
Abstract
Background:
Alcohol use disorder is associated with increased suicide risk; however, both alcohol use disorder and suicide share risk factors which must be accounted for in order to understand this relationship. This study aimed to explore the longitudinal relationship between alcohol use disorder and suicidal ideation in adulthood, while accounting for both child background and adult covariate factors.
Method:
Data were collected from the Christchurch Health and Development Study, a birth cohort of 1265 children born in Christchurch (New Zealand) in mid-1977. Alcohol use disorder (operationalised as alcohol abuse and alcohol dependence) was quantified between age 18 and 40 in five data waves. The outcome measure suicidal ideation was reported over the same time periods. Childhood confounding variables were controlled for, as well as time-dynamic covariates collected in adulthood, including internalising disorders, distress due to relationship dissolutions and other substance use disorders.
Results:
The association between alcohol abuse and suicidal ideation was not statistically significant before or after adjusting for childhood confounding and adulthood covariate factors, when compared to no alcohol disorder. However, the association between alcohol dependence and suicidal ideation was significant both before and after adjustment (unadjusted odds ratio = 2.89, 95% confidence interval = [2.09, 3.99]; adjusted odds ratio = 1.52, 95% confidence interval = [1.04, 2.23]), when compared to no alcohol disorder. Furthermore, alcohol dependence remained significant when compared to alcohol abuse (unadjusted odds ratio = 2.33, 95% confidence interval = [1.61, 3.37]; adjusted odds ratio = 1.54, 95% confidence interval = [1.00, 2.37]).
Conclusion:
This analysis found an association between alcohol dependence and suicidal ideation within a New Zealand birth cohort, which persists even after adjustment for childhood confounding and adulthood covariate factors. Given the high rates of suicide and heavy drinking within the New Zealand population, any comprehensive national or regional suicide prevention plan should seek to reduce risky alcohol consumption at an individual and population level, as this represents a modifiable risk factor for suicide.
Introduction
Suicide is an ongoing public health issue, with almost 700,000 deaths worldwide annually (World Health Organization, 2021). An individual’s risk of suicide is complex and is influenced by the interaction of many different contributory factors. Among the most consistently established risk factors are alcohol use disorders (Norström and Rossow, 2016; Roerecke and Rehm, 2014), which constitute the second largest contribution to overall suicide risk after major depressive disorder (Pompili et al., 2010). Although formerly separated into diagnoses of alcohol abuse (meeting one or more of the four abuse criteria within a 12-month period) or alcohol dependence (meeting three or more of the seven dependence criteria within the same 12-month period), these disorders have since been aggregated into a single diagnosis (American Psychiatric Association, 1994, 2013); herein referred to collectively as alcohol use disorders (AUD). Their role as a key risk factor for suicide exists at both a proximal level, with heavy alcohol consumption being reported among many suicide deaths, and at a distal level, with lifetime rates of suicide being higher among those with a history of AUD (Edwards et al., 2020).
Suicidal ideation is more common than suicide, but represents a key risk factor within an ideation-to-action framework (Klonsky and May, 2014). Suicidal ideation is also closely linked to AUD, with a meta-analysis indicating that AUD almost doubles the likelihood of suicidal ideation (Darvishi et al., 2015). There are many possible explanations for this relationship, with one being the frequent comorbidity of AUD and mood disorders such as depression and bipolar disorder, both of which are associated with suicidal thoughts and behaviours (Oquendo et al., 2000; Sung et al., 2016). Another possibility is that AUD generates or compounds known risk factors for suicide, such as financial hardship and loss of close relationships (Boden et al., 2013; Pompili et al., 2010). In addition, heavy alcohol use by those with AUD may result in cognitive impairments (Bernardin et al., 2014), which may increase the likelihood of suicidal ideation by weakening problem solving and coping abilities (Lara et al., 2014). Although a recent meta-analysis identified nine cohort studies which examined the relationship between suicidal ideation and AUD (Darvishi et al., 2015), most of these studies recruited participants beyond age 16, limiting the ability to adjust for key background and intervening factors. In addition, many studies assessed participants over relatively limited time periods during adulthood, preventing a detailed examination of longitudinal associations between AUD and suicidal ideation at different ages, and of the trajectory of alcohol/suicide associations over the lifecourse. Finally, almost half involved only male participants and are thus not representative of the general population.
It is important to consider the likelihood of increased risk of suicidal ideation or behaviours among populations where heavy alcohol consumption is common. One such country is New Zealand, where recent findings indicate that around 21% of adults meet hazardous drinking criteria (New Zealand Ministry of Health, 2020). In this context, hazardous drinking was defined as an Alcohol Use Disorders Identification Test (AUDIT) score of 8 or more, which indicates drinking in a manner that could harm the individuals or others (New Zealand Ministry of Health, 2020). Suicide is also a major public health issue within New Zealand, with teenage suicide rates in particular being among the highest of all OECD countries (Gluckman, 2017). Although alcohol misuse is highlighted by the World Health Organization as a major modifiable risk factor for suicide prevention (World Health Organization, 2018b), few New Zealand studies have examined the relationship between alcohol and suicidal ideation or behaviours, and the current National Suicide Prevention Strategy has not suggested any alcohol-related interventions (New Zealand Ministry of Health, 2019).
When seeking to elucidate the relationship between AUD and suicidal ideation, known shared risk factors for both AUD and suicide should be accounted for. Additionally, because both childhood and adulthood factors are associated with AUD and suicide, longitudinal birth cohort studies are particularly well suited to explore these factors. Accordingly, the aims of this study are to explore the relationship between AUD (both abuse and dependence) and suicidal ideation in a manner which considers important confounding and potentially intervening factors, including whether findings varied by sex and ethnicity, in a representative sample of New Zealand individuals. To achieve this, we used data from the Christchurch Health and Development Study (CHDS). Using regularly collected data on alcohol abuse and dependence, suicidal ideation, and a number of potential confounding and intervening factors, this analysis seeks to investigate whether alcohol abuse or dependence is associated with suicidal ideation and to explore the utility of covariate factors to adjust the associations, as well as interactions of both sex and ethnicity with alcohol abuse and dependence. More broadly, the goal of the analysis is to identify whether AUD should be a target area for suicide prevention in New Zealand.
Method
Participants
Participants were members of the CHDS birth cohort. The CHDS is a prospective longitudinal study of 1265 children (630 females) born in Christchurch, New Zealand over a 4-month period during 1977. This cohort has been studied regularly from birth to age 40 using a combination of interviews with parents and cohort members, standardised testing, teacher reports and official record data (Fergusson and Horwood, 2001, 2013). All phases of the study have been subject to ethical approval by the Regional Health and Disabilities Ethics Committee.
Main outcome and exposure measures
Suicidal ideation (18–40 years)
At ages 21, 25, 30, 35 and 40 years, cohort members were questioned using custom-written survey items about whether they had ever thought about killing themselves or had attempted suicide since the previous assessment. Using this information, respondents were classified on a dichotomous measure reflecting whether they reported any suicidal ideation for the intervals: ages 18–21, 21–25, 25–30, 30–35 and 35–40 years (Fergusson et al., 2008).
Alcohol use disorders (alcohol abuse and dependence) (18–40 years)
At ages 21, 25, 30, 35 and 40 years, cohort members were interviewed about alcohol use since the previous assessment. Interviews used components of the Composite International Diagnostic Interview (CIDI; World Health Organization, 1994) to assess Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) (American Psychiatric Association, 1994) symptom criteria for alcohol abuse and alcohol dependence. From this information, respondents were classified as either those having no alcohol abuse or dependence, those meeting criteria for DSM-IV alcohol abuse or those meeting criteria for DSM-IV alcohol dependence, for the intervals: ages 18–21, 21–25, 25–30, 30–35 and 35–40 years. These classifications enabled assessment of two levels of severity of disorder.
Childhood confounding factors
A number of candidate predictor variables were selected for the analysis from the CHDS database on the basis of previous research and theory, given their known association with both AUD and suicide (Deeken et al., 2020; Turecki et al., 2019). Additional predictor variables are described in the Online Supplement.
Māori ethnicity at birth
When the cohort members were enrolled in the study, their parents were asked to indicate whether the cohort member had any Māori ancestry. Those whose parents indicated that they did were coded as New Zealand Māori. Cohort members were classified on a dichotomous measure reflecting whether the respondent was identified as Māori (11.2%) or another ethnicity at birth.
Family socioeconomic status at birth
Family socioeconomic status at the time of the child’s birth was assessed using the Elley and Irving scale of socioeconomic status for New Zealand (Elley and Irving, 1976). This index ranks families into six levels on the basis of paternal occupation. For this analysis, the scale was reverse coded and collapsed into three levels as follows: (a) Levels 1–2 (semi-skilled, unskilled, unemployed), (b) Levels 3–4 (clerical, technical, skilled) and (c) Levels 5–6 (professional, managerial).
Family standard of living (0–10 years)
Interviewer ratings of family living standards were obtained at every year when the survey child was aged 1–10 years. In these ratings, the family’s living standards were assessed by the interviewer on a 5-point scale that ranged from ‘very good’ to ‘very poor’, based on their impressions of the interior and exterior of the accommodation. To create an overall scale score, these ratings were reverse coded and summed over the 10-year period and averaged to obtain an assessment of family living standards during childhood.
Childhood sexual abuse (<16 years)
At ages 18 and 21 years, cohort members reported on their exposure to any form of childhood sexual abuse prior to age 16 years, including (a) non-contact episodes involving indecent exposure, public masturbation or unwanted sexual propositions; (b) episodes involving sexual contact in the form of sexual fondling, genital contact or attempts to undress the respondent; and (c) episodes involving attempted or completed vaginal, oral or anal intercourse (Fergusson et al., 1996, 2000). Using these reports, respondents were classified into a single 4-point scale reflecting the most severe form of abuse exposure reported at either 18 or 21 years. This classification was: no childhood sexual abuse, non-contact childhood sexual abuse, contact childhood sexual abuse not involving attempted or completed sexual penetration, and severe childhood sexual abuse involving attempted or completed sexual penetration.
Childhood physical punishment (<16 years)
At ages 18 and 21 years, cohort members reported on the extent to which their parents used physical punishment or maltreatment during their childhood (prior to age 16 years). Respondents indicated whether parents never used physical punishment, parents seldom used physical punishment, at least one parent regularly used physical punishment and at least one parent used frequent or severe punishment or treated the respondent in a harsh/abusive manner (Fergusson and Lynskey, 1997). These answers were then combined into a single 4-point scale of parental physical punishment or maltreatment, based on the most severe rating at either the 18- or 21-year interview.
Childhood neglect (<16 years)
At age 40, cohort members were questioned about the presence of emotional neglect (i.e. ‘Did your parents/guardians understand your problems/worries?’) and physical neglect (i.e. ‘How often did you parents/guardians not give you enough food even when they could easily have done so?’) during their childhood, prior to 16 years of age. The scale developed used items from the Adverse Childhood Experiences International Questionnaire (ACE-IQ) (World Health Organization, 2018a). Respondents’ responses to physical neglect questions were reverse coded and all responses were categorised into a 4-point scale: no neglect, neglectful some of the time, neglectful most of the time and severe neglect.
Number of changes of parents (<16 years)
Comprehensive data on the child’s family placement and changes of parents were collected at annual intervals from birth to age 16 years. To assess the extent of parental change, a measure of the child’s exposure to parental change was constructed by counting the number of changes of parent(s) from birth to 16 years. Changes of parents included all changes resulting from parental separation/divorce, reconciliation, remarriage, death of a parent, fostering and other changes of custodial parents.
Parental history of alcohol misuse (15 years)
When the sample members were aged 15, their parents were questioned regarding whether any parent had a history of alcohol misuse. From this information, dichotomous variables were constructed representing whether or not the respondents’ parent(s) reported a history of alcohol misuse.
Parental history of criminal offending (15 years)
At the age 15 assessment, parents were questioned regarding any criminal offending history of either parent. From this information, dichotomous variables were constructed representing whether or not the respondents’ parent(s) reported a history of criminal offending.
Inter-parental violence (<16 years)
The reported experience of inter-parental violence during childhood (prior to age 16 years) was assessed via cohort members’ self-reports at age 18, through a series of eight items derived from the Conflict Tactics Scale (Straus, 1979). The eight items used included (1) threaten to hit or throw something; (2) push, grab or shove other parent; (3) slap, hit or punch other parent; (4) throw, hit, kick or smash something (in the other parent’s presence); (5) kick the other parent; (6) choke or strangle other parent; (7) threaten other parent with a knife, gun or other weapon; and (8) call other parent names or criticise other parent (or put other parent down). Each item was scored in dichotomous (absent/present) form and a score for the scale was created from the sum of these items.
Time-varying covariate factors
Covariate factors collected in adulthood and included in the analysis were time dynamic and measured concurrently with the exposure and outcome variables.
Welfare dependence
During interviews at ages 21, 25, 30, 35 and 40 years, cohort members were questioned about any times when they received a government income-tested benefit of job seeker support, sole-parent support or a supported living allowance since the previous interview. Using this information, responses were dichotomised to represent whether the cohort member had received a welfare benefit, during any of the 18–21, 21–25, 25–30, 30–35 and 35–40 year intervals.
Full-time employment
During interviews at ages 21, 25, 30, 35 and 40 years, cohort members were asked if they were currently in paid employment. Responses were dichotomised to represent whether the participants worked 30 hours or more per week, or 29 hours or less per week, at each age.
Adulthood internalising disorders
At ages 21, 25, 30, 35 and 40 years, cohort members were questioned about symptoms of major depression and a range of anxiety disorders (generalised anxiety disorder, panic disorder, agoraphobia, social phobia, specific phobia) since the previous assessment. Questioning was based on the relevant components of the CIDI (World Health Organization, 1994) and DSM-IV criteria (American Psychiatric Association, 1994). Using this information, separate dichotomous measures were constructed to reflect whether the respondent met the diagnostic criteria for a major depressive episode and/or any anxiety disorder for the intervals 18–21, 21–25, 25–30, 30–35 and 35–40 years.
Cannabis and other illicit substance use disorders
At ages 21, 25, 30, 35 and 40 years, the cohort members were questioned about their use of psychoactive substances since the previous assessment. These questions included several illegal substances available within New Zealand, including cannabis. The questions regarding the use of individual classes of substances were non-specific to allow comparison across assessment periods. If the respondents reported using any of these substances, they were also asked about symptoms of cannabis dependence or other illicit substance dependence using questions based on the generic DSM-IV criteria for substance dependence derived from the CIDI (Boden et al., 2006; World Health Organization, 1994). This information was used to generate a dichotomous measure reflecting whether the respondent reported an illicit substance use disorder during any of the 18–21, 21–25, 25–30, 30–35 and 35–40 year intervals.
Nicotine dependence
At ages 21, 25, 30, 35 and 40 years, the cohort members were questioned about their use of tobacco since the previous assessment. The questions assessed tobacco use disorders using the relevant components of the CIDI (World Health Organization, 1994) and DSM-IV (American Psychiatric Association, 1994) criteria. This variable was dichotomised based on whether or not the respondent had met the criteria for DSM-IV nicotine dependence during any of the 18–21, 21–25, 25–30, 30–35 and 35–40 year intervals.
Life satisfaction
At ages 21, 25, 30, 35 and 40 years, information about life satisfaction was collected using a custom-written questionnaire which required cohort members to rate their current satisfaction with each of 11 areas of their life: work; leisure time; partner relationships; relationships with people of the same sex; relationships with people of the opposite sex; social life; money; independence; daily interactions with others; the future; and life as a whole. Cohort members responded on a 4-point scale where ‘1’ was very unhappy; ‘2’ was unhappy; ‘3’ was happy; and ‘4’ was very happy. These 11 items were summed to provide life satisfaction scores for each age.
Dependent children
The number of dependent children who were both living in the same household and parented by the respondent was recorded at ages 21, 25, 30, 35 and 40-year assessments. This variable included children who were over the age of 16. This information was used to create a dichotomous variable representing whether the participant reported one or more dependent child(ren) at each assessment.
Cohabiting partner relationships
At ages 21, 25, 30, 35 and 40 years, the cohort members were asked whether they had a current cohabiting partner. This information was used to generate a dichotomous measure reflecting whether the respondent reported a cohabiting partner at each assessment.
Distress after relationship dissolution
At ages 21, 25, 30, 35 and 40 years, cohort members were asked whether they had separated from a partner/spouse since the previous interview. If the respondent answered yes to this question, they were also asked ‘How distressed were you by this event?’ where 0 = no event; 1 = not upset/distressed; 2 = a little upset/distressed; 3 = moderately upset/distressed; 4 = very upset/distressed. Using this information, a score was obtained to represent cohort members’ level of distress after relationship dissolution for each of the 18–21, 21–25, 25–30, 30–35 and 35–40 year intervals.
Statistical methods
Unadjusted associations
The repeated observations between AUD (classified as no alcohol abuse/dependence, DSM-IV alcohol abuse, DSM-IV alcohol dependence) and suicidal ideation during the intervals at ages 18–21, 21–25, 25–30, 30–35 and 35–40 years were pooled to obtain an estimate of the population-averaged associations. Associations between the classified AUD and the dichotomous outcome suicidal ideation (18–40 years) were tested for statistical significance using a generalised estimating equation (GEE) logistic regression modelling approach (Zeger and Liang, 1986a, 1986b) in which suicidal ideation was modelled as a function of classified AUD and age. Because the association between AUD and suicidal ideation was non-linear, alcohol abuse/dependence was treated as a categorical variable and modelled in a way that separated the different levels of alcohol use disorders. Pairwise comparisons of suicidal ideation across the different levels of AUD were examined (alcohol abuse vs none; alcohol dependence vs none; alcohol abuse vs alcohol dependence).
Adjusting for covariate factors
Associations between AUD and the potential covariate factors are reported in Tables 2 and 3. It should be noted that the selected covariates were dichotomised for Tables 2 and 3 for ease of description and presentation. For Table 2, the dichotomised covariates were tested for strength, direction and statistical significance with the categorical AUD measure by using Spearman’s rank correlation coefficient test. For Table 3, the dichotomised time-varying covariate factors were tested for statistically significant associations with alcohol use disorders using the population-averaged repeated-measures logistic regression framework described above.
The unadjusted regression model reported in Table 1 was extended to include the statistically significant covariates from Tables 2 and 3, using forward and backward selection processes to refine the model. All covariate factors selected in the model fitting process were included in their natural metric. The fitted model (Table 4) reports B (SE), p and odds ratios (95% confidence intervals) for the dichotomous suicidal ideation outcome by the categorical AUD measures.
Suicidal ideation by DSM-IV alcohol abuse and dependence status (collectively alcohol use disorders [AUD]), across assessment intervals 18–21, 21–25, 25–30, 30–35 and 35–40 years, and pooled across observations 18–40 years.
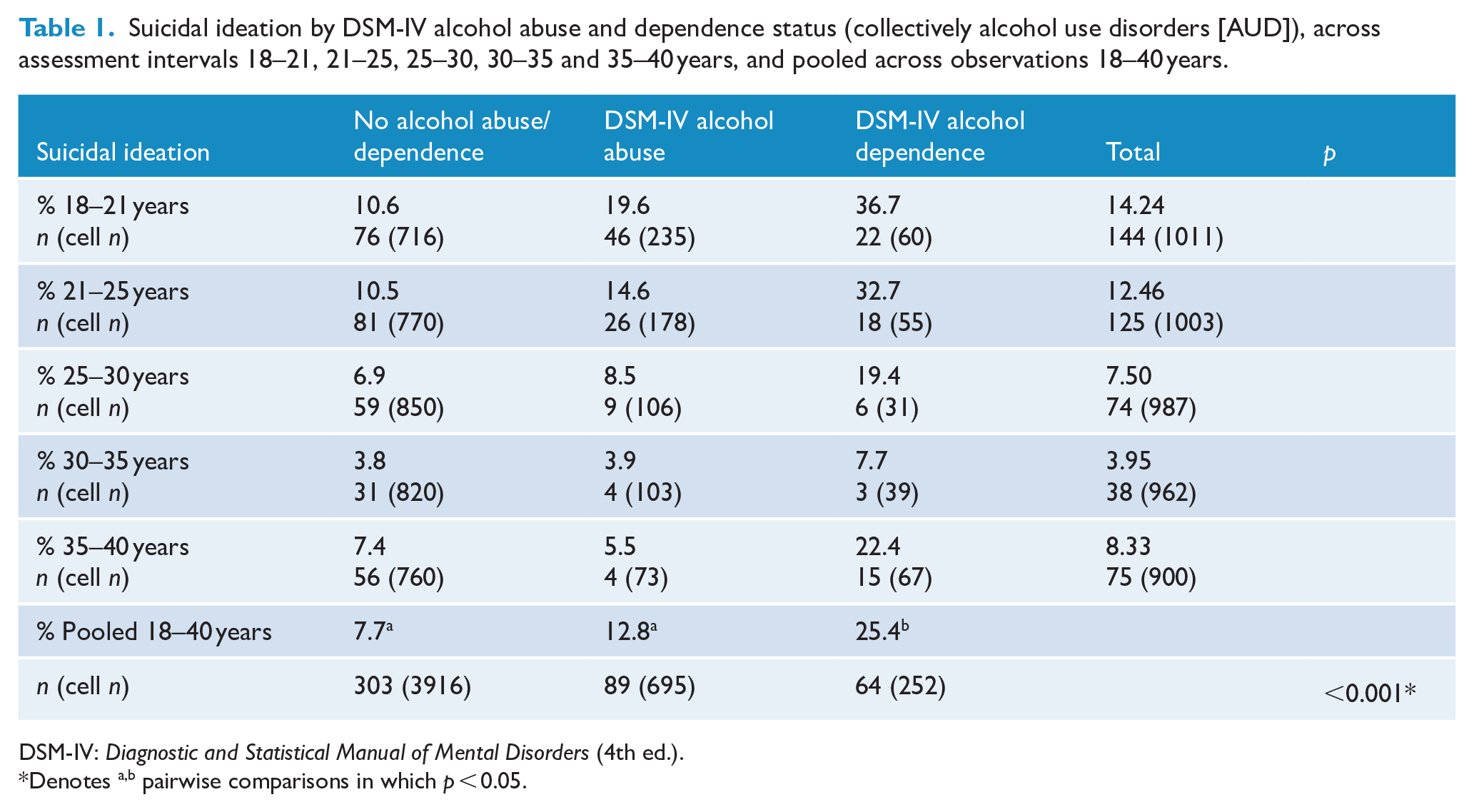
DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.).
Denotes a,b pairwise comparisons in which p < 0.05.
Associations between potential childhood confounding factors and alcohol use disorders (AUD), pooled across observations 18–40 years.
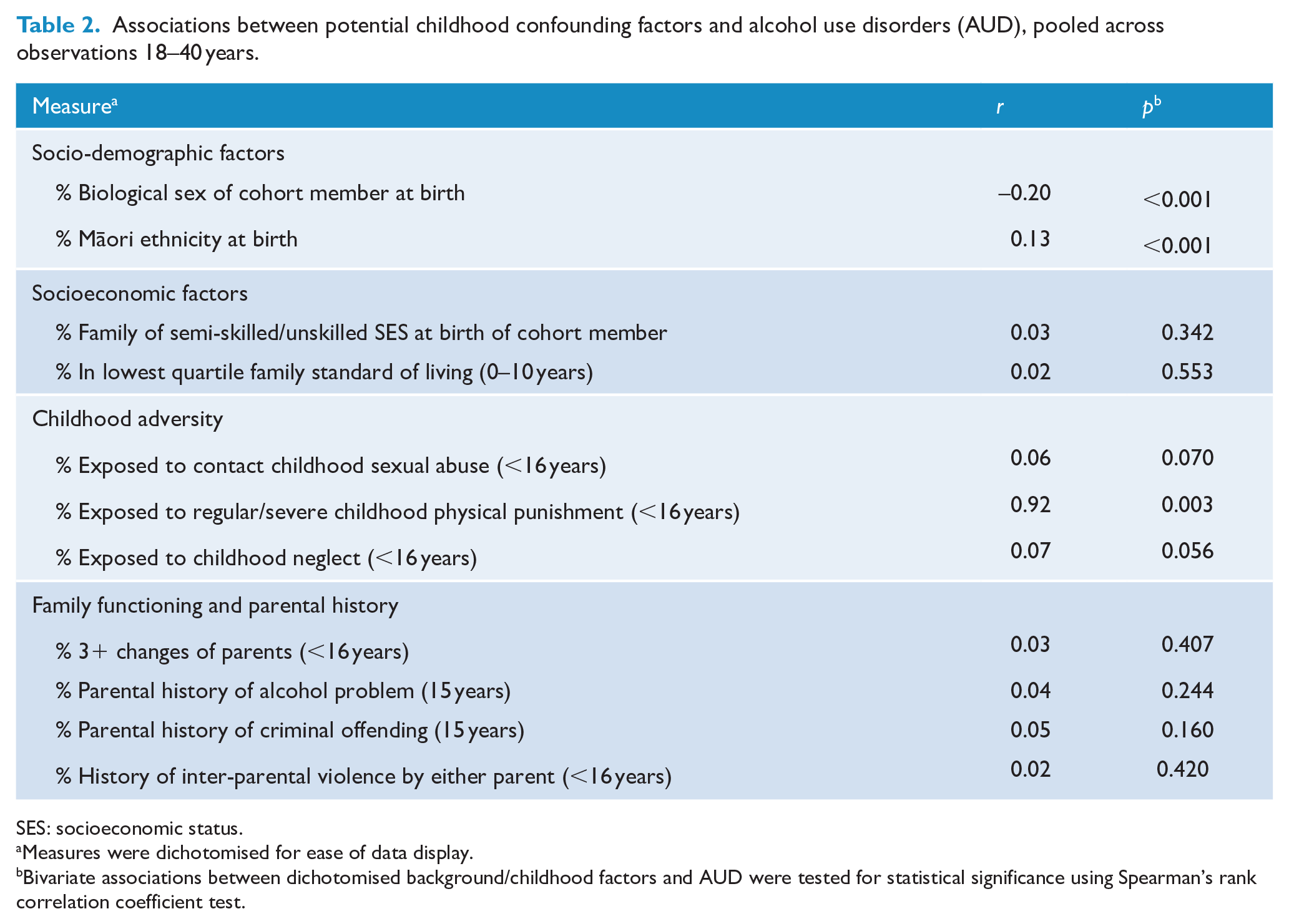
SES: socioeconomic status.
Measures were dichotomised for ease of data display.
Bivariate associations between dichotomised background/childhood factors and AUD were tested for statistical significance using Spearman’s rank correlation coefficient test.
Time-varying covariate factors by alcohol use disorders (AUD), pooled across observations 18–40 years.
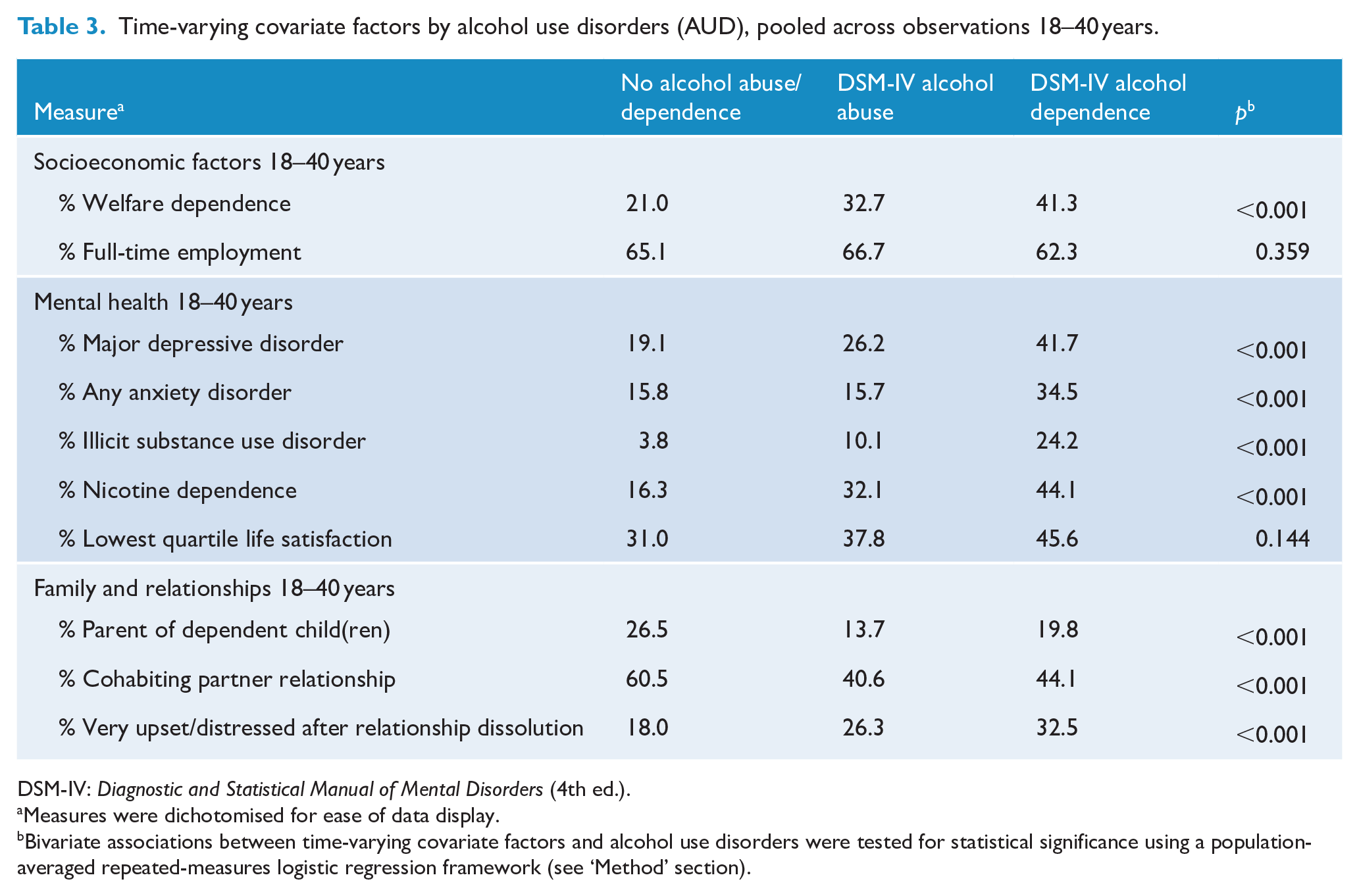
DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.).
Measures were dichotomised for ease of data display.
Bivariate associations between time-varying covariate factors and alcohol use disorders were tested for statistical significance using a population-averaged repeated-measures logistic regression framework (see ‘Method’ section).
Associations between alcohol use disorders (AUD) and suicidal ideation pooled across observations 18–40 years, unadjusted and adjusted for confounding and covariate factors.
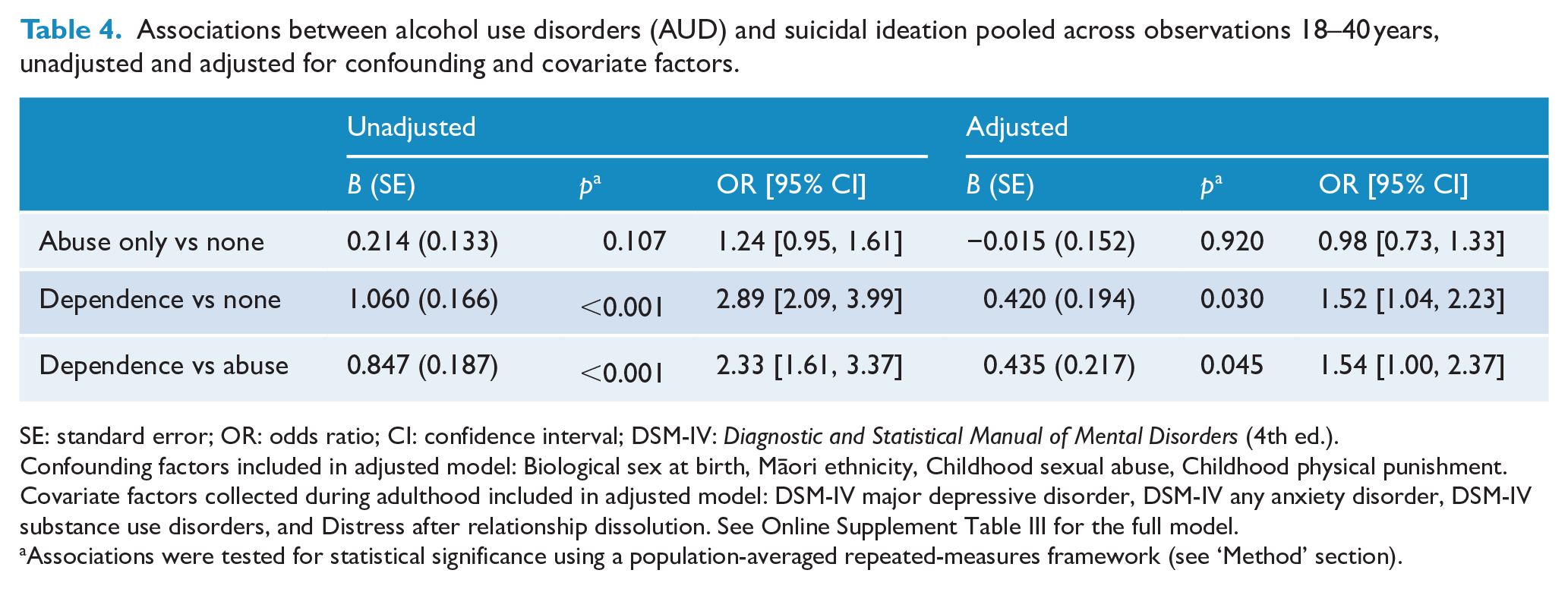
SE: standard error; OR: odds ratio; CI: confidence interval; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.).
Confounding factors included in adjusted model: Biological sex at birth, Māori ethnicity, Childhood sexual abuse, Childhood physical punishment. Covariate factors collected during adulthood included in adjusted model: DSM-IV major depressive disorder, DSM-IV any anxiety disorder, DSM-IV substance use disorders, and Distress after relationship dissolution. See Online Supplement Table III for the full model.
Associations were tested for statistical significance using a population-averaged repeated-measures framework (see ‘Method’ section).
Sex and ethnicity interactions
To examine whether the associations between AUD and suicidal ideation varied between males and females or between Māori and non-Māori, the covariate-adjusted models were extended to include multiplicative biological sex × AUD and ethnicity × AUD interaction terms.
Statistical significance for all tests was set at α = 0.05 for two-sided tests. Analyses were completed using SAS version 9.4 for Windows (SAS Institute Inc, 2012) and STATA 16 for Windows (StataCorp, 2019).
Sample size and sample bias
This analysis is based on data from respondents studied at age 21 years (n = 1011), age 25 years (n = 1003), age 30 years (n = 987), age 35 years (n = 962) and age 40 years (n = 904) for whom information was available on both AUD and suicidal ideation for at least one assessment from age 21 to 40 years. These samples represented between 74.0% and 81.5% of the participants surviving to age 21 years (n = 1240), age 25 years (n = 1234), age 30 years (n = 1231), age 35 years (n = 1223) and age 40 years (n = 1221). To examine whether selection bias due to the processes of sample attrition influenced the findings of this study, the data were re-analysed using a data-weighting method (Carlin et al., 1999). These analyses produced model parameters and tests of statistical significance that were essentially unaffected by missing data, suggesting the findings were unlikely to have been influenced by selection bias.
Results
Suicidal ideation and AUD
Table 1 shows the rates of suicidal ideation by AUD (classified on three levels of no alcohol abuse/dependence, DSM-IV alcohol abuse and DSM-IV alcohol dependence) pooled over the repeated observations obtained at 21, 25, 30, 35 and 40 years. At every assessment period, the frequency of those reporting suicidal ideation was highest among those who met the criteria for alcohol dependence during adulthood 18–40 years. While the rates of suicidal ideation declined as the cohort members aged, it can be seen that in general, the rates of suicidal ideation increased across the three AUD classifications. The only exception was the age 35–40 year assessment period in which the rate of suicidal ideation was lower for those classified DSM-IV alcohol abuse than those with no alcohol abuse/dependence. The associations between AUD and suicidal ideation were analysed by fitting a population-averaged regression model to the pooled data, in which suicidal ideation was modelled as a dichotomous function of AUD classified on three levels (see ‘Method’ section). Table 1 reports the pooled rate of suicidal ideation for each level of AUD and the test of statistical significance (p-value). The results show a statistically significant association (p < 0.001) such that increasing severity of AUD is associated with increasing suicidal ideation. Suicide attempt was not included in the modelling due to low prevalence; however, these results are provided for descriptive purposes in the Online Supplement (Table I).
Childhood/background factors and AUD
Table 2 shows the associations between AUD and a series of dichotomised potentially confounding childhood factors (see ‘Method’ section). Statistically significant bivariate associations (p < 0.003) with AUD were found for biological sex, Māori ethnicity and childhood physical punishment. The table shows that cohort members classified as having more severe AUD were likely to be male, be identified as Māori ethnicity at birth and have experienced regular/severe physical punishment as a child. The results of the analysis show that the associations varied from small to large in magnitude (r = 0.13, r = 0.92). Online Supplement Table II shows bivariate associations between additional childhood/background factors and AUD; none of which were statistically significant.
Time-varying covariate factors and AUD
Table 3 shows the associations between potential time-varying covariate factors gathered in adulthood and AUD (both alcohol abuse and dependence). The table shows that all factors spanning socioeconomic factors, mental health, family and relationships (18–40 years) were statistically significantly associated with AUD (p < 0.001) with the exception of full-time employment and life satisfaction. The analysis shows that cohort members classified as having more severe AUD (i.e. alcohol dependence) were likely to be experiencing higher rates of adverse socioeconomic circumstances, mental health problems and lower relationship quality.
Regression analyses
Taking into account the correlated effects of the statistically significant factors in Tables 2 and 3, the regression model in Table 1 was extended to incorporate these factors as covariates (see ‘Method’ section). Table 4 summarises the results of the analysis showing B (SE), p and odds ratios (95% confidence intervals) for the dichotomous suicidal ideation outcome by the categorical AUD measure (no alcohol abuse/dependence, alcohol abuse, alcohol dependence).
Table 4 shows that while the associations between alcohol abuse and suicidal ideation were not statistically significant before adjusting (p = 0.107) or after adjusting (p = 0.920) for childhood confounding and adult covariate factors, the association between alcohol dependence and suicidal ideation was significant before adjusting (p < 0.001) and after adjusting (p = 0.030) for these factors. Finally, the table shows that the association between alcohol dependence and suicidal ideation was also statistically significant both before adjusting (p < 0.001) and after adjusting for covariates (p = 0.045) when compared to alcohol abuse. The table shows that, after adjustment, those who met the criteria for alcohol dependence at some point during the period 18–40 years had a likelihood of suicidal ideation that was approximately 1.5 times higher than those who did not meet the criteria for an alcohol use disorder. Furthermore, those who met the criteria for alcohol dependence also had a likelihood of suicidal ideation that was approximately 1.5 times higher than those who met the criteria for alcohol abuse. The full model is reported in the Online Supplement Table III. This shows that after adjustment, the strongest effect was observed for major depression (adjusted B = 1.824, p < 0.001), followed by any anxiety disorders (adjusted B = 0.974, p < 0.001). No statistically significant interactions were identified (p < 0.05) when the covariate-adjusted models were extended to include multiplicative tests of sex × alcohol abuse/dependence and ethnicity × alcohol abuse/dependence interaction terms.
Discussion
Using data from the CHDS cohort, the present study aimed to identify whether either of DSM-IV alcohol abuse or dependence were associated with contemporaneous suicidal ideation during adulthood, and to investigate the role of confounding and covariate factors within this association. Throughout adulthood, alcohol abuse and, in particular, alcohol dependence were associated with suicidal ideation. Subsequent logistic regression modelling demonstrated that this relationship was robust for alcohol dependence but not for alcohol abuse and remained significant for alcohol dependence after adjusting for relevant confounding and intervening factors when compared to both no abuse/dependence and alcohol abuse. These findings highlight the importance of taking AUD severity into account when considering suicide risk. DSM-IV alcohol abuse has typically been regarded as a prerequisite to the more severe alcohol dependence category, which involves physiological symptoms associated with tolerance and withdrawal. Consistent with the present study, previous research has identified that risk of suicidal ideation and suicide attempt is influenced by the severity of AUD (Hoertel et al., 2018; Yaldizli et al., 2010) and by drinking intensity among those with AUD (Conner et al., 2003). Furthermore, a retrospective study of suicides identified DSM-IV alcohol dependence in 51% of cases, but DSM-IV alcohol abuse in only 10% of the cases (Kõlves et al., 2006).
In the present study, major depression was the strongest covariate in the adjusted relationship between AUD and suicidal ideation. Within this cohort, there is an established causal pathway from AUD to major depression, with the presence of alcohol abuse or dependence approximately doubling the likelihood of subsequently developing major depression (Fergusson et al., 2009). International research has consistently identified major depressive disorder as a key risk factor for suicidal ideation (Nock et al., 2008; Omary, 2021). Given the aforementioned linkages, the present findings support the hypothesis that alcohol dependence may also indirectly influence suicidal ideation through its contribution to the maintenance of major depressive disorder. While having a weaker effect within this model than major depressive disorder, anxiety disorders were also a key intervening factor; a result which is consistent with findings that within this cohort, there is a bidirectional association between alcohol use and anxiety disorder (Fergusson et al., 2011). While anxiety disorders have independently been linked to suicide attempts (Sareen et al., 2005), the present findings also suggest the possible role of alcohol use disorders in this relationship; this hypothesis justifies further investigation. While males in this cohort were more likely to meet criteria for AUD, there was no significant interaction by biological sex in the relationship between AUD and suicidal ideation, suggesting that AUD represents a risk factor for suicidal ideation for both males and females. While this study was not designed to examine the relationship between alcohol dependence and suicidal ideation specifically in females, future research could test whether sex-specific differences in associations and covariates exist. Similarly, there was no interaction observed for ethnicity; collectively this suggests that these findings are generalisable across the New Zealand population.
There are a number of limitations to consider when evaluating these findings. First, it was not practical to model suicide attempt or completed suicide given their lower incidence within this cohort. Consequently, focusing only on suicidal ideation also limits the extent to which risk of suicide itself can ultimately be inferred. In addition, these analyses focused upon associations between AUD and suicidal ideation over time, but did not aim to determine directionality or causal pathways. Having established an association, these may be valuable future research questions. Finally, although a number of potential confounding and covariate factors were examined during these analyses, the possibility of unobserved confounding factors cannot be entirely discounted.
Regardless of the above limitations, the present findings have pertinent implications for clinical treatment, alcohol policy and suicide prevention strategies. At an individual level, these findings suggest that screening for AUD should be undertaken for anyone presenting to healthcare services with suicidal ideation, and additionally, those diagnosed with AUD should be screened consistently for the emergence of suicidal ideation and suicide risk. Although there is not currently strong evidence for therapeutic interventions related to alcohol which reduce suicidal ideation, there is evidence that individual-level interventions to limit alcohol use may reduce risk of suicide attempt (Witt et al., 2021). Thus, alcohol-related interventions may reduce suicide risk for an individual, although much work is needed to optimise clinical practice and interventions in this area (Witt et al., 2021). Finally, while the study was conducted on a New Zealand birth cohort, the findings may have broader application internationally.
In multiple nations, systematic reviews have concluded that tighter regulation of alcohol has been followed by a marked reduction in suicide rates (Kõlves et al., 2020; Xuan et al., 2016). The World Health Organization has outlined a suite of policies to reduce harmful use of alcohol as a means of preventing suicide, including addressing issues such as alcohol availability, pricing policy and alcohol marketing (World Health Organization, 2014). Two interventions that should be particularly considered for New Zealand are implementation of minimum unit pricing for alcohol or an increase to the excise tax, and an increase in the minimum drinking age, as there is evidence for both of these policies being associated with decreased suicide rates internationally (Kõlves et al., 2020; Xuan et al., 2016). Building social capital and political will for such changes will require increased awareness from the public and from policy makers that there is a relationship between AUD and suicide risk. In particular, communications and advocacy should be targeted to local councillors, as New Zealand has devolved alcohol licensing to local councils, and to the public, who may not be aware of the relationship between alcohol and suicide risk.
Given the high rates of suicide, heavy drinking and binge drinking within New Zealand (Gluckman, 2017; New Zealand Ministry of Health, 2020), any comprehensive national or regional suicide prevention plan should seek to reduce risky levels of alcohol consumption within the population. Alcohol consumption has been demonstrated to be positively associated with suicide rates across 183 countries (Kim, 2021); therefore, policies targeting alcohol consumption should be targeted as a means of reducing suicide. We recommend that suicide prevention strategies in New Zealand should acknowledge alcohol as a modifiable risk factor for suicide and include recommendations and actions for reducing harmful alcohol use at a population-level, as well as individual-level interventions described above. Such recommendations and actions should be consistent with World Health Organization guidance (World Health Organization, 2014) and previous New Zealand specific recommendations, such as the 2018 Mental Health and Addiction Inquiry, which noted that reducing alcohol consumption was a key priority for improving mental health (Patterson et al., 2018).
Future alcohol policy changes should be evaluated for subsequent impacts on suicide and suicidal behaviour, with consideration of the potential for age- and sex-specific effects. Within the CHDS cohort, the observed association between alcohol dependence and suicidal ideation should continue to be examined as the cohort go through their forties, when suicide rates may increase (New Zealand Ministry of Health, 2019). Further research with this cohort could provide opportunities to evaluate the impacts of any major alcohol policy changes or changes to alcohol consumption patterns on suicidal ideation. It would also enable consideration of changes in the relationship between alcohol dependence and suicidal ideation across the lifespan, which may be impacted by changes to relevant covariates such as family roles, family structure and employment status.
In conclusion, this research has highlighted a relationship between alcohol dependence and suicidal ideation within New Zealand, which persists even after adjustment for childhood confounding and adulthood covariate factors. Given the imperative to reduce suicide in New Zealand and elsewhere, alcohol use represents a modifiable risk factor that should be acted on at an individual and population level, taking into consideration local laws and contexts. Addressing these interlinked issues will require a systems-based response, with integration between strategies aimed at reducing alcohol-related harm and those addressing suicide prevention.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211064183 – Supplemental material for The association between alcohol use disorder and suicidal ideation in a New Zealand birth cohort
Supplemental material, sj-docx-1-anp-10.1177_00048674211064183 for The association between alcohol use disorder and suicidal ideation in a New Zealand birth cohort by Rose Crossin, Lana Cleland, Geraldine FH McLeod, Annette Beautrais, Katrina Witt and Joseph M Boden in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project was funded by the Oakley Mental Health Foundation, grant awarded to R.C. and J.M.B. The Christchurch Health and Development Study is funded by the Health Research Council of New Zealand (Grant number 16/600). K.W. is funded by a fellowship from the National Health and Medical Research Council of Australia.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.