking behaviours in youth, particularly in times of crisis, may also be necessary.
In conclusion, parent-reported child and adolescent mental health symptoms were high during the initial stages of the COVID-19 pandemic in Australia. Mental health symptoms were greater in those with pre-existing vulnerabilities and whose parents had experienced greater psychological distress and financial hardship. Our findings highlight the need for targeted and adequate support for Australian youth and their families during the pandemic and beyond to reduce the burden of mental health difficulties.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221090174 – Supplemental material for Mental health symptoms in children and adolescents during COVID-19 in Australia
Supplemental material, sj-docx-1-anp-10.1177_00048674221090174 for Mental health symptoms in children and adolescents during COVID-19 in Australia by Gemma Sicouri, Sonja March, Elizabeth Pellicano, Alex C De Young, Caroline L Donovan, Vanessa E Cobham, Arlen Rowe, Simon Brett, Jeremy K Russell, Laura Uhlman and Jennifer L Hudson in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We thank Emily Daniel for assisting with collecting information, including her work developing the stage of lockdown variable.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.P. reports occasional fees for workshops and invited addresses, and grants from the Australian Research Council, Medical Research Future Fund (Australia), the Cooperative Research Centre for Living with Autism (‘Autism CRC’; Australia), the National Health and Medical Research Council (Australia), Positive Partnerships (Australia) and the European Commission, outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: G.S. was supported by a Macquarie University Research Fellowship for the duration of this project (MQIRGR0001041). E.P. was supported by an Australian Research Council Future Fellowship (FT190100077) for the duration of this project. S.M., C.D., V.C., A.R., J.R. and L.U. acknowledge funding provided by the Medical Research Future Fund through the Department of Health (APP1179490).
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.