
Abstract
Objective:
There are concerns that the diagnostic boundaries of bipolar disorder have expanded. This study seeks evidence of change in diagnostic practice at three boundaries: the ‘lower’ boundary with subclinical mood conditions, the ‘lateral’ boundary with other mental health conditions (psychotic, anxiety, substance and personality disorders) and the ‘internal’ boundary within affective disorders.
Methods:
Diagnoses recorded in health system administrative data collections were used as a measure of clinician diagnostic behaviour. We examined all diagnoses made by public (state operated) inpatient and community mental health services in New South Wales, Australia, from 2003 to 2014.
Results:
A total of 31,746 people had at least one recorded diagnosis of bipolar disorder in the period. There was a significant upward trend in the age-standardised population rate of diagnosis of bipolar disorder. Bipolar disorders made up an increasing proportion of psychosis diagnoses. There was no increase in the rate of comorbid diagnosis of bipolar disorders with non-psychotic disorders or in the likelihood of diagnosis of bipolar disorder at first or subsequent episodes of depression. There were significant reductions in diagnoses of schizophrenia, particularly in younger people.
Conclusion:
There may be some increase in diagnoses of bipolar disorder in New South Wales public mental health services. However, some changes in diagnosis, particularly in younger adults, may reflect movement away from diagnoses of schizophrenia towards a range of other diagnoses, rather than specific movement towards bipolar disorder. Expansion of bipolar disorder may have been more marked in private practice settings and may have involved the poorly defined bipolar II subtype.
Introduction
The boundaries of bipolar disorders remain unclear. Under-diagnosis of bipolar disorders may have adverse consequences, including delayed or ineffective treatment (Parker, 2015). However, there have been recent concerns that the boundaries of bipolar disorder have expanded, leading to over-diagnosis (Malhi and Porter, 2014; Ruggero et al., 2010; Zimmerman, 2010a). This may also have adverse personal and social consequences, including unnecessary exposure to the risks of medication, missed opportunities for treatment of other conditions or effects on work participation (Zimmerman et al., 2010a).
Health service data provide an ideal method to test concerns about changes in diagnostic practice. Routinely recorded diagnoses, although an indirect measure of the underlying true prevalence of a disorder (Morgan and Jablensky, 2010), do provide a direct measure of clinician diagnostic behaviour. The current study examines diagnoses recorded during routine clinical care in all specialist mental health services in the Australian state of New South Wales (NSW), between 2003 and 2014.
Boundary creep
Concerns about over- and under-diagnosis of bipolar disorder (Malhi and Berk, 2014) have centred on ‘boundary creep’ and focused specifically on three separate boundaries (Figure 1).
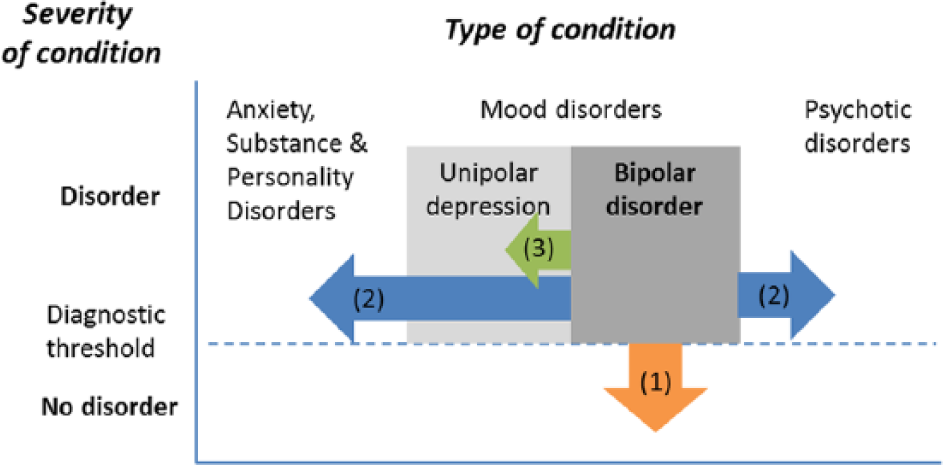
Possible directions of boundary expansion in bipolar disorder: (1) ‘lower’ boundary with subclinical mood swings, (2) ‘lateral’ boundaries with other conditions and (3) ‘internal’ boundaries within mood disorders.
First, bipolar disorders have a ‘lower’ boundary with normal or subclinical mood fluctuation. It has been suggested that
inability to characterise [bipolar disorder], and in particular a failure to identify a pristine lower boundary, has advanced the conflation of bipolar II disorder with normalcy and contributed to its over-diagnosis, particularly in young people, where it has seemingly given rise to an epidemic. (Malhi and Porter, 2014: 698)
We hypothesise that ‘downward’ expansion of bipolar disorder, particularly in younger people, would be reflected in health service data by (1) an apparent increase in the treated prevalence of bipolar disorder, (2) reduced average age of people being treated for bipolar disorder and (3) reduced age at an individual’s first diagnosis of bipolar disorder.
Second, there may have been expansion of the ‘lateral’ boundaries of bipolar disorder. In particular, the diagnosis of bipolar II disorder may have resulted in a broadening of the bipolar disorder concept to include abnormalities that would previously have been seen as a feature of other conditions. Substance disorders, anxiety disorders and personality disorders all frequently include abnormalities of mood and behaviour such as dysphoria, irritability, unstable mood, agitation, overactivity, impulsiveness or poor judgement (Leventhal and Zimmerman, 2010; Malhi, 2013a; Parker, 2015; Zimmerman, 2010b; Zimmerman et al., 2010b). These features may increasingly be seen as evidence of a bipolar disorder. The diagnostic boundary between bipolar disorders and various psychotic disorders is equally complex and includes the arguably spurious diagnostic category of schizoaffective disorder (Malhi, 2013b). In this context, a diagnosis of bipolar disorder may be less stigmatising and more hopeful than a diagnosis of schizophrenia for the individuals and families affected (Malhi and Porter, 2014). We hypothesise that ‘lateral’ diagnostic expansion would be evident in (1) an increased likelihood that individuals with substance, anxiety or personality disorders would receive a comorbid diagnosis of bipolar disorder and (2) an increase in the overall proportion of psychosis diagnosis made up by bipolar disorder diagnoses, especially in younger people.
Third, it has been suggested that there may have been repositioning of the ‘internal’ boundary separating unipolar from bipolar mood disorders: ‘mixed features that emerge in the context of depressive presentations (distractibility, agitation, irritability), which previously would have been regarded as superadded anxiety or agitated depression, may now be subsumed by bipolarity’ (Malhi and Porter, 2014: 699), resulting in a seeming expansion of bipolar disorder. We hypothesise that such change would be evident in (1) an increasing proportion of depressive episodes being diagnosed as bipolar disorder and (2) an increased likelihood that people with recurrent depressive episodes would receive a diagnosis of bipolar disorder.
Methods
Services and setting
We examined all diagnoses recorded by clinicians in public specialist mental health services for the Australian state of NSW, population 7.2 million. These are services funded and operated by the NSW state government, providing acute and non-acute inpatient and community mental health care. The services have primary responsibility for the care of NSW residents with serious mental illness and sole responsibility for involuntary mental health care. Diagnostic data from primary care, privately funded outpatient psychiatrists or private hospitals were not included.
De-identified and aggregated data from NSW Health’s administrative data warehouse, the Health Information Exchange (HIE), were used with permission of the data custodian.
Episodes of care
Episodes of inpatient and community care occurring between 1 January 2003 and 31 December 2014 and with at least one valid diagnosis were included. The start of this period was determined by the quality and completeness of diagnostic data. In NSW community mental health data, diagnoses are recorded at each individual contact. Therefore, for episode-level analyses, 3-month statistical episodes of care were first constructed, deriving community episode diagnoses from all contacts within that episode. For person-level analysis, inpatient and community episodes of care for an individual were then combined.
Diagnostic recording
Inpatient diagnoses are recorded at discharge from hospital by trained medical record coders, based on the diagnoses recorded by the treating psychiatrist or other medical officer. Community diagnoses are recorded by treating mental health clinicians. Data for both settings include principal (primary reason for hospitalisation or contact) and secondary diagnoses coded using the Australian Modification of International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10; National Centre for Classification in Health, 2010).
Because the study aimed to examine overlap of diagnoses within and between episodes, all diagnoses within an episode were recorded. Diagnoses of bipolar disorder were defined by the presence within a care episode of at least one primary or secondary diagnosis code of bipolar disorder (F31) or mania (F30). Other diagnoses were defined using ICD codes for psychosis (F20–29 plus specific codes for drug-induced psychoses), mood disorder (F32–39), anxiety disorder (F40–48), personality disorder (F60–62) and substance use disorder (F10–19). Bipolar depression was defined either by specific diagnosis codes for that condition (F31.2–31.5) or by diagnoses of depression (F32–33) and bipolar disorder (F31) occurring in the same episode of care. Psychosis diagnoses were broadly grouped into schizophrenia, bipolar disorder and other psychoses (including schizoaffective, brief, atypical and unspecified psychosis diagnoses).
Other variables
For inpatient episodes, year of contact was defined using the date of separation from hospital. Age and sex were recorded from an individual’s first episode of care occurring within the period of interest. Individual persons were counted in each year during which they had an episode of care. A first bipolar diagnosis for each person was defined using a maximum 5-year clearance period. Reference population data (www.healthstats.nsw.gov.au/Indicator/dem_pop_age) were used to calculate age- and sex-standardised estimates of treated prevalence. These estimates were calculated using population estimates for each calendar year, in order to account for effects of population growth, or changes in age or sex distribution over the study period.
Statistical analysis
Statistical analyses were conducted in Stata v13. For all variables, annual rates were calculated for each year from 2003 to 2014. Significance of linear trend for each variable was tested using Cuzick’s (1985) non-parametric trend test for ordered groups (Stata procedure nptrend).
Results
Results are summarised in Table 1 and Figure 2. Between 2003 and 2014, 1.99 million episodes of care were recorded. There were 31,746 individuals with at least one bipolar disorder diagnosis in this period, accounting for 77,489 person-years and 180,690 episodes of care (9.1% of total episodes of mental health care). The average age- and sex-standardised prevalence of bipolar disorder in 15- to 64-year-olds was 12.1 per 10,000 population, compared with 31.5 per 10,000 population for schizophrenia. Both estimates were higher when only 15- to 29-year-olds were examined (bipolar disorder, 14.6; schizophrenia, 39.9). The average age at first diagnosis of bipolar disorder was 41 years (standard deviation [SD] = 16 years), and 28% of people were aged less than 30 years at their first recorded bipolar disorder diagnosis.
Diagnoses of bipolar disorder in NSW public hospital and community mental health services, 2003–2014.
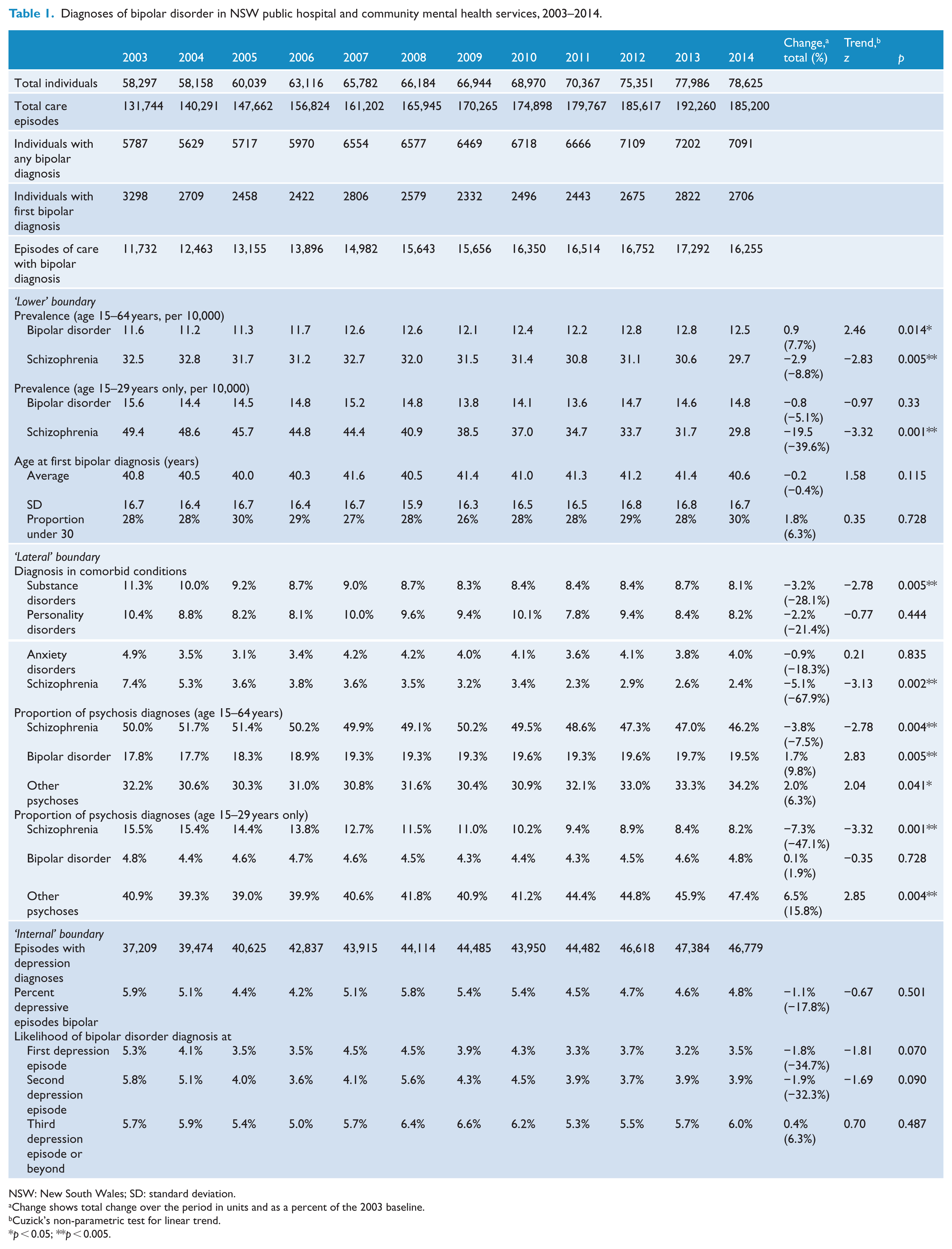
NSW: New South Wales; SD: standard deviation.
Change shows total change over the period in units and as a percent of the 2003 baseline.
Cuzick’s non-parametric test for linear trend.
p < 0.05; **p < 0.005.
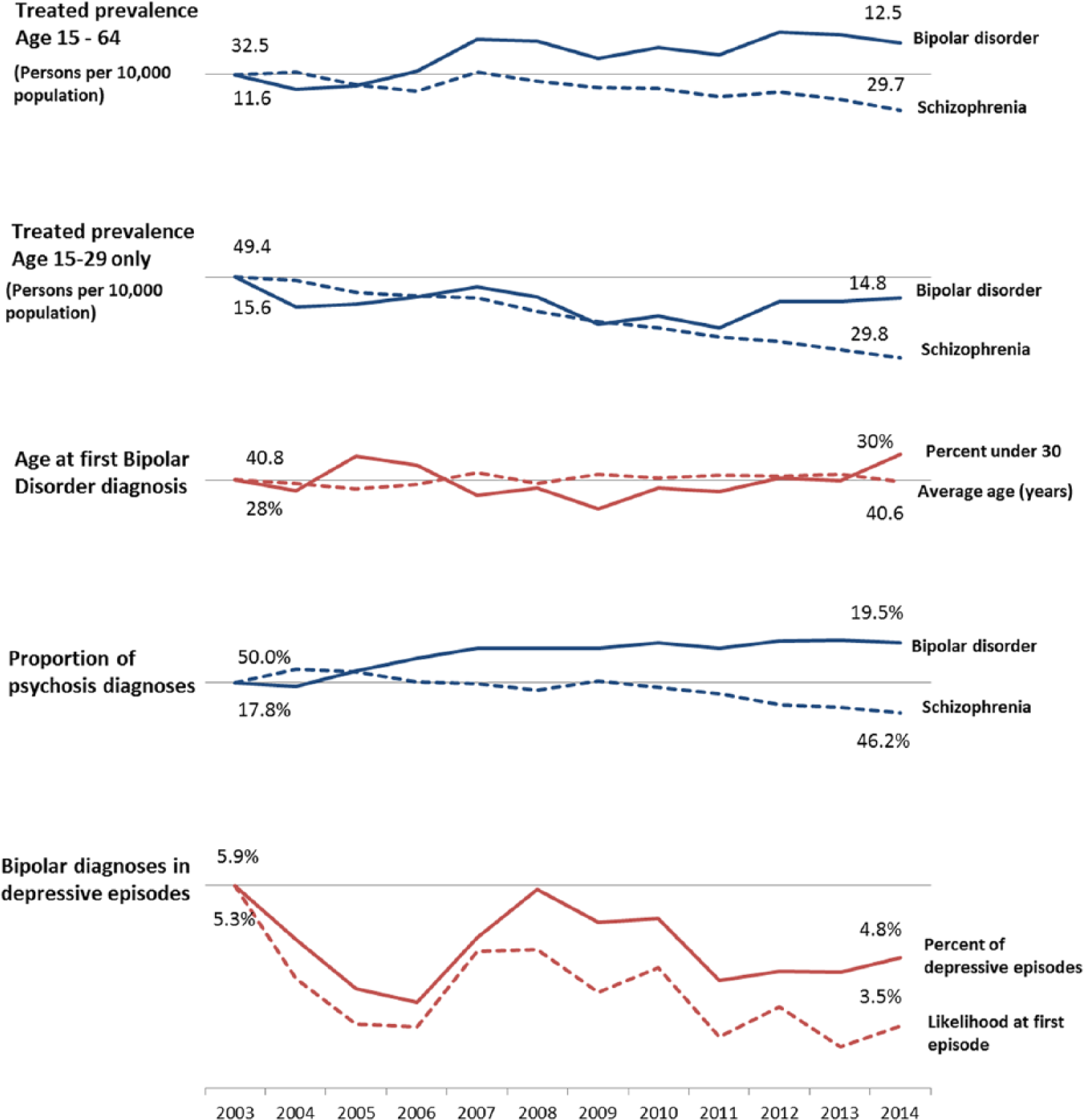
Selected indicators of diagnostic practice in bipolar disorder, NSW public mental health services, 2003–2014. Each variable plotted compared with its own 2003 baseline. Values for 2003 and 2014 labelled.
After adjusting for population growth, there was a significant upward trend in the diagnosed prevalence of bipolar disorder: age- and sex-standardised estimates increased by 0.9 persons per 10,000 (7.7%) compared to the 2003 baseline. There was also a corresponding (−8.8%) reduction in the diagnosed prevalence of schizophrenia in the same period. For people aged 15–29 years, there was no significant increase in diagnosed prevalence of bipolar disorder, but there was a significant downward trend in diagnosed prevalence of schizophrenia, which reduced from 49.4 per 10,000 to 29.8 per 10,000 over the study period. There was no significant change in the average age at first bipolar disorder diagnosis or the proportion of people aged less than 30 years at their first bipolar disorder diagnosis.
Examining ‘lateral’ boundaries of bipolar disorder with other psychiatric conditions, approximately 9% of people with diagnoses of substance disorder or personality disorder and approximately 4% of people with diagnoses of schizophrenia or anxiety disorder had comorbid diagnoses of bipolar disorder. There was no increase over time in the rate of comorbid bipolar disorder diagnoses in other specific mental health conditions. For schizophrenia and substance disorders, there was a significant linear trend in the opposite direction to that hypothesised, with a reduction in the rate of comorbid bipolar disorder diagnoses.
The mix of psychosis diagnoses changed substantially over the study period. There was a significant downward trend in the proportion of psychosis diagnoses which were schizophrenia and an upward trend in the proportion which were diagnoses of bipolar disorder or of other psychoses. For people aged 15–29 years, there was also a downward trend in diagnosis of schizophrenia and an upward trend in diagnosis of other psychoses; however, there was no significant change in the proportion of psychosis diagnoses which were bipolar disorder.
Examining the ‘internal’ boundary within affective disorders, only around 5% of episodes of care with diagnoses of depression also had a bipolar disorder diagnosis, and this proportion did not change over the study period. People were more likely to have a diagnosis of bipolar disorder made during a third or subsequent episode of depression (5.8%) than during a first or second episode (3.9%), and this rate did not change significantly over the study period.
Discussion
There is evidence that diagnostic practice in NSW public mental health services has changed between 2003 and 2014. These findings provide some support for concerns that the diagnostic boundaries of bipolar disorder are expanding, but also suggest that these changes are limited and are accompanied by diagnostic change for other conditions.
We found that the diagnosed prevalence of bipolar disorder increased by nearly 8% over the study period. There are several possible explanations for this finding. An apparent increase in bipolar disorder diagnoses may simply reflect better service access or data recording. However, there was not a corresponding increase in total psychosis diagnoses or in diagnoses of schizophrenia within the same period, which might be expected if the changes were merely due to service or system changes. Therefore, this finding could be consistent with an expansion in the ‘lower’ diagnostic boundary of bipolar disorder.
If such expansion has occurred, our findings do not support the concern that this has occurred primarily in younger people. There was no significant increase in diagnosed prevalence of bipolar disorder in people aged 15–29 years and no change in the average age at first bipolar diagnosis or the proportion of people aged under 30 years at their first diagnosis of bipolar disorder.
The most substantial change in diagnosis was seen at the ‘lateral’ boundary between bipolar disorder and schizophrenia. For the wider age group (aged 15–64 years), bipolar disorder increased and schizophrenia diagnoses declined as a proportion of all psychosis diagnoses. When only younger adults (15–29 years) were examined, the same proportional decline in schizophrenia diagnoses was seen, but with an increase in diagnoses of other psychoses (including brief and atypical psychoses) rather than bipolar disorder. Together, these findings may suggest a movement away from diagnoses of schizophrenia, particularly in younger people, rather than a specific movement towards diagnoses of bipolar disorder. This would be consistent with the impact of clinical staging models of psychosis on diagnostic practice (McGorry, 2010; Tandon et al., 2009), concerns about the demoralising impact of a diagnosis of schizophrenia in younger adults (Henderson and Malhi, 2014) and a shift towards a more dimensional approach to psychosis diagnosis (Van Os, 2014).
We did not find evidence of diagnostic expansion at the ‘lateral’ boundary between bipolar disorders and other non-psychotic conditions such as personality, substance and anxiety disorders in this particular population. The rate of comorbid bipolar disorder diagnoses was unchanged in people with anxiety or personality disorders and declined in people with substance disorder diagnoses. Interestingly, we also found no evidence of change in the ‘internal’ boundary between unipolar and bipolar depression.
Limitations
This study uses data only from state-operated (public) mental health services and therefore significantly under-enumerates the overall population rate of bipolar disorder in NSW. We found an annual treated prevalence of 0.12%. This is substantially lower than published estimates of the 12-month prevalence of bipolar disorder in the Australian population, which range from 0.5% (Mitchell et al., 2004) to 1.8% (Slade et al., 2009). Because our interest was in studying clinician behaviour rather than estimating prevalence, we chose a permissive diagnostic threshold (at least one diagnosis of bipolar disorder). This approach maximises sensitivity when compared to research interviews (Sara et al., 2014), but cannot account for the many people with bipolar disorder who have no contact with public mental health services.
Limiting the study to public mental health services also produces possible bias because these services typically care for people in more acute phases of illness or with more severe or disabling conditions. Therefore, our data may have been insensitive to changes in the ‘lower’ diagnostic boundary of bipolar disorder because few people with disorders of marginal severity are seen in public mental health services. We did not have access to data from primary care, private psychiatrists or private hospitals: mood disorder diagnoses may be made more variably in those settings (Malhi and Berk, 2014). Our findings cannot be generalised to apply to the diagnostic behaviour of ‘private’ clinicians in NSW, and further studies including primary care or private hospital data should examine this issue.
The lack of change in the ‘internal’ boundary between unipolar and bipolar depressive episodes may partly reflect the imprecision of diagnostic recording in routine health data. A very high proportion of episodes of depression receive non-specific clinical diagnoses such as ‘depressive episode’ or ‘major depression’, without more detailed specification of type. In our data, only 5% of all depressive episodes were diagnosed as occurring as part of a bipolar disorder. Bipolar disorder is clearly more common than this: diagnostic conversion from major depression to bipolar disorder has been shown to be of the order of 0.4–2.0% per year for bipolar I disorder and 0.5–1.8% per year for bipolar II disorder (Angst et al., 2005; Goldberg et al., 2001; Holma et al., 2008), suggesting perhaps that a diagnosis of bipolar disorder is often not documented during episodes of depression.
It is also possible that some of the changes seen over time reflect changes in information systems and data quality rather than true changes in diagnostic practice. Data systems in NSW community mental health services have undergone significant development during the study period. It would be possible to examine national hospital data to ensure that the changes seen are not specific to NSW information systems.
Summary and conclusion
Routinely recorded diagnoses may provide a useful measure of clinician diagnostic behaviour. In NSW public mental health services between 2003 and 2014, there was a significant increase in the population rate of diagnosis of bipolar disorders, which may suggest an expanded ‘lower’ boundary for diagnosing these conditions. There were substantial changes in the relative rates of diagnosis of bipolar disorder and schizophrenia, but these seemed driven more by movement away from diagnoses of schizophrenia than by specific movement towards diagnoses of bipolar disorder. The relatively modest increase in the diagnosis of bipolar disorder observed in a public service setting, which caters predominantly to the more severe end of the spectrum of mental illnesses, suggests that the apparent expansion in the diagnosis of bipolar disorder occurs within other sectors of health care and perhaps within a subset/subtype of bipolar disorder. Many patients with bipolar disorder are treated in private settings in NSW. This is especially the case for bipolar II disorder, which has a significant interface with personality disorders and anxiety, by definition does not include patients admitted to hospital when manic and is therefore more likely to be managed in outpatient settings. It is likely that an overemphasis on bipolar II disorder and the spectrum of bipolarity is the cause of the seeming expansion in bipolar disorder. Data from other settings need to be similarly examined to better understand this apparent diagnostic inflation.
Footnotes
Declaration of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.