
Abstract
Objective
Childhood maltreatment is associated with late-life depression. Preliminary evidence indicates that personality characteristics, in particular neuroticism and extroversion, and an anxious attachment style mediate this association. The objective is to evaluate 3 models, in which personality and attachment are considered mediators between childhood maltreatment and late-life depression in a socioeconomically disadvantaged Brazilian population.
Methods
This study included participants (n = 260) from socioeconomically disadvantaged neighborhoods of Porto Alegre, Brazil, who completed measures of childhood maltreatment (Childhood Trauma Questionnaire – CTQ), personality characteristics (NEO-Five Factor Inventory), attachment styles (Relationship Scales Questionnaire), and geriatric depression (Mini-International Neuropsychiatric Interview-Plus). General multiple and sequential mediation analyses were used to test for possible associations.
Results
Attachment anxiety but not attachment avoidance is a mediator between childhood maltreatment and geriatric depression. Neuroticism is a full mediator. At that, attachment anxiety was found to be a predictor of neuroticism. Finally, sequential mediation analysis shows a path from childhood maltreatment to geriatric depression through attachment anxiety and neuroticism.
Conclusions
The results suggest a pathway from childhood maltreatment to anxious attachment, which in turn predicts higher neuroticism that itself may favor late-life depression. This hypothesis could have implications for older adults living in low socioeconomic settings in that treating the high-risk group of maltreated children may help prevent late-life depression.
Introduction
Studies on mental conditions in older adults are mostly conducted in high-income countries even though most of them live in low- and middle-income countries. 1 There is a strong need for more inclusive and diverse population studies in this field. Looking into these socioeconomically disadvantaged populations is important as they present a high prevalence of depression averaging around 30% 2 and must cope with poverty that is related to maltreatment in the course of their development.
Childhood maltreatment can lead to long-term consequences and may contribute to the development of mental disorders throughout life.3-7 Low- and middle-income countries present higher maltreatment scores in comparison with the high-income ones. 8 In late life, childhood maltreatment is strongly associated with physical and mental health disorders, especially geriatric depression.9-11 Although it is important to help in the development of preventive and curative strategies to prevent depression in older ages, the mediators of the relationship between childhood maltreatment and depression in later life remain poorly investigated, attachment types and personality characteristics are plausible ones based on previous research.
Attachment styles are probable mediators since they are correlated to childhood maltreatment and geriatric depression. Only 1 study tested a mediator effect of attachment between childhood maltreatment and depression, finding the anxious, but not avoidant attachment style to be a mediator. 12 Attachment styles are also correlated with a wide variety of mental disorders, 13 especially with depression both in younger and older adults.14-16 In older adults, the severity of depression is correlated with dysfunctional attachment patterns. 16 Specific attachment styles were associated with childhood maltreatment subtypes in adults. For example, maltreated infants are more likely to develop an insecure or disorganized attachment style, 17 emotional and sexual maltreatment is correlated with anxious and avoidant attachment styles, 18 and physical abuse is correlated with attachment anxiety. 19
Adaptive personality characteristics predispose to successful aging and increased longevity.20,21 Conversely, they have been extensively investigated as mediators of the relation between childhood maltreatment and geriatric depression. Especially investigated was the neuroticism that moderates the relationship between stress exposure,22,23 childhood maltreatment, 24 and depression in adulthood and later life. A high level of neuroticism is associated with both adult depression22,25 and late-life depression.26-29 Neuroticism was found to be associated with childhood maltreatment.30-33 Previously, in single mediation analysis, neuroticism and extroversion were found to be complete mediators between childhood maltreatment and geriatric depression. 34
The foundation of the attachment style begins with the interactions with the parents during childhood, negative interactions such as early maltreatment have an influence on the development of secure attachment. Attachment insecurity is a central component of many personality disorders. 13 Anxiety and avoidant attachment styles may favour the development of dysfunctional personality traits later in adulthood that finally influence older age psychopathology.
As based on previous evidence in the literature, we hypothesize a wider and more direct multiple mediation effect of all 5 personality factors mainly due to neuroticism. We also wish to test the 2 attachment styles anxiety and avoidant in a multiple mediation analysis. Finally, we hypothesize a participation of attachment in the development of geriatric depression passing mainly through personality, to test this we use both multiple and sequential mediation models.
Methods
Participants
Our sample comprised 260 older age subjects who had participated in the “Cerebral Aging Program (PENCE)” study, which was conducted between July 2015 and July 2016 in collaboration with the Family Health Strategy (FHS) program in Porto Alegre, Brazil. PENCE aims to examine mental health in a socioeconomically disadvantaged sample of people 60 years old or older. The cross-sectional study presented here is a subproject of the PENCE cohort study.
General practitioners recruited participants in health clinics located within the participants’ neighborhoods. The family Health Strategy is part of the public health system who covers mainly poor communities in Brazil. They referred them to the São Lucas Hospital of Pontifical Catholic University of Rio Grande do Sul (PUCRS) for a face-to-face interview in order to assess the patient’s eligibility to enter the study. Exclusion criteria were a diagnosis of bipolar disorder, drug or alcohol abuse, a history of neurological disease (eg, tumor, cerebral ischemia, or epilepsy), a serious or incapacitating clinical disease that could interfere with the study assessment (eg, cancer or major visual impairment), and the inability to understand the questions. Inclusion criteria were age ≥60 years and adequate fluency in Brazilian Portuguese. Assessments were performed by board-certified psychiatrists and psychologists experienced in late-life neuropsychiatric disorders. Of the 346 subjects referred by the general practitioners, 260 were included in the study. All subjects who had clinical needs due to a psychiatric or neurological diagnosis were referred further to specialized consultations in the same hospital. The research ethics committees of both PUCRS and the Public Health Secretary of the City of Porto Alegre (Brazil) approved the research protocol. All participants or their legal representatives provided informed written consent and they received no compensation or reimbursement for participating in the study.
Measurements
Psychiatric disorders, including current depression, previous episode(s) of depression, posttraumatic stress disorder (PTSD) and generalized anxiety disorder (GAD), were diagnosed according to the Portuguese version of the Mini-International Neuropsychiatric Interview 5.0 Plus (MINI Plus), 35 which is a diagnostic algorithm based on the DSM-IV criteria that uses the symptoms and frequencies of each condition. Its accuracy is similar to that of more complex psychiatric interviews in different settings. 36
Childhood maltreatment was assessed using the shorter version of the Childhood Trauma Questionnaire (CTQ) 37 ; translated into Brazilian Portuguese 38 and validated for community and clinical samples, with good reliability and validity. 39 The CTQ is composed of 28 questions that evaluate a variety of maltreatment experiences (ie, emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect) as well as their intensity on a five-point Likert scale, yielding a maximal score of 140. The sum of the 5 low-to-moderate cut-offs (total ≤51) proposed in the administration manual was used.
Personality characteristics were assessed by the NEO-Five Factor Inventory (NEO-FFI. 40 ; The NEO-FFI is a 60-item, shortened version of the NEO Personality Inventory-Revised, which was translated into and validated for Brazilian Portuguese (Costa and McCrae, 2007). It measures the Big-Five personality domains of neuroticism, extroversion, openness to experience, conscientiousness, and agreeableness. High scores of neuroticism suggest emotional instability, susceptibility to psychological stress, maladjustment, and negative emotionality; extroversion is characterized by being energetic and assertive; openness to experience is described as being imaginative, independent-minded, and intellectually curious; conscientiousness is described as being responsible, dependable, and orderly; and agreeableness is characterized by empathic and cooperative behaviors. The extent to which a statement applies to the participant is rated on a 5-point Likert scale ranging from “strongly disagree” to “strongly agree”.
Attachment was assessed using the Relationship Scales Questionnaire (RSQ) according to the two-factor model of attachment (self-model–anxiety and others model–avoidance). 41 The RSQ assesses close relationships and more specifically relationships between romantic partners. The RSQ was translated into and adapted to Brazilian Portuguese. 42 To define avoidance and anxiety we used the proposal by Simpson et al (1992) as suggested by Kurdek, 2002), namely avoidance items 10, 12, 13, 15, 20, 24, 29, 30 and anxiety items 11, 18, 21, 23, and 25 of the RSQ questionnaire; this model yielded better goodness-of-fit values relative to other RSQ models 43 .
Statistical Analysis
Descriptive statistics were used to characterize the sample and to compare these characteristics between the 2 subgroups with and without depression. The social variables tested were age, sex, and level of education (years). They were used together with the Big 5 personality domains, attachment styles, GAD, PTSD and CTQ scores to compare the late-life depression group and the group without depression using chi-square and t-tests and Fisher’s exact test as appropriate.
To examine to what degree the relationship between childhood maltreatment and late-life depression is explained by attachment and personality multiple mediation analysis was used. This tool allows the measurement of the direct and indirect effects of childhood maltreatment on late-life depression, and it assesses whether the set of mediators transmits the effect of the independent variable to the dependent variable. The mediators in question were the Big 5 personality domains (ie, neuroticism, extroversion, agreeableness, openness to experience, and conscientiousness) and the 2 attachment styles (ie, anxious and avoidant).
The first model tested the 5 personality characteristics as a multi-mediation model between the CTQ childhood maltreatment score and the presence of late-life depression. The second model tested both attachment styles, ie avoidance and anxiety, as a multi-mediation model between the CTQ childhood maltreatment score and late-life depression. The third sequential mediation model included attachment styles and personality domains in a sequential way using structural equation modeling technics.
Moreover, as late-life depression was the primary outcome and a binary variable a generalized linear model was used to fit the mediation model as suggested elsewhere. 44 As mentioned, the exposure variable in each model was the total CTQ score. All models were controlled for age, sex, level of education, GAD, PTSD, and a history of past depression. A large number of bootstrap iterations (1000) allowed measuring the uncertainty of estimated parameters (total effect, indirect and direct effect etc. 45 The confidence intervals were constructed using the bias corrected bootstrap percentile. 46 We considered in all analyses the 95% confidence intervals calculated based on the normality assumption of the estimates.
Based on the findings (cf. Results) we further performed a post-hoc sequential mediation analysis of anxiety attachment and neuroticism as mediators between the CTQ score and geriatric depression.
All calculations were performed using the R software environment for statistical computing. Multiple and sequential mediation models were fitted via the lavaan package for R. 47 We used “SEM” function to fit our mediation models as structural equation models.
Results
Sample Characteristics
The mean age of the whole sample was 72.2 years, with a mean of 4.7 years of education, and 77% were women. No differences were found between the groups with and without depression with respect to age, sex, and education level.
Descriptive statistics and associations with depression.
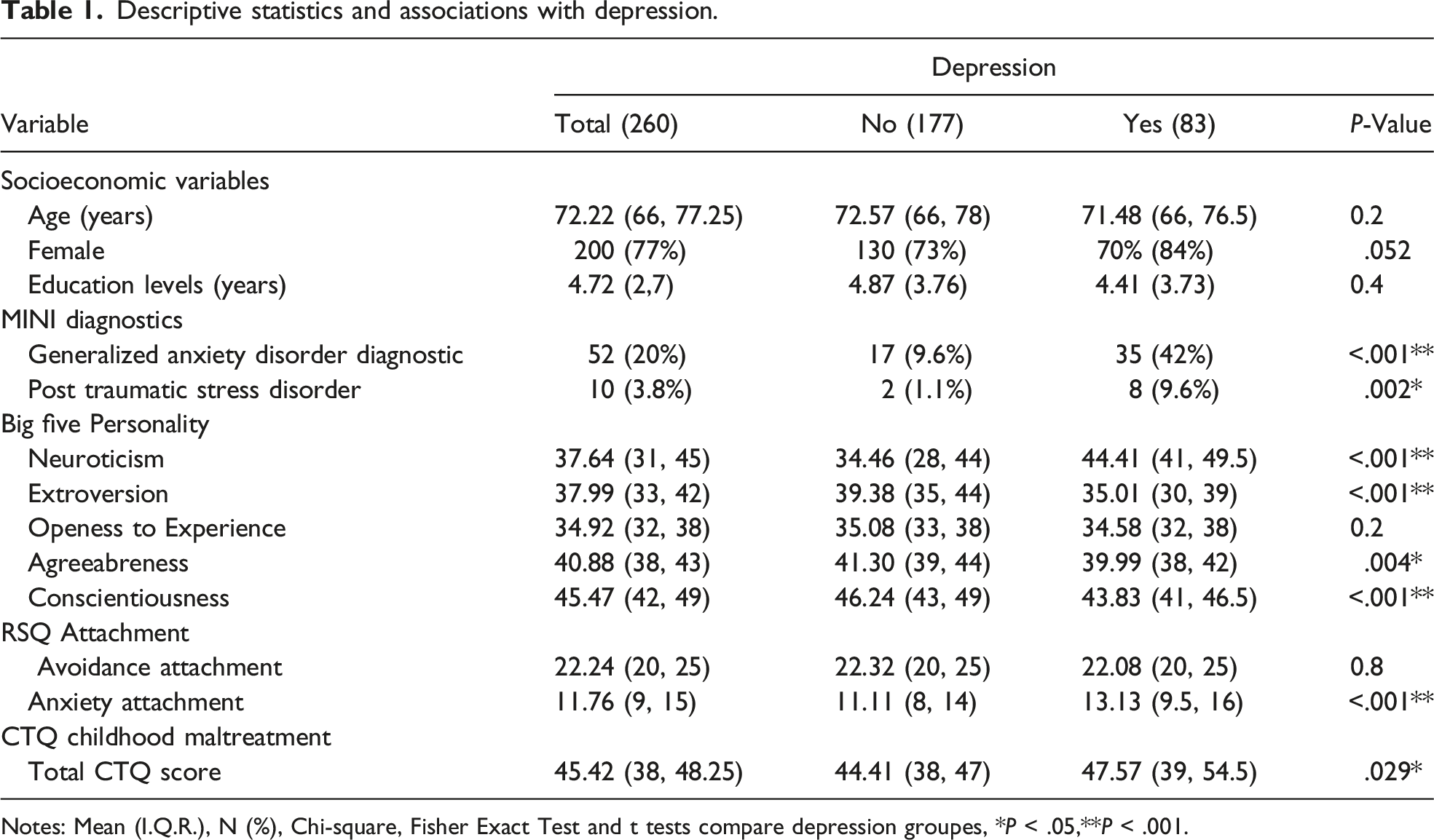
Notes: Mean (I.Q.R.), N (%), Chi-square, Fisher Exact Test and t tests compare depression groupes, *P < .05,**P < .001.
The depression group suffered significantly more often from generalized anxiety disorder (P <.001) and PTSD (P = .002). This group presented higher scores on neuroticism (P <.001) and lower scores on extroversion (P < .001), agreeableness (P = .004), and conscientiousness (P < .001).
Attachment Styles and Personality Multiple-Mediation Models
Multiple mediations models between childhood maltreatment and geriatric depression.
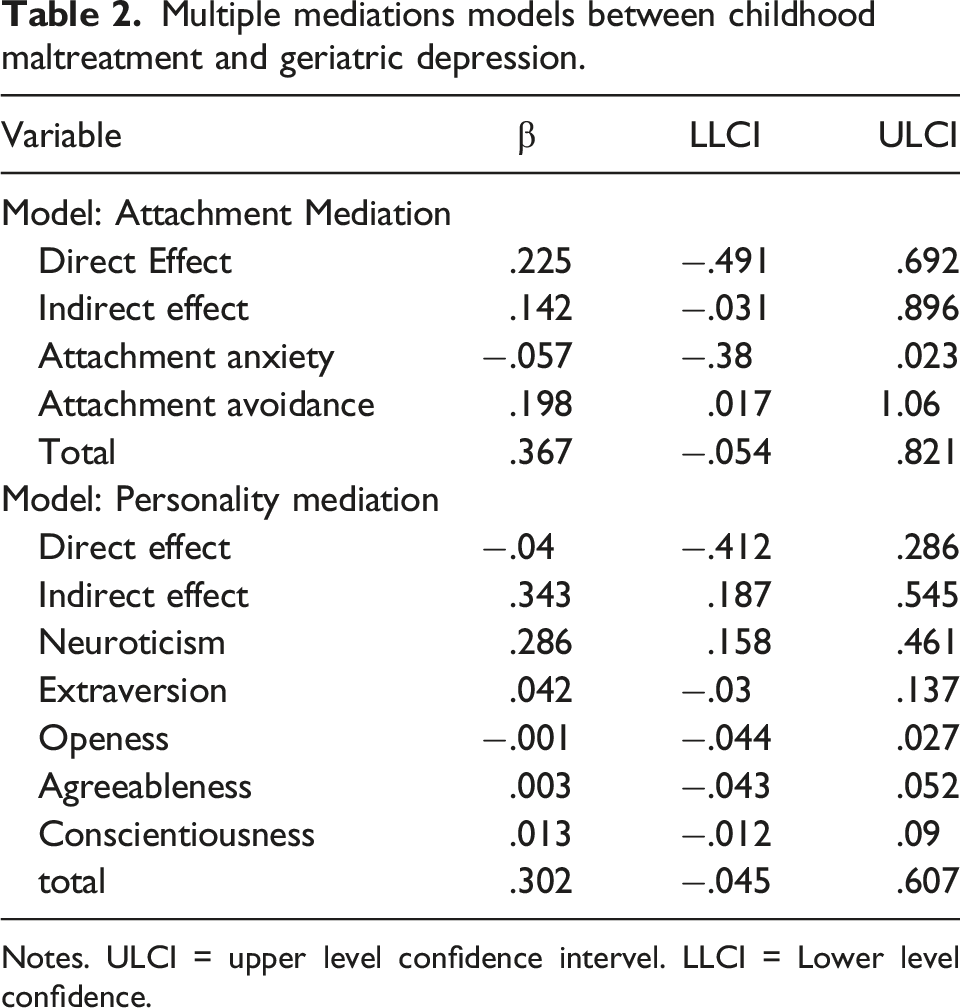
Notes. ULCI = upper level confidence intervel. LLCI = Lower level confidence.
The second multiple mediation analysis of the mediating role for the personality domains found a total indirect effect of the 5 traits (β = .343, 95%CI [.187,0.545]). More specifically, this effect was due to neuroticism (β = .286, 95%CI [.158, .461]) (cf. Table 2) (cf. Figure 1).
Regression Analysis
Regression analysis showed that attachment anxiety, but not attachment avoidance, was a predictor of neuroticism (β = .95, 95%CI [.66, 1.19], P <.001) after adjustment for age, sex, and years of education. Among these, female sex was also a significant predictor ((β = 4.64, 95%CI [2.26, 7.03], P <.001).
Given this result, we decided to carry out a further analysis and to look at the sequential mediation path including attachment anxiety and neuroticism.
Sequential Mediation of Attachment Anxiety and Neuroticism
Model Attachment > Personality (sequencial mediation).
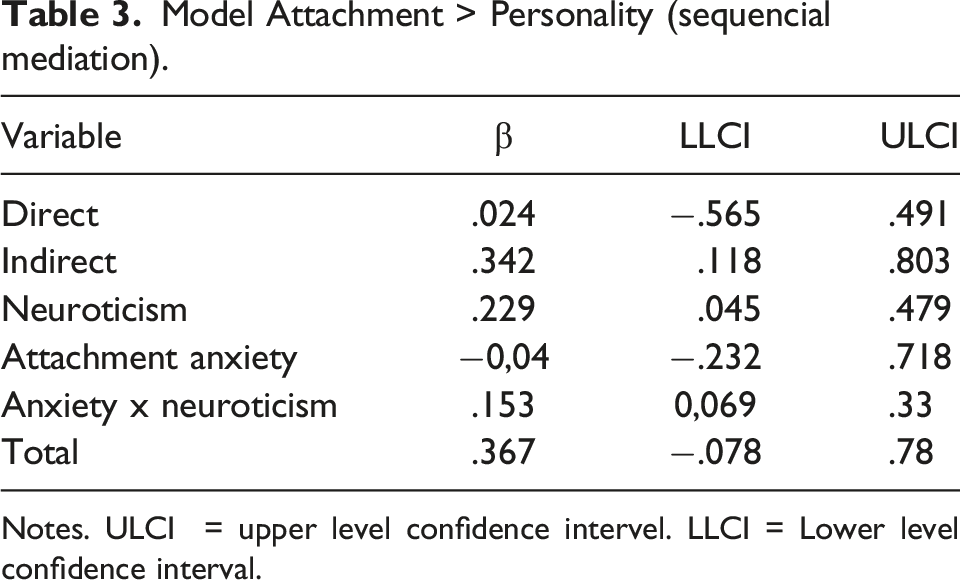
Notes. ULCI = upper level confidence intervel. LLCI = Lower level confidence interval.
Discussion
In this low socio-economic convenience sample of older adults, attachment anxiety as opposed to avoidance is a mediator of the relation between childhood maltreatment and geriatric depression. Moreover, neuroticism was a mediator unlike the other personality domains. Furthermore, childhood maltreatment predicted attachment anxiety that in turn predicted neuroticism. Additional sequential mediation analysis confirmed the path from childhood maltreatment to geriatric depression first through attachment anxiety and then neuroticism.
The temporal relationship between negative experiences during childhood predisposing and the development of dysfunctional attachment as this study suggests is in keeping with the original theory of attachment stipulating that the quality of early maternal parenting is related to the attachment style in adulthood. 13 In this study, only attachment anxiety but not avoidance is a mediator between childhood maltreatment and late-life depression, a finding that is similar to that of another study. 12 However, both attachment anxiety and attachment avoidance are related to a greater risk of depression in adulthood. 13
Why avoidant attachment is no mediator in our sample remains elusive. However, higher attachment anxiety as opposed to avoidance scores are correlated with higher levels of stress as suggested by hypothalamic–pituitary–adrenal (HPA) axis activation and subjective reports of negative affect, which is suggestive of higher levels or neuroticism. 48 Attachment anxiety in particular may favour the development of neuroticism. Indeed, observations of and interactions with early attachment figures may provide models to the child of how to deal with emotions that in turn influence the development of personality characteristics.13,49 Both attachment anxiety and neuroticism are well-validated constructs that remain stable over time. Of note, some may argue that, conceptually, attachment anxiety and neuroticism are similar if not identical constructs. However, although they share the facet of insecurity, 50 they are not the same construct. Indeed, attachment anxiety refers to the worry about being rejected or unloved in close relationships, while neuroticism is a more general personal characteristic referring to high negative affect, anxiety, worries, and loneliness. Similarly, others differentiated the Big 5 personality domains and attachment styles, but acknowledge that neuroticism is strongly negatively correlated with self-esteem and could serve as a marker for the anxious attachment style. 41
Following up on our previous study, 34 our results confirm the role of neuroticism as a mediator between childhood maltreatment and late-life depression after controlling for sociodemographic and concomitant psychopathology. However, extroversion is no longer a complete mediator in our model, as opposed to the single mediator model. Overall, this is in accordance with other studies corroborating that higher levels of neuroticism appear to mediate the relationship between childhood maltreatment and late-life depression. 24 Our results suggest a chronological relationship between exposure to childhood maltreatment and the development of personality characteristics later in life. Childhood maltreatment is an early negative experience that affects the brain during sensitive neurodevelopmental periods and may contribute to or expedite the development of later dysfunctional personality characteristics by altering stress sensitivity. 51 Thus, individuals with higher levels of neuroticism are more prone to the depressogenic effects of adversity 22 and stressful life events. 23
This study focuses on a population that is extremely large worldwide but hardly ever the target of research. Low education levels are ubiquitous in socio-economically poor communities living in precarious conditions. Poverty may well aggravate the negative effects of childhood trauma and contribute to fostering dysfunctional patterns of attachment and personality that themselves increase the risk of late-life depression. Among many other difficulties that were exposed, studying the pathways that lead to geriatric depression could help the development of curative and preventive strategies to improve mental health and surpass poverty.
Limitations and Strengths
Among other shortcomings, although the sequential mediation analysis suggests a temporal sequence of events, the cross-sectional design prevents from any causal conclusions. The retrospective assessment of childhood maltreatment and early attachment styles clearly limits the impact of our conclusions. Indeed, prospective and retrospective measures may identify different groups of individuals in relation to childhood maltreatment. 52 However, prospective studies over the entire human life course are extremely difficult to conduct for obvious reasons. Also, self-reporting of attachment style particularly attachment avoidance can be influenced by depression.
Furthermore, the study is based on a small convenience sample living in poor environments that may not be representative of larger communities, thereby limiting the generalizability of our conclusions. The study was carried out in communities known for their precarious conditions, but other socioeconomic variables, apart from education, are not available. The scarcity of studies within the realm of socioeconomically disadvantaged older age populations should be counter-acted upon in spite of the many difficulties including limited or hampered access to these communities, gang violence, and poor health resources.
Despite few studies at hand for confirmation, we expect more childhood maltreatment, neuroticism, attachment anxiety and depression in this population in comparison with those of a higher socioeconomic background. More generally, we would expect an increase of the negative consequences of poverty on this mediation pathway.
A previous episode of depression is among the more important risk factors for the development of late-life depression and our results support this fact. Therefore, we have controlled for this variable in all mediation analysis as well as for age, sex, level of education, and a diagnosis of generalized anxiety or PTSD. The time interval between past episodes of depression, as a possible mediator, and study baseline was not recorded.
We are aware of no other studies investigating a combination of personality and attachment factors in a multiple and sequential mediation model. Ours is also 1 of the few studies we know of investigating socioeconomically disadvantaged older adults in a middle-income country.
Conclusions and Future Directions
Anxious attachment seems to mediate the relationship between childhood maltreatment and geriatric depression through the pathway of higher levels of neuroticism. This study tries to shed some light on these complex developmental issues. Acting preventively upon childhood maltreatment may not only favor child development but also decrease the incidence of late-life depression in the seniors living in poor neighborhoods of many low and middle-income countries. This Hypothesis should be tested in larger and more diverse population. Also, it could be important to develop treatment strategies focused on these attachment and personality characteristics aiming to prevent the development of psychopathology in these maltreated seniors.
Footnotes
Acknowledgments
The authors would like to acknowledge the collaboration of professionals from the Family Health Strategy in Porto Alegre, Brazil.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the CAPES (Coodernação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil) scholarships, the PVE program (Programa Professor Visitante Especial) – finance code 001, PUCRS (Pontifícia Universidade Católica do Rio Grande do Sul), and the Swiss National Fund (FNS 320030_153378/1).