
Abstract
Background:
Refugees can suffer many experiences that threaten their trust in others. Although models of refugee mental health have postulated that attachment securities may be damaged by refugee experiences, this has yet to be empirically tested. This study aimed to understand the relationship between the nature of traumatic experiences sustained by refugees and attachment styles.
Method:
In a cross-sectional study, treatment-seeking refugees (N = 134) were assessed for traumatic exposure using the Harvard Trauma Questionnaire and Posttraumatic Diagnostic Scale. Attachment style was assessed using the Experiences in Close Relationship Scale.
Results:
Whereas gender and severity of interpersonal traumatic events predicted avoidant attachment style (accounting for 11% of the variance), neither these factors nor non-interpersonal trauma predicted anxious attachment.
Conclusions:
Exposure to interpersonal traumatic events, including torture, is associated with enduring avoidant attachment tendencies in refugees. This finding accords with attachment theories that prior adverse interpersonal experiences can undermine secure attachment systems, and may promote avoidance of attachment seeking. This finding may point to an important process maintaining poor psychological health in refugees affected by interpersonal trauma.
Introduction
There are estimated to be over 59 million refugees and internally displaced persons worldwide (United Nations High Commissioner for Refugees [UNHCR], 2014). Refugees commonly report an array of adverse experiences, including severe, multiple and sequential traumatization that can involve torture, assault and traumatic loss (Hollifield et al., 2002). Not surprisingly, elevated rates of trauma-related psychological disorders, including posttraumatic stress disorder (PTSD), depression and anxiety have been documented in refugees (Fazel et al., 2005; Heeren et al., 2012; Johnson and Thompson, 2008), and especially those affected by torture (Steel et al., 2009). Moreover, refugees show poorer response to treatment than others who suffer from posttraumatic stress conditions (Nickerson et al., 2011).
It has been proposed that one of the reasons refugees experience marked psychological difficulties is that a significant proportion of their traumatic history is characterized by interpersonal violence, including torture, rape and other forms of assault (Nickerson et al., 2011). There is solid evidence across various samples that interpersonal trauma results in more severe adverse psychological effects than other forms of traumatic experience (Forbes et al., 2012, 2014; Norris, 1992; Scott and Babcock, 2010). It has been suggested that interpersonal trauma may threaten one’s capacity to trust others, and this heightens one’s sense of vulnerability and can intensify posttraumatic stress reactions (Foa et al., 1989; Nickerson et al., 2014b).
It has been proposed that one central effect of prolonged interpersonal trauma and the culmination of numerous losses experienced by refugees is fragmentation of their attachment systems (Silove, 1999). This proposal accords with qualitative evidence that refugees experience disruptions to close attachments as a result of their traumatic and separation experiences (De Haene et al., 2010), and that recovery is associated with restored attachments (Ajdukovic et al., 2013). Attachment theory holds that people are programmed from an early age to seek the support of others at times of need, and that this reaction is activated whenever people are under threat (Bowlby, 1969). There is much empirical evidence that people do seek attachment figures during stress (Mikulincer et al., 2001, 2002), and that the availability of real or symbolic representations of attachments confer considerable psychological benefit (Mikulincer and Shaver, 2007). It has also been shown that priming people who have elevated posttraumatic stress with attachment representations reduces cognitive responses typically observed in PTSD (Mikulincer et al., 2006).
The extent to which people can benefit from attachment availability appears to be moderated by individual differences in how people seek attachments in response to stress. Attachment theories propose that prior experiences of unreliable relationships lead to differences in how individuals are able to benefit from attachments; prior experiences of unavailable or hostile attachment figures can result in people either excessively seeking attachments because they fear that support will not be provided, or avoiding attachments because they have learnt that attachment figures do not provide support during times of threat (Mikulincer et al., 2005). That is, people with avoidant attachment tendencies distance themselves from attachment figures as a means of coping (i.e. they hypoactivate the attachment system), while those with anxious attachments tend to hyperactivate their attachment needs as they search for attachments (Mikulincer and Shaver, 2007). Consistent with these predictions is evidence that, under conditions of threat, avoidantly attached individuals reduce proximity-seeking behaviour and are less likely to activate attachment representations (Mikulincer et al., 2005). People can be high and/or low on each attachment style, and thus the two attachment dimensions are not mutually exclusive. For example, people who are high on avoidant and low on anxious attachment tendencies may be described as ‘dismissive’ (insofar as they distance themselves with little anxiety), while those high on avoidant and high on anxious attachment tendencies have a ‘fearful avoidance’ (involving avoidance in association with anxieties about insecure attachment, presumably as a coping response to being abandoned) (Mikulincer et al., 2005). Attachment theories traditionally posit that the predominant influence on one’s attachment style is the experiences they have with primary caregivers during formative developmental years during childhood, and that these attachment tendencies persist to adulthood (Bowlby, 1969). More recent adaptations of attachment theory propose that other life experiences can modulate attachment style, including events that violate one’s secure attachment representations (Defrin et al., 2013).
Despite the many commentaries on the potential impact of refugee experiences, interpersonal trauma and torture on attachment, there is very little quantitative study of this issue. On the premise that torture, interpersonal persecution and forced separation from loved ones may disrupt one’s attachment system, it is possible that refugee experiences may be associated with fragmented attachments. In this context, it is interesting that one study of prisoners of war found that priming attachments did not provide benefit to these individuals, possibly because they may lack the requisite secure attachment systems necessary to benefit from attachments (Mikulincer et al., 2014). The present study represents an initial investigation of attachment styles of refugees and attempts to shed empirical light on the notion that insecure attachments are associated with severe and interpersonal trauma. On the basis that torture and other forms of interpersonal persecution may undermine attachment security, we hypothesized that the degree of interpersonal trauma experienced by the refugees (but not non-interpersonal trauma) would be associated with insecure attachment tendencies.
Method
Participants and procedure
The study was approved by the Ethics Committee of the Cantons of Zurich and Bern, Switzerland, and was conducted in compliance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). The data presented in this paper were collected between May 2012 and August 2013 in the context of a broader study of adjustment of traumatized refugees (Nickerson et al., 2015a, 2015b; Schnyder et al., 2015). Participants were refugees or asylum seekers who had survived war and/or torture. They came from a variety of refugee backgrounds (see Table 1) and were currently receiving treatment at the outpatient units for victims of torture and war in either Zurich or Bern for their trauma-related mental health problems. Further inclusion criteria were written informed consent, being 18 years or older and speaking one of the study languages (i.e. German, English, Turkish, Arabic, Farsi, and Tamil). Patients were excluded if, on the basis of clinician judgement, they were (a) cognitively unable to use a therapist-assisted computer-based assessment tool (Knaevelsrud and Müller, 2008), (b) had severely impaired distress tolerance (including severe dissociative symptoms), (c) psychotic, (d) acutely suicidal, or (e) had borderline personality disorder; these clinical judgements were made in consultation with the refugee’s therapist. Although 152 patients were eligible for the study, informed consent was obtained from 137 patients (90.1%), of whom 134 patients completed the research session (three did not complete because of scheduling difficulties).
Sociodemographic characteristics of N = 134 treatment-seeking traumatized refugees and asylums seekers.
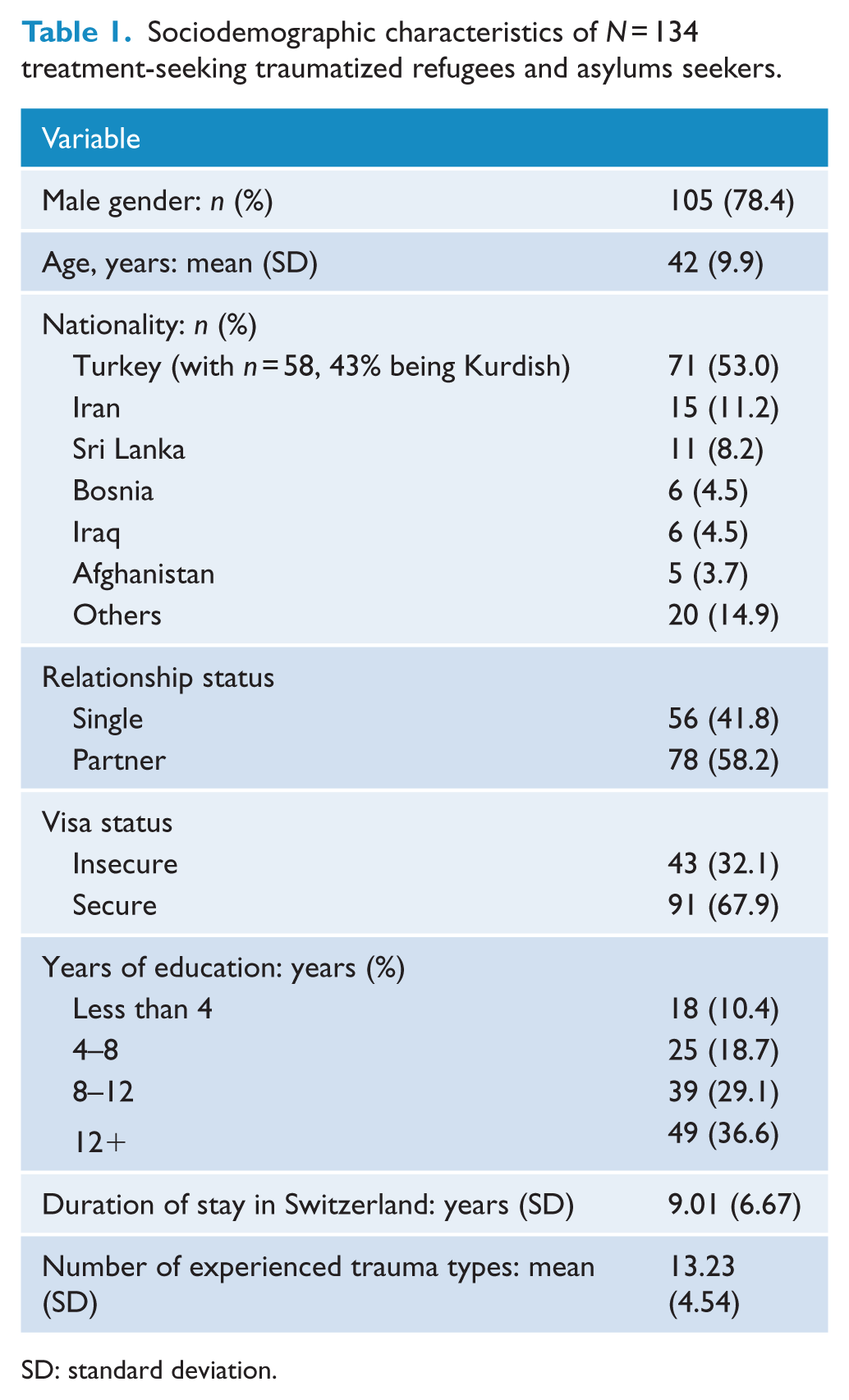
SD: standard deviation.
A therapist-assisted computer-based assessment tool was used to implement the self-report measures (MultiCASI; Knaevelsrud and Müller, 2008). In MultiCASI, participants can read each item and see the range of possible responses in their respective mother tongue on a tablet screen and – in case of illiteracy – can listen to the audio-recorded items/responses. Items are answered by touching the screen. A study team member explained the purpose of the study to potential participants. Written informed consent was obtained from all participants. Participants were informed that they were free to withdraw from the study at any time without jeopardizing their ongoing treatment. Participants attended a research assessment of 60–120 minutes duration; they obtained CHF 40 (approximately USD 40) for participation.
Measures
The measures used in this study were translated into Turkish, Arabic, Farsi and Tamil by accredited translators. Blind back-translation procedures were also implemented (Bontempo, 1993), with differences between the two translations being rectified by independent bilingual individuals experienced in working with health-related questionnaires.
Potentially traumatic events (PTEs) were measured by combining the trauma event lists of two standardized questionnaires, the Harvard Trauma Questionnaire (HTQ) (Mollica et al., 1992) and the first part of the Posttraumatic Diagnostic Scale (PDS) (Foa, 1996; Foa et al., 1997). This combined scale indexes exposure to 23 types of traumatic events associated with the refugee experience and traumatic experiences associated with other civil trauma. A count of the number of types of PTEs experienced by each participant was computed. Fifteen of these PTEs were classifiable as interpersonal, whereas eight were non-interpersonal (see Table 2), respectively.
Interpersonal and non-interpersonal trauma exposure reported by 134 treatment-seeking refugees and asylum seekers.
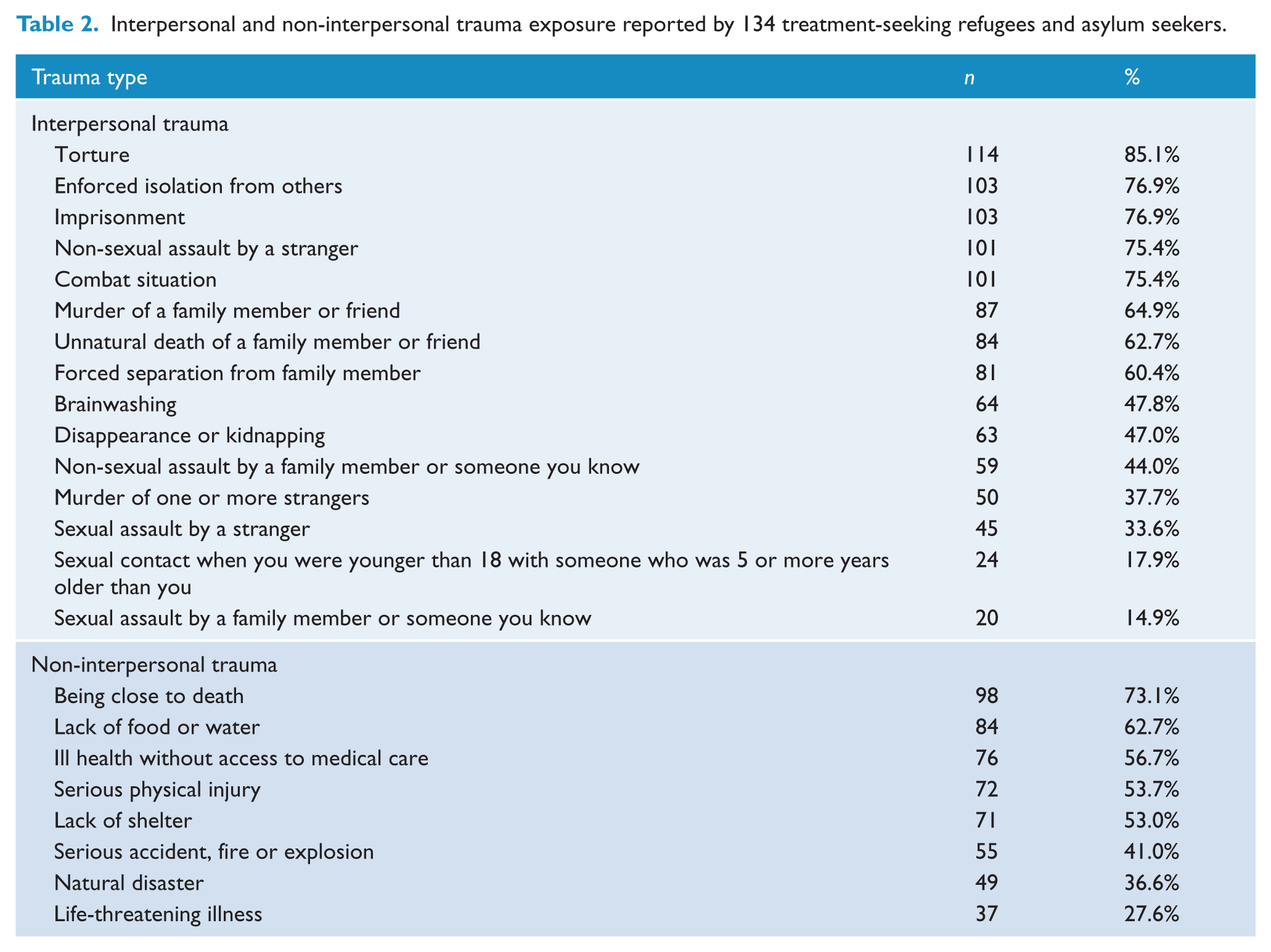
Participants in this study had experienced a mean of 13.23 (SD = 4.54) types of PTEs. Over 85% of the sample had been tortured (n = 114, 85.1%), and over three-quarters had experienced forced isolation from others (n = 103, 78.0%), had been imprisoned (n = 103, 76.9%), assaulted (n = 101, 75.4%) or had been exposed to combat situations (n = 101, 75.4%).
Attachment was assessed with the 12-item version of the Experiences in Close Relationship Scale (ECR; Wei et al., 2007). The ECR scale indexes two subscales assessing anxious and avoidant attachment style (mapping onto attachment theory’s dimensions of anxious and avoidant attachment tendencies), with each item rated on a 7-point scale (1 = strongly disagree, 7 = strongly agree) in relation to how they feel currently towards their attachment figures. Following previous adaptations of the ECR, we referenced each question to ‘someone who I consider close to me’ (Bryant and Chan, 2015). High scores on the anxious attachment dimension indicate intense worries about separation and fear of abandonment by others (e.g. ‘I worry about being abandoned’). High scores on the avoidant attachment dimension indicate distancing from emotional connections (e.g. ‘I don’t feel comfortable opening up to others’). The subscales in this study have reasonable internal consistency (anxious attachment: α = 0.79; avoidant attachment: α = 0.72) (Brennan et al., 1998).
Results
Participant characteristics
Participants had a mean age of 42.4 years (SD = 9.8), and the sample comprised 78.4% (n = 105) males from a variety of refugee backgrounds. Further sociodemographic characteristics of the sample in this study are shown in Table 1.
Predictors of attachment style
Two separate hierarchical linear regression (using the enter method) examined the relationship between attachment style (anxious and avoidant attachment, respectively) as the dependent variables and age, gender, relatlionship, duration of stay in Switzerland, visa status, potentially traumatic life events (interpersonal and non-interpersonal) as predictors. Specifically, demographics (age, gender and duration of stay in Switzerland) were entered at Step 1 because attachment styles have been shown to be related to both age (Davis et al., 2003) and gender (Bartholomew and Horowitz, 1991), and length of time in Switzerland may impact on capacity to form attachments in the host country. These variables were controlled for in the regression model prior to entering interpersonal trauma exposure and non-interpersonal trauma exposure at Step 2 to determine the additive effects of these different types of traumatic experience. Assumptions for regression analyses were checked in terms of linearity of the relationship between attachment and independent variables, autocorrelation of residuals (Durbin–Watson test = 2.014), homoscedasticity and normal distribution of residuals and were found to be satisfactory. In terms of the avoidant attachment tendencies, female gender and interpersonal trauma was a significant predictor, accounting for 11% of the variance. In terms of anxious attachment, there were no significant predictors (see Table 3).
Summary of hierarchical linear regression analyses of attachment style and trauma.
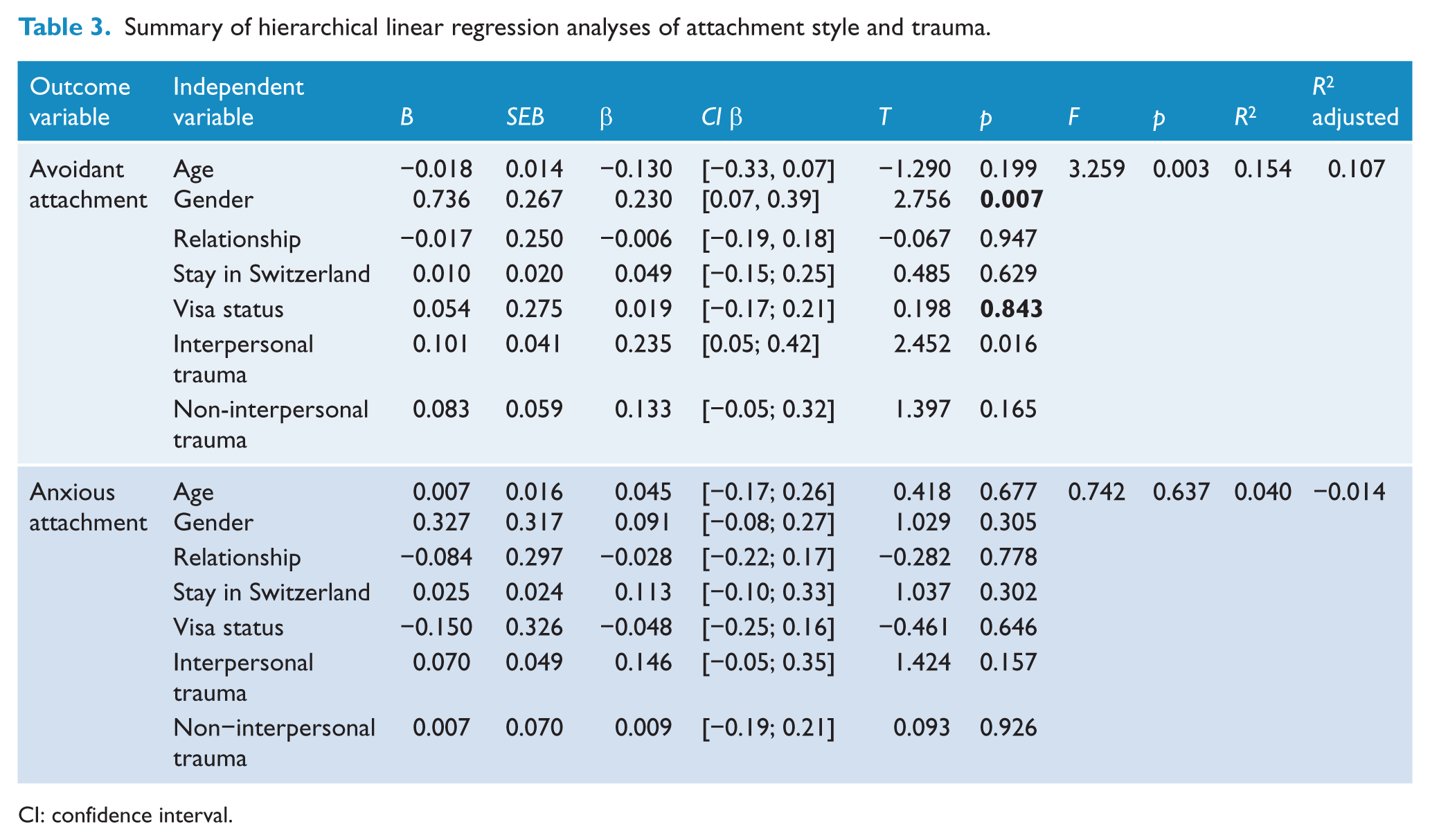
CI: confidence interval.
Discussion
The present study investigated the relationship of PTEs and attachment styles in a sample of treatment-seeking, severely traumatized refugees. The main outcome of this study was that avoidant attachment style was associated with interpersonal, but not non-interpersonal, trauma. Neither form of traumatic events was associated with anxious attachment style.
This pattern of findings is consistent with propositions of attachment theories that experiences of disturbed interpersonal relationships can damage one’s attachment system. Attachment theory posits that avoidant attachment tendencies can develop in the aftermath of seminal events in which one experiences disruptions in secure attachments (Mikulincer et al., 2005). It is possible that the extent to which refugees were exposed to interpersonal trauma, such as torture, eroded their capacity to trust others. Accordingly, they may have responded by distancing themselves from potential attachment figures. This possibility is consistent with evidence that distressed refugees may display disordered attachment and social withdrawal (Almqvist and Broberg, 2003; Schnyder et al., 2015). We did not index factors, such as trust or perceived malevolence of others, and so we can draw strong inferences on the mechanism underpinning this association. It has been noted that refugees can suffer disturbed attachments because of the separation from their primary supports (De Haene et al., 2010); however, it is worth noting that over three-quarters of our sample were currently living with their partner, suggesting that their primary source of support was available. This indicates that unavailability of supports was not an apparent explanation for respondents’ attachment styles in the current study.
The observed association in refugees of interpersonal trauma and avoidant attachment also converges with the notion of complex PTSD, proposed in the International Classification of Diseases, 11th Revision (ICD-11) (Maercker et al., 2013) to describe PTSD presentations that emerge after prolonged and typically interpersonal trauma; one of the characteristics of this presentation is disturbed capacity to relate to others, which may overlap to an extent with avoidant attachment tendencies. Proposals for complex PTSD explicitly recognise refugees as one group who can develop this interpersonal dysregulation as adults if exposed to sufficiently prolonged trauma (Bryant, 2010).
The cumulative effects of interpersonal trauma may result in avoidant attachment tendencies that involve deactivating the attachment system at times of threat or stress. It is apparent the refugees in the current sample experience marked posttraumatic stress, and so it is possible that the ongoing stress experienced in the aftermath of their refugee experiences prompt those exposed to marked interpersonal trauma to engage in avoidant attachment responses. Evidence points to avoidant attachment styles being associated with reduced activation of attachment representations during threat (Mikulincer et al., 2000), and minimization of social support seeking (Mikulincer et al., 2009). Moreover, where securely attached people who are primed with attachment figures show reduced noradrenergic increase following a stressor, this effect is not observed in those who are avoidantly attached (Bryant and Chan, 2015). These findings indicate that people with avoidant attachment styles are less capable of benefiting from the availability of attachment figures. This interpretation is also consistent with evidence that prisoners of war, who have typically experienced interpersonal trauma over a sustained period, do not benefit from the presence of attachment figures (Mikulincer et al., 2014). This scenario raises the possibility that refugees who have suffered considerable interpersonal trauma may be at risk of further psychological and social dysfunction because they are less likely to benefit from attachment figures. These possible interpretations remain speculative until experimental research is undertaken to determine the causal link between exposure to threat and attachment deactivation.
The finding that neither interpersonal nor other forms of trauma predicted anxious attachment tendencies is noteworthy. People with anxious attachment styles tend to be excessively vigilant for the availability of attachment figures, are sensitive to threats of abandonment, and behave in ways that seek reassurance about the attachment figure’s support (Mikulincer and Shaver, 2007). Recent work has observed adult separation anxiety in refugee populations (Silove et al., 2010; Tay et al., 2015), and there is also evidence that adult separation anxiety is linked to anxious attachment (Manicavasagar et al., 2009). In this context, it is somewhat surprising that the refugee experiences were not associated with anxious attachment. One possible explanation may be the nature of persecution experienced by refugees in this sample, which may lead to distrust and negative expectations of others (Nickerson et al., 2014b, 2015b), potentially culminating in avoidance of social interactions (Nickerson et al., 2014a). That is, interpersonal trauma may lead to traumatized refugees developing long-term avoidant attachment, rather than anxious attachment, tendencies. It is worth noting that this association with avoidant attachment converges to an extent with the notion of complex PTSD, proposed in ICD-11 (Maercker et al., 2013) to describe PTSD presentations that emerge after prolonged and typically interpersonal trauma; one of the characteristics of this presentation is disturbed capacity to relate to others, which may overlap to an extent with avoidant attachment tendencies.
We note that avoidant attachment style was predicted by female gender. We qualify this finding by noting the disproportionate males in the sample, which limits the generalizability of this finding. There is some evidence that males can display more dismissive attachment styles than females (Bartholomew and Horowitz, 1991), and that there are gender differences in how familial and other forms of conflict can impact on attachment style (Matsuoka et al., 2006). No previous work has studied gender differences in attachment style in the aftermath of severe interpersonal trauma, as reflected in refugee experiences. It is possible that the effects of interpersonal trauma impacted on females in the current sample in particular ways because the acts imposed on them may have transgressed fundamental social value systems of trust (e.g. rape or other forms of sexual abuse), and this may have contributed to avoidant attachment. At this point, these suggestions remain speculative until replication is done with larger and more representative samples of male and female refugees.
The current study had several limitations. First, we note that the construct of attachment, and our measure of attachment, has not been studied systematically in cross-cultural contexts, particularly across individualistic and collectivist societies. Accordingly, interpretation of the findings needs to consider the limited knowledge we have about attachment in different cultural settings; this limitation is underscored by the fact that our sample comprised participants from a range of cultural settings. Second, participants were all treatment-seeking individuals, and thus it is not possible to generalize these findings to the broader community of traumatized refugees. Third, many complex factors may contribute to refugees’ attachment patterns, including past and present attachments and fear for family back home, which could not be comprehensively measured in this study. Fourth, there was an overrepresentation of men (78%) in our sample, which precludes disentangling the effects of gender and interpersonal trauma. Fifth, assessments were conducted via a tablet-based survey battery, and it is possible this is not as sensitive as clinician-based interviews. Finally, this study implemented a cross-sectional design which precludes inferences about causality. Furthermore, childhood attachment was not taken into account. These limitations notwithstanding, this study presents new insights into the potential impact of interpersonal trauma on refugees’ capacities to engage in and benefit from attachment figures. Given the critical role of attachments as a source of emotion regulation at times of stress (Mikulincer et al., 2005), and the marked stressors experienced by refugees throughout their relocation and resettlement periods (Keller et al., 2003; Steel et al., 2006), this issue needs to be further explored with the goal of enhancing impaired attachment systems in affected refugees.
Conclusion
This study provides initial evidence that interpersonal trauma experienced by refugees adversely impacts their attachment style. Specifically, these forms of experiences are associated with more avoidant attachment tendencies. These findings shed light on a potential mechanism for the ongoing psychological difficulties of traumatized refugees. There is abundant evidence that refugees suffer elevated rates of psychological disorders (Heeren et al., 2012), especially after severe interpersonal trauma (Steel et al., 2006). Attachment theory posits that people can benefit psychologically from accessing attachment figures at times of stress; however, this potential is limited in people with avoidant attachment tendencies because they have learnt to not seek the help of others when threatened (Mikulincer et al., 2005). It is possible that refugees who are exposed to interpersonal trauma are more vulnerable to subsequent psychological disturbance because they are less able to access attachment figures, either realistically or symbolically, because of the lingering effects on their attachment system arising from the interpersonal trauma. This interpretation accords with a previous finding that prisoners of war were unable to benefit from attachment priming many years after their release (Mikulincer et al., 2014). This effect may also have detrimental effects on the capacity of refugees exposed to interpersonal trauma to settle into new countries because of their reluctance to engage with others. These initial findings indicate that the role of attachment style in refugees needs to be investigated more closely, and this line of inquiry may lead to more effective interventions for treating refugees who suffer emotional disorders following torture and other forms of interpersonal trauma.
Footnotes
Acknowledgements
N.M., U.S., M.S., A.N. and R.A.B. conceived and developed the study. N.M. and M.S. collected the data. All authors contributed to the data analysis, interpretation of the data and manuscript composition. R.A.B. and N.M. wrote the first draft of the manuscript. All authors have approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was supported by the Parrotia Foundation, the Swiss Federal Office for Migration (3a-12-0495), and the Swiss Federal Office for Health (12.005187). Angela Nickerson was supported by a National Health and Medical Research Council Clinical Early Career Fellowship (1037091).