
Abstract
Aims:
Services for individuals with a first episode of psychosis or at ultra-high risk of psychosis have become a treatment model of choice in mental health care. The longitudinal changes in clinical and functional outcomes as a result of real-world treatment remain under-reported.
Methods:
We analysed data from first episode of psychosis and ultra-high risk services delivered across Australian primary youth mental health care services known as headspace between 19 June 2017 and 30 September 2019. Outcome measures were completed and entered into a minimum dataset every 90 days a participant was receiving treatment and included psychiatric symptomatology (Brief Psychiatric Rating Scale and psychological distress, K10) and psychosocial functioning (Social and Occupational Functioning Assessment Scale and My Life Tracker). Linear mixed-effects models were used to evaluate changes in outcome over time.
Results:
Outcome data from a total of 1252 young people were evaluated (643 first episode of psychosis, 609 ultra-high risk). Of those who entered ultra-high risk services, 11.8% transitioned to first episode of psychosis services. Overall, substantial improvement in clinical (Brief Psychiatric Rating Scale, K10) and functional (Social and Occupational Functioning Assessment Scale, My Life Tracker) outcomes were seen across groups and outcomes. Ultra-high risk patients showed a greater reduction in distress symptoms, while first episode of psychosis patients experienced a greater reduction in positive psychosis symptoms. Although clinical outcomes showed a plateau effect after approximately 3 months of care, improvement in functional outcomes (Social and Occupational Functioning Assessment Scale, My Life Tracker) continued later in treatment.
Conclusion:
These findings support the use of real-time, real-world and low-cost administrative data to rigorously evaluate symptomatic and functional outcomes in early psychosis treatment settings. Findings that functional outcomes improve past the remittance of clinical outcomes also support the functional recovery focus of early psychosis services and remaining high levels of distress suggest the need for ultra-high risk services to extend beyond 6 months of care.
Keywords
Introduction
Early Intervention in Psychosis (EIP) services are widely accepted as a model of care that is both clinically and cost-effective at supporting individuals experiencing a first episode of psychosis (FEP). A 2018 meta-analysis demonstrated superior functional and symptomatic outcomes (Correll et al., 2018) and economic analyses frequently demonstrate cost-effectiveness (Mihalopoulos et al., 2009), particularly when considering the societal costs of untreated psychosis (Behan et al., 2019). EIP services are based on the principles of early detection, assessment and treatment, alongside treatment optimism, i.e. promoting recovery from psychosis. It has been proposed that one of the key ways that EIP services improve outcomes is by reducing the duration of untreated psychosis (DUP) an individual experiences before they receive treatment (Drake et al., 2020; McGorry et al., 2007; Marshall et al., 2014). DUP is found to reduce further when services also encompass the provision of ‘ultra-high risk (UHR)’ service, also known as the at-risk mental state (ARMS) or clinical high risk criteria (Miller et al., 2003).
One of the earliest proponents of EIP services was the Early Psychosis Prevention and Intervention Centre (EPPIC) established in 1992 in Melbourne, Australia and subsequently the Personal Assessment and Crisis Evaluation (PACE) Clinic for UHR individuals (McGorry et al., 1996; Yung et al., 2007), now part of the Orygen Specialist Program (formally known as Orygen Youth Health). However, the presence of similar specialist services across the rest of Australia has been slower to emerge, despite Australia being an early proponent of a broader primary early intervention model of mental health care, known as headspace (McGorry et al., 2014; Rickwood et al., 2019). Following the recognition of the need for specialist early psychosis services across the country (Williams et al., 2021), 2014 saw the commissioning of services based on the Australian Early Psychosis Model to be delivered through headspace. This headspace Early Psychosis (hEP) programme was established in 14 headspace centres in six key clusters across the states and territories of Australia; South East Melbourne, Western Sydney, North Perth, Adelaide, South East Queensland and Darwin and are situated in large, mostly metropolitan areas.
To ensure the effectiveness of these services being delivered and to monitor important outcomes, enhancements were made to the existing headspace minimum dataset to allow for the routine collection of key service and outcome data (Rickwood et al., 2014). To date, outcome data on first episode cohorts is dominated by the results of research studies rather than prospectively collected routine clinical data. One quasi-real-world study of the impact of FEP services is the National EDEN project which was established in England in 2005 (Correll et al., 2018). This research-led study has allowed for extensive ongoing analysis of a longitudinal cohort (e.g. Leighton et al., 2019a), which continues to substantially improved our understanding of the development and trajectory of early psychosis. However, as less than half of those accessing services consented to take part in the data collection for the project, the data analysed may not be representative of the broader population of service users. A more recent analysis of real-world implementation of FEP services (Posselt et al., 2021) focused on outcomes obtained from Danish national registries with the authors comparing these findings to similar outcome measures from the original Danish OPUS trial (Petersen et al., 2005). They reported improved outcomes for individuals who received treatment after implementation of FEP services nationally, including fewer and shorter psychiatric admissions and higher rates of employment. This novel analysis has overcome the challenge of population representativeness but remains limited by the selection of outcome measures available within the national registry. Cannon (2021) argues that further evaluation of interventions implemented as a standard of care is much needed in psychiatric research.
To date, the majority of outcome studies have focused on FEP patients, with naturalistic outcomes of UHR patients being limited to a handful of single sites (Fusar-Poli et al., 2020; Lin et al., 2015; Nelson et al., 2013). This is an issue as there remains considerable academic debate about the efficacy of clinical service provision and the target UHR populations (Yung et al., 2021).
To address these knowledge gaps, the current study used secondary data from the minimum dataset to determine the impact that receiving treatment from the hEP services has on clinical and functional outcomes for young people experiencing a FEP or being at UHR. Specifically, we aim to (1) test the potential of using real-time, real-world, low-cost administrative data to establish treatment outcomes and trajectories, (2) evaluated the longitudinal changes of clinical (psychiatric symptomatology and psychological distress) and functional outcomes across both cohorts and (3) establish the proportion of our sample that are identified as UHR that transition to full threshold psychosis.
Methods
Setting
Participating sites were the six clusters (comprising of 15 specific treatment centres) of the hEP programme. Based in a primary care setting, the hEP programme aims to detect young people experiencing a FEP or at UHR, and treat them with evidence-based care based on the models developed at EPPIC and PACE. The clusters aim to deliver the 16 core components based on the Australian Clinical Guidelines for Early Psychosis, and set out in the Australian Early Psychosis model and service implementation guide (Stavely et al., 2013), thus ensuring a comprehensive approach with easy access to youth-friendly care, outreach through home visits, case management, medication, and psychosocial interventions including psychological therapies and functional recovery programmes.
Fidelity to this model has been measured annually and shown to be ‘superior’ in all services (Williams et al., 2021). Tenure of care for those with a FEP is a minimum of 2 years up to a maximum of 5 years for those with more complex or enduring needs. For young people assessed as UHR, the service is typically available for 6 months due to the current funding model in place.
Participants
This study consists of data collected on young people meeting criteria for FEP or UHR, aged between 12 and 25, who registered with a hEP service between 19 June 2017 and 30 September 2019 and provided informed consent. This start date was used due to new data collection systems and consent procedures being initiated.
Measures
Data were collected by case managers upon entry to the hEP service and at regular 90-day intervals during the young person’s tenure within services using a standard battery of outcome measures contained within the hEP minimum dataset (MDS). At baseline, demographic details were collected, including gender, age, sexuality, and Aboriginal and Torres Strait Islander (ATSI) and Culturally and Linguistically Diverse (CALD) background.
Data were captured within units of ‘Episodes Of Care (EOC)’, with each EOC representing a distinct period spent within the service. It was possible for an individual to have multiple EOCs if, e.g., they moved out of the local area but then returned. All the service records involving multiple EOCs of the same individual were manually reviewed to determine whether the EOCs could be combined due to a minimal time gap in between (<30 days).
The following specific measures were collected throughout a young person’s EOC in the electronic MDS.
Clinical outcomes
The 24-item Brief Psychiatric Rating Scale (BPRS) (Overall and Gorham, 1962) is a clinician-rated scale covering a range of psychiatric symptoms such as depression, anxiety, hallucinations and unusual behaviour. A total score (range, 24–168) gives an indication of overall psychopathology. In addition, items in the BPRS can be used to create subscales (Lachar et al., 2001). Here, we focused on two subscales, namely BPRS-Psychosis (item 9: Suspiciousness, 10: Hallucinations, 11: Unusual thought content and 15: Conceptual disorganisation; total score ranges from 4 to 28) (Overall and Gorham, 1962) and BPRS-Negative (item 16: Blunted affect, 17: Emotional withdrawal and 18: Motor retardation; total score ranges from 3 to 21) (Shafer, 2005). These subscales were chosen as they are among the most relevant to understanding the presentation of individuals with early psychosis (Shafer, 2005).
The Kessler Psychological Distress Scale (K10) (Kessler et al., 2003) was used to measure distress associated with depression and anxiety. The total score of K10 ranges from 10 to 50, with a score above 30 indicating a very high level of distress (Furukawa et al., 2003).
Functional outcomes
The Social and Occupational Functioning Assessment Scale (SOFAS) (American Psychiatric Association, 2000) provides a single score out of 100 that captures the clinician’s perspective on the level of functioning in social and occupational domains. According to the anchor points of the scale, a score of 50 represents ‘serious impairment in social, occupational, or school functioning (e.g. no friends, unable to keep a job)’, and 80 represents ‘no more than a slight impairment in social, occupational, or school functioning (e.g. infrequent interpersonal conflict, temporarily falling behind in schoolwork)’.
My Life Tracker (MLT) (Kwan et al., 2018) is a five-item self-report measure to assess the quality of life in five areas: general well-being, day-to-day activities, relationships with friends, relationships with family and coping/dealing with life. Responses to each item are given on a sliding scale with anchors accompanied by a visual analogue of a sad and happy face. Total MLT scores are calculated by averaging across the five items, ranging from 0 to 100, with a higher score indicating a higher quality of life.
DUP
For those experiencing a FEP, a marker of DUP was captured as the time elapsed between the start of the first frank psychotic symptoms (manifest psychosis) and the commencement of antipsychotic medication or treatment by the hEP team. These dates are collected by clinicians during the assessment process for acceptance into the service. Due to the nature of the data structure, the commencement date of FEP treatment was only captured for the current EOC and treatments of historical EOCs or treatment provided by other services were not available. Given the hEP services only accept individuals experiencing their FEP, the impact is likely to be limited.
Analysis
Descriptive statistics were used to describe the characteristics of participants across UHR and FEP EOCs. Kruskal–Wallis test and chi-square test of independence were used to compare the profiles between the two groups. Distributions of outcome measurements across time were visualised using a line graph and boxplot. Linear mixed-effects models were used to evaluate longitudinal treatment responses while controlling for key confounders, including age at the start of EOC, gender, sexuality, ATSI status, CALD background and treatment clusters. DUP was not included as a confounding factor in these models due to the slightly higher proportion of missingness and possible coding errors (data collected as date rather than days). Sensitivity analysis was performed including DUP as a confounder for FEP group.
Clustering at the EOC level was controlled using random intercept. A small proportion of patients presented with multiple EOCs (3%) over the study period. However, most of these EOCs had a large time gap between treatment sessions (those multiple EOCs with a minimal time gap were combined during data cleaning), therefore correlations between separate EOCs from the same patient were not modelled as random intercepts. All analyses were conducted separately for UHR and FEP. Individuals who transitioned were coded as UHR, with sensitivity analyses performed in the UHR group, excluding those who transitioned to FEP. Due to the non-linear temporal treatment response patterns, mixed-effects models were conducted separately for 6 months, 12 months and all treatment period data to reflect averaged treatment effect at different time windows.
Missing data were imputed using multiple imputation via chained random forest using missRanger function from missRanger R package (Mayer, 2019). This is a multiple imputation method that applies a fast implementation of chained Random Forest (Wright and Ziegler, 2017) and predictive mean matching to avoid prediction out of range. Data were only imputed cross-sectionally due to the unbalanced data structure (different numbers of follow-up time points for different patients). Both individual items and total scores were included in the imputation model to improve imputation model performance and the use of random forest avoids the issues of collinearity in the imputation models (Shah et al., 2014). There were 20 imputed datasets used, and regression model results were combined using Rubin’s rule (Rubin, 1987).
Ethics
Ethical approval for this project was obtained from the University of Melbourne Human Research Ethics Committee (2021-20371-13617-3). Data are only reported on young people who consented to have their data collected for research purposes.
Results
Sample demographics
Participant flow is detailed in Figure 1. A total of 5296 EOCs were collected during the study period, among which 66% had patient consented to the study leaving 3511 EOCs subsequently obtained from headspace. Among these records, 672 EOCs were excluded as they were retrospectively entered with only a small number of data fields collected and 1052 EOCs that were assessed by – but not admitted to – the services were also excluded. Also removed from this analysis were 413 EOCs from one of the clusters that reported data collection issues during this time period. Finally, 84 EOCs were merged with subsequent EOC(s) from the same person following data cleaning. The time gap between those records and subsequent EOC(s) varied from 1 to 30 days, thus representing either data management error or patients being discharged and re-admitted again soon after. The consent rate among the valid EOCs was 92.5%.
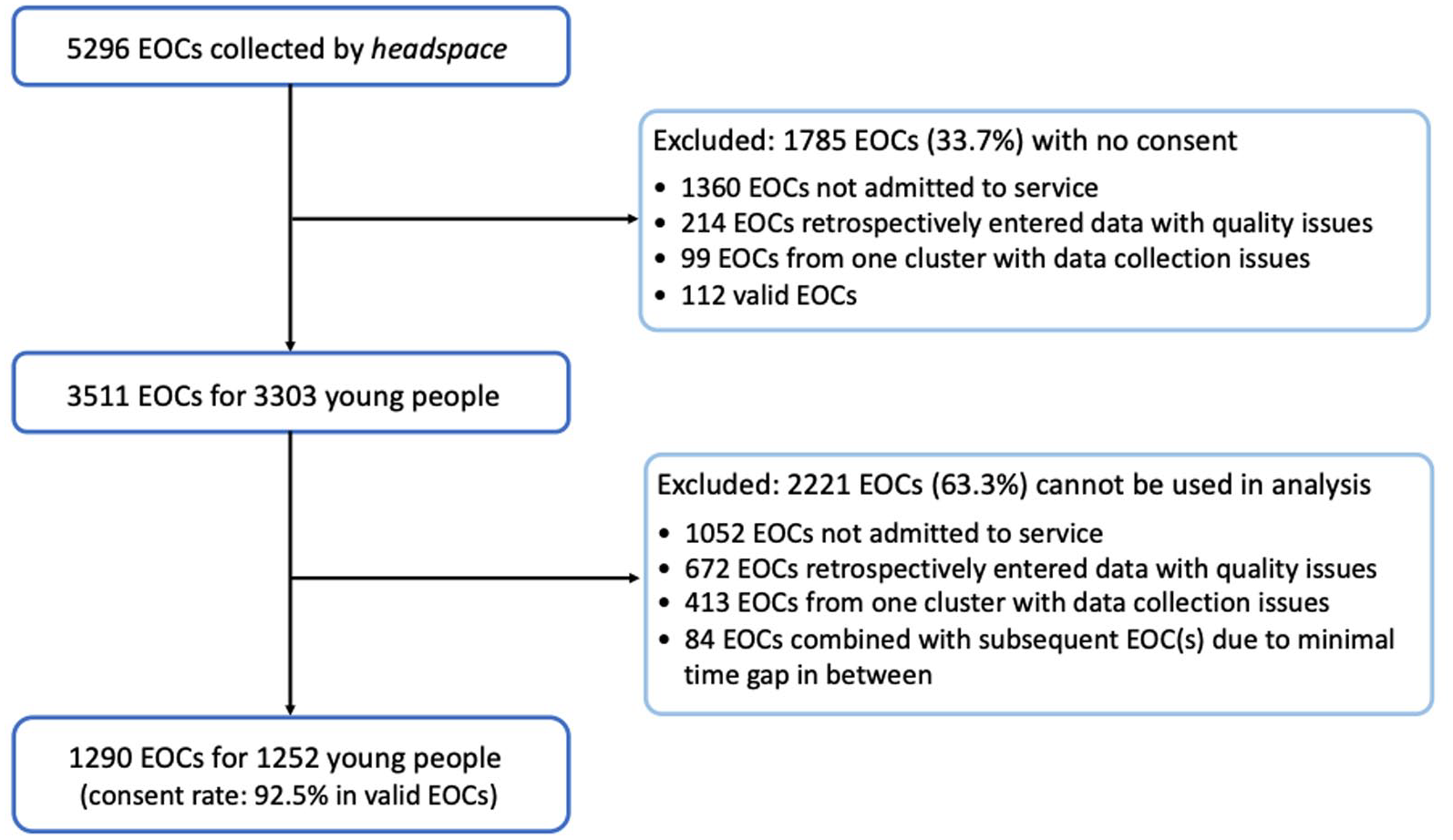
Process for determining sample for analysis.
In total, 1290 EOCs from 1252 young people were used in the analysis, of which 643 met the criteria for FEP and 609 for UHR. About 57% of the FEP patients and 28% of UHR patients were still being actively treated at the end of the data collection period. Participant characteristics are provided in Table 1.
Participant demographics by treatment group.
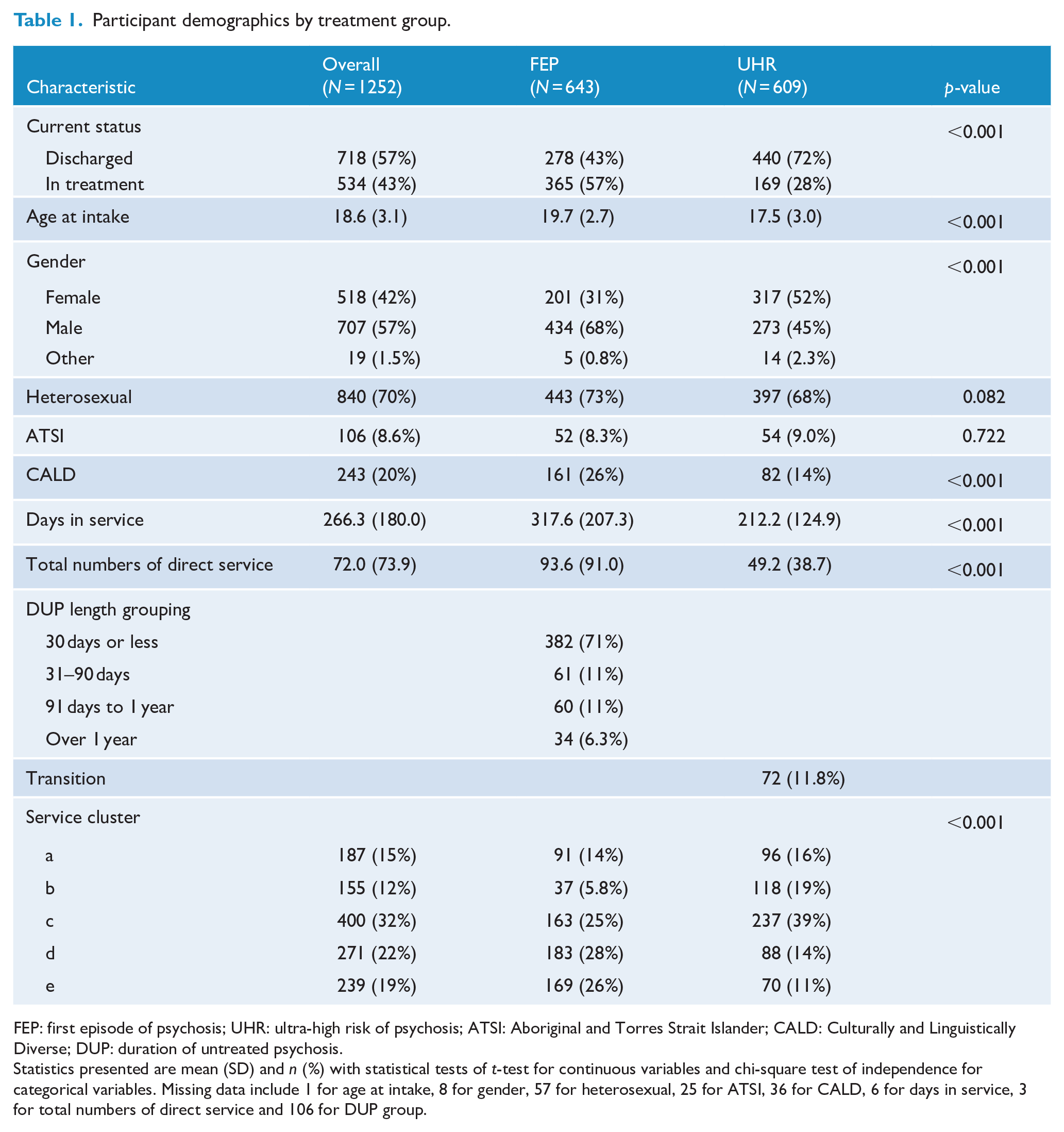
FEP: first episode of psychosis; UHR: ultra-high risk of psychosis; ATSI: Aboriginal and Torres Strait Islander; CALD: Culturally and Linguistically Diverse; DUP: duration of untreated psychosis.
Statistics presented are mean (SD) and n (%) with statistical tests of t-test for continuous variables and chi-square test of independence for categorical variables. Missing data include 1 for age at intake, 8 for gender, 57 for heterosexual, 25 for ATSI, 36 for CALD, 6 for days in service, 3 for total numbers of direct service and 106 for DUP group.
The UHR group was slightly younger with a median age of 17 (interquartile range [IQR]: 15–20) and a mean age of 17.5 (standard deviation [SD]: 3.0) compared with the FEP group, which had a median age of 20 (IQR: 18–22) and a mean age of 19.7 (SD: 2.7). There were also more females accessing UHR services than FEP services (52% vs 31%). The proportion of ATSI young people were comparable between groups, but a higher proportion of FEP patients were from CALD backgrounds compared with UHR patients (26% vs 14%).
DUP
Data on DUP were available for 537 out of 643 young people with FEP. There were 382 (71%) with a DUP of 30 days or less, among which 177 participants reported being prescribed antipsychotic medication on or before the first threshold-level psychotic symptom started.
Transition to psychosis
Of the 609 young people in the UHR group, 72 were known to experience a FEP, representing a transition rate of 11.8%. The transition rate outside of the treatment engagement period (i.e. those who transitioned after being discharged, referred to other services or disengaging from the hEP services) was, of course, unknown.
Clinical outcomes
Psychiatric symptomatology (BPRS)
Substantial changes were observed across all clinical and functional outcomes among UHR participants at the 6-month review, see Table 2. BPRS reduced from an average of 46.3 (SD: 11.9) at baseline to 37.7 (SD: 10.3) at the 6-month review with a mean score reduction of 7.7 (SD: 13.4), which was equivalent to about 17% of the mean baseline level. A considerable change was observed in the BPRS-Psychosis subscale with a mean score reduction of 2.4 (SD: 3.6), which is comparable to about 28% of the baseline level. A moderate level of reduction in BPRS-Negative was observed in the UHR group, which is related to the relatively low score at the baseline.
UHR and FEP patients’ outcome by treatment time (for each EOC).
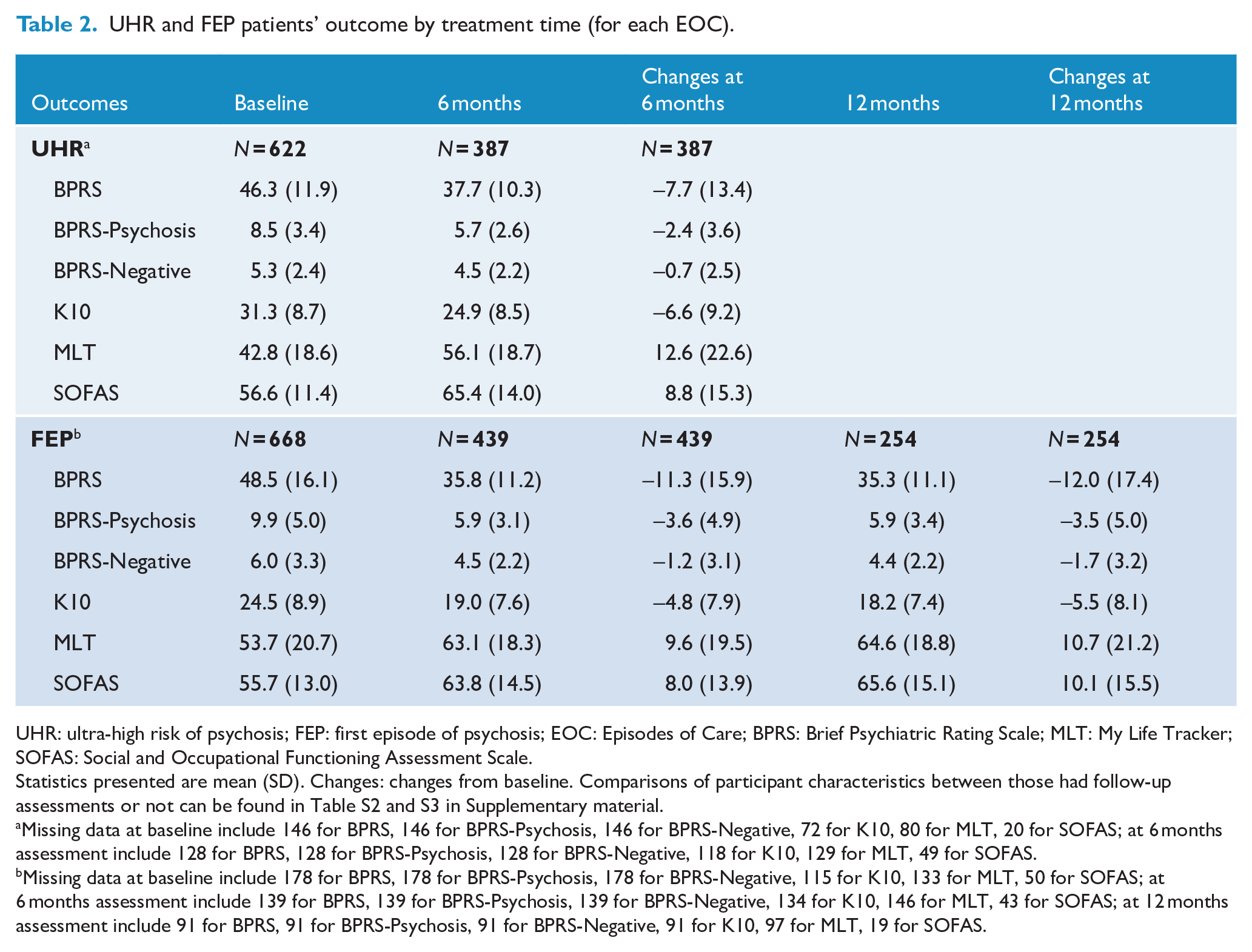
UHR: ultra-high risk of psychosis; FEP: first episode of psychosis; EOC: Episodes of Care; BPRS: Brief Psychiatric Rating Scale; MLT: My Life Tracker; SOFAS: Social and Occupational Functioning Assessment Scale.
Statistics presented are mean (SD). Changes: changes from baseline. Comparisons of participant characteristics between those had follow-up assessments or not can be found in Table S2 and S3 in Supplementary material.
Missing data at baseline include 146 for BPRS, 146 for BPRS-Psychosis, 146 for BPRS-Negative, 72 for K10, 80 for MLT, 20 for SOFAS; at 6 months assessment include 128 for BPRS, 128 for BPRS-Psychosis, 128 for BPRS-Negative, 118 for K10, 129 for MLT, 49 for SOFAS.
Missing data at baseline include 178 for BPRS, 178 for BPRS-Psychosis, 178 for BPRS-Negative, 115 for K10, 133 for MLT, 50 for SOFAS; at 6 months assessment include 139 for BPRS, 139 for BPRS-Psychosis, 139 for BPRS-Negative, 134 for K10, 146 for MLT, 43 for SOFAS; at 12 months assessment include 91 for BPRS, 91 for BPRS-Psychosis, 91 for BPRS-Negative, 91 for K10, 97 for MLT, 19 for SOFAS.
Compared with UHR, FEP patients showed a greater reduction in BPRS as well as the psychosis and negative subscales of the BPRS at the 6-month review, see Table 2. BPRS reduced from an average of 48.5 (SD: 16.1) to 35.8 (SD: 11.2) at 6-month review, representing a mean score reduction of 11.3 (SD: 15.9), which is equivalent to about 23% of the mean baseline level. The largest change in the FEP group was also observed in the BPRS-Psychosis subscale with a mean score reduction of 3.6 (SD: 4.9), comparable to about 36% of the baseline level. However, the treatment effect on this measure seems to plateau after 12 months of treatment; see the trajectories of outcomes mean scores plotted in Figure 2 and estimated changes in outcomes and associated 95% confidence interval (CI) for each 6 months of treatment in Figure 3.
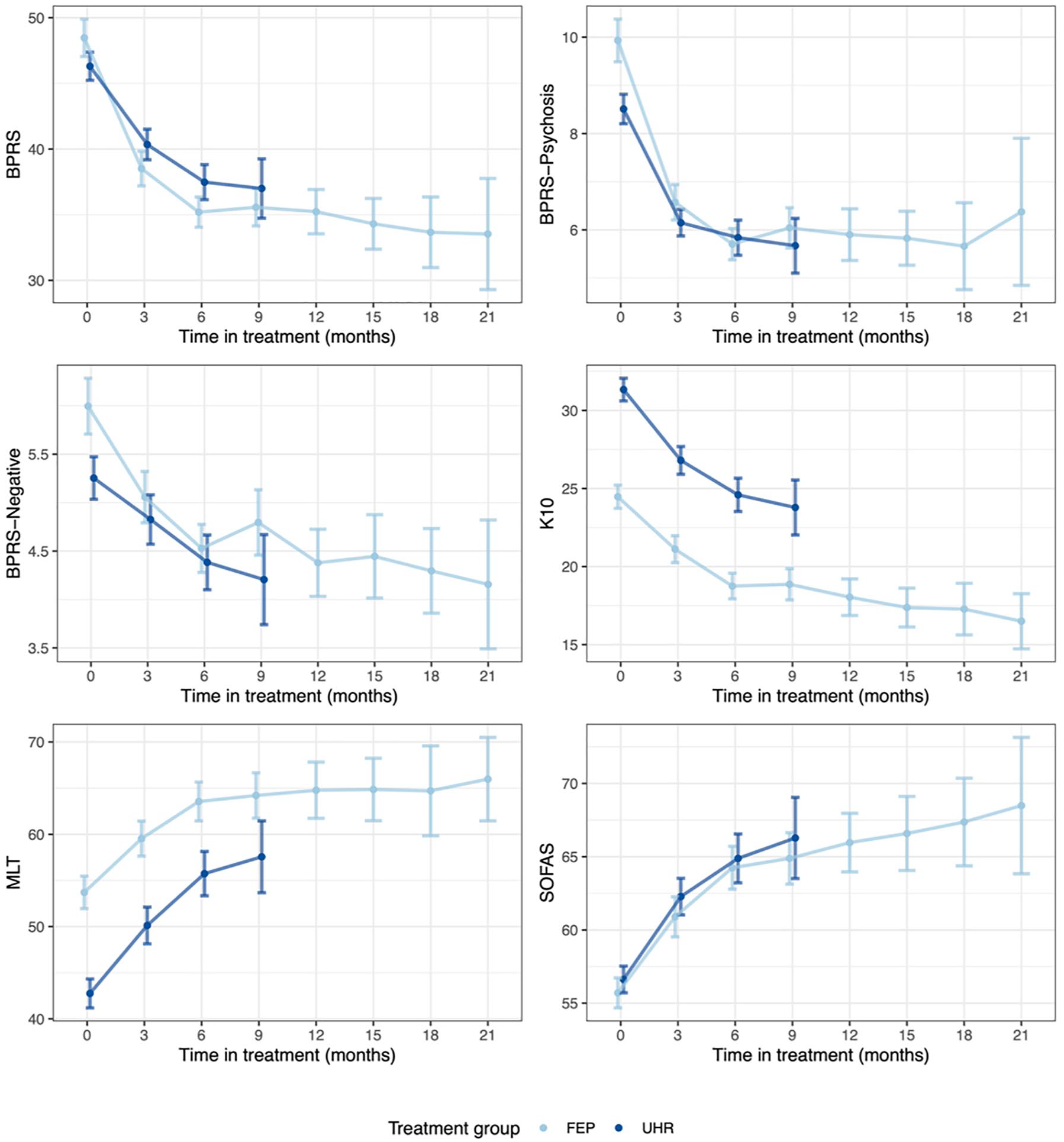
Changes in outcomes (mean and SE) over time by treatment group.
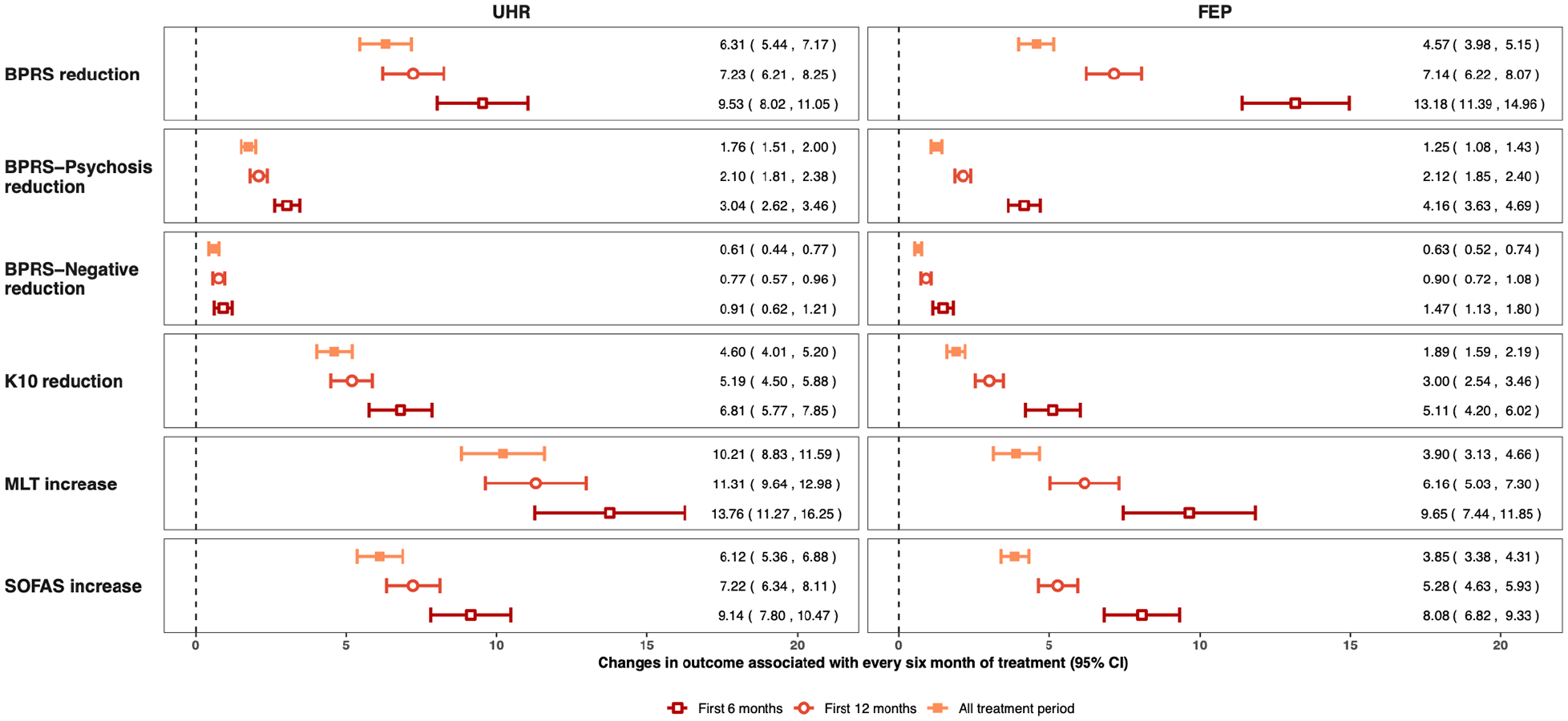
Estimated changes in outcomes and associated 95% CI for 6 months of treatment by treatment group. Note: all coefficients were estimated from mixed-effect linear regression controlling for age, gender, sexuality, ATSI status and service cluster. Random intercepts at individual level were included and missing data were imputed using multiple imputation with 20 imputed datasets.
Psychological distress (K10)
Reductions in distress level were also apparent for both groups. The UHR group started with higher average K10 scores at baseline, 31.3 (SD: 8.7), which were reduced to 24.9 (SD: 8.5) after 6 months of treatment (the mean score reduction was 6.6 [SD: 9.2]). As shown in Figure 2, the FEP group had lower K10 scores at baseline and improved to a lesser extent (the mean score reduction was 4.8 [SD: 7.9] after 6 months). Unlike the plateau effect observed in BPRS, K10 scores continued to improve after 12 months, seen visually in Figure 3. On average, among those who continued to access services at 12 months, the mean score reduction from baseline was 5.5 (SD: 8.1).
Functional outcomes
MLT
Similar treatment-response trajectories were found in the Quality of Life indicator, MLT. The UHR group presented with a lower quality of life at baseline compared with FEP; however, greater improvement can be seen over 6 months of treatment. Among those completing the 6-month review, the mean score increase was 12.6 (SD: 22.6) in the UHR group and 9.6 (SD: 19.5) in the FEP group. Further improvements were also observed after 12 months in the FEP group 10.7 (SD: 21.2); however, changes were minimal beyond 12 months, see Figures 2 and 3.
SOFAS
Functioning, as measured by the SOFAS, was also found to improve by a considerable amount in both the UHR group (56.6 [SD: 11.4] at baseline to 65.4 [SD: 14.0] after 6 months) and FEP group (55.7 [SD: 13.0] at baseline to 63.8 [SD: 14.5] after 6 months). As shown in Figures 2 and 3, functioning was found to continue to improve post 6 months and 12 months in the FEP group, unlike the plateau effects seen on the psychotic symptom measures.
Linear mixed-effects model
Linear mixed-effects models were used to quantify treatment responses, controlling for the clustering effect of repeated measurements and other confounding factors including age, gender, sexuality, ATSI background, CALD background and service cluster. Estimated treatment responses associated with 6 months of treatment are summarised in Figure S1 (Supplementary material), and individual regression results for the total treatment period are provided in Tables S3–S14. There is strong evidence of positive treatment responses across all outcome domains with the greatest improvement observed during the first 6 months. For example, during the first 6 months of treatment, the BPRS scores were estimated to reduce by 9.53 (95% CI: [8.02, 11.05]) in the UHR group and 13.18 (95% CI: [11.39, 14.96]) in the FEP group. Due to the plateau effect, the averaged treatment-response effect estimates were smaller when all first 12 months’ review data were evaluated, with BPRS scores estimated to reduce 7.23 (95% CI: [6.21, 8.25]) in the UHR group and 7.14 (95% CI: [6.22, 8.07]) in the FEP group per 6 month’s treatment.
Estimated treatment effects when all outcome scores were scaled to a range of 0–100 are displayed in Figure S2 in the supplementary material. Relative to the scale range, the FEP group showed the highest treatment response in the BPRS-Psychosis subscale, whereas the UHR group showed the highest treatment response in K10. Sensitivity analysis comparing estimated effect sizes in the UHR group with the UHR group excluding those who transitioned to FEP is provided in Figure S3. Estimated treatment responses for FEP group were found to be almost identical from models including and excluding DUP as a confounder (results not shown). Results suggest a slightly higher level of treatment responses among those who did not transition across all outcome measures.
Discussion
This analysis of 1252 young people accessing early psychosis services across Australia (643 FEP, 609 UHR) suggests that by engaging with early psychosis services, significant improvement can be achieved across standardised measures of clinical and functional outcomes. FEP patients experienced a higher level of reduction in psychosis symptoms, whereas UHR patients showed a greater level of reduction in psychological distress symptoms as measured by the K10. Although clinical outcomes showed a plateau effect after approximately 3 months of care, improvement in functional outcomes continued at the later stage of treatment.
This study aimed to establish the naturalistic treatment trajectories of young people accessing these services outside the setting of a structured research project with the associated sample bias (Posselt et al., 2021). The improvement seen in functional outcomes across the course of care provides face validity to recovery orientated treatment programmes. These findings further support Posselt et al.’s (2021) conclusions that the outcomes of individuals accessing FEP services in the real world can be better than during the original trials of the model. In contrast to Posselt and colleagues’ analysis of objective registry data, our current study provides a more detailed exploration of symptomatic and functional outcomes. This allows for the identification of future potential treatment targets, e.g. the problem of treating negative symptoms in FEP. The current study is also one of the first presentations of real-world outcomes for UHR cohorts and as these data are from a national sample, they will also be useful to benchmark between services and provide a baseline for comparison of new treatment models.
To give context to the improvements seen during the course of treatment, it can be helpful to consider how they compared to other published FEP cohort studies. In comparison, functional data collected from the national EDEN project in the United Kingdom, a similar naturalistic cohort, shows that on average participants improved by around 10 points on the Global Assessment of Functioning (GAF) disability scale in a similar timeline (Rowland et al., 2019; Thompson et al., 2016). The current FEP cohort also improved by around 10 points on the SOFAS and improvement continued out to 21 months (Figure 2). A 10-point improvement on the GAF or SOFAS refers to a change from one anchor point to another, e.g. from ‘moderate difficulty’ (score of 51–60) to ‘some difficulty’ (score of 61–70).
While the sample for the National EDEN project was slightly more impaired at baseline (GAF 50 vs SOFAS 55), these results suggest there is substantial functional benefit from treatment programmes that focus on long-term functional recovery as well as symptomatic treatment. Supporting individuals to remain engaged with early intervention services and/or improving strategies to support the re-engagement with services could optimise the impact on functional outcomes (Kim et al., 2019).
Given the limited number of service-based UHR studies (e.g. Beck et al., 2019), comparison of outcomes for the UHR cohort is difficult. In comparison to outcomes from participants in the PACE400 dataset (Nelson et al., 2013, on which the current model of care for UHR was based), at follow-up, average scores on the SOFAS were 67 (McHugh et al., 2018), comparable to the current finding at 6 months of an average SOFAS score of 66. However, data from the PACE400 study were not service data and therefore the cohort may differ from individuals attending hEP services here.
Within the UHR group, a transition rate of 11.8% was observed, lower than the 18% at 6-month follow-up found in a 2012 meta-analysis of transition rates (Fusar-Poli, 2012). These authors also reported that the transition rate over a 2-year follow-up increased to 29% and given the tenure of care for those with UHR in the hEP services is 6 months, it is likely that the current finding of 11.8% is an underestimation as individuals could have gone on to transition to psychosis following referral out of service.
Concerningly, despite considerable reduction in K10 scores for those at UHR, distress symptoms remained ‘high’ on the K10 at 6 months of treatment. The reason for this is possibly due to the complex presentations of the young people who meet eligibility for these services, both diagnostically and socio-economically. Distress from ongoing Attenuating Psychotic Symptoms (APS) may also compound these scores (Wilson et al., 2020), and further exploration of this issue of high levels of distress is warranted.
We argue that these current findings support the international calls for the duration of care to be extended past 6 or even 12 months for this at-risk group (Fusar-Poli et al., 2020), particularly in the current setting here in Australia. Justification for this policy shift is twofold; first, the risk of transition to psychosis increases long past the 6-month cutoff (De Pablo et al., 2021). Second, high levels of distress clearly remain at 6 months and these young people often present with multiple co-morbidities meaning that these young people will likely require further mental health care. It would be counter-intuitive to require them to find alternative services at a time when their needs remain so high.
Clinical implications
Overall, the findings from these current analyses suggest that receiving a clinical early intervention service has a positive impact on the functioning and well-being of young people at ultra high risk of psychosis or experiencing a FEP. Figure 2 shows visually the progression of symptom reduction, with substantial reductions in the first 3 months of service engagement, but then reaching a plateau after approximately 6 months for those with FEP. This plateauing contrasts with the continuation of improvement in functional outcomes (SOFAS, MLT) after 6 months, which is likely due to the lag in functional response compared to symptom response in psychosis. Breaking the BPRS down into sub-domains reveals that symptomatic improvement is driven by the reduction in positive symptoms, with BPRS negative symptoms taking the longest to respond to treatment, reflecting the fact that negative symptoms of psychosis remain those hardest to treat (Aleman et al., 2017; Lutgens et al., 2017). Potential novel approaches to addressing negative symptoms such as behavioural activation (Choi et al., 2016; Mairs et al., 2011) or novel pharmacological agents, e.g. cannabidiol (Davies and Bhattacharyya, 2019), need further investigation.
Our study has also demonstrated the feasibility of using real-time, real-world and low-cost administrative data to rigorously evaluate symptomatic and functional outcomes in early psychosis treatment settings. Such data also provide a unique opportunity to broadly understand the patient profile (e.g. heterogeneity) and treatment responsiveness (e.g. risk associated with transition) with a low level of participation bias. As data are routinely collected as part of clinical treatment, they have the potential to be used to develop real-time risk tools to assist with treatment planning and delivery (Cannon et al., 2016; Leighton et al., 2019b).
As more data are collected from the services, we will be in the position to develop real-time prediction models based on patient profiles as well as their treatment responses. These state-of-the-art prediction models could impact real-world clinical treatment decisions as we try to move towards precision medicine in psychiatry. This work will be supported by data linkage facilitated by the establishment of a national data registry which will also allow for the long-term, real-world outcomes of this still under-researched group to be properly established.
Study limitations
The results of these analyses must be viewed in light of a number of limitations. Although data were extracted from a high-quality data collection platform (which included the provision of appropriate training in the outcome measures and a degree of quality assurance provided by onsite data officers) to capture patient outcomes, they are still vulnerable to the limitations experienced by digital healthcare data collection tools (Dinov, 2016). Examples of these limitations include variations in individual clinician’s interpretation of clinical tools, high level of missing data in some data fields and data entry errors. Biases in data interpretation may arise from non-participation (the non-consenting cohort) and longitudinal attrition, which is a common problem in longitudinal studies. However, this may not impact our study substantially due to high level of consent rate among participants in services and comparable characteristics between those who had follow-up assessment or not (see Table S2 and S3). Many clinicians and service planners/organisations, as well as clinical quality registries (Ruseckaite et al., 2019), now advocate for opt-out consent with regard to routine clinical data collection supported by the linking of service record data with external data sources such as hospital admission records to overcome this challenge (Perera et al., 2016).
A further limitation is that in this cohort the DUP was calculated as the time from first frank psychotic symptom to either prescription of antipsychotic medication or acceptance into service for the current EOC, which is different to the way some services measure DUP (which is often based on antipsychotic prescription, Barnes et al., 2000; Compton et al., 2007). It may also be over-estimated among those with recorded long DUP due to the fact that historical treatment information was not captured. As DUP was captured as dates in the database, it was missing for a high proportion of records and also more likely to have coding error. DUP was not therefore included in the regression models as a risk factor. Further simplification of DUP measures in clinical services is required. Another limitation of the current data presented is that the BPRS may not be sensitive enough to pick up change in UHR symptomatology. While the CAARMS (Comprehensive Assessment of At Risk Mental States) is now undertaken as part of routine data collection in hEP services, it was not possible to include these data here. A final limitation of these findings presented in this paper is the lack of a control group to compare our functional and symptomatic outcomes. However, as we have pointed out above, the current outcomes are similar to, if not better than existing longitudinal and randomised controlled studies.
Conclusion
This study represents one of the largest, naturalistic treatment outcomes studies globally in early psychosis, and certainly within Australia. Clinical and functional outcome improvements for young people in these services were encouraging, with psychiatric symptomatology improving fairly rapidly and functioning continuing to improve even after symptoms may have plateaued. Building on the successful collection and analysis of these data with data linkage would allow a longitudinal understanding of effectiveness of early intervention on clinical, functional and service use outcomes for young people. We are planning to use this minimum dataset to form the basis of a national clinical quality registry that allows individual and service-wide monitoring of outcomes to ensure maintenance of the high-quality outcomes achieved.
Supplemental Material
sj-pdf-1-anp-10.1177_00048674211061285 – Supplemental material for The clinical and functional outcomes of a large naturalistic cohort of young people accessing national early psychosis services
Supplemental material, sj-pdf-1-anp-10.1177_00048674211061285 for The clinical and functional outcomes of a large naturalistic cohort of young people accessing national early psychosis services by Ellie Brown, Caroline X. Gao, Heather Staveley, Georgia Williams, Simone Farrelly, Debra Rickwood, Nic Telford, Cerissa Papanastasiou, Pat McGorry and Andrew Thompson in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We gratefully acknowledge the contribution of the young people accessing services who consented to having their data made available for evaluation purposes. We would also like to thank the clinical staff at the hEP programs for their diligent data collection and those at headspace National who support the data management systems.
Author Note
Caroline X. Gao is now affiliated to School of Public Health and Preventive Medicine, Monash University, Melbourne, VIC, Australia
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by funding from the Australian Commonwealth Government as part of the Australian Early Psychosis Program.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.