
Abstract
Objective:
Understanding the relationship between attachment and mental health has an important role in informing management of perinatal mental disorders and for infant mental health. It has been suggested that experiences of attachment are transmitted from one generation to the next. Maternal sensitivity has been proposed as a mediator, although findings have not been as strong as hypothesised. A meta-analysis suggested that this intergenerational transmission of attachment may vary across populations with lower concordance between parent and infant attachment classifications in clinical compared to community samples. However, no previous study has examined major depression and adult attachment in pregnancy as predictors of infant–parent attachment classification at 12 months postpartum.
Methods:
Data were obtained on 52 first-time mothers recruited in early pregnancy, which included 22 women who met diagnostic criteria for current major depression using the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders. The Adult Attachment Interview was also administered before 20 weeks of pregnancy. A history of early trauma was measured using the Childhood Trauma Questionnaire and maternal sensitivity was measured at 6 months postpartum using the observational measure of the Emotional Availability Scales. Infant–parent attachment was measured using the Strange Situation Procedure at 12 months.
Results:
Overall, we found no significant association between the Adult Attachment Interview and the Strange Situation Procedure classifications. However, a combination of maternal non-autonomous attachment on the Adult Attachment Interview and major depression was a significant predictor of insecure attachment on the Strange Situation Procedure. We did not find that maternal sensitivity mediated parental and infant attachment security in this sample.
Conclusion:
While previous meta-analyses identified lower concordance in clinical samples, our findings suggest women with major depression and non-autonomous attachment have a greater concordance with insecure attachment on the Strange Situation Procedure. These findings can guide future research and suggest a focus on depression in pregnancy may be important for subsequent infant attachment.
Background
Attachment theory is important for mental health clinicians in understanding the development of early human relationships and in particular understanding the potential impact of parental mental health as a predictor of infant attachment, as well as infant attachment as a potential predictor of later mental health outcomes for children. Infant attachment, i.e. a stable emotional bond between the infant and a caregiver, has been shown to have enduring significance for children’s social-emotional development. It has been shown that secure infant attachment relationships are related to later social competence and social-emotional well-being, whereas insecure attachment has been associated with a higher risk of emotional and behaviour problems and as such attachment is of interest to both perinatal and child mental health clinicians and services (Galbally et al., 2013; Groh et al., 2017). Furthermore, there is a search for predictors of individual differences in attachment security, as it has been suggested that attachment experiences are transmitted from one generation to the next (van IJzendoorn, 1995; Verhage et al., 2016). An area of particular focus has been intergenerational transmission, operationalised in this area and for this paper, as referring to the pathway through parental attachment measured using the adult attachment interview, a measure of an adult’s mental representation of attachment through the coherence of their discourse during a standardised interview (Main et al., 2002) and then typically infant attachment measured using the Strange Situation Procedure (SSP), a separation reunion task typically undertaken in infants around 18 months of age (Ainsworth et al., 1978).
The intergenerational transmission of attachment, from adult attachment through to infant–parent attachment, has been explored in studies containing more than 4000 parent–child dyads from infancy to adolescence, with a recent individual participant data meta-analysis confirming a combined effect size of approximately r = 0.29 (Verhage et al., 2018). A previous meta-analysis identified studies with a combined sample of 661 mother–infant dyads where the Adult Attachment Interview (AAI) and the Strange Situations Procedure (SSP) had been undertaken to measure parental and then infant–parent attachment; for these studies, an overall 75% concordance was found between parental state of mind with regard to attachment measured using the AAI and parent–infant attachment security measured with the SSP (van Ijzendoorn, 1995). However, concordance between parental and child attachment classification appears to also vary across populations: Both previous meta-analyses identified lower concordance for clinical samples as well as variation with the age of children at assessment (van IJzendoorn, 1995; Verhage et al., 2016). Highlighted has also been the lack of clarity of what constitutes the remaining ‘transmission gap’ for intergenerational attachment, as defined in this context and following these meta-analytic findings (van IJzendoorn, 1995; Verhage et al., 2016). Recent reviews have explored a number of factors, including maternal depression, parental trauma and stress, socio-economic status, maternal sensitivity as well as child-related factors, in understanding the possible differences in transmission of attachment in different populations (Verhage et al., 2016, 2018). Understanding those factors which are important in the intergenerational transmission of attachment is crucial to the development and targeting of interventions.
Maternal depression, trauma and stress are all thought to influence the evolving relationship with her child, including infant–parent attachment (Sliwerski et al., 2020). However, despite the increasing focus by clinical services on antenatal depression as a predictor of attachment, there are no studies that have examined antenatal depressive disorders together with AAI as predictors of infant–parent attachment. Indeed, most studies examining intergenerational attachment that include depression do not draw on clinical samples and do not include current diagnostic measures of depression (Verhage et al., 2016). In their meta-analysis, Verhage et al. (2016) did examine the influence of clinical or high-risk samples on concordance of attachment and in particular factors within this group as potential moderators across a broader range of parental and child risk factors. However, there are few replicated findings or sufficient sample sizes (van IJzendoorn and Bakermans-Kranenburg, 2021). Maternal experiences of childhood trauma may influence both a woman’s own attachment state of mind and her parenting with previous research finding associated with unresolved state of mind, atypical parenting such as characterised by frightened/frightening parenting and disorganised attachment and hence clear relevance to understanding factors moderating the transmission of attachment (Abrams et al., 2006; Out et al., 2009). Indeed, in samples where there is a history of significant maltreatment, there has been a call for careful consideration and potential modification of coding of AAIs in this context (Speranza et al., 2017; Turton et al., 2001).
Arguably, parenting begins in pregnancy and from conception onwards there are increasing influences, both biological and psychological, on the developing relationship between mother and child. While the AAI has demonstrated stability, there remains interest as to whether an AAI conducted in pregnancy can predict infant–parent attachment in the postpartum (Bakermans-Kranenburg and van IJzendoorn, 1993; Fonagy et al., 1991; Sagi et al., 1994). Indeed, there have been 23 studies identified within the meta-analysis undertaken by Verhage et al. that had examined the AAI prior to birth of the child with follow-up to examine infant–parent attachment (Verhage et al., 2016). These studies were undertaken with the rationale that this will reduce the likelihood of confounding by the current infant–parent relationship; all studies identified had undertaken the AAI in late pregnancy and most in first-time mothers (Arnott and Meins, 2007; Benoit and Parker, 1994; Fonagy et al., 1991; Kondo-Ikemura et al., 2018; Shah et al., 2010; Steele et al., 1996; Tambelli et al., 2020; Ward and Carlson, 1995). Unfortunately, the meta-analysis did not focus specifically on those studies undertaken in the antenatal period and did not specifically analyse or report on this group of studies and as such key studies will be described here (Verhage et al., 2016). The first study to examine late pregnancy maternal attachment as a predictor of infant–parent attachment found within a sample of 100 women and children for two-way classification 75% concordance and for three-way classification 66% concordance with the AAI classifications of dismissing, autonomous and pre-occupied with SSP ABC or B and non-B classifications suggesting strong support for intergenerational transmission of attachment beginning in the womb (Fonagy et al., 1991). Further studies have found 68% concordance for four-way classification in a sample of adolescent mothers and, similarly, in a community sample (Benoit and Parker, 1994; Ward and Carlson, 1995). A recent study in a Japanese community sample equally found a significant association between antenatal maternal adult attachment and SSP classification in infant–parent dyads (Kondo-Ikemura et al., 2018).
This paper examines the roles of maternal past trauma experiences, depression and maternal sensitivity in the intergenerational transmission of attachment. We first aimed to examine the concordance between maternal state of mind with regard to attachment assessed using the AAI during early pregnancy and mother–infant attachment security assessed using the SSP at 12 months postpartum. We hypothesised significant concordance between AAI and SSP classification. Second, we examined associations between intergenerational attachment security, maternal trauma, depression, and sensitivity, testing maternal trauma and depression as moderators of integenerational attachment security and testing maternal sensitivity as a mediator of intergenerational attachment security.
Method
Sample
This study draws on pilot data drawn from the Mercy Pregnancy and Emotional Wellbeing Study (MPEWS), a longitudinal, pregnancy cohort study in Melbourne, Australia. The study uses data on 52 first-time mothers and their infants. Women were recruited at less than 20 weeks pregnant and completed the AAI. Overall recruitment for this study commenced in September 2012 and was completed in October 2014 with the last participant delivering in late May 2015. Further details of the study are described in the published cohort profile (Galbally et al., 2017).
The Mercy Health Human Research Ethics Committee approved this study and a written informed consent statement was obtained from each woman. Inclusion criteria were being less than 20 weeks pregnant and English proficiency. Women who developed pregnancy complications were not excluded. Participants were excluded if they had bipolar or psychotic disorders, substance abuse disorder, child protection involvement, intellectual disability, serious pre-existing physical illness and psychiatric illness requiring current acute inpatient admission. The demographic variables for the participants included in this study are reported in Table 1.
Sample sociodemographic and other key characteristics (N = 52).
SCID-IV: Structured Clinical Interview for DSM-IV.
Valid percent presented when data are missing.
Measures
Maternal depression
At recruitment at less than 20 weeks of pregnancy and repeated at 6 months postpartum, the Structured Clinical Interview for DSM-IV (SCID-IV) was administered (First et al., 1997). Women who met diagnostic criteria for a major depressive episode occurring during pregnancy and the first 6 months postpartum (coded 1) were compared against women who did not meet diagnostic criteria for major depression during this period (coded 0).
Maternal attachment
Maternal state of mind with regard to attachment was assessed using the AAI conducted during early pregnancy up to 20 weeks gestation (George et al., 1996). The AAI is a semi-structured interview comprising a set of 20 questions and suggestions for follow-up exploring the interviewee’s perception of childhood experiences with parents, experiences of abuse and loss and the impact of these experiences on their current relationship with his or her parents. The interview is thought to create conditions that direct attention towards attachment-related experiences and is coded for the speaker’s ability to integrate episodic (i.e. specific events) and semantic (i.e. certain beliefs) information. Patterns in the way interviewees talk about attachment experiences are thought to reflect the speaker’s state of mind with respect to attachment autonomy. Using several subscales according to the Main and colleagues’ manual, transcripts can be classified into one of four attachment classification: Insecure dismissing (D), secure autonomous (F), insecure pre-occupied (E) and unresolved/disorganised (U). Binary classifications of attachment autonomy (D, E and U = 0 and F = 1) unresolved/disorganised (D, E and F = 0 and U = 1) can also be derived. There were two certified reliable coders for the AAI. Of the 52 AAIs, 10 were coded by both coders. Using the four-way DFEU classification for the AAI, there was 90% agreement (kappa = 0.63, p = 0.008) between the two coders, and using AAI Security as a binary coding (Secure/Insecure), there was also 90% agreement (kappa = 0.61).
Infant–mother attachment
Infant–mother attachment security was measured using the SSP at 12 months of age (Ainsworth et al., 1978). The SSP is an observational laboratory procedure utilising a standardised protocol of eight 3-minute episodes of separation and reunion with the mother. The procedure should act as a mild stressor for the child and is designed to activate attachment behaviours. The separation episodes were curtailed when the infant was too distressed about the parent’s absence; this was defined as showing physiological signs of distress or prolonged distress and no infant was left distressed for more than 1 minute not resolving. The SSP is coded for three organised patterns of attachment: secure (B), insecure-avoidant (A) and insecure-ambivalent (C). Attachment disorganisation (D) was coded using the Main and Solomon coding system (Main and Solomon, 1990). Richters continuous security scale was also calculated using continuous attachment interactive scales but without infant crying, and respective discriminant functions reported in van IJzendoorn and Kroonenberg (1990). Richters scores equal to 0 and higher suggest secure attachment, whereas Richters scores below 0 suggest insecure attachment. Consistent with van IJzendoorn and Kroonenberg, the derived Richters security score without crying was able to predict secure versus insecure dyads with 90.5% accuracy in our sample. The SSPs were coded by two certified reliable coders. Inter-rater reliability (kappa statistic) between these two coders was 0.64 for the four-way classification, and the intraclass correlation coefficient (ICC) was 0.49 for the Richters security and 0.61 for the continuous disorganisation single measure scores. Following initial assessment of inter-rater reliability, both coders engaged in discussions to arrive at a consensus for each case where there was a disagreement between codes.
History of maternal childhood trauma
Maternal childhood trauma history was measured using the brief version of the Childhood Trauma Questionnaire (CTQ), which is a 28-item self-report measure (Bernstein et al., 2003). Previously, in this cohort, the total CTQ and each of the five subscales (emotional abuse and neglect, physical abuse and neglect and sexual abuse) have demonstrated adequate to strong internal consistency, with Cronbach’s alphas ranging from 0.75 to 0.92 (Galbally et al., 2019). In this study, we dichotomise the total CTQ score because of the positively skewed reports of CTQ. Responses were dichotomised using severity cut-off scores provided by the CTQ manual to create binary groups (0 = None-to-Minimal, 1 = Moderate-to-Severe) (Bernstein et al., 2003).
Maternal sensitivity
Maternal sensitivity was assessed using the maternal sensitivity scale from the Emotional Availability Scales (EAS) at 6 months postpartum (Biringen, 2008). The EAS is an observational assessment designed to evaluate emotional availability by observing and rating parent–child interactions. Both mother and child ratings are produced during coding to derive four maternal total scores and two child total scores; however, we use only the maternal sensitivity total score in this study. Details for the procedure, coding and inter-rater reliability for the EAS in our cohort have been documented previously (MacMillan et al., 2020a, 2020b).
Statistical analyses
We first present sample sociodemographic and other key variable characteristics, as well as univariate distributions of the four- and two-way AAI and SSP classifications, and classifications and scale scores from the AAI and SSP by depression groups. To address the first aim of this paper, we analysed the concordance between the AAI and SSP classifications by presenting the percentage of cases with a concordant classification, accompanied by a kappa test of categorical agreement (kappa) and a χ2 test of independence. Due this relatively small pilot sample, we chose to analyse the concordance between the binary autonomy/security and unresolved/disorganised classifications for the AAI and SSP, respectively. To address the second aim of the paper, we conduct a series of moderated regression models using AAI autonomy to predict SSP attachment security and path analyses to test for mediation. Again, due to the smaller size of this pilot sample, we chose to use the continuous Richters security score, instead of binary SSP attachment security, as the outcome for all regressions and the path analyses. Although the focus of the paper is on the classifications of maternal autonomy of mind, we also replicate all regression models by replacing the binary AAI autonomy with the continuous sense of coherence score and compare results of these alternative models. To test maternal childhood trauma and major depression separately as moderators of the association between AAI autonomy and SSP security, we included the multiplicative interaction term between AAI autonomy and childhood trauma (Model 1) and AAI autonomy and depression (Model 2) into separate linear regression models. Significant interaction terms were then probed by calculating the simple associations and plotting the these as slopes. To test maternal sensitivity as a mediator between AAI autonomy and SSP security, we conducted a path analysis and present both direct and indirect effects. The indirect effect testing for mediation in this path model was estimated using 10,000 bootstrapped samples. Given the smaller pilot sample size, we also provide achieved power estimates for variance explained (i.e. partial R2) by interaction terms and indirect effects. Data management and descriptive statistics conducted using SPSS version 26 and regression modelling conducted using Mplus version 8. Statistical significance for all inferential tests was determined using p < 0.05.
Results
Demographic characteristics of the sample (N = 52) are presented in Table 1. Notably, the sample is exclusively nulliparous. Twenty-one women (40%) met diagnostic criteria for a major depressive disorder. Approximately one-third of women reported experiencing moderate-to-severe trauma during their childhood (32.7%). Average age at recruitment was 30.45 (SD = 5.29; range: 19–42).
For the four-way AAI classification, 7 (13.2%) were classified as insecure dismissing (D), 37 (69.9%) as secure autonomous (F), 4 (7.5%) as insecure pre-occupied (E) and 5 (9.4%) as unresolved/disorganised (U), whereas for the four-way SSP classification, 10 (18.9%) were classified as insecure-avoidant (A), 30 (56.6%) as secure (B), 3 (5.7%) as insecure-ambivalent (C) and 10 (18.9%) as disorganised (D). For AAI autonomy, 37 (69.8%) were classified as autonomous and 16 (30.2%) classified as not autonomous, whereas for SSP security, 30 (56.6%) were classified as secure and 23 (43.4%) as insecure. Figure 1 displays the distributions of the Richters security score across two-way SSP security (Figure 1(a)) and AAI autonomy (Figure 1(b)), with SSP secure and insecure strongly differentiating Richters security scores but broader variation observed across AAI autonomous and not autonomous groups. Table 2 presents classifications and selected continuous scores derived from coding for the AAI and SSP by depression group, demonstrating no significant differences between depression groups across all attachment measures.
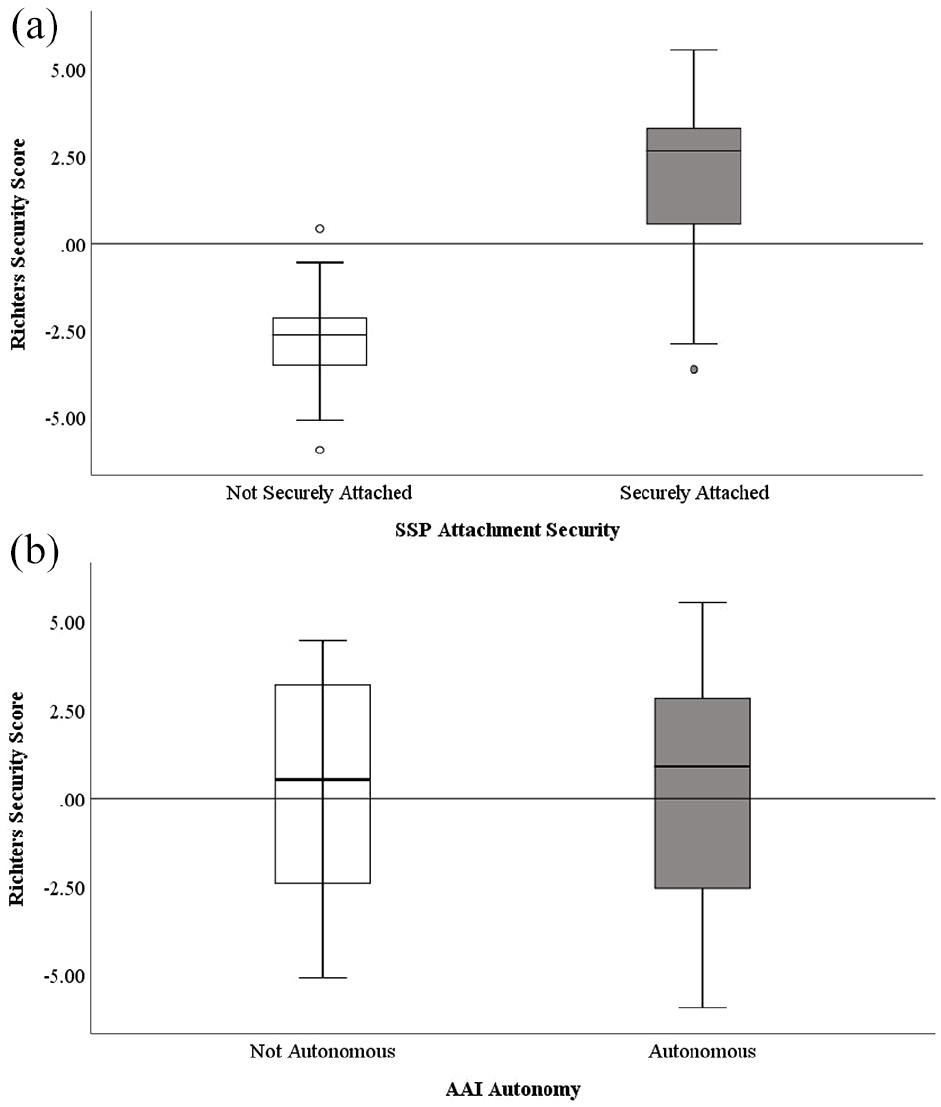
Boxplot displaying the distribution of the Richters security score by (a) SSP two-way attachment security classification and (b) AAI two-way autonomy classification.
AAI and SSP classifications and scales by major depression group (N = 52).
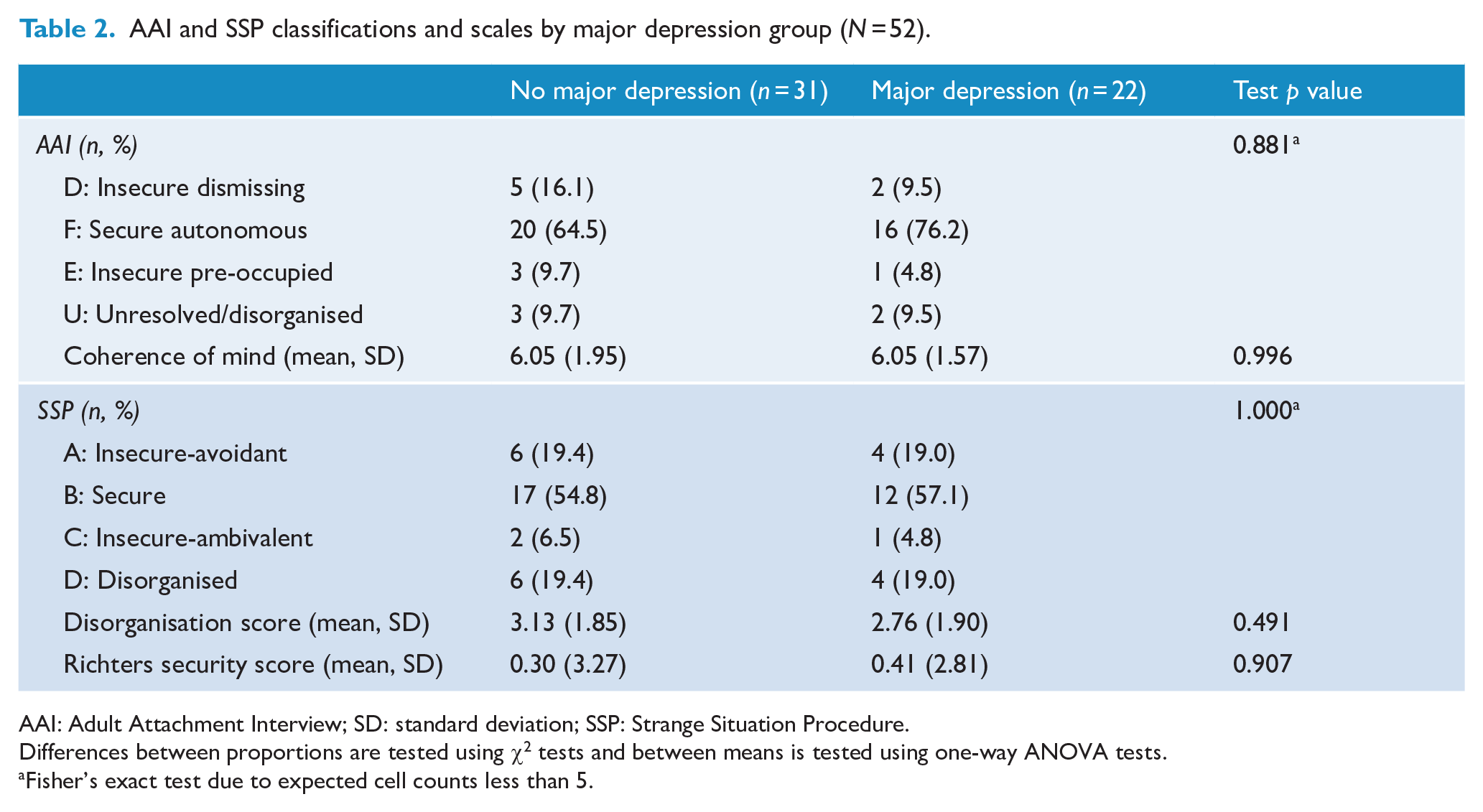
AAI: Adult Attachment Interview; SD: standard deviation; SSP: Strange Situation Procedure.
Differences between proportions are tested using χ2 tests and between means is tested using one-way ANOVA tests.
Fisher’s exact test due to expected cell counts less than 5.
Intergenerational concordance of attachment security
Table 3 presents the concordance between the binary AAI and SSP attachment security and disorganisation classifications. Only 57.7% (n = 30 of 52) of the sample matched on their AAI autonomy and SSP security classifications, which was not significant (p = 0.771), and demonstrated poor agreement (kappa = 0.04). Although 75% (n = 39 of 52) matched on binary AAI unresolved/disorganised and SSP disorganised classifications, this represented poor agreement (kappa = 0.01, p = 0.963) due to low prevalence of AAI unresolved/disorganised states of mind in this sample. These results suggests that mother’s two-way classifications for both AAI autonomy and unresolved/disorganised conducted in early pregnancy and the SSP security and disorganisation, respectively, conducted at 12 months postpartum were related no more strongly than chance in this pilot sample.
Match between distributions of AAI autonomy and SSP security, and AAI unresolved/disorganised and SSP disorganisation (N = 52).
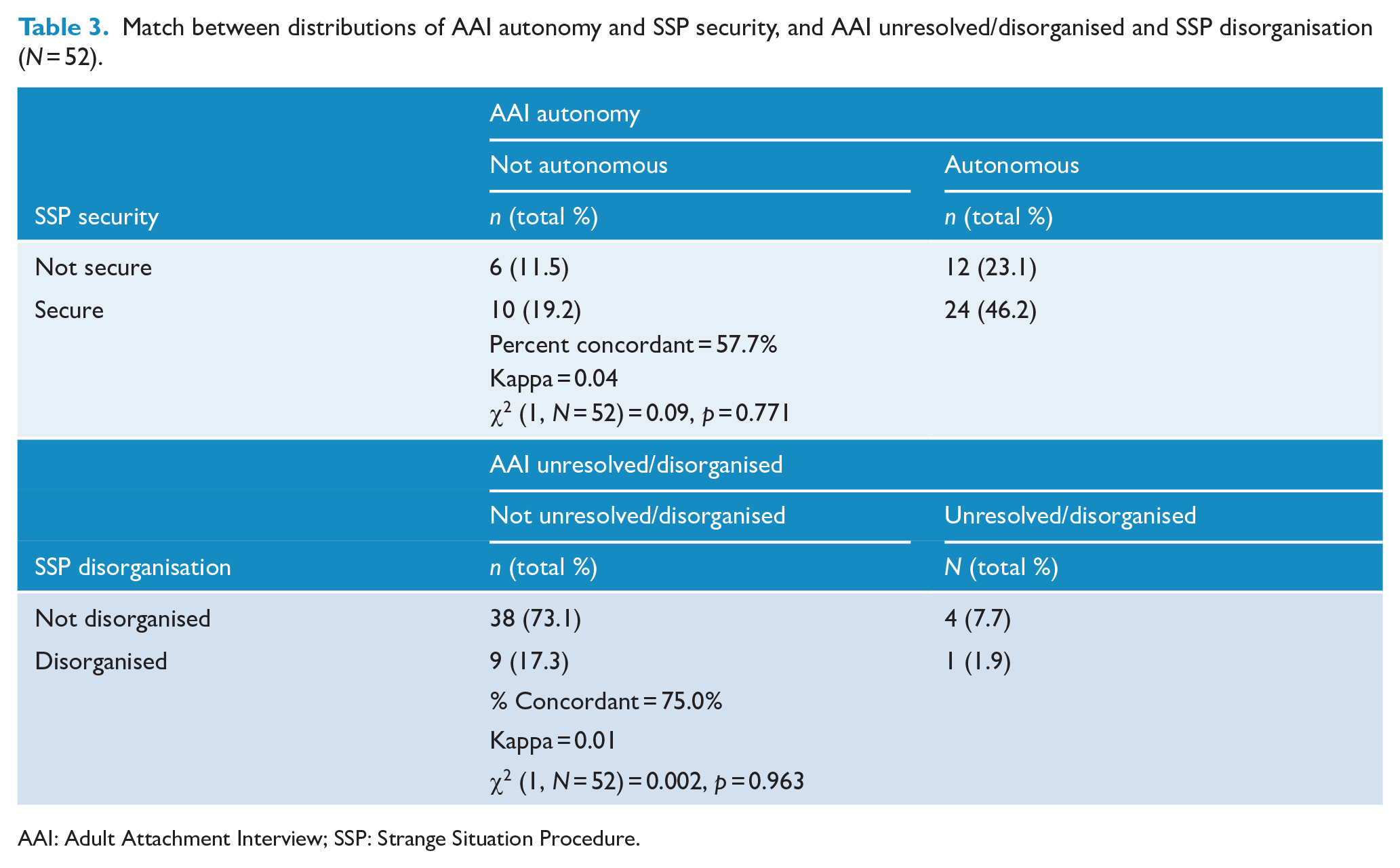
AAI: Adult Attachment Interview; SSP: Strange Situation Procedure.
Trauma, depression and maternal sensitivity associations with intergenerational attachment security
Table 4 displays zero-order bivariate correlations between AAI autonomous and SSP secure classifications, including continuous AAI and SSP scores, coherence of mind, disorganisation and Richters security and other key maternal variables. Notably, maternal autonomous state of mind with regard to attachment was negatively associated with maternal childhood trauma and significantly positively associated with maternal sensitivity at 6 months postpartum. These associations suggest that an autonomous AAI classification was less likely when women reported experiencing moderate-to-severe trauma during their childhood and was associated with higher levels of sensitivity observed from the mother to her infant at 6 months of age. There were no significant associations between maternal childhood trauma, depression and maternal sensitivity at 6 months postpartum with SSP security (measured by both secure/insecure and Richters security score) and disorganisation and AAI coherence of mind scores.
Zero-order bivariate associations between attachment security, maternal trauma and depression and parenting variables (N = 52).
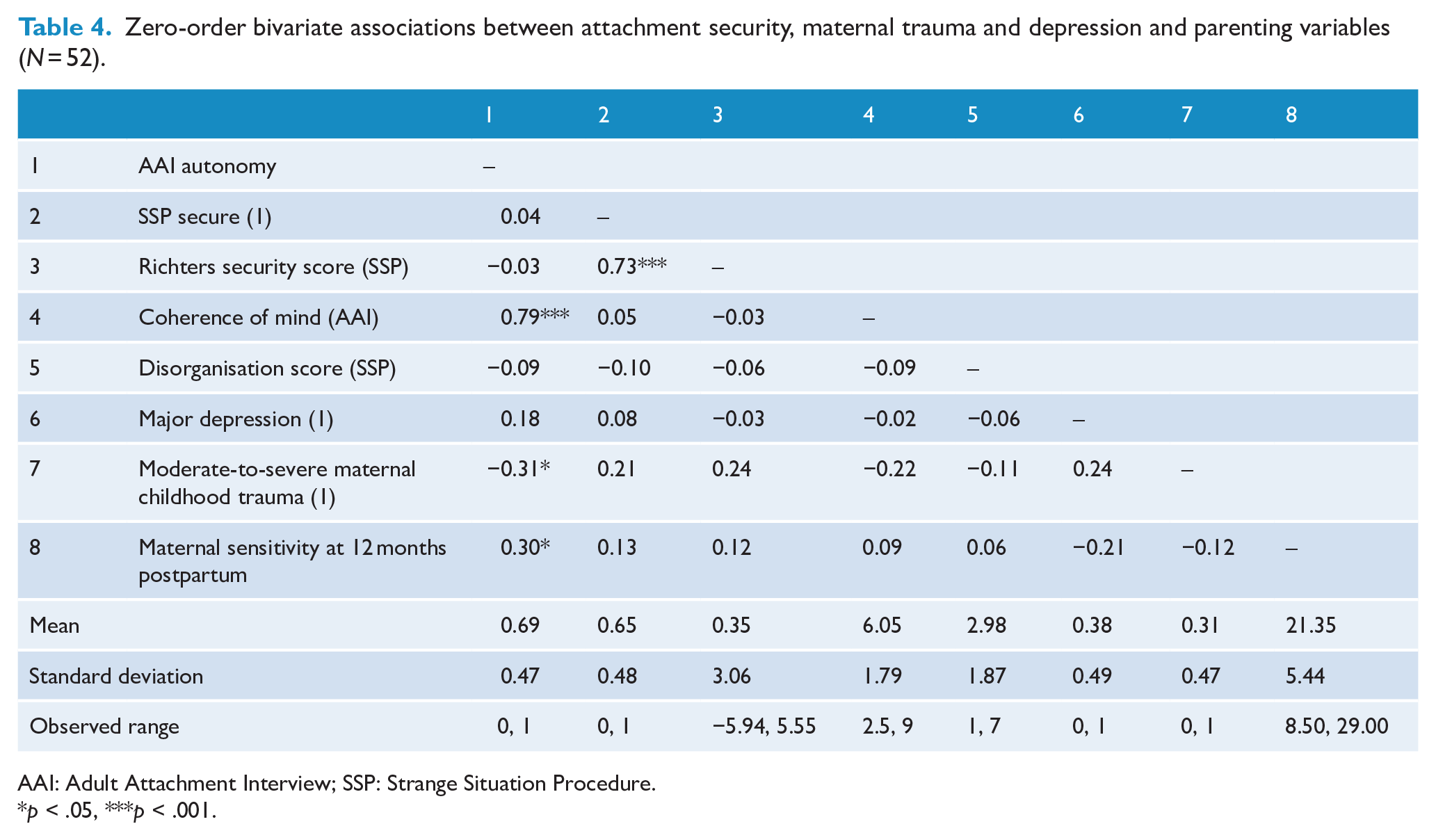
AAI: Adult Attachment Interview; SSP: Strange Situation Procedure.
p < .05, ***p < .001.
Results for the linear models predicting Richters security score (i.e. Models 1 and 2) are presented in Table 5. In Model 1, the interaction between AAI binary autonomy and maternal childhood trauma was not significant, accounting for 5.2% in variance explained in the Richters security score (achieved power = 0.51). However, the interaction between AAI autonomy and maternal major depression in Model 2 was a significant predictor of Richters security score, accounting for 8.7% of the variance in the outcome (achieved power = 0.72). For women with no major depression, the association between AAI autonomy and Richters security was not significant (b = −0.72, p = 0.492), whereas for women who met diagnostic criteria on the SCID-IV for major depression, AAI autonomy was a significant positive predictor of Richters security scores (b = 3.71, p = 0.001). The pattern of this interaction is presented in Figure 2, which indicates that for women with major depression, non-autonomous representations in early pregnancy of their early attachment to caregivers were associated with the lowest Richters security scores (i.e. insecurity); this is in contrast to women with major depression and autonomous representations of attachment to caregivers whose Richters scores were significantly higher and comparable to women without depression regardless of AAI autonomy. In conducting the alterative models replacing binary AAI autonomy groups with the continuous AAI coherence of mind score, there were no substantive differences. In fact, although there was a significant interaction between AAI coherence of mind and depression on Richters security score (β = 0.34, p = 0.026), the simple effects for each depression group of coherence of mind on Richters security were not significant.
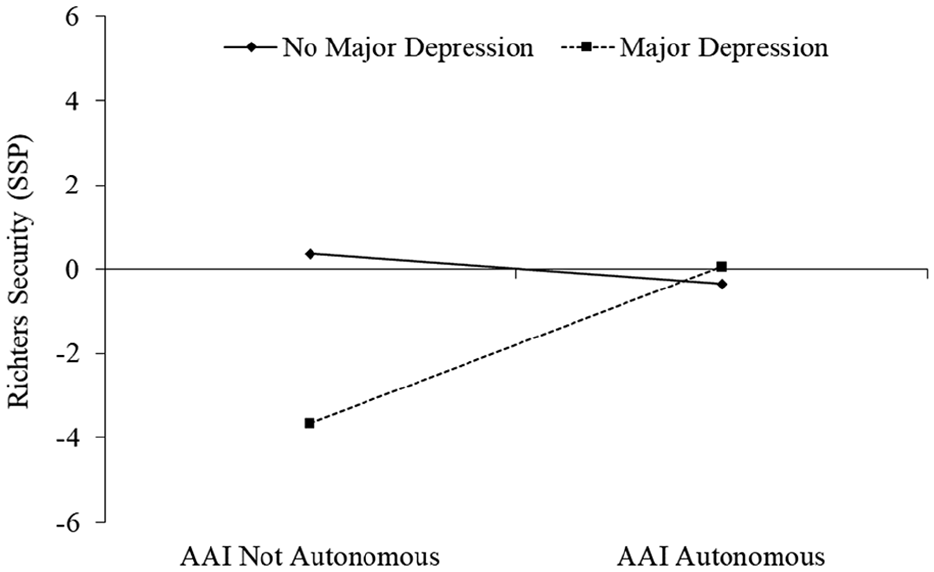
Slopes estimated by Model 2 showing the simple associations between AAI autonomy and Richters security scores for women meeting diagnostic criteria for major depression and women not meeting criteria.
Results for the linear regression models predicting the Richters security score (N = 52).
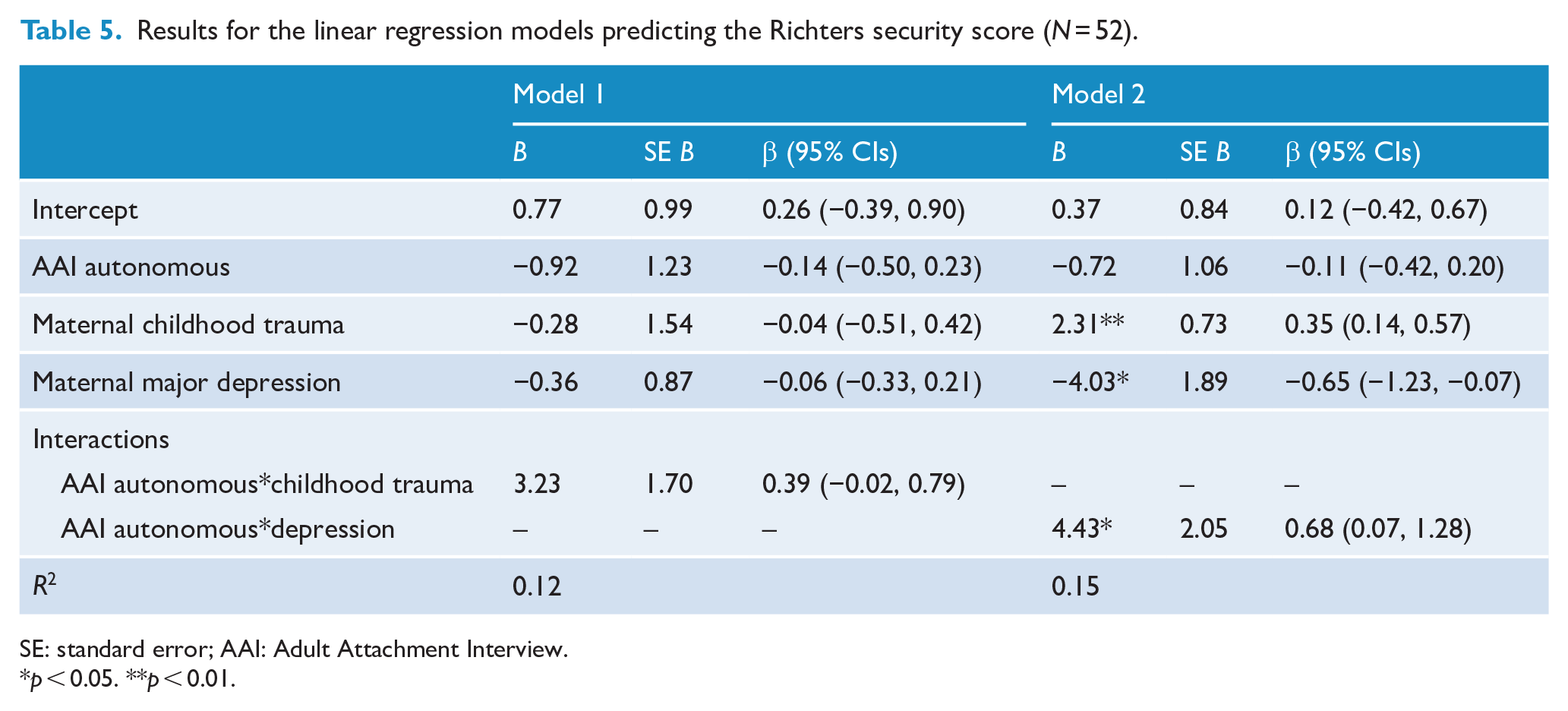
SE: standard error; AAI: Adult Attachment Interview.
p < 0.05. **p < 0.01.
For the final model, which tested maternal sensitivity at 6 months during a mother–baby interaction task as a mediator of the association between maternal AAI autonomy and Richters security score, results of the direct effects are presented in Figure 3. The bootstrapped indirect effect of AAI autonomy on Richters security through maternal sensitivity was not significant (β = 0.03 [bootstrapped 95% CIs: −0.09, 0.14], p = 0.629, partial R2 < 0.01), representing a negligible effect size. Consistent with the bivariate correlations, AAI autonomy was associated with significantly higher maternal sensitivity, but maternal sensitivity was not associated with the Richters security score. Given the prevalence of trauma and depression in this clinical pilot sample, the strength of this indirect effect may be conditioned by maternal childhood trauma, depression or other sources of stress; however, due to the limitations associated with a smaller sample, this would need to be tested using a clinical sample with larger numbers. Consistent with the non-significant bivariate correlations observed in Table 4, there were no significant effects, both direct and indirect, between AAI sense of security, maternal sensitivity and Richters security in the alternative mediation model.
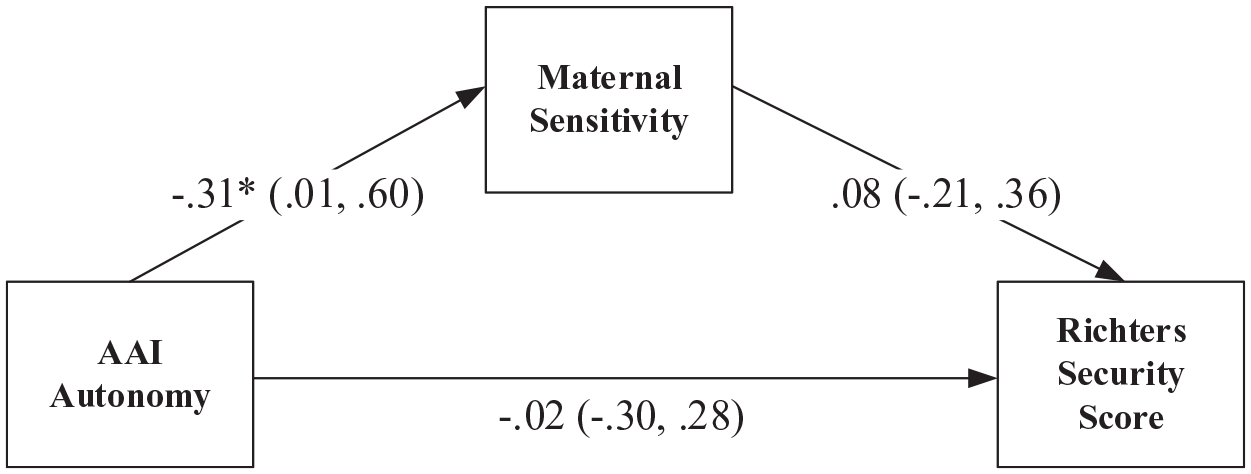
Path model showing standardised regression coefficients and 95% confidence intervals.
Discussion
Our study examining the intergenerational transmission of attachment found no significant association between maternal secure autonomous state of mind regarding attachment during early pregnancy and infant–mother attachment security at 12 months postpartum. Concordance for AAI autonomous/non-autonomous and SSP on secure/insecure attachment classification was 57.7%. This is lower than reported in previous studies specifically examining AAI in late pregnancy and subsequent SSP in infancy and also the concordance reported in a meta-analysis between adult attachment and infant/child attachment (Fonagy et al., 1991; Verhage et al., 2018). We did find for those mothers with both non-autonomous attachment state of mind and major depression in early pregnancy, this was a significant predictor of insecurity in the SSP. Maternal childhood trauma history was not a significant moderator and neither was maternal sensitivity a significant mediator for concordance of security between AAI and SSP.
There are several reasons why our findings differ from previous studies examining antenatal AAI and subsequent SSP. First, our study cohort has over-representation of women with current antenatal depressive disorder with 40% of the sample meeting current criteria for major depression in early pregnancy. There is no other study of antenatal AAI and postnatal SSP that has examined women who were assessed and met criteria for antenatal depressive disorders. While the recent meta-analysis on intergenerational attachment examined 13 clinical/at-risk samples, these combined studies with a broad range of risks including preterm birth, teenage parenthood, adoptive parents and did not specifically focus on mental health or depressive disorders (Verhage et al., 2016). Within our sample 32.7% of women had a history of moderate to severe trauma and this is consistent with previous studies within community as well as in clinical samples using the same measure (Scher et al., 2004). Second, we administered the AAI in pregnancy in first-time mothers, and in our study, this was undertaken in early pregnancy rather than late pregnancy. There have been no previous studies that we are aware of that has examined the AAI measured in early pregnancy. Furthermore, the infant–parent attachment assessed on the SSP suggests there were more disorganised infants than predicted from the antenatal maternal AAI classification undertaken in early pregnancy; this may reflect the influence of some of the samples developing depressive disorders after the AAIs were conducted. In addition, it may reflect intervening influential or traumatic events or losses in the gap in time from early pregnancy AAIs to assessment of infant–parent attachment at 12 months postpartum; this includes possible trauma associated with childbirth. Third, our sample also differs in that while there are high levels of depression, this sample is a socio-economically advantaged sample with nearly 70% university educated. This differs from either community samples or the high-risk samples where typically socio-economic disadvantage covaries with the other psychosocial risk factors. While clearly there is a need to replicate these findings in a larger sample, it is interesting to note the differences in findings for this sample for concordance for AAI and SSP.
What was surprising, but has not previously been examined, is how clinical depression in early pregnancy may influence this trajectory seen in our study particularly for women with both depression and non-autonomous AAI. While this study poses more questions than can be answered from our findings, it does shed light on recent findings from attachment interventions when specifically applied with samples of women with clinical depression. For instance, Stein et al. (2018) found no additional benefit of an attachment intervention for child and attachment outcomes compared to treating depression alone. However, they did not measure a mother’s attachment state of mind using the AAI in this study. The first randomised controlled trial of Circle of Security within a sample of women with postnatal depression found no difference in attachment between Circle of Security treatment and treatment as usual (Ramsauer et al., 2019). This study did measure both the AAI and SSP, and in a secondary analysis, they found for unresolved mothers on the AAI there was improvement in sensitivity although not attachment. Taken together with our observational findings this suggests that in future studies consideration across both attachment state of mind as well as depression is required to understand the influence of depression on transmission of attachment. Understanding this specifically in the context of current perinatal depression is vital if we are to appropriately and more specifically identify those women who require interventions and support in the development of infant–parent attachment where there is also maternal depression (Galbally et al., 2020a).
Considering these findings in the light of neurocognitive studies of the influence of clinical depression on memory and recall may also be fruitful in future research. Studies of those with current depressive disorders have found negative bias in recall as well as less details when required to provide recall autobiographical memory (Duyser et al., 2020; Kuyken and Dalgleish, 1995). How this may influence a measure such as the AAI which relies on recall and memory is unclear and requires further elucidation across those with current mental disorders. What is also unclear in the context of maternal depression and the relationship to attachment is the influence of treatment of depression, such as with antidepressant medication. While there is some evidence that this reduces parenting stress, it is unknown whether treatment may alter aspects of parental behaviour and response such as sensitivity to the infant cues or attachment (Galbally et al., 2020b). While not explored in this study it is of equal importance to consider the role of both psychological interventions and psychosocial support for managing depression and how this may be protective for attachment.
Our findings of no moderation of childhood trauma on attachment security concordance and that maternal sensitivity did not mediate attachment security concordance should both be regarded in light of the small sample size. While the recent meta-analysis did in contrast show this, it was noted the strength of this mediation was smaller in more recent studies (Verhage et al., 2016). Furthermore, the meta-analysis did not define what measures were included for parental sensitivity. Overall, this meta-analysis also noted both publication bias and decline over time of effect in findings for intergenerational transmission of attachment, an issue of replication that was noted in a recent discussion of attachment research findings (van IJzendoorn and Bakermans-Kranenburg, 2021). Our findings in a small sample using the EAS as our measure of maternal sensitivity require further replication in larger samples before any definitive conclusions can be drawn on this mediation utilising the EAS, and by testing for variation of this mediated pathway due to past maternal trauma and perinatal depression. Finally, it is important when considering these findings not to view attachment classification as analogous to psychopathology, as both AAI and SSP, while valid research measures are not valid instruments for deriving clinical diagnoses or determining clinical outcomes (Forslund et al., 2021; Granqvist et al., 2017; van IJzendoorn and Bakermans-Kranenburg, 2021).
While the strengths of our study include the quality of measurement including depression using a diagnostic measure and the inclusion of a clinical sample, measuring maternal sensitivity using an observation measure and attachment using the AAI and SSP, there are also limitations. These include the sample size and inter-rater concordance between the two coders for the SSP. The AAI and CTQ are also measures where it is unclear whether they may be influenced by the effects of current depression on autobiographical memory and recall. We also did not include samples of women with other relevant mental disorders such as bipolar disorder (Aran et al., 2021). Our sample also lacks ethnic diversity, is predominantly married and educated and lacks socio-economic diversity, and as such our findings require replication in more diverse samples as well as in larger numbers. Furthermore, we were unable to report on significant life events or childbirth-associated trauma which may have the potential to influence this transmission of attachment.
Our findings should be considered in view of these limitations and particularly the sample size of our study. Furthermore, we caution the interpretation of these findings into the premature translation in the clinical context, as recently discussed by van IJzendoorn and Bakermans-Kranenburg (2021). However, our findings do provide a valuable insight and future focus for studies understanding the influence of psychosocial risks such as mental health and the intergenerational transmission of attachment. These findings also continue to highlight the importance of identifying and treating depression as early as possible in pregnancy, not only for maternal well-being but also for the emerging relationship with their infant.
Footnotes
Acknowledgements
The authors would like to thank those who have supported the development of MPEWS including Michael Permezel, Marinus van IJzendoorn and Marian Bakermans-Kranenburg. The authors also thank staff, students and volunteers on the MPEWS study as well as study co-ordinators: Nicole Brooks and Tina Vaiano for their contribution to MPEWS. Thank you to Deane Dozier for her assistance with coding the AAIs. We are also sincerely grateful to the study participants who have contributed a substantial amount of time to participating in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study is supported through the 2012 National Priority Founding Round of Beyondblue in a 3-year research grant (ID 519240), a 2015 National Health and Medical Research Council (NHMRC) project grant for 5 years (APP1106823) and a 2015 RANZJP Pat, Toni and Peter Kinsman Research Scholarship awarded to Dr Josephine Power. Financial support has also been obtained from the Academic Research and Development Grants, Mercy Health and Centre for Mental Health and Well-Being, Deakin University.