
Abstract
Objective:
Caregivers of individuals with severe mental illness often experience significant negative experiences of care, which can be associated with higher levels of expressed emotion. Expressed emotion is potentially a modifiable target early in the course of illness, which might improve outcomes for caregivers and patients. However, expressed emotion and caregiver experiences in the early stages of disorders might be moderated by the type of severe mental illness. The aim was to determine whether experiences of the caregiver role and expressed emotion differ in caregivers of young people with first-episode psychosis versus young people with ‘first-presentation’ borderline personality disorder features.
Method:
Secondary analysis of baseline (pre-treatment) data from three clinical trials focused on improving caregiver outcomes for young people with first-episode psychosis and young people with borderline personality disorder features was conducted (ACTRN12616000968471, ACTRN12616000304437, ACTRN12618000616279). Caregivers completed self-report measures of experiences of the caregiver role and expressed emotion. Multivariate generalised linear models and moderation analyses were used to determine group differences.
Results:
Data were available for 265 caregivers. Higher levels of negative experiences and expressed emotion, and stronger correlations between negative experiences and expressed emotion domains, were found in caregivers of young people with borderline personality disorder than first-episode psychosis. Caregiver group (borderline personality disorder, first-episode psychosis) moderated the relationship between expressed emotion and caregiver experiences in the domains of need to provide backup and positive personal experiences.
Conclusion:
Caregivers of young people with borderline personality disorder experience higher levels of negative experiences related to their role and expressed emotion compared with caregivers of young people with first-episode psychosis. The mechanisms underpinning associations between caregiver experiences and expressed emotion differ between these two caregiver groups, indicating that different supports are needed. For borderline personality disorder caregivers, emotional over-involvement is associated with both negative and positive experiences, so a more detailed understanding of the nature of emotional over-involvement for each relationship is required to guide action.
Introduction
An unintended consequence of deinstitutionalisation and the shift to community care for many people with severe mental illness (SMI) was a transferral of greater care responsibility onto families (Morrison and Stomski, 2019). Informal caregivers are usually family members, but can be non-family members such as friends, who provide essential care supporting those with SMI to live independently within the community (Diminic et al., 2021). Unfortunately, this shift has not equated to increased caregiver support. Despite a growing evidence base of interventions that are effective in reducing caregiver burden (e.g. Martín-Carrasco et al., 2016; Perlick et al., 2018), there are many barriers encountered with respect to implementation into standard care (Eassom et al., 2014). As a consequence of their care role, caregivers encounter multiple challenges including increased burden (Hayes et al., 2015; Ribé et al., 2018); psychological distress, anxiety and depression (Hayes et al., 2015; Jansen et al., 2015; Scheirs and Bok, 2007; Seigerman et al., 2020); poorer physical health (Poon et al., 2018; Thunyadee et al., 2015), including changes to endocrine and immune systems (Lovell and Wetherell, 2011), greater social exclusion (Filia et al., 2019; Hayes et al., 2015; Ribé et al., 2018), poorer quality of life (QoL) (Caqueo-Urízar et al., 2017; Stanley et al., 2017) and can be at greater risk of violence initiated by their loved one (Onwumere et al., 2018).
Caregiver burden refers to a range of difficulties experienced by families caring for a family member with SMI (Kuipers et al., 2010). However, the notion of burden has proven to be elusive, and some have argued that appraisal of caregiving experiences is a better outcome measure (Szmukler et al., 1996, 2003). High expressed emotion (EE) represents an adverse family environment and communication style between the caregiver and the patient with SMI (Butzlaff and Hooley, 1998). EE from caregiver includes critical comments (CC), emotional over-involvement (EOI) and hostility (Vaughn and Leff, 1976).
High EE has been associated with caregiver burden and negative experiences (Zanetti et al., 2018) and worse outcomes for patients (e.g. relapse; Bailey and Grenyer, 2015; Butzlaff and Hooley, 1998) with schizophrenia (Scazufca and Kuipers, 1999; Vaughn and Leff, 1976), and mood and eating disorders (Butzlaff and Hooley, 1998). Conversely, high EE, particularly EOI, has been associated with better outcomes in individuals with borderline personality disorder (BPD) (e.g. Hooley and Hoffman, 1999). EE, if addressed, can improve outcomes for the caregiver (e.g. burden and distress; Scazufca and Kuipers, 1999) and the patient (e.g. psychotic relapse; Butzlaff and Hooley, 1998). Different EE domains may be differentially associated with burden (Alvarez-Jimenez et al., 2010).
It has been argued that high EE might be associated more with caregivers’ psychological appraisal of the situation, rather than patient illness factors (Hinojosa-Marqués et al., 2020). If this is the case, then one would expect that the relationship between high EE and caregivers’ appraisal would not differ according to the patients’ diagnosis. However, as highlighted earlier, high EOI can have both positive and negative impacts on caregivers and patients. However, there have been no studies which have directly examined the impact of diagnosis on EE and caregivers’ appraisal.
To design appropriate supports for caregivers, it is important to understand whether different types of SMI lead to differential experiences and outcomes for caregivers. Here, we examine caregivers’ experiences and EE in first-episode psychosis (FEP) and BPD in young people; both SMI types typically emerge in adolescence and young adulthood (Chanen et al., 2017; Kessler et al., 2007) and both disorders have been noted to have significant consequences for caregivers (Betts et al., 2018; Cotton et al., 2013; Gleeson et al., 2020; Seigerman et al., 2020). In cohorts of people with enduring SMI, however, caregivers of individuals with BPD have been reported to experience greater levels of objective and subjective burden, poorer well-being and more grief than caregivers of individuals with other SMI such as schizophrenia (Bailey and Grenyer, 2013). We do not know whether this is true for caregivers of young people who have been newly diagnosed with FEP or BPD.
Our first aim was to determine differences in the degree of negative appraisals of the caregiving role and manifestation of EE among caregivers of young people who have experienced a FEP, compared with caregivers of young people with BPD features. Our second aim was to establish whether the SMI type moderates the associations between the burden and EE domains.
Methods
Design
Baseline data were collated from three clinical trials. The first trial comprised caregivers of young people who had experienced a FEP (Altitudes; ACTRN12616000968471; Gleeson et al., 2017). Altitudes was an cluster randomised controlled trial of a purpose-built online application which involved social networking, expert and peer moderation, and evidence-based psychoeducation (Gleeson et al., 2017). There were two trials for families/caregivers of young people with BPD. Making Sense of Borderline Personality Disorder (MS-BPD, ACTRN12616000304437; Betts et al., 2018) was a randomised controlled trial of an online psychoeducation programme versus and a combined online and face-to-face psychoeducation programme. Kindred was a trial of an online intervention similar to Altitudes, but designed and adapted for caregivers of young people with BPD (ACTRN12618000616279; Gleeson et al., 2020).
Sample and setting
Caregivers (family or friends) of young people (aged 15–25 years, inclusive) were recruited through two Specialist Programs at Orygen, a specialist mental health service for young people residing in the northwest and west of metropolitan Melbourne, Australia. Young people with FEP (Altitudes) were receiving treatment through the Early Psychosis Prevention and Intervention Centre (EPPIC) between October 2015 and July 2018. Young people with features of BPD (⩾3 BPD; Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5) were receiving treatment in the Helping Young People Early (HYPE) programme. In MS-BPD, recruitment occurred between March 2016 and November 2017 and Kindred between June and September 2018. In all three studies, an exclusion criterion was inability to read or converse in English.
Measures
Caregivers’ experiences
The Experience of Caregiving Inventory (ECI; Szmukler et al., 1996) is a self-report measure of caregivers’ perceptions or appraisal of burden associated with their role over the past month. It comprises 66 items and 10 subscales indexing positive (e.g. ‘I have become more confident in dealing with others’) and negative aspects (e.g. ‘being unable to do things that you want to’) of the caregiving experience. Each item is rated on a 4-point scale (0 = never to 4 = nearly always). Subscales include Difficult Behaviours, Negative Symptoms, Stigma, Problems with Services, Effects on the Family, Loss, Dependency, Need to Back-Up, Positive Personal Experience, and Good Aspects of the Relationship with Patient. Higher scores on negative subscales and lower scores on positive subscales indicate negative appraisal. In our study, Cronbach’s α for the ECI subscales ranged from 0.70 (Need to Back-Up) to 0.90 (Negative Symptoms).
Expressed emotion
EE was measured using the 20-item self-report Family Questionnaire (FQ; Wiedemann et al., 2002). Each item is measured on a 1 ‘never/very rarely’ to 4 ‘very often’ scale, with two 10-item subscales, CC and EOI. The EOI subscale includes items such as ‘I often think about what is to become of him or her’ and the CC subscale includes items such as, ‘he or she does some things out of spite’. Scores range from 10 to 40 with higher scores reflecting higher EE. The FQ has good internal consistency (Cronbach’s alpha > 0.78 for EOI and > 0.90 for CC; Wiedemann et al., 2002). Importantly, it has been shown to have good construct validity against the gold standard semi-structured interviewer-based measure of EE, known as Camberwell Family Interview (Wiedemann et al., 2002). In our study, across all caregivers, Cronbach’s α for the EOI was 0.85 and 0.90 for CC.
Demographic information
Caregiver demographic data were harmonised across the three studies and included sex, age, relationship with the young person, and educational and vocation backgrounds.
Procedure
Ethical approval was obtained from Melbourne Health Research and Ethics Committee (Altitudes No. 2014.175; MS-BPD No. 2014.105, Kindred No. 2017.132). Procedures for recruitment were comparable across studies; researchers and clinicians approached caregivers attending Orygen and obtained written informed consent. Caregivers completed the self-report questionnaires prior to participating in the interventions. Only caregivers who consented to have their data used in future studies were included in this study.
Data analysis
Descriptive statistics were used to characterise the two caregiver groups. Independent samples t-tests and chi-square (χ2) analyses were conducted to determine group differences. Significant chi-square tests were followed by comparison of proportions across columns with Bonferroni-adjusted p-values. To determine group differences on the negative ECI subscales, we used multivariate general linear models (GLMs) with caregiver group (referred to as GROUP) as the factor and the eight negative ECI subscales as dependent variables. A similar approach was used for the two ECI positive experiences subscales and the two FQ subscales. Partial eta squared (η2) effect sizes were interpreted as 0.01 small, 0.06 medium and 0.14 large (Cohen, 1988).
Pearson’s correlations (r) were calculated to determine the relationships between EE and burden domains within the two caregiver groups. Regression analyses were conducted to elucidate how CC and/or EOI related to the different domains of burden within each disorder group. From these regression models, parameters reported include R2adj, F statistic associated with overall model fit, standardised β for EE domains and associated p values.
To explore whether diagnosis moderated the interrelationships between caregivers’ experiences and EE, we conducted simple moderation analyses with PROCESS 3.5 (Hayes, 2013). For these models, x was the EE variable, y was the experience domain and w was the caregiver group.
Results
In the original studies, there were 265 caregivers; however, there were 35 (Altitudes, n = 34; Kindred = 1) who did not consent to have their data used for other purposes and were excluded. Therefore, this study comprised a total of 230 caregivers; 130 caregivers of young people with FEP and 100 caregivers of young people with BPD features (MS-BPD n = 82, BPD criteria M = 4.7 [SD = 1.1]; Kindred n = 18, BPD criteria M = 4.4 [SD = 1.3]) (see Table 1). Caregivers of young people with BPD features compared to the FEP group were significantly younger (p = 0.002), less likely to be a parent (p = 0.001) and were more likely to have only completed secondary education as their highest level of educational attainment (p < 0.001).
Demographic characteristics for the total cohort as well as separately for caregivers of young people with FEP and BPD.
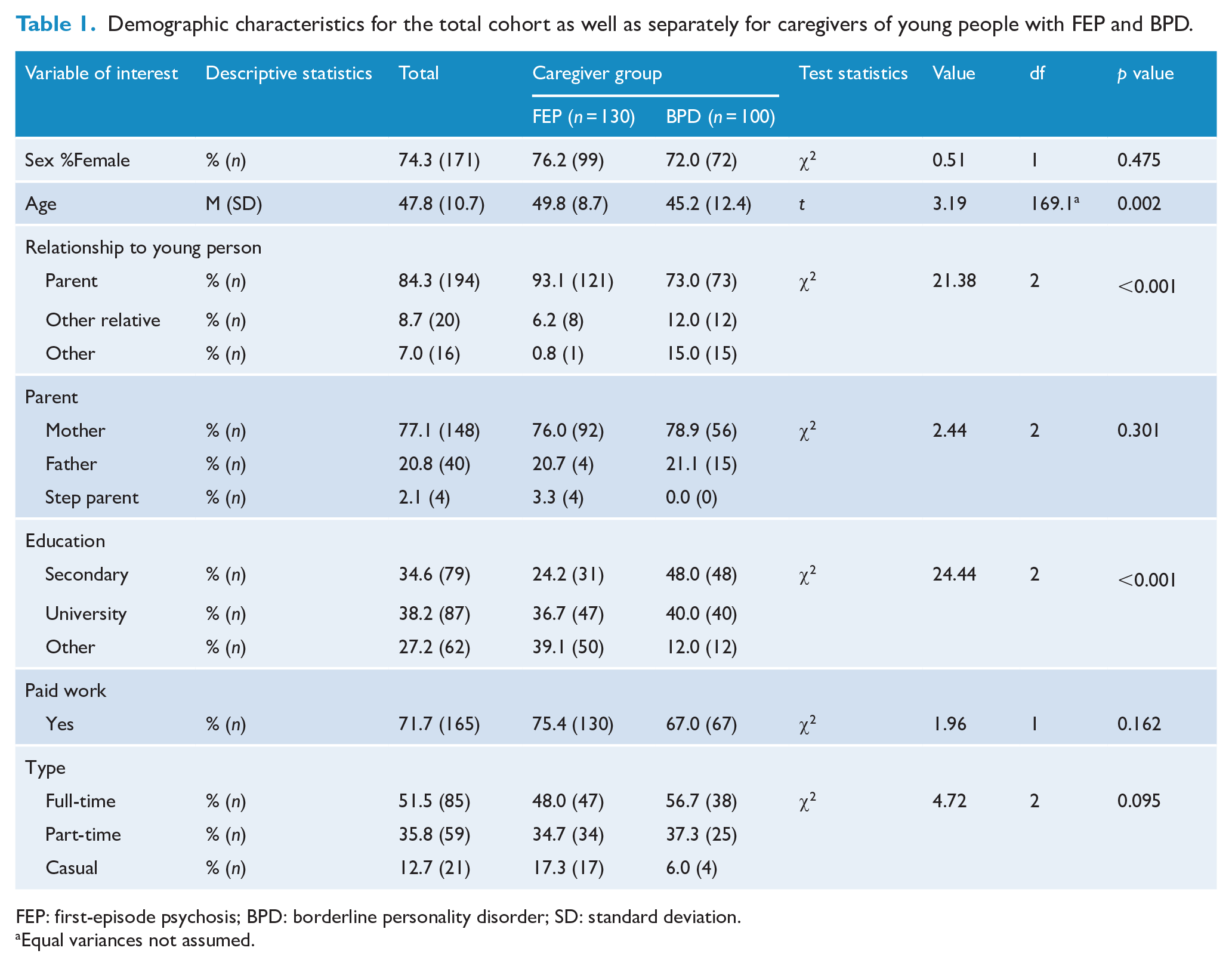
FEP: first-episode psychosis; BPD: borderline personality disorder; SD: standard deviation.
Equal variances not assumed.
The FEP caregivers were caring for young people with a range of psychotic disorders including schizophrenia (21.5%, n = 28), schizophreniform (22.3%, n = 29), affective psychoses (major depressive disorder [MDD] with psychotic symptoms, 13.8%, n = 18; bipolar disorder, 6.2%, n = 8; schizoaffective disorder, 5.4%, n = 7), substance-induced psychosis (10.8%, n = 14), psychosis not otherwise specified (16.9%, n = 22) and other psychoses (3.1%, n = 4).
Caregiver experiences
Multivariate GLMs were planned to separately examine positive and negative aspects of caring for a young person with SMI. For these models, we controlled for caregivers’ age (AGE), so adjusted mean for GROUPs are provided. We also wanted to control for caregivers’ relationship with young person (RELATION) and caregivers’ education (EDUCATION) in the models. Because of small cell sizes, RELATION was dichotomised to parent (yes/no, including step parent) and EDUCATION to secondary as highest level (yes/no). However, despite this recoding, the cell sizes for RELATION (other relationship n = 9 in FEP group) were still too small for meaningful comparison. When we included EDUCATION in the models, as well as the interaction term between GROUP and EDUCATION, none of these parameters were significant. Therefore, we limited our multivariate GLMS with GROUP as the independent variable and AGE as a covariate. Adjusted means (± SE) for the eight negative subscales and two positive subscales of the ECI are presented in Table 2.
Estimated means (± standard errors) and univariate effects from multivariate GLMs with caregiver group and caregivers’ relationship with young person, and the interaction between group and relationship as factors, and age as a covariate.
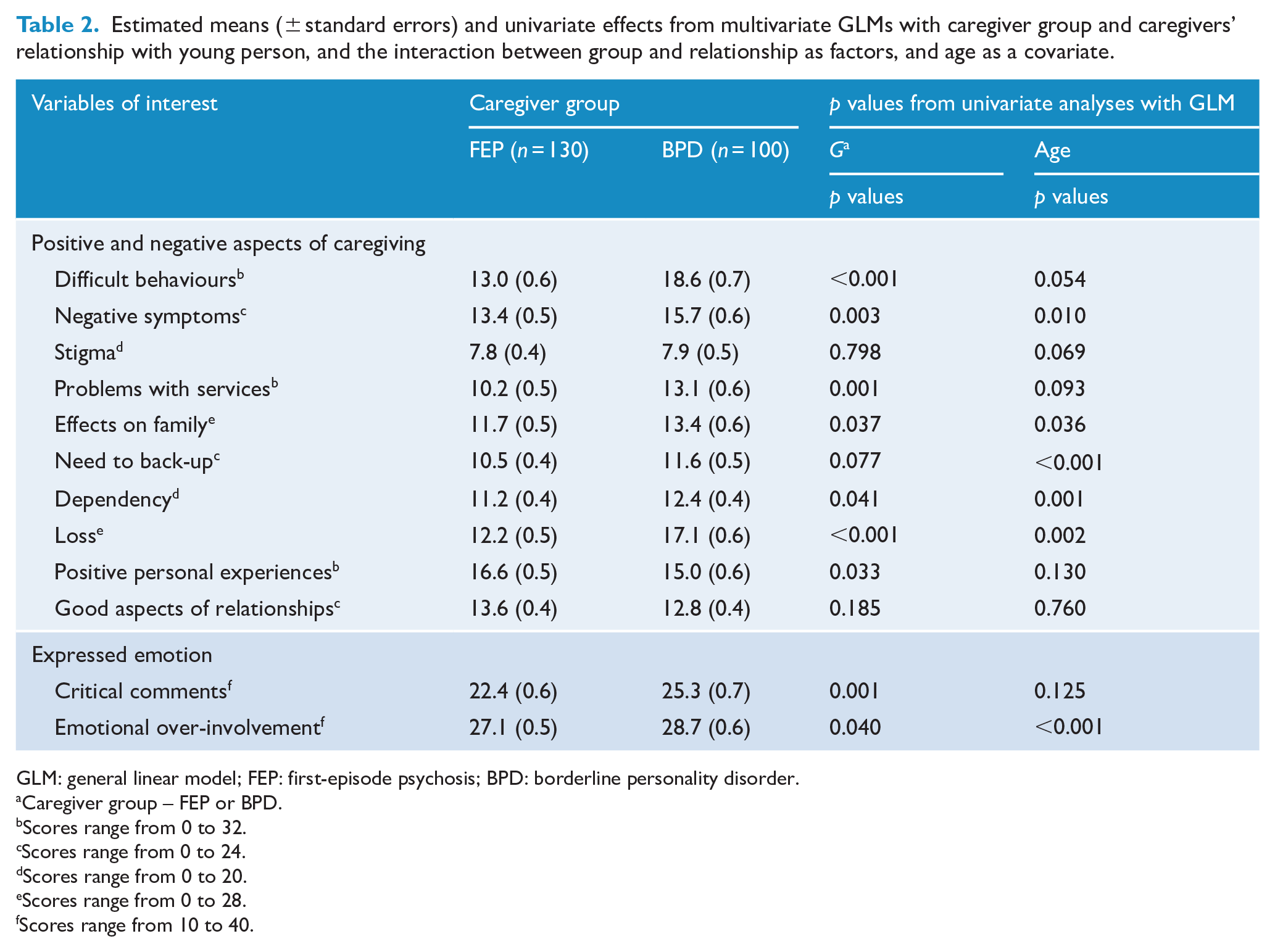
GLM: general linear model; FEP: first-episode psychosis; BPD: borderline personality disorder.
Caregiver group – FEP or BPD.
Scores range from 0 to 32.
Scores range from 0 to 24.
Scores range from 0 to 20.
Scores range from 0 to 28.
Scores range from 10 to 40.
For the linear combination of eight negative burden subscales of the ECI, there was a significant difference between the two GROUPS, F(8, 219) = 8.87, p < 0.001, η2 = 0.25 after controlling for AGE, F(8, 219) = 2.78, p < 0.006, η2 = 0.09. Univariate tests indicated that the BPD caregivers were significantly more likely than FEP caregivers to perceive more burden due to Difficult Behaviours, F(1, 226) = 35.12, p < 0.001, η2 = 0.14, Negative Symptoms F(1, 226) = 9.30, p = 0.003, η2 = 0.04, Problems with Services, F(1, 226) = 12.04, p = 0.001, η2 = 0.05, Effects on Family, F(1, 226) = 4.38, p = 0.037, η2 = 0.02, Dependency, F(1, 226) = 4.22, p = 0.041, η2 = 0.02, and Loss, F(1, 226) = 39.53, p < 0.001, η2 = 0.15. Age was related to burden due to Negative Symptoms, F(1, 226) = 6.80, p = 0.010, η2 = 0.03, Effects on Family, F(1, 226) = 4.45, p = 0.036, η2 = 0.02, Need to Provide Back-Up, F(1, 226) = 18.06, p < 0.001, η2 = 0.07, Dependency, F(1, 226) = 11.17, p = 0.001, η2 = 0.05, and Loss F(1, 226) = 9.78, p = 0.002, η2 = 0.04. Significant positive relationships were found with AGE and Need to Provide Back-Up, r = 0.25, p < 0.001 and AGE and Dependency, r = 0.19, p = 0.003, but not the other burden domains.
For the linear combination of the two positive ECI subscales, the GROUP main effect, F(1, 225) = 2.31, p = 0.101, η2 = 0.02, and covariate AGE, F(1, 225) = 1.34, p = 0.263, η2 = 0.01, were not significant. With respect to the univariate analyses, the Positive Personal Experiences were significantly lower in the BPD caregivers than in the FEP caregivers, F(1, 226) = 4.61, p = 0.033, η2 = 0.02.
Expressed emotion
Multivariate effects for the linear combination of the two subscales of the FQ indicated that there was a significant effect for GROUP, F(2, 224) = 5.26, p = 0.006, η2 = 0.05, and AGE, F(2, 224) = 7.28, p = 0.001, η2 = 0.06. Examination of univariate effects indicated that there were significant differences between GROUPS on both CC, F(1, 225) = 10.52, p = 0.001, η2 = 0.05, and EOI, F(1, 225) = 4.25, p = 0.040, η2 = 0.02, with the BPD caregivers having significantly higher EE on both subscales. Age was related only to EOI, F(1, 225) = 13.96, ps < 0.001, η2 = 0.06.
Relationship among caregiver burden and EE
For the FEP caregivers, correlations between EE and burden domains ranged from 0.08 (Positive Personal Experiences with EOI) to 0.70 (Difficult Behaviours with CC and Loss with EOI) (see Table 3). For the BPD caregivers, they ranged from 0.06 (Good Aspects of Relationships with EOI) to 0.77 (Dependency and EOI).
The univariate and multivariate relationships between CC, EOI and positive and negative aspects of caregiving across the two caregiver groups.
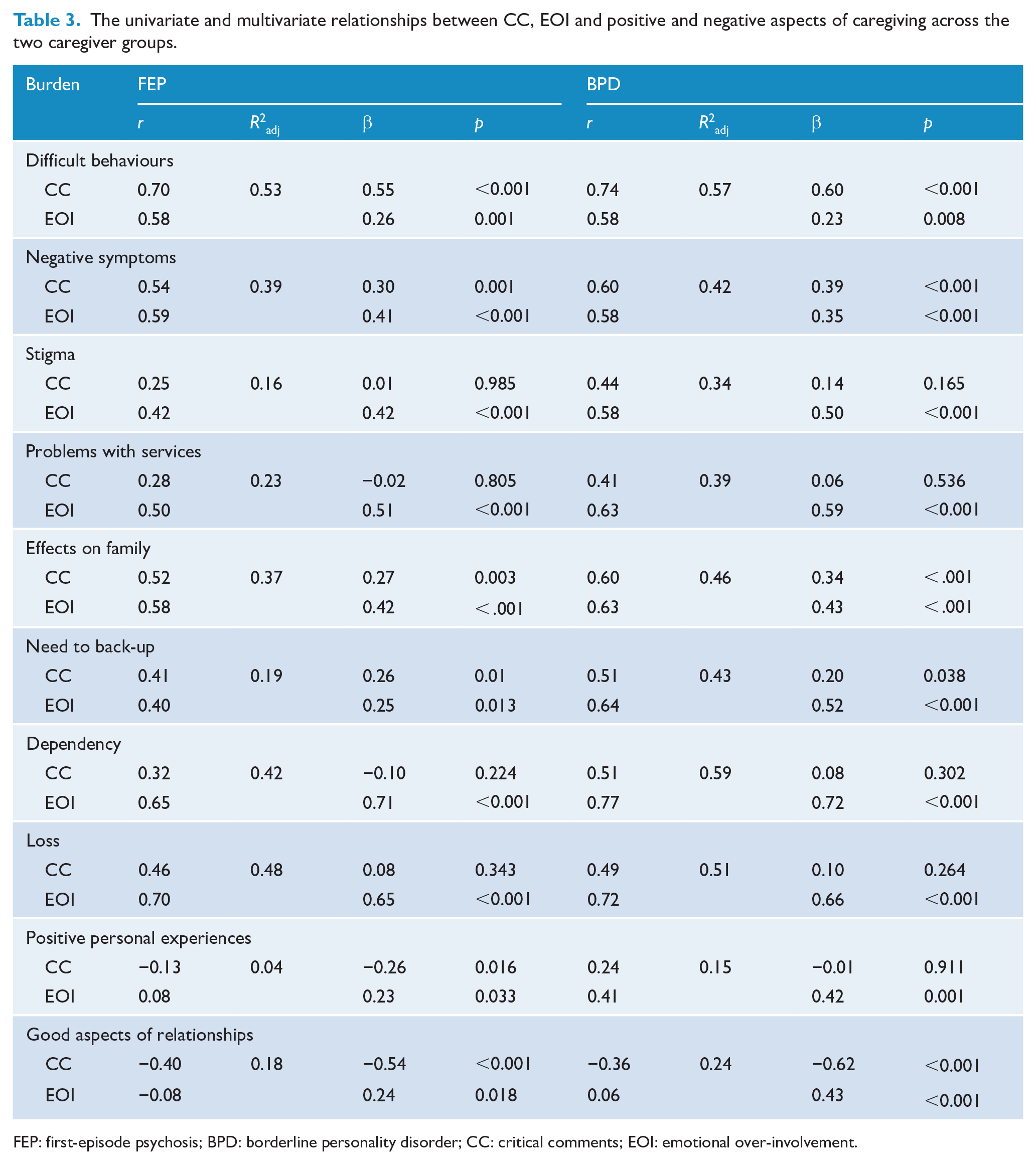
FEP: first-episode psychosis; BPD: borderline personality disorder; CC: critical comments; EOI: emotional over-involvement.
Regression analyses indicated that EOI was significantly associated with each experience domain within each group (see Table 3). In both groups, CC was associated with Difficult Behaviours, Negative Symptoms, Effects on Family, Need to Back-Up, and Good Aspects of Relationships (negative association). There were no significant associations between CC and Stigma, Problems with Services, Dependency and Loss. For the FEP caregivers, CC was significantly associated with Positive Personal Experiences, but this was not found in BPD caregivers. The amount of variability explained in burden domains was substantial (up to 59% in the BPD caregivers for Dependency) and more variability in burden was explained in the BPD caregivers. GROUP was found to moderate the association between Positive Personal Experiences and both CC and EOI.
Table 4 and Figure 1 display results for moderation analyses. Figure 1(a) depicts the nature of interaction between Positive Personal Experiences and CC; a negative association was found for the FEP caregiver group whereas a significant positive relationship was observed in the BPD caregiver group (see Figure 1(a)). For EOI, the association with Positive Personal Experiences was much greater in the BPD caregivers than in the FEP caregivers (Figure 1(b)). For Need to Provide Back-Up (Figure 1(c)), the correlations with EOI were significantly stronger in the BPD caregivers than in FEP caregivers.
Models depicting how caregiver group moderates the relationships between expressed emotion and caregiver experiences.
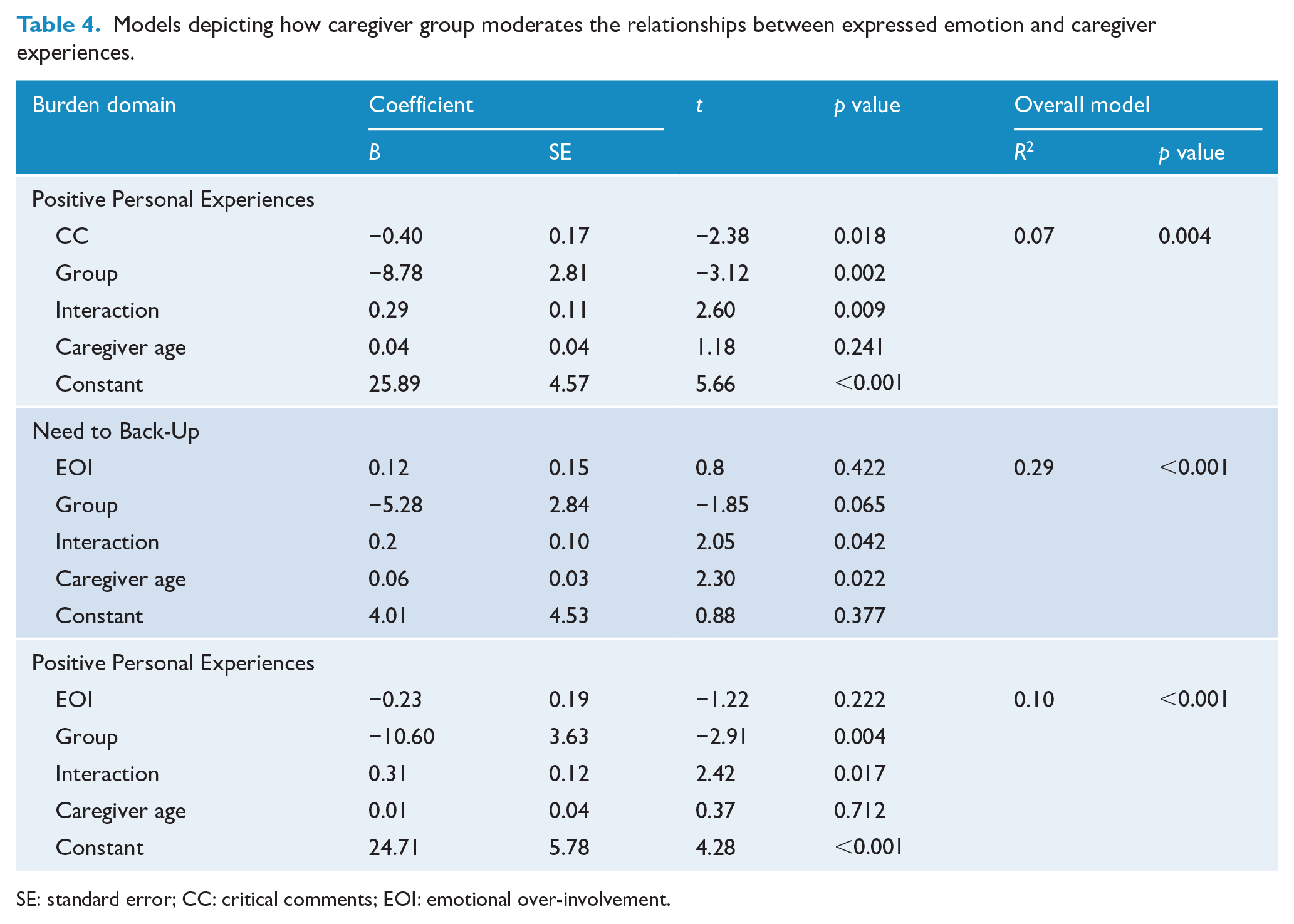
SE: standard error; CC: critical comments; EOI: emotional over-involvement.
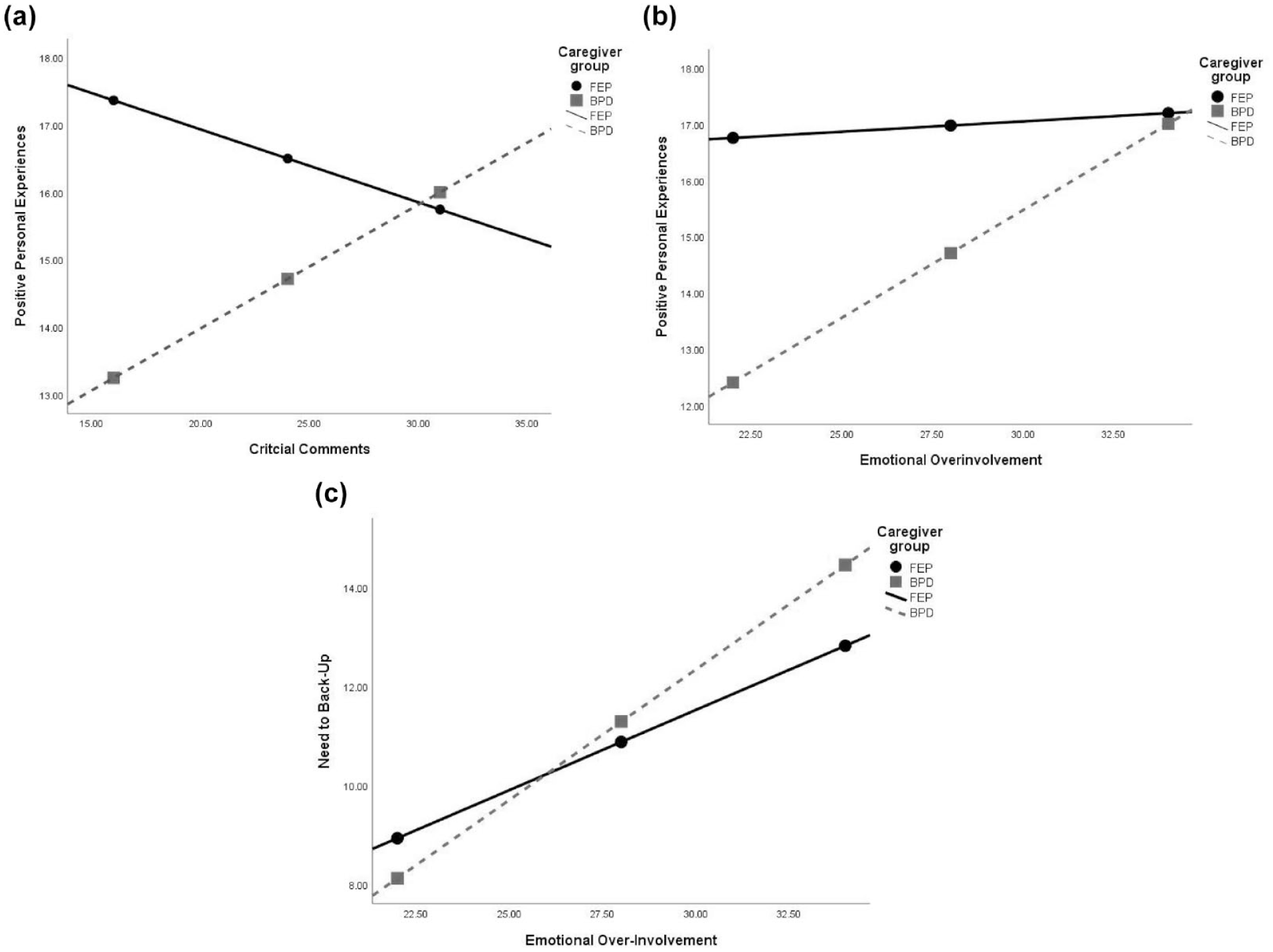
Regression estimates depicting the moderation of caregiver group on the relationship between EE and caregiver experiences: (a) CC and Positive Personal Experiences, (b) EOI and Positive Personal Experiences and (c) EOI and Need to Provide Back-Up.
Discussion
This is the first study to compare the burden and EE in caregivers of young people with FEP and BPD features, with data collected contemporaneously over a 3-year period from an early intervention service. Importantly, we highlight that caregivers’ experiences might differ among different patient diagnostic groups and that targeted treatments might be required to accommodate these differences.
Key findings
Four key findings are noted. First, caregivers of young people with BPD reported much greater levels of negative and fewer positive experiences than caregivers of young people with FEP. Second, some experience domains did not differ between groups, including burden due to stigma, need to provide support and good aspects of relationships. Third, EE was significantly higher among caregivers of those with BPD. Fourth, EE was strongly associated with caregivers’ experiences with caregiver group moderating both the strength and/or direction of some of these associations.
Caregivers’ experiences
We undertook a fine-grained analysis of caregivers’ appraisals of their caregiving experiences, including capturing positive aspects of caregiving (often overlooked). We found striking differences, with more negative appraisal experienced by BPD than FEP caregivers with respect to problematic behaviours (e.g. moodiness, irritability), negative symptoms (e.g. apathy, anhedonia), problems with services (e.g. how mental health professionals do not take you seriously), effects on family relationships, dependency (e.g. limitations to participation because of caregiver role) and loss (e.g. what sort of life he or she may have). These findings are consistent with past research indicating caregivers of those with BPD experience more burden than caregivers of individuals with chronic schizophrenia (Kirtley et al., 2019), anorexia nervosa and FEP (Seigerman et al., 2020). Although differences in disorder onset and symptomatology may explain some of these findings, it is likely that mechanisms are complex and not only due to these factors.
Although FEP and BPD can both first appear in adolescence, the nature of their developments may differentially impact caregivers’ perceptions and subsequent burden. Young people with FEP might have a period of adaptive development, prior to their acute illness onset, leading to the establishment of more adaptive self-management and stronger familial relationships. Initial treatment usually involves medication, and psychoeducation focuses on FEP as an ‘illness’, which might mean caregivers view the challenges differently and therefore feel less burdened. Persistent caregiver burden in those with psychosis is associated with younger age of individuals with psychosis, financial burden, increased duration of untreated illness, presence of disability (e.g. in self-care, unemployment), and poor insight, paranoia, delusions, hostility and aggression (Kamil and Velligan, 2019).
Alternatively, young people with BPD generally have had a history of enduring relational problems (often with caregivers/parents) and maladaptive behaviours (e.g. self-harm, impulsive behaviour, emotional dysregulation) leading to adaptive failure during the transition from childhood to adulthood. Caregivers, and especially parents, are likely to have been struggling for longer and experience more burden. With psychoeducation and guidelines recommending psychosocial interventions rather than medication, caregivers might view BPD as a condition the young person has some control over and less as an ‘illness’. This would accord with the way that clinicians view BPD. Given the intensity and volatility of the relationships with family members, over time, caregivers may be less equipped to respond to the challenges of their role (Hoffman et al., 2005); this may account for why there were fewer parents in the BPD group.
Grief was significantly higher in the BPD than in FEP caregivers, commensurate with comparisons in adults with these disorders (Struening et al., 1995). Two types of grief have been identified in caregivers of adults with BPD: (1) perceived loss of future potential and (2) worry about who will provide long-term care for the patient when the caregiver can no longer perform that role (Ekdahl et al., 2011). BPD caregivers’ worry about the young person’s future may be driven by the higher suicide risk associated with the disorder (suicide risk estimate = 45.1, 95% confidence interval [CI] = [29.0, 61.3]), which is much higher than suicide risk estimates for schizophrenia (12.9, 95% CI = [0.7, 174.3]) (Chesney et al., 2014).
The grief experienced by caregivers of individuals with BPD should be alleviated by effective engagement with services (Bailey and Grenyer, 2013). However, caregivers of individuals with BPD often experience reduced empowerment as a consequence of their interactions with mental health services, including inconsistent or conflicting guidance, limited provision of appropriate information, general lack of understanding of their situation, stigma, blame, and exclusion from treatment and discharge planning (Bailey and Grenyer, 2013; Hoffman et al., 2005). Furthermore, two of the key failures in the prevention and early intervention field have included a failure of identification (i.e. non-diagnosis or delayed diagnosis) and a failure of access (e.g. infrequent referral to specialist services, limited services leading to waiting lists for care) for young people with personality disorder (Chanen and Nicol, 2021). Consistent with this, in our study, the caregivers of young people with BPD reported greater difficulties engaging services; however, both caregiver groups had comparable burden with respect to stigma, and needing to provide back-up to the young person. It is unclear as to which services that the caregivers of young people with BPD are rating. Delayed treatment and difficulty getting help from services commonly occurs (Chanen et al., 2016); it might have occurred before receiving treatment at Orygen; however, further research would be required to determine whether this is the case. At Orygen, extensive support is provided to the young people and their family (Betts et al., 2018; McGorry et al., 1996). Both programmes see families and caregivers as invaluable contributors to the recovery of the young person. Families have access to family peer support and psychoeducation, as well as family interventions, if required. This model of care might lead to families experiencing less stigma. It would be of interest to compare burden in these areas with caregivers’ experiences in other service settings.
Expressed emotion
High levels of EE have been associated with poor outcomes for both caregivers and individuals with psychosis (Alvarez-Jimenez et al., 2010; Butzlaff and Hooley, 1998) and BPD (Bailey and Grenyer, 2015; Hooley and Hoffman, 1999). However, we found that levels of both CC and EOI were substantially greater among BPD than FEP caregivers. Intense negative interpersonal feedback processes, such as CC, can be particularly problematic in families with a young person with BPD (Whalen et al., 2015).
Association between caregiver experience and EE
There were differences in how CC and EOI related to the burden domains, and these associations were moderated by the young person’s diagnosis. EOI was related (including both positive and negative associations) with almost every aspect of burden, whereas, in some instances, CC was unrelated to burden, including in the domains of stigma, problems with services, dependency and positive personal experiences (only in the BPD caregivers). These differences might be due to different mechanisms underpinning CC and EOI, with CC conceptualised as a coping strategy and EOI being considered an anxious attachment style (Alvarez-Jimenez et al., 2010). However, as we did not include measures of coping and attachment style in this study, further research is needed.
The amount of variability explained by EE in some burden domains was substantial. In FEP caregivers, 53% of the variability in difficult behaviours was explained by EE. Across most burden domains, EE explained more variability in burden among BPD caregivers. For burden due to dependency, 59% of the variability was explained by EE (only EOI was significant) in BPD caregivers and only 42% was explained in FEP caregivers. EE contributes strongly to caregivers’ sense of burden, perceived risk, and sense of helplessness, findings consistent with previous research especially in caregivers of patients with BPD (Bailey and Grenyer, 2015).
Positive personal experiences were differentially related to EE in the two caregiver groups. CC was associated with less positive personal experiences for the FEP caregiver, consistent with previous research (Koutra et al., 2015; Zanetti et al., 2018). EOI, however, was unrelated to positive personal experiences in the FEP group, which is inconsistent with other studies (Alvarez-Jimenez et al., 2010).Others have found that in FEP caregivers, EOI is only related to negative caregiver experiences whereas other factors such as greater meta cognition (e.g. understanding emotional reactions in self and others) drive more positive experiences of the caregiving role (Jansen et al., 2014).
A different pattern of relationships was found for BPD caregivers with both CC and EOI being positively associated with affirmative personal experiences. It is possible that anxious over-concern, conflict and emotional closeness might be experienced by caregivers of people with BPD as both burdensome and an opportunity for positive personal experiences with their young person. Conflict might be seen as an intrinsic feature of having a family member with BPD. However, anxious over-concern might reflect caregivers’ attempts at an adaptive response to the challenges of such conflict. Conflict and emotional closeness are not orthogonal and might also reflect two sides of the same coin with regard to be idealised and then devalued relationship pattern that is characteristic of BPD.
Elevated EOI has been associated with better outcomes for people with BPD, possibly as this is perceived as validating by the patient (Hooley and Hoffman, 1999), which may in turn reinforce the heightened involvement of the caregiver and provide the caregiver with a more positive experience of the caring role. However, elevated EOI and CC are also associated with burden (especially with dependency and need to provide back-up) and poor mental health outcomes in BPD caregivers (Bailey and Grenyer, 2015), suggesting caregivers might be at risk of burnout. What these results highlight is that the mechanisms underpinning the relationships between EE and caregiver outcomes are complex, multifaceted and can have both positive and negative impacts that are different for caregivers of young people with BPD versus FEP.
Limitations
There were a number of limitations to the study. First, the generalisability of the cohorts might be limited to those who consented to participate in clinical trials and who could read and converse in English. It is also unclear as to whether there were differences between the caregiver groups who did and did not consent for the trial as well as consent for their data to be used in future studies. Thus, there is the need for future research to validate the generalisability of our findings. Second, there were differences between the caregiver groups with respect to caregivers’ age, education and relationships to the young person, and we were unable to consider all combinations of these factors due to small cell sizes. However, after controlling for these variables, diagnosis explained differences in both the intensity and relationships between burden and EE domains. A third limitation was that we were unable to consolidate information across the three studies on key constructs such as caregivers’ distress, mental ill-health and coping skills; the interplay between these constructs and caregiver burden and EE could be examined in future studies. Fourth, although we had information on young people’s diagnosis, we did not have details on other patient characteristics (e.g. length of disorder, comorbidities, functioning) as they were not recruited to these studies. We could also not determine the interrelationships between parental EE and burden and the young person’s outcomes. Fifth, further work is needed to determine the suitability of the ECI and FQ in caregivers of those with BPD; these scales were largely developed for caregivers of those with chronic schizophrenia. Finally, the absence of longitudinal data makes it difficult to delineate the extent of variations in both caregiver and young persons’ outcomes as well as changes in the interrelationships between constructs.
Clinical implications and future directions
In most clinical guidelines, the importance of incorporating families in the care of individuals with psychiatric diagnoses has been highlighted (Early Psychosis Guidelines Writing Group and EPPIC National Support Program, 2016; National Health and Medical Research Council, 2012). Accordingly, there are a growing number of interventional studies aiming to provide support for caregivers of young people with FEP, but fewer for young people with BPD. We are trying to address these issues by building an evidence base for novel interventions for caregivers for FEP (Gleeson et al., 2010, 2017; McCann et al., 2013) and BPD (Betts et al., 2018; Gleeson et al., 2020; Pearce et al., 2017; Seigerman et al., 2020), but more work is needed. As we have demonstrated, caregivers in both groups experience burden across various domains, with differential relationships of these domains with EE.
Several therapeutic strategies might be needed to support caregivers. First, delivery of the intervention must be flexible to address fluctuations in EOI and CC (Alvarez-Jimenez et al., 2010). If changes in EE are not addressed appropriately, there might be adverse clinical outcomes (Alvarez-Jimenez et al., 2010). Second, for caregivers of young people with FEP, there needs to be a focus on facilitating adaptive communication styles, reducing both CC and EOI and the application of adaptive coping strategies (Alvarez-Jimenez et al., 2010). For caregivers of young people with BPD, psychoeducation regarding the disorder might support caregivers to be more able to understand and manage their responses to high-risk behaviours, such as self-harm. However, there is a need to improve the quality of psychoeducation, as evidence suggests that too much knowledge can result in caregivers feeling more burdened and exhibiting high levels of EE (Hoffman et al., 2003). There is also a need to support caregivers of those with BPD to understand the nature and function of EOI in their relationship with their loved one. For example, overprotection, anxious concern and emotional closeness might be considered validating and helpful for patient recovery (Hooley and Hoffman, 1999), but can also be associated with negative caregiving experiences (Bailey and Grenyer, 2015), such as feeling burden associated with needing to provide backup for the young person.
More research, however, is needed to delineate the core components of interventions for these two groups. What is generally missing is the knowledge of other factors that might drive these associations, such as patient characteristics, caregiver personality, attributions and coping styles. We also do not have a good understanding of the psychosocial and physical consequences of caring on caregivers. We need to understand the mechanisms underpinning negative caregiver experiences and distress in order to be effective in bringing about change, specifically to inform what type of interventions to offer (i.e. psychoeducational, peer support, psychotherapy), how to best deliver an intervention (in-person, online, individual, group format) and when is the optimal time to provide such support (in terms of stage of illness and stage of treatment). Are different interventions needed for family members compared to other caregivers? We may need to go beyond moderation (and mediation) models to examine complex interpersonal interactions in real time (Hofmann et al., 2020). We also need to better understand how the caregiver and patient relationships and outcomes change over time. Are different supports needed for caregivers of those in the early versus more established stages of disorder or who have their onset in adolescence versus adulthood? Because the associations are so complex, we need a more individualised approach. Caring for caregivers should be a priority for clinical and research agendas.
Footnotes
Acknowledgements
The authors wish to thank the young people, family, friends and staff of the HYPE and EPPIC programmes at Orygen.
Author Contributions
All authors have had extensive experience in working with young people with first-episode psychosis and/or borderline personality disorder and their caregivers in both clinical and research settings. A range of co-authors were involved in the design and conduct of the original studies and the current study: Altitudes study (J.F.M.G., M.A.-J., D.E., S.B., S.M.C.), MS-BPD (A.M.C., J.M.B., S.M.C., M.S., V.K.R., M.J., B.M., C.A.H., L.M., E.B., C.M.) and Kindred (J.F.M.G., A.M.C., S.M.C., J.M.B., B.M., E.B., L.M., S.B., S.M., M.A.-J.). S.M.C. was responsible for the data analysis and drafting of the article. All authors critically revised and approved the final manuscript for submission. All authors agree to be accountable for all aspects of the work in ensuring that the questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Altitudes was funded through the Australian Government’s Collaborative Research Networks (CRN) programme. Kindred was also funded through the CRN programme. The trial administer of the funds was The Australian Catholic University. MS-BPD was funded through a Melbourne Health Grant in Aid (GIA-013-2015). S.M.C. is funded by a National Health and Medical Research Council Senior Research Fellowship (APP1136344).
Data Availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.