
Abstract
Objective:
Medical comorbidities are prevalent in patients with bipolar disorder. Evaluating longitudinal trends of the incidence of medical illnesses enables implementation of early prevention strategies to reduce the high mortality rate in this at-risk population. However, the incidence risks of medical illnesses in the early stages of bipolar disorder remain unclear. This study investigated the incidence and 5-year trend of medical illnesses following bipolar disorder diagnosis.
Methods:
We identified 11,884 patients aged 13–40 years who were newly diagnosed as having bipolar disorder during 1996–2012 and 47,536 age- and sex-matched controls (1:4 ratio) who represented the general population from Taiwan’s National Health Insurance Research Database. We estimated the prevalence and incidence of individual medical illnesses yearly across the first 5 years after the index date. The adjusted incidence rate ratio was calculated to compare the occurrence of specific medical illnesses each year between the bipolar disorder group and control group using the Poisson regression model.
Results:
Apart from the prevalence, the adjusted incidence rate ratios of most medical illnesses were >1.00 across the first 5-year period after bipolar disorder diagnosis. Cerebrovascular diseases, ischaemic heart disease, congestive heart failure, other forms of heart disease, renal disease and human immunodeficiency virus infection exhibited the highest adjusted incidence rate ratios during the first year. Except for that of renal disease, the 5-year trends of the adjusted incidence rate ratios decreased for cerebrovascular diseases, cardiovascular diseases (e.g. ischaemic heart disease, other forms of heart disease, and vein and lymphatic disease), gastrointestinal diseases (e.g. chronic hepatic disease and ulcer disease) and communicable diseases (e.g. human immunodeficiency virus infection, upper respiratory tract infection and pneumonia).
Conclusion:
Incidence risks of medical illnesses are increased in the first year after bipolar disorder diagnosis. Clinicians must carefully evaluate medical illnesses during this period because the mortality rates from medical illnesses are particularly high in people with bipolar disorder.
Introduction
Bipolar disorder is a severe mental illness that usually manifests as episodic mood swings, cognitive impairment and socio-occupational dysfunction (Baune and Malhi, 2015; Grande et al., 2016; Jauhar et al., 2019). Compared with the general population, individuals with bipolar disorder are at 1.5–3 times higher risk of developing various medical illnesses (Correll et al., 2017; Crump et al., 2013; Firth et al., 2019; Forty et al., 2014; Goldstein et al., 2015; Leboyer et al., 2012). Furthermore, among individuals with bipolar disorder, medical comorbidities markedly increase the severity of mood symptoms, rate of suicide attempts, chance of relapse and rehospitalisations, and number of life-years lost (Crump et al., 2013; Forty et al., 2014; Kemp et al., 2010, 2014; Leboyer et al., 2012; Plana-Ripoll et al., 2019). Numerous studies have indicated the bidirectional association between mental and physical dimensions during the progression of bipolar disorder (Forty et al., 2014; Kemp et al., 2010; Kemp et al., 2014; Leboyer et al., 2012) and have proposed the incorporation of medical illnesses into staging models of bipolar disorder to determine their chronicity and complexity in terms of bipolar illness (Berk et al., 2017; Leboyer et al., 2012; Morris et al., 2019; Shah et al., 2020). Implementing this proposal necessitates an accurate description of the onset of medical illnesses and their longitudinal course during the progression of bipolar disorder. In particular, research focusing on the occurrence of medical illnesses during the early stages of bipolar disorder would be helpful in guiding early intervention strategies against premature deaths in this at-risk group. Several studies have investigated the prevalence of medical illnesses among young patients with early-onset bipolar disorder (Evans-Lacko et al., 2009; Goldstein et al., 2015; Jerrell et al., 2010) and have revealed that medical comorbidities are already prevalent even in patients with bipolar disorder during adolescence and young adulthood. Incidence is a measure of the frequency at which new cases occur over a specified period; accordingly, evaluating longitudinal trends for the incidence of medical illnesses can provide insights into the progression of such illnesses. However, data regarding the incidence of medical illnesses during the early stages of bipolar disorder are lacking.
In regard to the knowledge gap and clinical merits, we conducted this study to investigate the incidence of various medical illnesses in a large bipolar disorder cohort using a nationwide population-based claims database. We randomly selected age- and sex-matched controls (at a 1:4 ratio) from a representative cohort of the general population in Taiwan. The trends of the incidence rate ratios (IRRs) of medical illnesses were evaluated in each of the first 5 years following bipolar disorder diagnosis to determine the incidence risks of such illnesses during the early stages of this disorder.
Methods
The Taipei City Hospital Research Ethics Committee approved the present study protocol (TCHIRB-10708113-E) and waived the need for informed consent due to the deidentified and retrospective nature of data. Data that could be used to identify beneficiaries and medical care providers were encrypted by the Taiwan National Health Insurance (NHI) Administration.
Data sources
Data used in this study were derived from the Psychiatric Inpatient Medical Claims (PIMC) database – a subset of the Taiwan National Health Insurance Research Database (NHIRD) – for the period between 1 January 1996 and 31 December 2012. In Taiwan, the NHI programme was implemented in 1995 and provides comprehensive medical care for nearly 98% of the 23,000,000 people in Taiwan. The NHIRD contains the registration files and medical claims data of beneficiaries covered by the NHI programme. Information available in the NHIRD includes detailed diagnostic codes according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
The PIMC database includes data on psychiatric inpatients with ICD-9-CM codes of 290–319 for the period between 1 January 1996 and 31 December 2012. Each year, the NHI Administration conducts randomised reviews of medical records to verify the diagnoses. In addition, the Taiwan Joint Commission on Hospital Accreditation oversees the accreditation of hospitals contracted with the NHI. The accreditation for qualified psychiatric services requires board-certified psychiatrists to diagnose patients. Therefore, the PIMC database has acceptable diagnostic coding accuracy for epidemiological research. To date, the PIMC database has been the data source for numerous epidemiological studies (Chen et al., 2019b, 2020b).
Identification of newly diagnosed bipolar disorder cohort
To identify the bipolar disorder cohort, we first selected a cohort of patients from the PIMC database who had at least one psychiatric admission for bipolar disorder (ICD-9-CM codes: 296.0–296.16, 296.4–296.81 and 296.89) between 1 January 1998 and 31 December 2012 (e-Figure 1 in the Supplemental Material). Subsequently, we excluded patients who had psychiatric admission between 1 January 1996 and 31 December 1997 to ensure that we included only patients who had their first incident of bipolar disorder that required psychiatric hospitalisation during the study period. We then excluded patients who ever received a diagnosis of schizophrenia (ICD-9-CM codes: 295.**) between 1 January 1996 and 31 December 2012. By adopting the definition of early-onset bipolar disorder (i.e. onset before the age of 40 years) proposed recently by the International Society for Bipolar Disorders Task Force (Sajatovic et al., 2015), we restricted the patient age to 13–40 years and eventually identified 11,884 patients who received a diagnosis of early-onset bipolar disorder between 1 January 1998 and 31 December 2011 (i.e. the study cohort).
To minimise the confounding effects of age and sex, for each patient with bipolar disorder, we randomly selected four age-matched (±0 year) and sex-matched controls from the NHIRD that represented the general population in Taiwan (e-Figure 1 in the Supplemental Material). The controls were assigned the same index date (i.e. the date of the first diagnosis of bipolar disorder) as their corresponding case. To confirm that the controls were alive before the corresponding index dates, each control was required to have at least one claims record after the corresponding index date. Accordingly, a total of 11,884 patients with bipolar disorder were matched with 47,536 controls.
Demographic and clinical variables
We obtained demographic and clinical variables, namely, sex, age, urbanisation level of residence location, employment and Charlson Comorbidity Index (CCI) score, at the index date for both patients and age- and sex-matched controls. Urbanisation was categorised into the following five levels, which are used specifically in Taiwan: Level 1 (highly urbanised area), Level 2 (moderately urbanised area), Level 3 (township area), Level 4 (subrural area) and Level 5 (rural area). The CCI was used to categorise the severity of medical comorbidities (assigned with scores of 0, 1 or ⩾2) according to the ICD-9-CM codes for primary and other diagnoses in the NHIRD (Charlson et al., 1987; Romano et al., 1993). The CCI comprised 17 medical illnesses within 1 year prior to the index date, namely, myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic pulmonary disease, connective tissue disease, ulcer disease, mild liver disease, diabetes, diabetes with end organ damage, hemiplegia, moderate or severe renal disease, any tumour, moderate or severe liver disease, metastatic solid tumour and acquired immune deficiency syndrome.
Variables of medical illnesses
In this study, we categorised medical illnesses into the following seven major organ systems: cardiovascular, cerebrovascular, respiratory, gastrointestinal, renal, endocrine/metabolic and musculoskeletal/integument. We also investigated the prevalence and incidence of human immunodeficiency virus (HIV) infection and cancer because these illnesses are increasing in young patients with bipolar disorder (Chen et al., 2019a; Hung et al., 2014). Detailed information on ICD-9-CM codes for the medical illnesses considered in this study is listed in e-Table 1 in the Supplemental Material.
Statistical analysis
We first computed the prevalence of each medical illness within the first year after the diagnosis of bipolar disorder. The risks of prevalent medical illnesses between the bipolar disorder cohort and control cohort were initially compared using a univariable conditional logistic regression analysis (Table 2). Subsequently, we conducted a multiple conditional logistic regression analysis to estimate the risk of each prevalent medical illness within 1 year after bipolar disorder. The backward stepwise strategy was used to select variables with p < 0.001 in the final model (Table 3).
Next, we calculated the first-year incidence of each medical illness after the diagnosis of bipolar disorder (Table 4). Consider, for example, hypertension: To estimate the incidence of hypertension, we first excluded patients who had hypertension prior to bipolar disorder diagnosis (i.e. between the date of the first diagnosis of bipolar disorder and 1 January 1996). Subsequently, we computed the incidence of hypertension after the diagnosis of bipolar disorder as the number of new cases with hypertension divided by the contributed person-years of the cohort without preexisting hypertension. We used the same method to calculate the incidence of each medical illness after the index date in the matched control cohort. The IRR was calculated as the ratio of the incidence of a specified medical illness between the bipolar disorder cohort and control cohort to determine whether the occurrence of this medical illness in the bipolar disorder cohort differed from that in the control cohort. To reveal the trends of the incidence and IRRs across the 5-year period after the diagnosis of bipolar disorder, we calculated the IRRs of each medical illness in the first, second, third, fourth and fifth year after the date of the first diagnosis of bipolar disorder (Figure 1). We applied the Poisson regression model to estimate the adjusted IRRs (aIRRs) and their 95% confidence intervals (Szklo and Nieto, 2019). A person–time value was registered for each patient and control from the index date until the occurrence of a specified disease incidence or mortality. Besides, we respectively conducted the Poisson regression model to evaluate the aIRRs of each medical illness between the first year and subsequent second, third, fourth and fifth year after the diagnosis of bipolar disorder. A p value of <0.001 was considered statistically significant in this study.
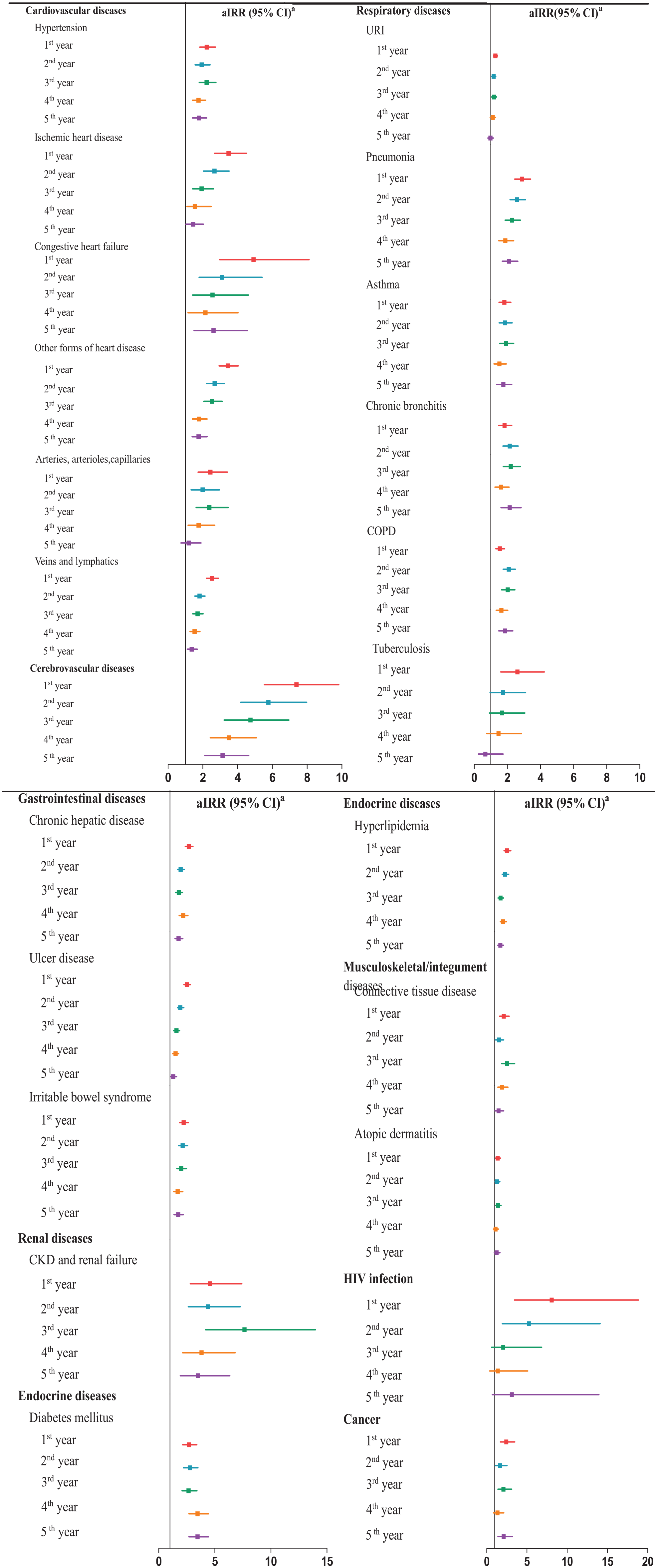
Adjusted incidence rate ratio (95% CI) of various medical illnesses within the first 5 years after the index date among patients with newly diagnosed bipolar disorder compared with age- and sex-matched controls.
Sensitivity analysis
Because patients with new-onset bipolar disorder could be younger than 30 years, and approximately 38% of the patients included in this study were aged above 30 years when they received their first diagnosis of bipolar disorder, we performed a sensitivity analysis using a subgroup of patients aged 13–29 years to estimate the incidence and aIRRs of each medical illness within 1 year after the index date in the patient cohort and control cohort. The study flow diagram is illustrated in e-Figure 2 in the Supplemental Material. Furthermore, to consolidate our results for patients with a first diagnosis of bipolar disorder, we performed another sensitivity analysis using a subgroup of patients who were entered into the cohort between 1 January 2001 and 31 December 2011 to allow for a 5-year washout period (i.e. between 1 January 1996 and 31 December 2000). The study flow diagram is presented in e-Figure 3 in the Supplemental Material. All statistical analyses were conducted using SAS v9.4 (SAS Institute, Cary, NC, USA).
Results
Demographic and clinical characteristics
Table 1 presents the demographic and clinical characteristics of the patient cohort and control cohort. The male-to-female sex ratio in the study cohort was 1.30. Approximately 60% of the patients in the study cohort were newly diagnosed as having bipolar disorder before the age of 30 years. Compared with the control group, the patients tended to live in highly urbanised area, be unemployed and have significantly higher CCI scores.
Demographic and clinical characteristics of patients with newly diagnosed bipolar disorder and age- and sex-matched controls at the index (corresponding) date.
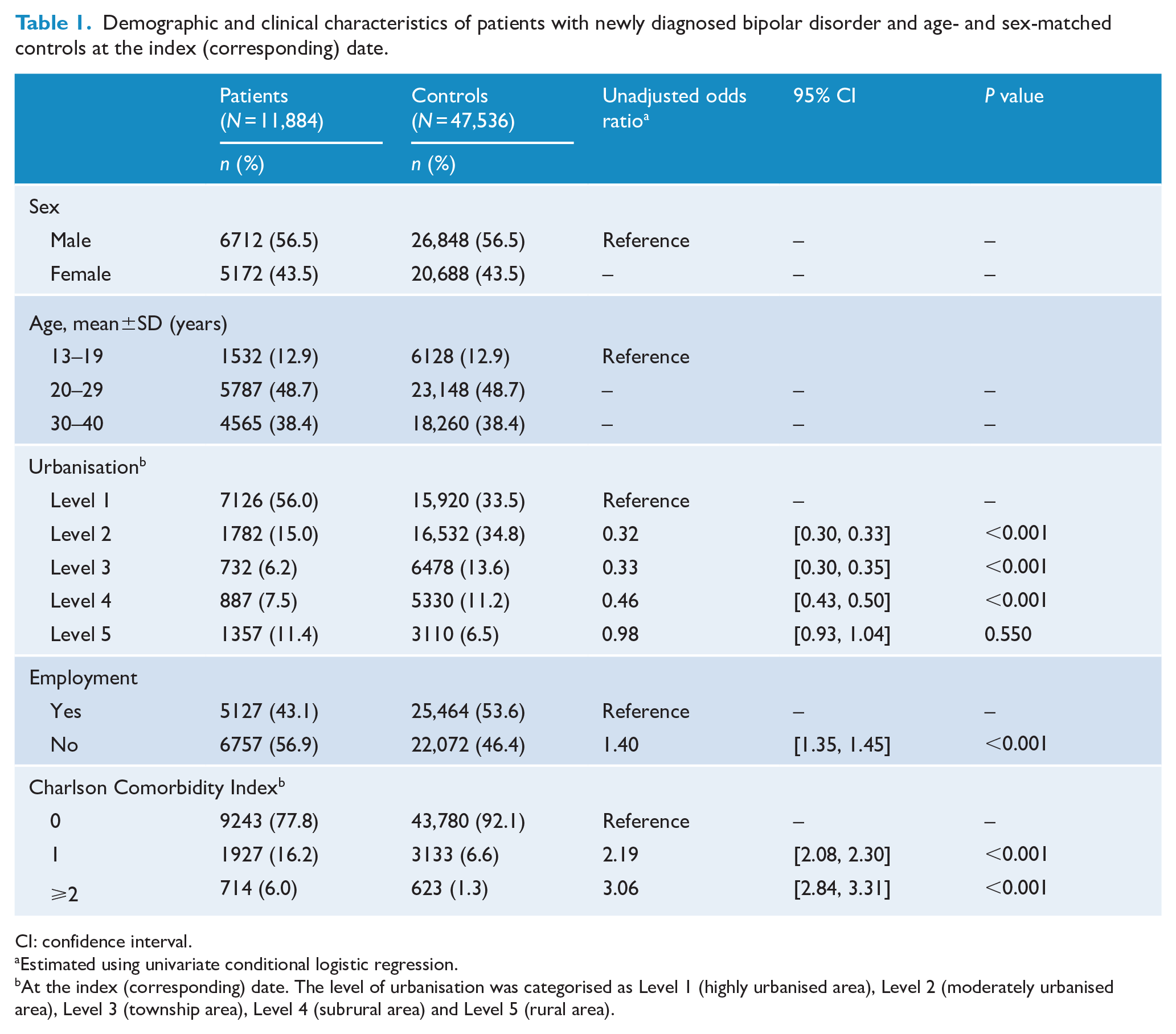
CI: confidence interval.
Estimated using univariate conditional logistic regression.
At the index (corresponding) date. The level of urbanisation was categorised as Level 1 (highly urbanised area), Level 2 (moderately urbanised area), Level 3 (township area), Level 4 (subrural area) and Level 5 (rural area).
Medical illnesses within 1 year after bipolar disorder diagnosis
Table 2 shows the prevalence of medical illnesses within the first year after bipolar disorder diagnosis. Compared with the control cohort, the patients exhibited an increased risk of numerous medical illnesses across all major organ systems. Furthermore, the multiple conditional logistic regression analysis results demonstrated that the patient cohort had a significantly higher risk of medical illnesses among six organ systems in the first year after diagnosis (Table 3). The risk of HIV infection also increased for patients within 1 year following bipolar disorder diagnosis.
Prevalence of medical illnesses within 1 year after the index date among patients with newly diagnosed bipolar disorder and age- and sex-matched controls.
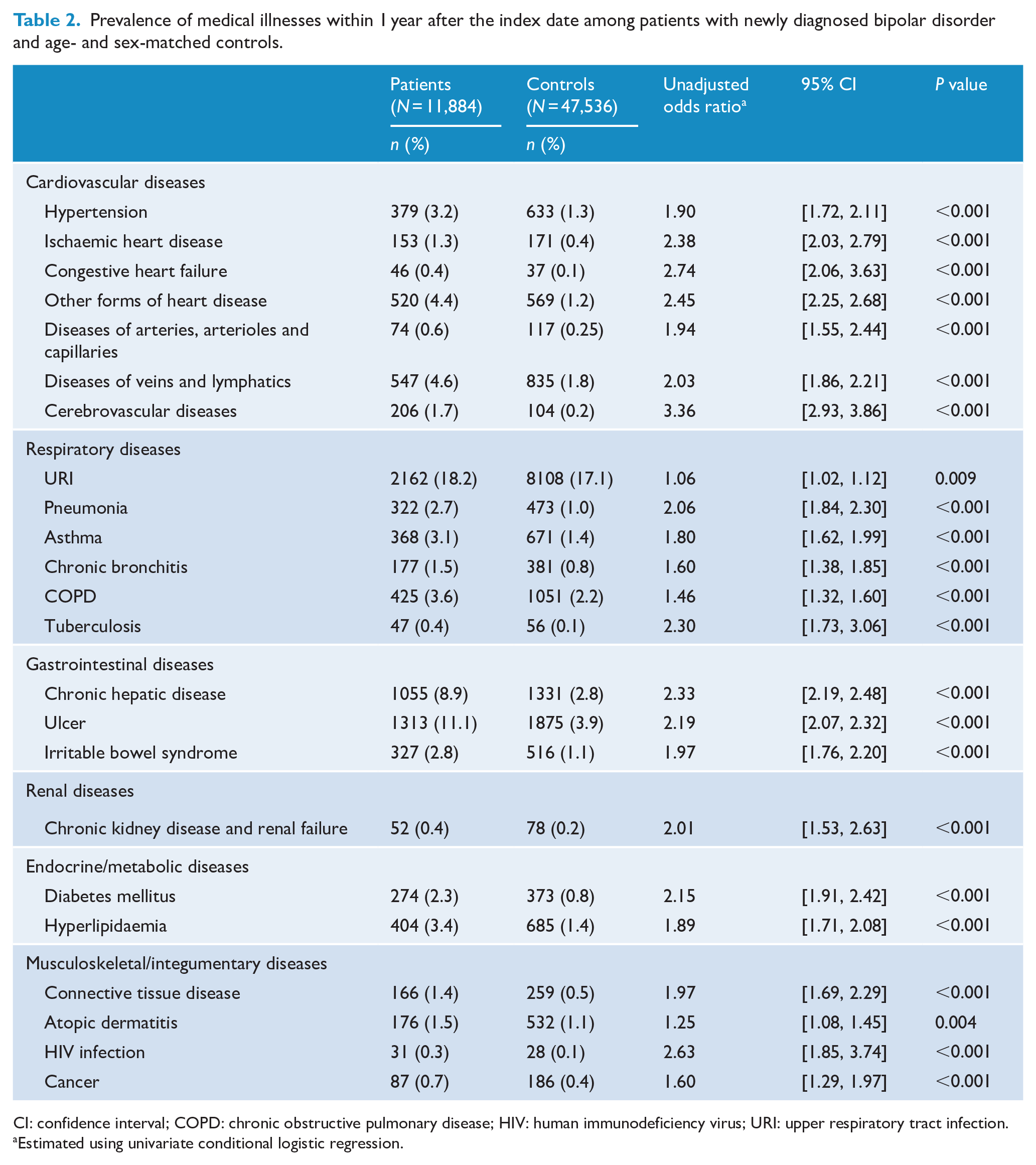
CI: confidence interval; COPD: chronic obstructive pulmonary disease; HIV: human immunodeficiency virus; URI: upper respiratory tract infection.
Estimated using univariate conditional logistic regression.
Multiple conditional logistic regression of prevalent medical illnesses within 1 year after the index date among patients with newly diagnosed bipolar disorder and age- and sex-matched controls.
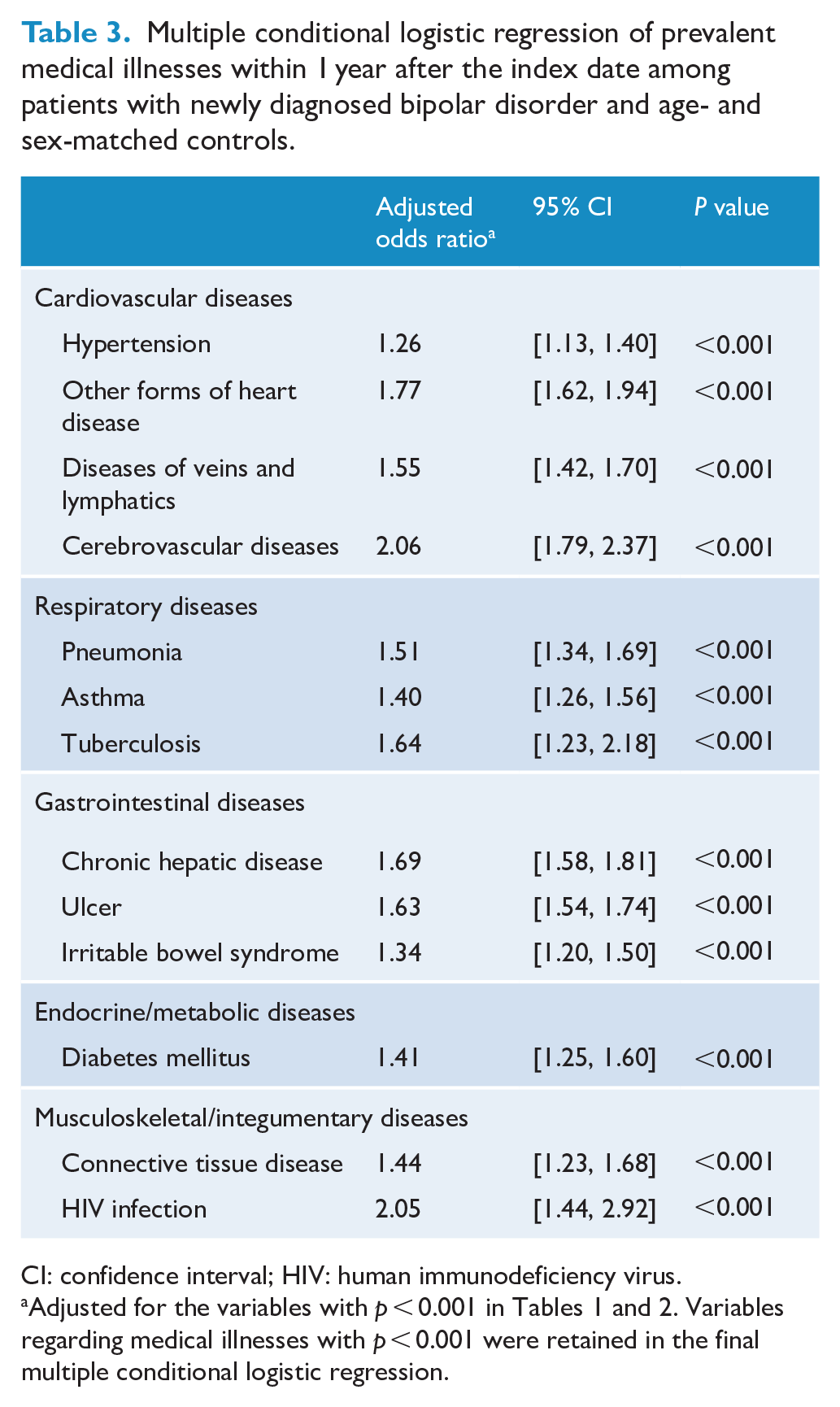
CI: confidence interval; HIV: human immunodeficiency virus.
Incidence of medical illnesses within 1 year after bipolar disorder diagnosis
We estimated the incidence of each specific medical illness across organ systems in the patient cohort and control cohort. Table 4 presents the incidence and aIRRs of specific medical illnesses between the patient cohort and the control cohort during the first year after the index date. Notably, the aIRRs of the medical illnesses were >1.00 across the organ systems. In particular, HIV infection, cerebrovascular diseases, ischaemic heart disease, congestive heart failure, other forms of heart disease, chronic kidney disease and renal failure had the highest aIRRs within the first year.
Incidence and adjusted incidence rate ratios of medical illnesses in the first year after the index date among patients with newly diagnosed bipolar disorder compared with age- and sex-matched controls.
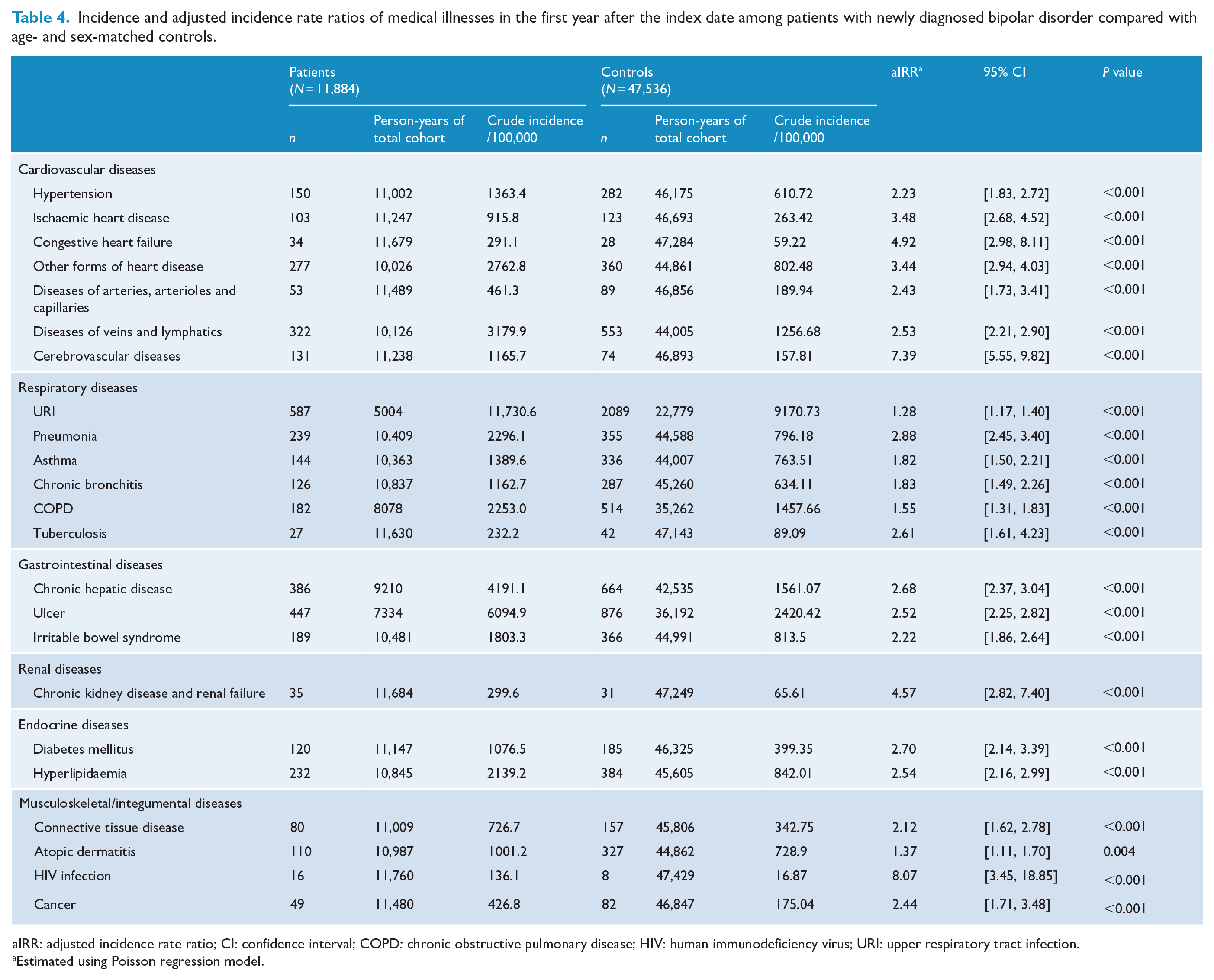
aIRR: adjusted incidence rate ratio; CI: confidence interval; COPD: chronic obstructive pulmonary disease; HIV: human immunodeficiency virus; URI: upper respiratory tract infection.
Estimated using Poisson regression model.
Incidence of medical illnesses across the first 5 years after bipolar disorder diagnosis
Figure 1 illustrates the aIRRs of specific medical illnesses between the patient cohort and control cohort within 5 years after the index date (for detailed information, see e-Tables 2–5 in the Supplemental Material). Notably, the aIRRs of most medical illnesses between patients and controls were consistently greater than 1.00 throughout the first 5 years after the index date. In addition, among patients with bipolar disorder, the 5-year trends of the aIRRs based on the first-year incidence rates as the reference revealed a decline for cardiovascular diseases (e.g. ischaemic heart disease, other forms of heart disease and diseases of veins and lymphatics), cerebrovascular diseases, gastrointestinal diseases (e.g. chronic hepatic disease and ulcer disease) and communicable diseases (e.g. HIV infection, upper respiratory tract infection and pneumonia) (for detailed information, see e-Table 6 in the Supplemental Material).
Subgroup analyses of patients with adolescent-onset bipolar disorder (i.e. age of onset: 13–18 years) showed that the aIRR in the first year of bipolar disorder was the highest for cerebrovascular diseases, followed by connective tissue disease and hypertension (for detailed information, see e-Table 7 in the Supplemental Material). On the contrary, for patients with adult-onset bipolar disorder (i.e. age of onset: >18 years), the aIRR in the first year following bipolar disorder diagnosis was the highest for HIV infection, followed by cerebrovascular diseases and congestive heart failure (for detailed information, see e-Table 8 in the Supplemental Material).
Sensitivity analysis
In the first sensitivity analysis of patients aged between 13 and 29 years, we used ischaemic heart disease and cerebrovascular diseases as examples; the results revealed aIRRs of 2.54 and 7.12 within the first year after bipolar disorder diagnosis, respectively (for detailed information, see e-Table 9 in the Supplemental Material). These findings were similar to those obtained from the main analysis of the entire cohort (3.48 and 7.39). In the second sensitivity analysis that involved a 5-year washout period, the aIRRs of ischaemic heart disease and cerebrovascular diseases within the first year after bipolar disorder diagnosis were 3.94 and 9.43, respectively, and were similar to those obtained from the main analysis of the entire cohort (e-Table 10 in the Supplemental Material).
Discussion
This is the first nationwide population-based cohort study to investigate the incidence and IRRs of medical illnesses in early-stage bipolar disorder. Our data provided detailed information on the trends of the incidence and aIRRs of medical illnesses in the early stages of bipolar disorder, revealing that the aIRRs of most medical illnesses were consistently greater than 1.00 within the first 5 years following bipolar disorder diagnosis. Notably, cerebrovascular diseases, cardiovascular diseases, renal diseases and HIV infection had the highest aIRRs during the first year after bipolar disorder diagnosis. In addition, observing the 5-year trends of the aIRRs revealed a decline in the aIRRs of cardiovascular diseases, cerebrovascular diseases, gastrointestinal diseases and communicable diseases such as HIV infection. Consistent with the findings of previous studies (Crump et al., 2013; Firth et al., 2019; Forty et al., 2014; Leboyer et al., 2012), our results confirm that bipolar disorder is a multisystem disease that begins manifesting in the early stage of illness.
In this study, cerebrovascular diseases and cardiovascular diseases were the noncommunicable medical illnesses with the highest incidence risk during the first year after bipolar disorder diagnosis. Our findings are in line with those of studies that have indicated an increased vascular risk among patients with early-onset bipolar disorder (Goldstein et al., 2015; Hatch et al., 2015; Naiberg et al., 2017; Westman et al., 2013). Although most well-known vascular risk factors are lifestyle-related (Arnett et al., 2019; Kotseva et al., 2019), our results, along with those of previous studies (Goldstein et al., 2015; Hatch et al., 2015; Naiberg et al., 2017; Westman et al., 2013), suggest that vascular risks are similar in patients with bipolar disorder across different countries where people have different lifestyles. These findings imply that in addition to lifestyle-related factors, certain vascular risk factors might be inherent to the disease process of bipolar disorder.
Our analyses also demonstrated that the aIRRs of cerebrovascular and cardiovascular diseases decreased over the 5-year period after the diagnosis of bipolar disorder. Evidence indicates that vascular risk begins to increase in patients with bipolar disorder since adolescence and young adulthood (Goldstein et al., 2015; Hatch et al., 2015; Naiberg et al., 2017). Somatic diseases are often underdiagnosed in this population (Goldstein et al., 2015; Liu et al., 2017). Therefore, our observations on the downward trends of the aIRRs of cerebrovascular disease and cardiovascular disease may reflect the trends of diagnosis at the time of clinical encounters. However, these downward trends could also be attributed to the potential benefits of the psychiatric care for patients with bipolar disorder. For instance, lithium is associated with a reduced risk of cerebrovascular diseases and cardiovascular diseases in patients with bipolar disorder (Lan et al., 2015; Prosser and Fieve, 2016), likely through the inhibition of proinflammatory responses, reactive oxidative stress and endothelial dysfunction (Kim et al., 2015; Lee et al., 2014). Furthermore, adjunctive psychosocial therapy can prevent relapse and enhance mood stability (Miklowitz et al., 2021), which in turn improves adherence to somatic treatment in patients with bipolar disorder (Levin et al., 2017). Few studies have evaluated whether contact with the mental health system or a specific treatment modality offers protective effects against cardiovascular risk factors in the bipolar disorder population. Considering that patients with bipolar disorder are at a high risk of cardiovascular mortality (Chen et al., 2020a; Westman et al., 2013), future studies are urgently required in this area. Such data could guide further trial studies on the effectiveness of a specific intervention or treatment modality against the initiation and progression of cardiovascular diseases in patients with bipolar disorder.
Among communicable diseases, HIV infection had the highest aIRR during the first year after bipolar disorder diagnosis, and its aIRR declined across the first 5 years after diagnosis. Studies have shown that adolescents and young adults with bipolar disorder have an increased risk of sexually transmitted diseases such as HIV infection (Chen et al., 2019a). The mood symptoms of bipolar disorder and the comorbidities of substance and alcohol use disorders increase the risk of sexually transmitted diseases, including HIV infection, among patients with bipolar disorder (Krantz et al., 2018; Meade et al., 2011). In particular, use of mood stabilisers and second-generation antipsychotics attenuates the observed risk (Chen et al., 2019a). The protective effects of psychopharmacotherapy against sexually transmitted diseases may be mediated by the reduction in affective symptoms, comorbid substance and alcohol use disorders, and risky behaviours (Chen et al., 2019a), which may also explain our observation.
Notably, the aIRRs of renal diseases were consistently >3.50 across the 5-year period following the diagnosis of bipolar disorder. The underlying mechanisms remain unclear and should be investigated in further research. A possible explanation is related to the nephrotoxicity of psychotropic medications used to treat bipolar disorder. Lithium and anticonvulsant mood stabilisers increase the risk of chronic kidney disease by approximately twofold in patients with bipolar disorder (Kessing et al., 2015). Furthermore, lithium may increase the risk of renal failure in patients with coexisting somatic diseases (Aiff et al., 2019). Nevertheless, other studies have not observed this association between lithium use and the risk of chronic kidney disease or renal failure (Kessing et al., 2017; McKnight et al., 2012). Therefore, future studies should investigate whether exposure to psychotropic medications contributes to the increased risk of renal diseases in early-stage bipolar disorder.
In this study, although the aIRRs of certain medical illnesses were the highest in the first year and reduced steadily in each subsequent year following bipolar disorder diagnosis, other medical illnesses did not exhibit this trend. Although we proposed some possible explanations for these complex observations, understanding the nature of these complex manifestations requires further research. A series of studies need to target each specific medical illness and identify factors that aggravate or alleviate the initiation and progression of each in the bipolar disorder population. Furthermore, studies must also integrate medical illnesses as an extended dimension in the multidimensional staging model and examine the correlations of clinical courses of medical illnesses and other core components of bipolar disorder. Such data could be used in the development of a clinical staging model of multisystem bipolar disorder and meaningfully guide mental health workers in the delivery of multidisciplinary healthcare.
Studies have increasingly suggested that adolescent- and adult-onset bipolar disorder may be distinct subtypes in terms of their pathophysiology, psychiatric comorbidity and clinical outcomes (Baldessarini et al., 2012; Baykara et al., 2021; Frahm Laursen et al., 2019; Goldstein and Levitt, 2006). However, few studies have investigated the initiation and progression of medical illnesses between these two subtypes during the early stage of bipolar disorder. Our subgroup analyses revealed that patients with adolescent-onset bipolar disorder tended to be at an increased risk of connective tissue disease in addition to cerebrovascular and cardiovascular diseases in the first year of bipolar disorder, but those with adult-onset bipolar disorder were at an elevated risk of HIV infection in addition to cerebrovascular and cardiovascular diseases. The results indicated that patients with adolescent- or adult-onset bipolar disorder may have differential risks of certain medical illnesses during the progression of bipolar disorder. Given the relatively small sample size of patients with adolescent-onset bipolar disorder in this study, larger naturalistic clinical cohorts are required to examine the risk of various medical illnesses between adolescent- and adult-onset bipolar disorder.
Strengths and limitations
The use of a Taiwanese population–based database enabled us to investigate the incidence of medical illnesses in a representative bipolar disorder cohort. Therefore, our results are less confounded by selection bias. Moreover, the NHIRD comprises detailed information on the diagnostic codes of all NHI beneficiaries, allowing us to examine various types of medical illnesses across different organ systems.
Nevertheless, our study has several limitations. First, in this study, we matched patients and controls based on age and sex to limit potential confounding by these two factors. However, statistical power may have been reduced, limiting our ability to detect differences in certain medical illnesses between patients and controls. In addition, this study calculated incidence rates using person-exposure years, which could be problematic when hazards (i.e. the risk of adverse events) are not constant over time (Kraemer, 2009). However, we used adjusted IRR as the index based on Poisson regression model for the best estimation. Second, the diagnoses of psychiatric and medical illnesses were based solely on ICD-9-CM codes, and hence, their validity could be questioned. However, the NHI Administration randomly reviews medical records to verify diagnoses each year; consequently, the NHIRD has acceptable coding accuracy for epidemiological analysis. Third, although we applied a washout period from 1 January 1996 to 31 December 1997 to exclude prevalent cases, some cases in our study may have been prevalent because bipolar disorder can occur much earlier during teenage years and early adulthood (Goldstein et al., 2017). This concern was especially relevant to 38% of the cohort aged between 30 and 40 years. Our sensitivity analyses conducted using a subgroup aged between 13 and 29 years as well as another subgroup that entered the cohort between 2001 and 2011 (i.e. allowing for a 5-year washout period) also revealed increased IRRs of medical illnesses across all organ systems. However, we were unable to dismiss the possibility of an index mood episode or preexisting medical illness prior to 1 January 1996. Similarly, the order of illness onset based on the diagnosis at the time of clinical encounters may not reflect the true directional links between medical and mental disorders before 1 January 1996. Fourth, to improve diagnostic accuracy, we selected inpatients with bipolar disorder from the PIMC database. Therefore, our findings may not be generalisable to patients without records of psychiatric admission. Fifth, because of limitations inherent to the NHIRD, we could not obtain variables related to lifestyle or compliance with medical treatment. In addition, we were unable to collect laboratory test data from the NHIRD. These data may be helpful for future research on pathogenetic mechanisms underlying the association between medical illnesses and bipolar disorder. Sixth, the mortality rates of patients with bipolar disorder were higher than those of the controls during the 5-year period after the index date, especially within the first-year period (data not shown). Survivorship bias may have affected our analyses of the IRR, particularly for medical illnesses with a high risk of mortality at a young age.
Conclusion
Despite the aforementioned limitations, this national population–based cohort study revealed that patients with bipolar disorder have an increased risk of numerous medical illnesses across multiple organ systems in the early stages of illness, particularly cerebrovascular diseases, cardiovascular diseases, renal diseases and communicable diseases such as HIV infection. In addition, their incidence risks, except for those of renal diseases, declined across the 5-year period after the diagnosis of bipolar disorder. To obtain a deeper understanding of the progression of medical illnesses in patients with bipolar disorder during the early stages, additional studies are required to investigate both risk and protective factors specific to individual medical illnesses in this at-risk population.
Supplemental Material
sj-doc-1-anp-10.1177_00048674211046891 – Supplemental material for Prevalence and 5-year trend of incidence for medical illnesses after the diagnosis of bipolar disorder: A nationwide cohort study
Supplemental material, sj-doc-1-anp-10.1177_00048674211046891 for Prevalence and 5-year trend of incidence for medical illnesses after the diagnosis of bipolar disorder: A nationwide cohort study by Pao-Huan Chen, Shang-Ying Tsai, Chun-Hung Pan, Yi-Lung Chen, Sheng-Siang Su, Chiao-Chicy Chen and Chian-Jue Kuo in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This manuscript was edited by Wallace Academic Editing.
Author Contributions
Drs P.-H.C. and C.-J.K. conceived and designed the study. Dr C.-J.K. acquired the data. Mr S.-S.S. performed the statistical analysis. Drs P.-H.C. and C.-J.K. drafted the manuscript. Drs C.-H.P. and Y.-L.C. made critical revisions to the manuscript for intellectual content. Drs S.-Y.T. and C.-C.C. provided administrative and material support and supervised the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was supported by grants from the Ministry of Science and Technology, Taiwan (MOST 105-2314-B-532-006-MY3 and MOST 108-2314-B-532-005) and Taipei City Hospital (10601-62-002). The funding sources had no involvement in the study design, data collection, data analysis, data interpretation, writing of the report or the decision to submit the paper for publication.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.